
Abstract
Objective:
The pathophysiology of atopic dermatitis (AD) involves a complex interplay between immune system dysfunction, genetics, and environmental factors. It is well known that nutritional status is essential to a proper functioning immune system, leading to a highly debated question regarding the role of dietary factors in the pathogenesis of AD. Food allergies and elimination diets have been broadly studied in atopy; however, less consideration has been given to how vitamins, minerals, and other micronutrients influence the risk for AD and severity of symptoms. This systematic review discusses evidence on how various micronutrients, including vitamins (C, E, and D) and trace minerals (zinc, selenium, iron, copper, magnesium, and strontium) are associated with AD, and how supplementation influence disease severity.
Design:
A systematic search was conducted to identify the role that oral micronutrients have on AD. The authors reviewed 49 studies herein.
Results:
While there are weak associations between vitamins C or E and AD, there is sufficient evidence to suggest that vitamin D supplementation provides benefit in AD patients. Deficiency of selenium and zinc may exacerbate AD. Current reports are not sufficient to confidently discern the role of other vitamins and trace minerals on AD.
Conclusions:
Though oral micronutrients may play a role in AD, the current literature is limited, and there is a need for more comprehensive randomized controlled trials (RCTs) to truly decipher the role between oral micronutrients and AD.
Introduction
Atopic dermatitis (AD) is a chronic inflammatory skin condition involving complex interactions between immunologic, hereditary, and environmental influences. 1 Over the last 30 years, the prevalence of AD has risen globally, affecting ∼20% of children and 3% of adults worldwide. 2 Proper nutrition, especially adequate intake of vitamins, minerals, and elements, plays an active role in immune health. 3 The relationship between nutrition and AD pathogenesis has been debated for many years. 4
The influence of macronutrients has been widely studied, especially in food allergies and elimination diets; however, less attention has been paid to the role that micronutrients imparts on patients with AD. 5,6 This systematic review discusses the associations among AD and various micronutrients, including vitamins C, E, and D, zinc, copper, iron, selenium, magnesium, and strontium. Evidence discussed includes investigations of blood and hair levels of micronutrients and risk for developing AD, as well as the role of oral supplementation for AD management.
Methods
A systematic search was conducted on PubMed and EMBASE electronic databases for articles from January 1, 1946, to December 10, 2018. Search terms included “vitamin C,” “vitamin D,” “vitamin E,” “vitamin,” “magnesium,” “trace elements,” “atopic dermatitis,” “eczema,” and “atopic eczema.”
Studies were selected based on the following inclusion criteria: clinical trials, published in English, vitamin or trace element as the main agent being evaluated, and the effects of supplementation on AD. Studies that evaluated the association between AD in children and/or adults and the various micronutrients or trace elements were selected. In addition, studies that investigated the role of oral supplementation in AD prevention and management were included. Literature that was non-English, review articles, animal studies, and in vitro experiments were excluded. Three authors independently reviewed the studies for eligibility. A total of 49 randomized controlled trials (RCTs), clinical trials, cohort studies, and case reports were selected, which meet the inclusion and exclusion criteria for this systematic review (Fig. 1).
