
Abstract
Objective:
Toutongning (TTN) capsule, a Chinese patent medicine, is used as a prophylactic treatment for migraine. The present study was conducted as a postmarketing evaluation of the efficacy and safety of TTN capsule.
Design:
A randomized, double-blind, placebo-controlled trial.
Location:
Patients recruited from 14 medical centers in China from May 2014 to August 2015.
Subjects:
Patients between 18 and 65 years of age with a diagnosis of migraine.
Interventions:
The patients were randomly assigned to receive either TTN (1200 mg, three times daily) or a matched placebo (1:1) for 4 weeks.
Outcome measures:
The primary outcome measured was a minimum 50% reduction in the frequency of headaches from the 4-week baseline period to the last 4 weeks of the 12-week trial. Secondary outcomes included duration, days, and visual analog score of headache attack, interval between headache attacks, usage of acute analgesics, and score on the Headache Impact Test-6. In addition, all patients were evaluated for adverse events (AEs).
Results:
This study initially enrolled 400 patients; a total of 378 participants completed the experiment while fulfilling all study requirements. TTN had a superior effect compared with the placebo on both the primary and secondary outcome measures without any serious AEs or unexpected side effects.
Conclusion:
TTN can effectively prevent the occurrence of migraine headaches and is well-tolerated and safe. TTN may exhibit a persistent therapeutic effect even after cessation of use. Trial Registration number: ChiCTR-IPR-15007058.
Introduction
Migraine is a very common and disabling brain disorder. In the 2016 Global Burden of Disease Survey, migraine ranked as the second leading cause of years lived with disabilities (YLDs). 1 In China, the prevalence of migraine in adults from 18 to 65 years of age is ∼9.3%. 2 Worldwide, migraine is the leading cause of YLDs in the age group 15–49 years. 3 The precise pathogenesis of migraine is not clearly understood, 4 which compounds the difficulty of developing effective antimigraine agents.
Current acute migraine treatments comprise two categories: nonspecific agents, including analgesics, and nonsteroidal anti-inflammatory drugs (NSAIDs); and relatively specific agents, such as ergot alkaloids and triptans. 5 The gastrointestinal side effects of NSAIDs, potential for opioid addiction, and the risk of medication overuse for all acute treatment agents often limit their use. 5,6 Patients refractory to acute therapy or with a high frequency of attacks require prophylactic treatment, 7 which helps prevent chronicity and medication overuse. 8 The main prophylactic pharmacological agents include antidepressants, antiepileptics, β-adrenergic receptor blockers, antihistamines, calcium ion channel antagonists, botulinum toxin A, progestogen, and nutraceuticals. 9,10 None of these agents is specific for migraine treatment.
Toutongning (TTN) capsule, a Chinese patent medicine, is used as a prophylactic treatment for migraine, and has been approved by the State Food and Drug Administration of China (authorized document number: Z20026851). It takes rhizome Gastrodia 0.27 g, Rhizoma Smilacis Glabrae 0.36 g, prepared Radix polygoni multiflori 0.27 g, angelica sinensis 0.18 g, Saposhnikovia divaricata 0.18 g, and scorpion 0.03 g to make one capsule. Several studies have demonstrated TTN's efficacy as a treatment for migraines induced by various mechanisms: inhibition of peripheral blood levels of calcitonin gene-related peptide 11 ; restricting dural blood flow with electrically stimulated trigeminal ganglia; changing blood platelet and hemorheological parameters in patients with migraine 12 ; reducing the expression of c-fos and c-jun 13 ; upregulating substance P mRNA expression in the midbrain 14 ; downregulating the protein expression of brain-derived neurotrophic factor, tyrosine kinase receptor B, extracellular signal-regulated kinase, and phosphorylating cyclic adenosine monophosphate-response element binding protein 15 ; and reducing levels of plasma lysophosphatidic acid and acidic phospholipids in rats receiving subcutaneous injections of nitroglycerin. 16 Nie et al. found that TTN reduced migraine via regulation of the tumor necrosis factor signaling pathway. 17
Although the TTN capsule has been widely used in clinical practice in China as a prophylactic migraine treatment, evidence-based postmarketing evaluation of the efficacy and safety of the TTN capsule is still lacking. The present randomized, double-blind, placebo-controlled trial reevaluated the efficacy of TTN capsules. The International Headache Society Clinical Trial Guidelines define a clinically meaningful endpoint as a reduction of 50% or more in the frequency of headache attacks. 18 This trial used a primary endpoint of a minimum of 50% reduction in the frequency of headaches from the 4-week baseline period to the last 4 weeks of the 12-week trial, based on the hypothesis that TTN would provide greater relief than the placebo.
Methods
Study design and oversight
The present study was a multicenter, randomized, double-blind, placebo-controlled clinical trial that enrolled migraine patients from 14 academic centers in China. The Chinese PLA General Hospital was responsible for the design and execution of the clinical trial. The study protocol complied with the World Medical Association's Declaration of Helsinki and China's regulations and guidelines for Good Clinical Practice, and was approved by the Ethics Committee at the Chinese PLA General Hospital and the institutional review boards at each participating institution. All participants provided written informed consent. Buchang Pharmaceutical Company donated the medication and placebo used in the study, but had no other role in the research. This study was registered in the Chinese Clinical Trial Registry (ChiCTR-IPR-15007058).
Participants
Eligibility criteria included a diagnosis of migraine with or without aura according to the International Classification of Headache Disorders, 3rd edition, beta version (ICHD-3β) 19 ; age 18–65 years; a migraine frequency of 2–8 from a prospective headache diary during the baseline period of 4 weeks; and accurate comprehensive identification of migraine attacks and completion of the research diary.
Exclusion criteria were as follows: intake of analgesics >10 days per month due to headache attacks; serious comorbidities such as cardiovascular system disease, cerebrovascular disease, intracranial space-occupying lesions, traumatic brain injury, and/or gastrointestinal, renal, hepatic, hematologic, respiratory, or endocrine disease; combined with other primary or secondary headache; the presence of alcohol or other drug abuse; and pregnant or lactating women or those planning to become pregnant.
Interventions
The study included three phases, each of which lasted for 4 weeks: baseline, treatment, and follow-up. During the baseline period, all patients were treated with an oral placebo that was identical in appearance to the TTN capsule (TTN simulation medicinal preparation) and received health education. After the baseline period, eligible patients were randomly assigned in a 1:1 ratio to receive TTN (1200 mg) or a placebo three times daily for 4 weeks. Investigators ceased drug treatment for patients who experienced severe adverse events (AEs) during the trial period; these patients were monitored for safety. The 4-week treatment period was followed by a 4-week follow-up period.