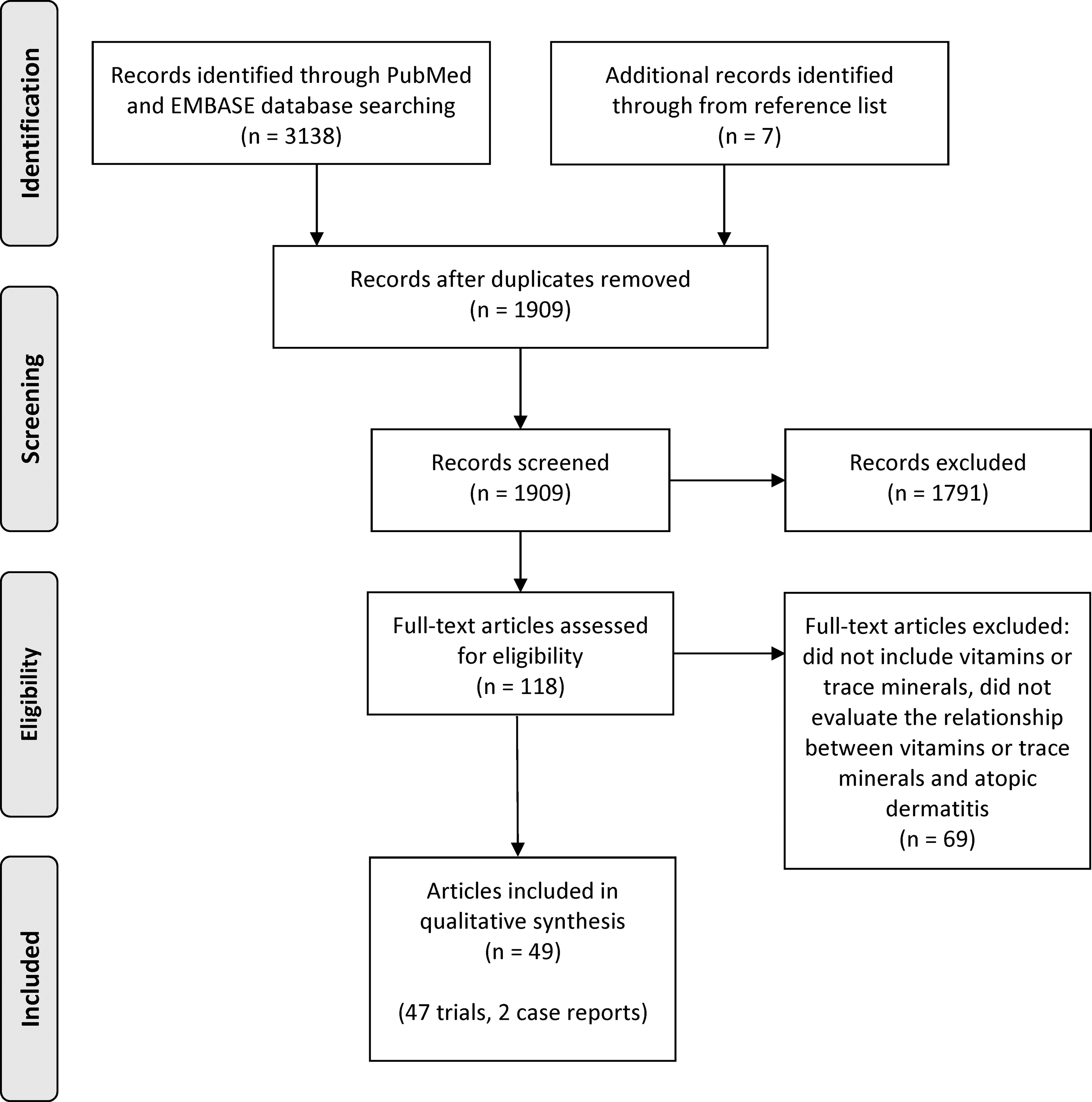
PRISMA flow diagram.