Figure 1 presents a detailed flow chart of the experiment course. The randomization list was generated by an independent statistician, and each headache clinical center was supplied with kits of the study drug that were labeled with sequential numbers corresponding to the computer-generated random medication code list. Each participant was assigned a numbered kit at each center by the investigators according to the clinic sequence. Patients, caregivers, center investigators, and outcome assessors were blind to the treatment allocation and compliance was assessed by counting unused capsules remaining in the medicine bottle.
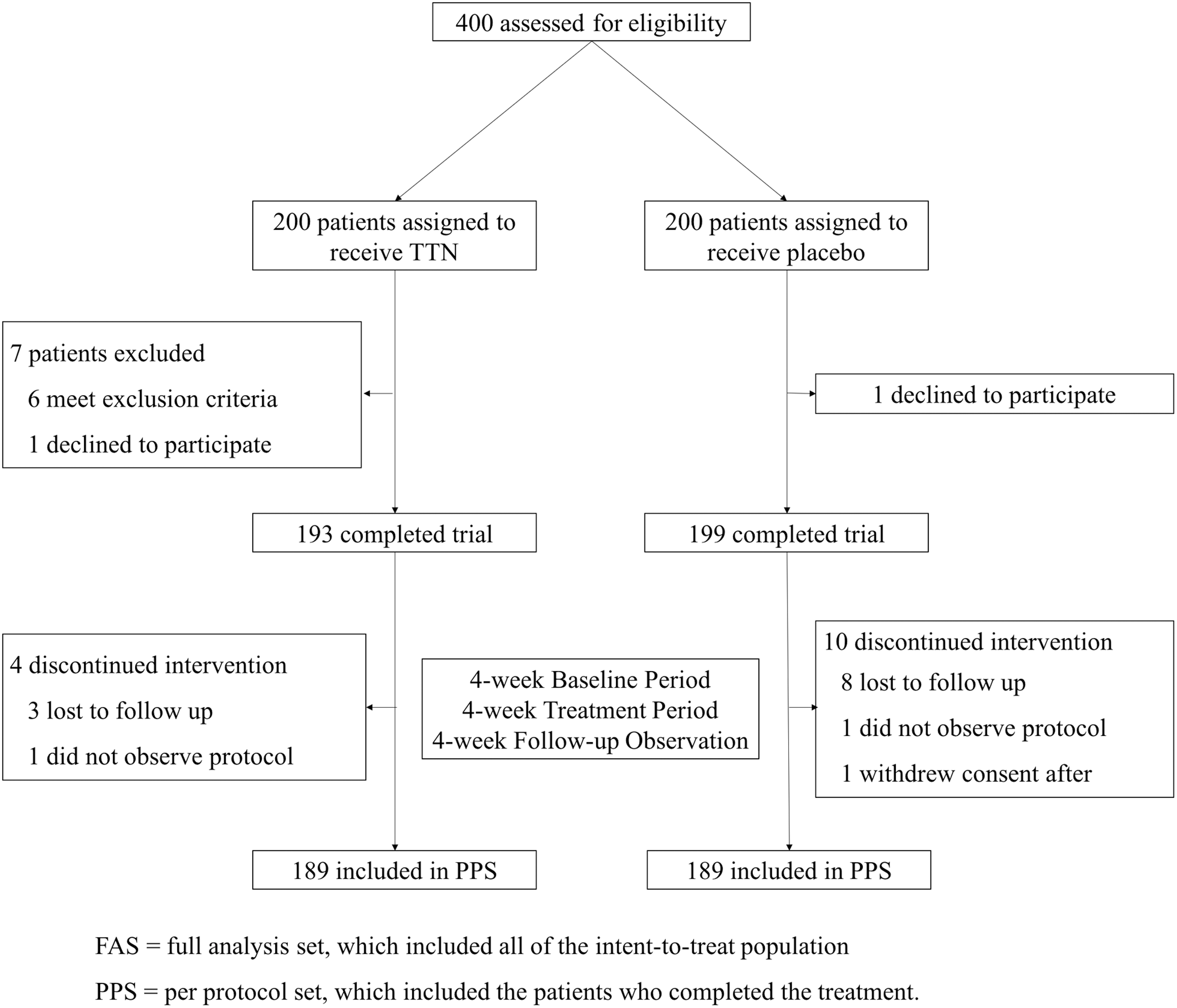
Experimental flow chart.
Outcome measures
Throughout the trial, patients recorded their headache symptoms daily using a headache diary, in conformity to the National Institute of Neurological Disorders and Stroke Common Data Elements. 20 Headache frequency was defined as the number of headache attacks per 4 weeks. The primary endpoint was a minimum of 50% reduction in the frequency of headaches from the 4-week baseline period to the last 4 weeks of the 12-week trial. Secondary outcomes included duration, days, visual analog score (VAS) of headache attack, time interval between headache attacks, usage of acute analgesics, and score on the Headache Impact Test-6 (HIT-6). The HIT-6 is a six-item self-reported questionnaire used to evaluate the severity of headache impact on patients' daily activities. 21
Safety measures in the present study consisted of physical examinations, assessments of vital signs, electrocardiography, clinical laboratory tests (hematological tests, blood chemical values, urinalysis, and stool analysis), and the recording of AEs. AEs were recorded and documented with information about the date of onset, resolution date, severity, duration, frequency, relationship to study treatment, action taken, and outcome. All interviewers and experts received uniform training regarding the standard administration of the assessment tools and diagnosis.
Statistical analyses
Sample size was calculated based on a comparison of the percentage of patients with a minimum of 50% reduction in the frequency of headaches in the TTN and placebo groups. The results of a previous study indicated that 18% of patients in the placebo group experienced a reduction of 50% or more in the frequency of headache attacks. TTN was assumed to have a positive effect if it increased the percentage by at least 30%. A total sample size of 340 subjects (170 for each treatment group) was required to detect a difference, assuming a type I error of 5% and power of test of 80%. Accounting for a follow-up loss of 20%, a total of 400 participants were required.
Analyses of the primary and secondary efficacy measures were performed on the full analysis set (FAS) and per protocol set (PPS). The FAS population consisted of all randomized patients who received at least one dose of trial medication, had a complete baseline assessment, and had at least one post-treatment assessment of the primary outcome measures; missing values were replaced using the last-observation-carried-forward method. The PPS population included patients who had primary efficacy measurements and completed the 12-week experiment as planned with no major protocol violations.
The homogeneity values of the baseline characteristics between the two groups were analyzed with Fisher's exact tests, chi-squared (χ 2 ) tests, or Cochran–Mantel–Haenszel tests for categorical measures, and t-tests or Wilcoxon rank-sum tests for continuous measures. Safety analyses were performed on a safety set that consisted of all randomized patients who had received at least one dose of the study medication and performed at least one post-treatment safety measurement. χ 2 Tests were used to analyze the incidences of AEs. All statistical analyses were performed with SAS software, version 9.3 (SAS Institute, Cary, NC) and p values ≤0.05 were considered to indicate statistical significance; all tests were two tailed.
Results
Patients
From May 2014 to August 2015, 400 eligible Chinese patients with migraine were recruited and randomized (1:1 ratio) to receive either TTN or a placebo treatment. Figure 1 summarizes the recruitment, participation, and attrition rates of the patients. All 400 randomized patients were eligible for the safety analysis and the PPS population consisted of 378 subjects (TTN: n = 189; placebo: n = 189). No significant differences were observed between the two groups in the baseline characteristics, including demographic features and laboratory examinations (Table 1). At baseline, the severity (VAS scores) and duration of the headache attacks were slightly greater and longer, respectively, in the TTN group than in the placebo group (p < 0.05), while the other baseline efficacy measures did not significantly differ (Table 2).
Baseline Characteristics of Participants
p < 0.05.
HIT-6, Headache Impact Test-6; SD, standard deviation; TTN, Toutongning.