Results
Vitamins
Vitamin C
Vitamin C status and oxidative stress
Vitamin C, also known as ascorbic acid (AA), is a water-soluble vitamin with antioxidant properties that neutralizes reactive oxygen species (ROS), thus reducing oxidative damage to cells and tissues. 7,8 Vitamin C aids in the synthesis of ceramides in the epidermis, a major building block of the epidermal lipid barrier. Emerging evidence has shown that oxidative stress may play an important role in the pathogenesis of AD. 9 In fact, urine and serum markers of oxidative stress were shown to be higher in children with AD than healthy children. 1,9 In a pilot study by Sivaranjani et al. involving 25 adults with and without AD, those with AD had significantly lower serum vitamin C levels compared to healthy controls (1.33 mg% vs. 0.63 mg%, respectively; p = 0.001), suggesting that AD patients may have lower oxidative repair ability. 10 In a study involving 17 adults with AD, Shin et al. reported a significant inverse association between serum vitamin C levels and the Scoring of Atopic Dermatitis (SCORAD) score in all patients (r = −0.512, p = 0.035). In addition, plasma vitamin C positively correlated with epidermal ceramide levels. 11
Vitamin C and breast milk
It is well known that infants from atopic mothers are at an increased risk for developing atopic diseases. 12 To further understand this association, Hoppu et al. analyzed breast milk in 34 mothers to measure the antioxidant composition based on vitamins C and vitamin E levels. A higher breast milk vitamin C concentration was associated with reduced risk of atopy in infants (p = 0.038), further supporting the notion that vitamin C may prevent atopy. 12
Dietary vitamin C intake
A few studies have investigated the role of vitamin C intake in AD risk and severity. 13 –16 In a prospective follow-up study by Laitinen et al., 13 159 children with a positive family history of AD, who had participated in a previous allergy prevention study, 17,18 were evaluated from birth to 4 years of age, and the authors reported that a higher dietary vitamin C intake correlated with the development of AD, suggesting vitamin C intake increases the risk for AD in offspring. 13 In a prospective questionnaire-based study of 1924 infants and their mothers, a weak, but positive, association between AD during the second year of life and maternal dietary vitamin C intake during pregnancy was found. 14 In contrast, in two separate studies investigating the association between vitamin C and AD in children, no significant correlations between dietary vitamin C intake, plasma vitamin C levels, and risk for AD were found. 15,16 Thus, based on the available literature, there are conflicting data on the effect of dietary vitamin C intake, vitamin C levels in breast milk, serum vitamin C levels in infants, and risk for the development of AD in children.
Vitamin E
Vitamin E, or tocopherol, includes a group of fat-soluble vitamins with strong antioxidant and anti-inflammatory properties. There are four types of vitamin E: α, β, δ, and γ. 19 Vitamin E impedes synthesis and release of prostaglandins, and supplementation has been shown to decrease serum IgE in AD patients. 20 –22 In an RCT involving 70 adults with mild-to-moderate AD, oral vitamin E (400 IU/day for 4 months) significantly improved itching, lesion extent, and SCORAD index, compared to placebo (p < 0.05). 20 Improvement was sustained after 3 months of discontinuing supplementation. The authors concluded that low-dose vitamin E supplementation is an effective adjunctive therapy for AD. 20 In a separate single-blinded RCT by Tsoureli-Nikita et al., 96 AD patients were supplemented orally with vitamin E (400 IU/day) or placebo for 8 months. 22 Nearly 50% of the patients in the vitamin E group had a significant improvement in AD symptoms. Among the same group, there was a notable decrease in serum IgE after 8 months of supplementation, although the authors did not mention whether these differences were statistically significant. In a food-questionnaire study by Oh et al. involving 180 children with AD and 242 non-AD children, those without AD had a significantly higher dietary vitamin E intake (p = 0.0377), suggesting that higher intake of foods containing vitamin E may be protective against AD. 15 In a separate prospective questionnaire-based study following infants and their mothers, the investigators detected a significant association between vitamin E intake by atopic mothers during pregnancy and a reduced risk of eczema in their offspring (p = 0.024). 15 However, results from questionnaire-based study designs are limited by recall bias. In a prospective study involving 34 pregnant women, serum γ-tocopherol levels as well as serum α- and γ-tocopherol to fat ratios were significantly correlated in mothers and their infants (p = 0.008, p = 0.004, and p < 0.0001, respectively). 23 However, serum tocopherol levels were similar between the infants with and without AD, which suggest that tocopherol levels may not contribute significantly to the development of AD. 23 It is unclear why similar serum tocopherol levels were observed among infants born of mothers with and without atopy in this study, although vitamin E likely plays a protective role in AD.