Efficacy Measures of Participants in Baseline Period at Week Four
p < 0.05.
VAS, visual analog score.
Primary outcomes
The FAS analysis revealed that the percentage of patients with ≥50% reduction in frequency of headache attacks was 86.5% and 19% in the TTN and placebo groups, respectively, when comparing the baseline period with the last 4 weeks of the 12-week trial (Fig. 2A; Table 4). The percentage of patients with a relative reduction of ≥50% in the frequency of headache attacks was 72.5% at week 8 (Fig. 2A; Table 3). The difference in effect between the TTN group and the placebo group continued to increase, even after ceasing drug administration.
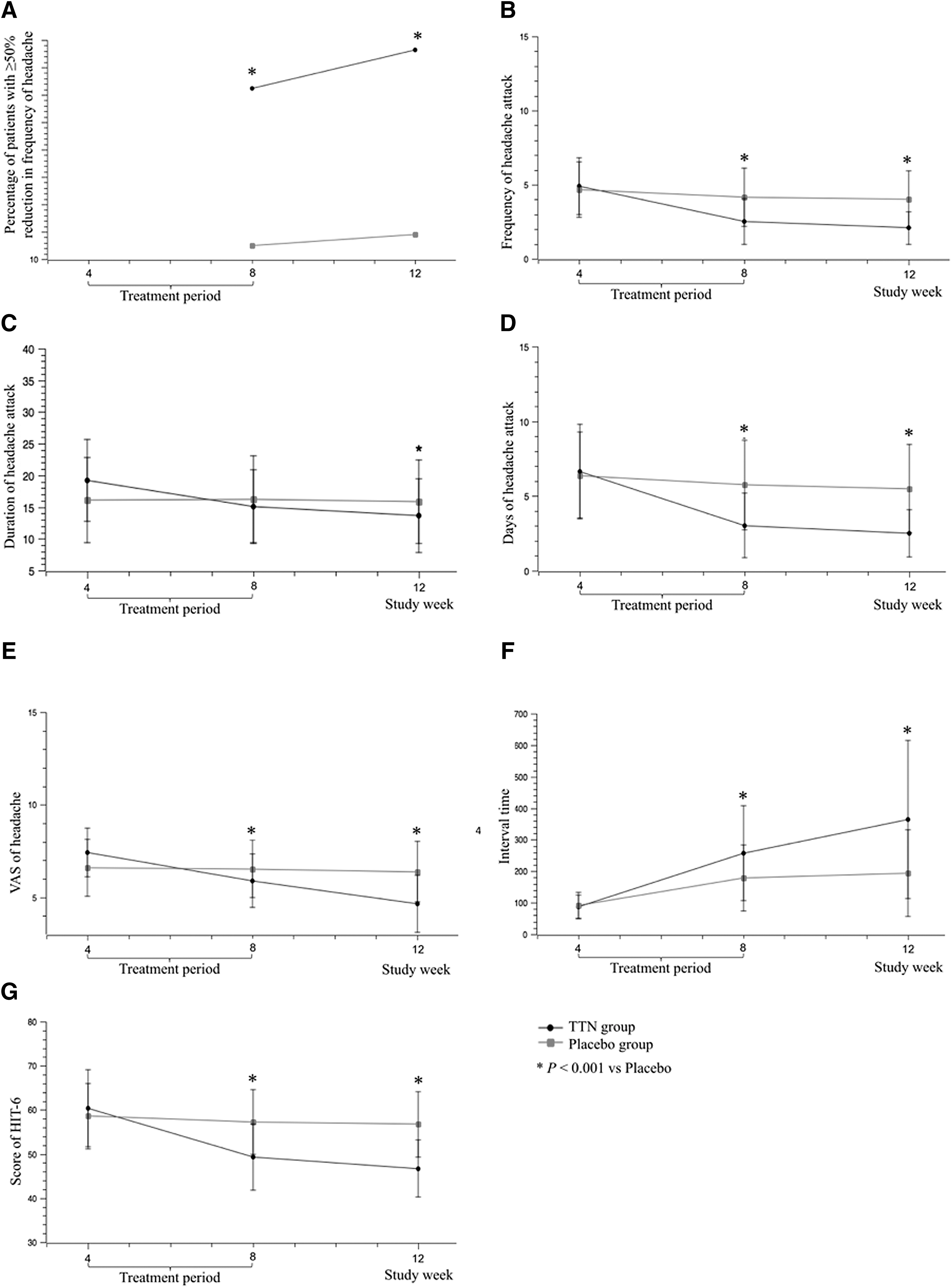
Primary and secondary outcome measures in the full analysis set.
Efficacy Measurements in Full Analysis Set Population at Week Eight
p < 0.05.
Efficacy Measurements in Full Analysis Set Population at Week Twelve
p < 0.05.
Secondary outcomes
The adjusted mean change from baseline in the frequency of headache at week 8 was 2.52 in the TTN group and 4.16 in the placebo group (TTN baseline difference: −2.37; placebo baseline difference: −0.51, p < 0.001; Table 3; Fig. 2B). The other estimated measures of headache, including the days, duration, and VAS scores of headache in the TTN group, also significantly decreased at week 8 relative to the placebo group. Although the reduction in the duration of headache was numerically greater in the TTN group, this change did not reach statistical significance compared with the placebo group at week 8 (Table 3; Fig. 2C). However, the adjusted mean change from baseline for the duration of headache decreased significantly (Table 3). Headache days decreased from 5.75 to 3.03 (p < 0.001; Table 3; Fig. 2D). The mean VAS score was 5.90 in the TTN group and 6.54 in the placebo group (p < 0.001; Table 3; Fig. 2E) at week 8. The qualitative classification of headache severity revealed marked reductions in the VAS scores (Tables 3 and 4; Fig. 3). The interval time between headache attacks increased to 257.17 and 178.95 h in the TTN and placebo groups, respectively (p < 0.001, Table 3; Fig. 2F). In addition, the HIT-6 score of the TTN group at week 8 was significantly better than that of the placebo group (49.27 vs. 57.24, p < 0.001, Table 3; Fig. 2G).
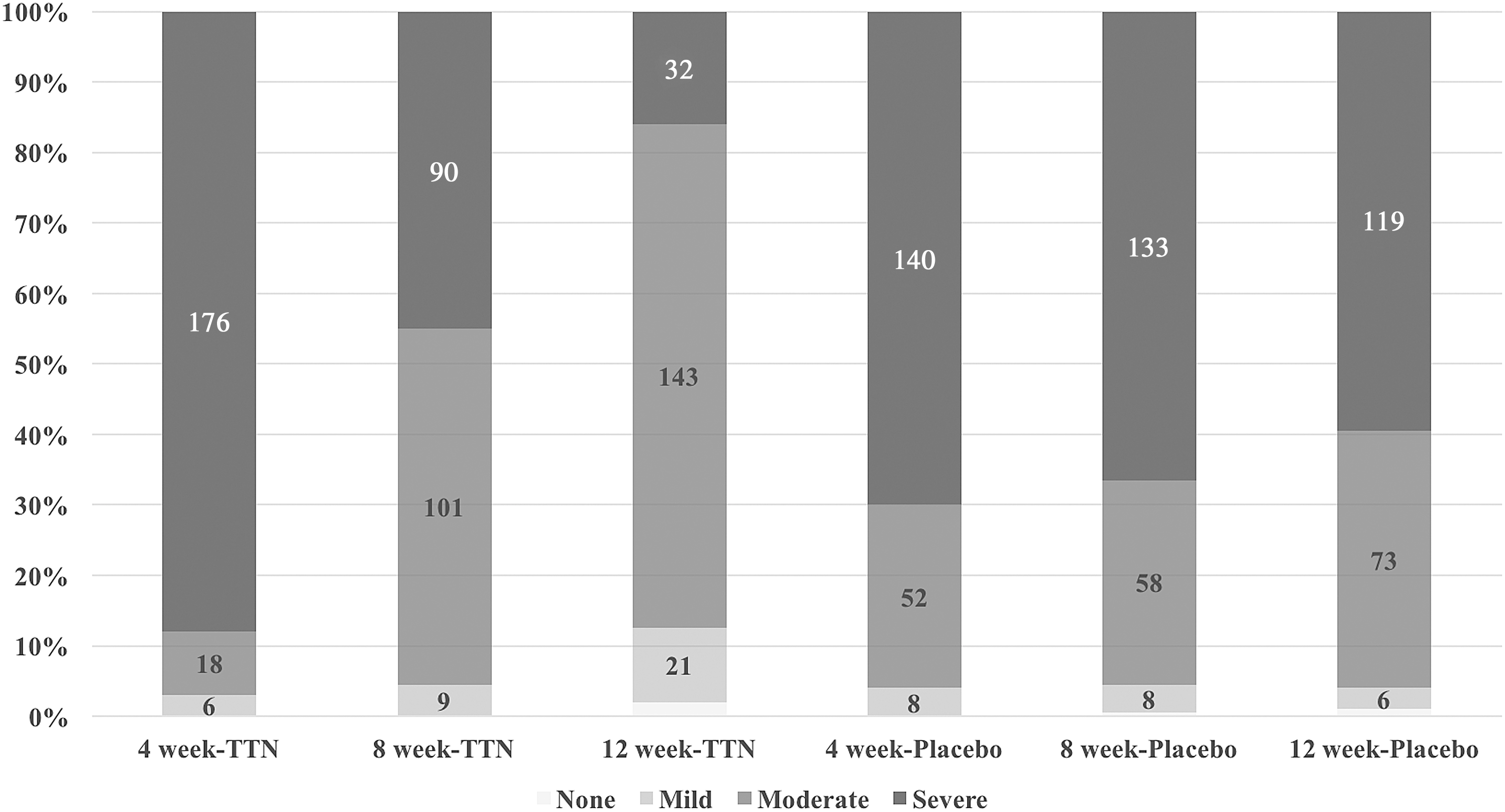
Distribution of patients in different severity of headache.
More favorable differences were also observed in all of the secondary efficacy outcomes in the TTN group compared with the baseline and placebo group at week 12 (p < 0.001; Table 4; Fig. 2). The frequency of headache decreased from 2.52 at week 8 to 2.09 at week 12 (p < 0.001; Table 4; Fig. 2B). The duration of headache attacks decreased from 15.04 h at week 8 to 13.65 h at week 12 (p < 0.001; Table 4; Fig. 2C). When comparing the number of days in which patients had a headache in the baseline period and the 4 weeks preceding week 12, patients experienced a change of −2.8 and −0.64 days with TTN and placebo, respectively (p < 0.001; Table 4; Fig. 2D). The VAS sores decreased to 4.66 at week 12 compared with 5.9 at week 8 (p < 0.001; Table 4; Fig. 2E). The interval time increased markedly to 364.19 at week 12 compared with 257.17 at week 8 (p < 0.001; Table 4; Fig. 2F). The HIT-6 scores also decreased more significantly at week 12 than at week 8 in the TTN group (−13.63 vs. −11.09, p < 0.001; Table 4; Fig. 2G). All differences in primary and secondary outcomes were greater in the PPS analysis.