Vitamin D
Vitamin D status
Vitamin D is a fat-soluble vitamin responsible for regulating serum calcium, magnesium, and phosphate levels. Studies have suggested serum vitamin D levels at 40–60 ng/mL for proper immune function. 24 Its role in AD lies in its widespread effects on immune reactivity and skin barrier integrity. 25,26 A large number of trials in both adults and children have assessed the link between serum blood vitamin D, cord blood vitamin D, as well as dietary vitamin D intake, on risk for developing AD. Significant correlations have been reported among umbilical cord blood vitamin and mineral contents, including vitamin D, and nutrient status of both mother and infant. 27 Multiple studies have found a significant association between vitamin D deficiency and an increased risk for AD development and severity. 28 –31 Eight separate studies in children have found that higher vitamin D levels are significantly associated with decreased AD severity and SCORAD. 32 –39 One study did not report lower serum vitamin D concentrations in children with AD, but found that greater AD severity correlated significantly with lower vitamin D levels (p < 0.05). 40
Vitamin D supplementation
Several RCTs have evaluated the effects of vitamin D supplementation on children and adults with AD. 41 –46 Five RCTs, one cross-sectional study, one case–control study, and one case study reported that vitamin D supplementation had beneficial outcomes on symptom severity in both children and adults. 32,41,43,45 –49 In an RCT study by Sidbury et al., 80% of AD patients supplemented with ergocalciferol (vitamin D2) at 1000 IU daily had improved investigator's global assessment (IGA) score of one point after just 1 month (p = 0.04). 45 In an RCT study by Camargo et al., involving 107 children with AD, daily vitamin D3 supplementation (1000 IU for 1 month) led to significantly greater improvements in the Eczema Area and Severity Index (EASI) (p = 0.02) and IGA scores (p = 0.03) compared to placebo. 41 In a separate RCT involving 60 children with AD, daily vitamin D3 (1600 IU) supplementation resulted in significant improvement in SCORAD and three item severity scores compared to the control group after 60 days (p < 0.05). 46 In a similar 60-day RCT study on both adults and children, supplementation of vitamin D, vitamin E, vitamin D and E, or placebo in 45 patients resulted in a significant negative effect between plasma vitamin E level and SCORAD. No correlation was found between SCORAD and vitamin D. Subjects who received both vitamin D and E had the greatest SCORAD reduction (64.3% improvement in combined supplementation vs. 34.5% in vitamin D only and 35.7% in vitamin E only; p = 0.04), suggesting potential synergistic effects. 43 In an RCT study involving 65 children and adults supplemented with either 5000 IU/day of D3 or placebo for 3 months, there was a lower SCORAD if serum levels of 25(OH)D ≥20 ng/mL (p = 0.03), regardless of randomization group, suggesting no impact of vitamin D on lessening SCORAD. 48
A cross-sectional study evaluated the relationship between vitamin D levels and SCORAD in 153 adults with and without AD, and the effects of 2000 IU/day of 25(OH)D3 in a subset of 20 adults with AD for 3 months. 32 While a significant reduction in SCORAD occurred in those supplemented with vitamin D (p < 0.001), differences in serum vitamin D were not seen between the two cohorts, suggesting external factors such as living in an urban environment have a greater impact on serum vitamin D. In one case–control study, 50 children with and without AD were evaluated, and a subset of AD subjects was supplemented with 500 IU/day of cholecalciferol drops for 1 month. 49 Serum vitamin D levels were significantly lower in the AD group (p < 0.001), an inverse relationship was reported between serum vitamin D and SCORAD (p < 0.001), and there was a significant reduction in SCORAD after supplementation with vitamin D (p = 0.05). This may suggest that supplementation with vitamin D can positively influence the severity of AD. A singular case report of an 8-year-old female with AD (SCORAD 70) was supplemented with 0.5 mcg × 3/day calcitriol (D3) and 4000 IU/day cholecalciferol orally for 6 months with a sevenfold decrease in SCORAD. 47 This substantial improvement supports the need for studies assessing the role of increased oral cholecalciferol supplementation. Hypercalcemia, hypercalciuria, weakness, and fatigue are some of the known toxic effects associated with excess vitamin D supplementation when serum level reaches above 100–150 ng/mL, although the daily dose limit before reaching toxicity is yet to be determined. 50 Despite significant associations detected between vitamin D status and supplementation in AD patients mentioned above, Hata et al. found no effect of vitamin D supplementation (4000 IU vitamin D3 or placebo for 21 days) on AD severity from baseline in 60 adults with and without AD. 42
Maternal vitamin D status and AD risk
The risk of developing AD was identified through correlation of maternal vitamin D blood levels during pregnancy and serum levels in offspring. Jones et al. analyzed cord blood in a group of infants with at least one parent who had a history of allergic disease, 51 and found a significant association between low cord blood vitamin D concentration and increased risk for infantile AD at age 1. The authors hypothesized that lower vitamin D exposure in utero may increase the risk for developing AD. 51 Chiu et al. suggested that a lower blood level of vitamin D during early childhood increases the likelihood of developing AD. 52 In this study, children who were born to mothers deficient in vitamin D had significantly lower levels of vitamin D than children who were born to mothers with normal vitamin D levels. 52 In addition, two separate studies concluded that sufficient vitamin D levels in cord blood were significantly associated with a lower risk for eczema in offspring. 52,53 Conversely, three other studies concluded that maternal serum vitamin D concentrations during pregnancy did not significantly correlate with risk for AD in offspring. 54 –56 Based on available evidence, it remains unclear whether maternal vitamin D blood level is directly associated with AD, and whether high or low serum levels contribute to the incidence of AD in infants and children.
Two separate studies reported a significant positive correlation between maternal dietary vitamin D intake during pregnancy and infantile AD. 57,58 In contrast, three other studies found no significant correlation between maternal vitamin D intake during pregnancy and risk for AD in their offspring. 59 Two studies reported that higher dietary vitamin D intake by children actually increases their risk for developing AD. 60,61 A cross-sectional and prospective cohort study among 644 children did not find an association between vitamin D levels and the presence or severity of atopic eczema in the first 2 years of life. 62 In summary, there is conflicting evidence on the association between maternal vitamin D status and risk for offspring to develop AD. However, overall evidence exists to support a protective role of vitamin D in AD.
Trace minerals
A large variety of trace minerals are essential for cellular processes throughout the body, including cell turnover, cell metabolism, and apoptosis. Several studies have investigated connections between AD and various minerals, including zinc, copper, iron, and magnesium.
Zinc
Zinc serves as a cofactor in cell growth, proliferation, and regeneration. 3,63 Zinc possesses anti-inflammatory properties and supplementation has been shown to suppress inflammatory cytokine production. 64 Although a definitive link between zinc deficiency and AD remains unclear, it appears to play a role in the disease process. 63
Both genetic and acquired zinc deficiency can lead to a skin condition called acrodermatitis enteropathica, which can be morphologically similar to AD-like eruptions. 65 In a study by David et al., involving 65 children with AD and 79 without AD, those with AD had significantly lower serum zinc concentrations than healthy controls (p < 0.0001). 66 Due to a skewed age distribution between the two groups (with over 57% of children in the AD group being younger than 3), a subanalysis was conducted, excluding patients less younger than 3, confirming the initial finding that AD children had lower serum zinc levels than healthy ones (p = 0.0002). No significant correlation was found between the serum zinc concentration and either the severity of AD or height/weight percentile. 66
Karabacak et al. conducted a similar investigation involving 67 AD patients and 49 healthy controls (mean age 17.9 years old) using serum zinc and erythrocyte zinc (EZ) levels (a measure of nutritional zinc status), 3 and found that AD patients had significantly lower mean EZ levels than healthy controls (34.4 μg/g vs. 40.4 μg/g hemoglobin, respectively; p < 0.001). There was a strong negative correlation between SCORAD and EZ levels (r = −0.791, p < 0.001). When subjects were stratified based on AD severity, those with severe AD had the lowest EZ levels. Interestingly, although there were significant differences in EZ levels, no significant differences were seen in the serum zinc levels between the two groups. 3 It remains unclear whether serum or EZ level is a more accurate assessment of nutritional zinc status.