Safety assessments
In the present study, 11.5% of patients in the TTN group and 9.50% of patients in the placebo group experienced at least one AE during the experiment (Table 5). However, most AEs were mild in severity and were either not related or unlikely to be related to the study medication. AEs that were possibly related to the study drug occurred in two patients: one patient in the TTN group experienced a mild increase in total bilirubin levels and one patient in the placebo group experienced nasal hemorrhaging twice. Overall, no serious AEs were reported and no clinically meaningful changes from baseline were observed in any of the laboratory examinations in either group (Table 6).
Patients Experiencing Adverse Events
Security Measurements in Full Analysis Set Population
Discussion
To the best of knowledge, the present study was the first multicenter, randomized, double-blind, placebo-controlled trial to focus on the efficacy and safety of TTN. The methods and findings of the present study may contribute important insights into patient selection, outcome measures, sample and effect sizes, and the study duration of headache drug trials. In addition, the results may provide credible evidence for the clinical application of TTN capsules for prophylactic treatment of migraine.
The present study demonstrated a favorable effect of TTN for prophylactic treatment of migraine. A large portion of the TTN group (72.50%) had a 50% or more reduction in the frequency of headache after 4 weeks of treatment and several secondary measures, including the days, duration, VAS scores, interval time, and HIT-6 scores, indicating that TTN was significantly superior to the placebo for prophylactic treatment of migraine. In addition, differences in the efficacy measures at week 12 were more evident than at week 8. These results suggest that the effects of TTN may persist even after the discontinuation of treatment. While designing the course of the experiment, the prolonged effects of TTN were not anticipated; therefore, the planned follow-up period was not sufficiently long enough to appropriately estimate the treatment effects. In addition, the mechanisms underlying these treatment effects remain unclear, and future studies will be necessary to determine these processes.
It is important to note that there was a high placebo response rate in the present trial. It is possible that the migraine patients had a high expectation of relief, and the response to placebo treatment is known to be sensitive to the close relationship between headache and psychological problems. 22 Regardless, the TTN capsules in the present trial had a favorable safety profile in the absence of serious AEs; no hepatic or renal damages were reported, other than a mild increase in total bilirubin levels in one patient, and only a single patient suffered nasal hemorrhaging. Also, no unexpected side effects were observed.
The present study had several limitations that should be noted. First, the diagnosis of migraine and some subjective measurements (e.g., VAS) was determined in different groups recruited from 14 clinical centers that participated in the study. Although each researcher was rigorously trained to guarantee consistent standards, it is possible that investigator bias influenced the results. Second, baseline characteristics of participants differed between the TTN group and control group, including HIT-6 scores, VAS scores, and duration of headache attacks. Although headache symptoms were serious in the TTN group at baseline, the frequency, severity, and duration of headache attacks decreased significantly after 4 weeks of treatment with TTN. Finally, because all patients were recruited from China, the results generally only apply to the Chinese population. More research is needed to ascertain whether the findings are generalizable to other populations.
Conclusions
The present trial demonstrated that 4 weeks of treatment with the TTN capsule effectively prevents migraine headaches and the medication was well-tolerated and safe. The TTN capsule may exhibit a persistent therapeutic effect even after cessation of drug administration.
Authors' Contributions
S.Y. was the principal investigator who was responsible for the study design, data analysis and interpretation, and revision of the article. Y.R. analyzed and interpreted the patient data, and was responsible for reviewing the literature and writing the article. Q.W., X.Y., H.C., H.W., X.H., S.M., T.Y., G.L., Y.G., X.G., X.L., M.Z., and Y.L. were regional leaders of this survey. As the corresponding author, Dr. S.Y. had full access to all the data in the study and had the final responsibility for the decision to submit for publication. All authors read and approved the final article.
Footnotes
Acknowledgments
This work was supported by the National Scientific Research Fund of China (grant number 81671077), the Beijing Science and Technology Project (grant Z161100002616013), and the “One Hundred Advantage Projects” Fund of Chinese PLA General Hospital (grant number YS201414).
Author Disclosure Statement
No competing financial interests exist. Buchang Pharmaceutical Company donated the medication and placebo used in study, but had no other role in the research.