Zinc and copper
Zinc and copper are both known to play a role in cell and tissue growth and function as cofactors in many enzyme systems. 67 Hair mineral concentration has been used as a surrogate measure for relative levels of trace elements in the body. 63 Kim et al. reported that hair zinc levels in children with mild-to-moderate AD were significantly lower than hair zinc levels of healthy controls (113.1 μg/g vs. 130.9 μg/g, p = 0.012). Due to limitations with standardization of reference ranges with hair mineral analysis, other outcome measures such as blood should be utilized. 68
Although the mechanism remains unclear, serum copper levels have been investigated in a number of studies involving allergic diseases, such as AD and asthma. 69 –71 A study by el-Kholy et al. found that children with AD and/or asthma have higher serum IgE and ceruloplasmin levels compared to the healthy controls (p < 0.001). Compared to healthy controls, AD children had lower serum and hair zinc levels (p < 0.001), whereas asthmatic children had higher serum and hair copper content (p < 0.001). 67
In a similar study, Di Toro et al. reported that hair zinc content was significantly lower in AD patients compared to control group (p < 0.05), but hair copper levels were significantly greater than the healthy children (p < 0.05). 69 In accordance with the previous study by el-Kholy et al., the investigators concluded that nutrient intake for allergic children, particularly zinc, should be monitored to ensure that any trace element deficiency is addressed. 69 Based on the results of these studies, it appears that hair and serum copper levels are positively correlated with atopic risk, whereas zinc levels appear to be inversely correlated with atopic risk. However, the interplay between zinc, copper, and AD remains unclear.
Zinc supplementation
In a parallel, randomized, double-blind, placebo-controlled study involving 50 children (ages 1–16 years) with AD, those who were supplemented with zinc sulfate (61.8 mg thrice daily for 8 weeks) or placebo did not differ in clinical severity score or the need for topical or oral medications (emollients, topical steroids, or trimeprazine). 72
In the aforementioned study by Kim et al., when AD children with low baseline hair zinc levels were supplemented with either oral zinc oxide tablets (12 mg zinc per day as Zn-TZA plus®) along with oral antihistamines and moisturizers, or oral antihistamines and moisturizers alone for a period of 8 weeks, those who received oral zinc had significantly increased hair zinc levels after 8 weeks compared to baseline (p < 0.001). 63 In addition, the oral zinc group had an improvement in EASI and a decrease in transepidermal water loss (p = 0.015), whereas the nonsupplemented group had a decline in EASI. Compared to baseline, the oral zinc group also had significantly higher hair zinc levels than the nonsupplemented group at weeks 4 and 8 (p = 0.013 and p = 0.044, respectively), and a significant decrease in the visual analogue scale at week 8 (p < 0.001) compared to baseline, indicating a decrease in sleep disturbance and pruritus. Zinc supplementation was well tolerated. The authors suggested that zinc levels should be monitored as part of AD management. 63
In a case report by Sugiura et al., a 2-year-old boy presented with signs of developmental delay, skin atrophy, and brittle hair after receiving high-dose zinc gluconate supplementation for 6 months (314 mg/day, equivalent of 45 mg/day elemental zinc, which is over 12 times the recommended daily dose for his age group 73 ) as part of his AD treatment. 74 His AD improved with ultra-high-dose zinc supplementation. Skin atrophy and brittle hair resolved 1 month after discontinuing zinc supplementation. However, his neurologic development did not improve, which the authors believed may have been caused by high zinc supplementation. The authors suggest that periodic monitoring and careful caution should be exercised when supplementing patients with zinc, especially in children still undergoing neurological development. 74 Altogether, significantly lower serum zinc and EZ have been detected in children and adults with AD, respectively. However, zinc supplementation in children does not appear to improve clinical severity or reduce the need for oral and topical medications to control symptoms. Foremost, carefully designed studies are needed to establish safe and effective zinc dosing to better understand if supplementation improves AD severity. It is important to note that nausea and gastrointestinal distress are very common with zinc supplementation, severely limiting its use.
In the lumen of the intestine, zinc may interact with the uptake of copper. 75 Zinc may interfere with intestinal absorption of copper. 75 Chronic high-dose zinc supplementation can lead to copper deficiency. Therefore, zinc should be supplemented with copper at a ratio of ∼10:1.
Iron
Free iron in the blood can lead to production of ROS through a mechanism called the Fenton reaction, increasing oxidative stress within cells. 76 There is a delicate balance between iron homeostasis, AA, and ROS levels in the skin. It is thought that skin inflammatory responses can trigger “catalytic iron” to be released from its stored form and perpetuate the production of ROS leading to further damage, which necessitates the need for antioxidant compounds such as AA. 77
Several studies have sought to understand the association between blood and skin-free iron and AA levels, and AD symptoms. Leveque et al. compared dermal and serum iron and AA concentrations in a cohort of five AD patients and five healthy controls, and found that the AD patients had significantly lower mean dermal AA concentration (46.7 ± 0.6 μg/mL vs. 176.8 ± 14.5 μg/mL, respectively; p < 0.05) and higher mean dermal iron concentration (44.3 ± 4.6 μg/L vs. 21.8 ± 1.2 μg/L; p < 0.05). There were no significant differences in iron or AA levels in the serum between the two groups. 78 The finding suggests that dermal iron and AA levels may serve as useful diagnostic, prognostic, and therapeutic markers in inflammatory skin diseases. The authors also postulated that insufficient antioxidant activity is one key factor in AD pathogenesis. 78 It has been proposed that storage proteins release “catalytic iron” during inflammation leading to more ROS, and there may be a close relationship between ROS in the skin and iron concentration. 77
David et al. examined a possible relationship between the serum concentration of three trace metals (zinc, copper, and iron) among 134 children with AD and 112 healthy children, and found that AD children had significantly higher serum copper and orosomucoid (an acute phase reactant) levels (p < 0.001) and lower serum ferritin (a measure of iron status) levels, compared to healthy infants at 1 and 10 months of age (p = 0.0003). 79 There was no significant difference between the serum concentrations of zinc and iron between the two groups. 79 The authors suggested that AD patients likely have depleted body iron stores, reflected by the low serum ferritin.
Selenium
Selenium functions as a cofactor at the active site of glutathione peroxidase, an antioxidative enzyme present in numerous cell types. Thus, it is plausible that sufficient selenium is necessary to ensure optimal antioxidative capacity of skin cells, as increased oxidative stress has been reported in AD and other inflammatory skin diseases. 80 Selenium-enriched yeast has been shown to have enhanced bioavailability and antioxidant capacity compared to other forms of selenium, such as selenomethionine. 81 In a double-blinded RCT by Fairris et al., 60 adults with AD were randomized into 1 of 3 groups: selenium-enriched yeast plus vitamin E supplementation, selenium-enriched yeast supplementation alone, or placebo. Supplementation with selenium-enriched yeast (600 μg) plus vitamin E (600 IU) each daily for 12 weeks led to a significantly increased blood selenium concentration compared to baseline. Those who received selenium-enriched yeast alone or placebo had no significant changes in blood selenium levels from baseline after 12 weeks. 82 No significant changes in cutaneous selenium content or AD severity were observed in any of the three groups. There is a need for more clinical studies to establish the utility of selenium supplementation to improve AD.
Selenium and strontium
In a prospective cohort study by Yamada et al., hair mineral content of a random sample of 834 mother-infant pairs was analyzed by Proton-induced X-ray emission to evaluate the relationship between AD and 32 different hair minerals. 83 Hair selenium and strontium contents were significantly higher in the infants who developed AD compared to those who did not at 10 months of age (p = 0.048 and p = 0.023, respectively). Furthermore, selenium deficiency in either the infant or mother was associated with an increased relative risk of 4.2% for the development of AD in the infant. Interestingly, infant strontium deficiency was associated with an increased risk of developing AD, while maternal strontium deficiency was associated with a decreased risk of developing AD. 83
Magnesium
Magnesium plays a role in cell proliferation and differentiation, and magnesium deficiency is associated with an exaggerated inflammatory response. 84,85 In 1963, Lipkin et al. reported that whole skin and dermal magnesium levels were significantly higher in adults with AD compared to healthy controls (1.5 ± 0.4 vs. 0.9 ± 0.4, respectively; p < 0.01), while epidermal magnesium content was not significantly different between the two groups. 86 The authors commented that it was difficult to draw conclusions since water content was not accounted for before wet washing of tissue and spectrographic analysis.
Toyran et al. measured the serum concentrations of iron, magnesium, and copper and EZ levels in 92 children with AD and 70 healthy controls. 71 AD patients had significantly lower serum magnesium and EZ levels compared to controls (p = 0.007 and p < 0.001, respectively). Iron and copper serum concentrations were not significantly different between the two groups. The investigators did not find a correlation between SCORAD and the serum concentrations of copper, iron, and magnesium, and EZ levels. This study hinted at the relationship between the serum levels of zinc and magnesium, and the potential roles they play in the pathogenesis of AD, although mechanisms have not been elucidated. 71
Discussion
Research on the role that micronutrients play in AD is limited and conflicting in some cases (Table 1). With regard to the relationship between vitamins and AD, there appears to be a weak association between vitamins C or E and AD. Very few studies evaluated the relationship between vitamin E and AD. 14,15,23,87 –89 Current findings appear to be more consistent and suggestive of a negative correlation between vitamin E status and risk for the development of AD.
Summary of Evidence for the Role of Oral Micronutrients in Atopic Dermatitis
AA, ascorbic acid; AD, atopic dermatitis; EASI, Eczema Area and Severity Index; EZ, erythrocyte zinc; IGA, investigator's global assessment; SCORAD, Scoring of Atopic Dermatitis; TEWL, transepidermal water loss; TIS, three item severity; VAS, visual analog score.
There are a vast number of studies on the role of vitamin D in AD. While there are only a few RCTs, most of the current studies evaluated the relationship between cord blood or serum vitamin D and AD. Most RCTs found that vitamin D supplementation provided a beneficial outcome in AD prevalence and symptom severity. Seven studies assessed whether there was a correlation between umbilical cord blood, specifically vitamin D levels, and AD incidence. There is a need for more studies on cord blood and AD incidence before a conclusion can be reached. Current evidence regarding serum vitamin D and AD status remains inconclusive.
Based on the available literature, current evidence supports the role of zinc in improving AD. 63,74 A majority of studies on zinc reported that AD patients had lower hair, serum, and EZ zinc levels. 3,66,67,69 However, at least one study reported that zinc did not appear to play a role in AD. 72 A few studies hypothesize that selenium deficiency may increase the risk for AD. 82,83 A significant association between strontium deficiency in infants and increased risk for AD was reported. However, there was a decreased risk for AD in association with maternal strontium deficiency, necessitating the need for further research to understand this correlation. There is a need for more research investigating iron, since this trace element had a role in inflammatory processes as well as potentially harmful fetal exposure to iron from cord blood. 78,90 A distinct association between AD, copper, and iron still cannot be made. 67,79
There are several limitations in the research of micronutrients' role on AD. First, there are a small number of available studies regarding the levels of trace minerals and vitamins among the AD population. Although there is a correlation in the serum levels of trace minerals and vitamins with the presence of AD, an extrapolation on the role of these micronutrients on the cellular levels is difficult. There is intricate interplay between the immune system, cellular function, and vitamins and minerals; the isolated effect of a single or few compounds is difficult to conclude. However, in the studies that did evaluate trace minerals, the study sample sizes were small, making it difficult to obtain significant results. Interventional studies examining whether supplementation influences serum levels of micronutrients and AD severity are difficult to standardize due to confounding variables, heterogeneity of study populations (age, disease severity), and lack of adequate control. Studies utilizing questionnaires to assess dietary intake impose a significant risk for recall bias.
Adding to the complexity of micronutrient investigation is the concept of nutrigenomics: nutrition's influence on gene expression, which in turn affects how the body responds to specific nutrients. Each study participant likely has distinct responses to micronutrient supplementation. Various formulations of vitamins and minerals, such as zinc gluconate versus zinc sulfate, and different supplementation regimens can also significantly influence study results, which limit cross comparison across different studies. In addition, since FDA regulation of supplements (including vitamins and trace minerals) differ from regulation of prescription and over-the-counter medications, variabilities are present in the quality control and assurance. Overall, there is a need for more comprehensive randomized controlled studies involving larger populations to decipher the relationship between micronutrients and AD.
Footnotes
Acknowledgment
No funding source was received for the preparation of this article.
Author Disclosure Statement
V.Y.S. has stock options for Dermveda, and served as an advisor for Pfizer, Sanofi, Novartis, SUN, Menlo Therapeutics, Burt's Bees, GpSkin, BSN Medical, The National Eczema Association, and Global Parents for Eczema Research Group. V.Y.S. has served as an investigator for AbbVie and LeoPharma, and has received research funding from Skin Active Scientific and the Atopic Dermatitis Foundation. A.R.V., N.F., M.M., and K.A.T. have no conflicts of interest to report.