
Abstract
Objectives:
The study aims to assess, evaluate, and compare the efficacy of acupressure and hypnotherapy in the management of pain in patients presenting with chronic brachial neuralgia (CBN).
Design:
Randomized controlled trial.
Settings/location:
Department of Orthopaedic Surgery, University Malaya Medical Centre, Kuala Lumpur, Malaysia.
Subjects:
Forty patients with CBN following traumatic brachial plexus injury from 2012 to 2017.
Intervention:
Therapy for a duration of 1 month in two groups; subjects in the hypnotherapy group received a weekly session of clinical hypnotherapy (total of four times) using a standardized protocol, while subjects in the acupressure group were guided by an acupuncturist during the initial session, received 2 month take home supply of acupressure patches, and were reviewed fortnightly.
Outcome measures:
The Visual Analog Scale, the Brief Pain Inventory, and the SF-36v2® Health Survey were recorded at different time points; 1 month pretreatment (week 0), pretreatment (week 4), post-treatment (week 8), and 4 months post-treatment (week 20).
Results:
There was a statistically significant improvement in the average pain intensity from pretreatment to post-treatment score in both groups. The pain intensity increased 4 months later; however, the pain intensity was still significantly reduced in comparison with pretreatment scores. The study suggests that both treatment outcomes are effective in terms of alleviating pain and improving quality of life in subjects with CBN, to a different degree.
Conclusion:
Overall, both therapies were able to improve the pain intensity and quality of life significantly during the treatment period. Hypnotherapy was observed to have a better carryover effect compared to acupressure, especially in terms of improving quality of life and the mental component score.
Introduction
Brachial plexus injury is usually caused by traction to the brachial plexus during trauma. It often leads to impaired physical function of the upper limb and may cause severe neuropathic pain, which could alter the psychologic outlook of the sufferers. 1 –6 There is mounting interest in complementary alternative medicine as a result of ineffective first line treatment in these neurologic conditions; and more emphasis could be placed on the quality of life of the patients.
With accumulating evidence, both acupressure and hypnotherapy have gained much popularity among chronic pain sufferers and have been widely used in treating chronic pain. There are reports of acupressure and hypnotherapy demonstrating the ability to reduce intensity of chronic pain. 7,8 A search of the literature yielded no studies that specifically addressed the efficacy of either hypnotherapy or acupressure in pain management of patients presenting with chronic brachial neuralgia (CBN). The aim of this study is to assess and compare the efficacy of acupressure and hypnotherapy in terms of reducing pain intensity and improving the quality of life in patients presenting with CBN following traumatic brachial plexus injury (TBPI).
Materials and Methods
The study was conducted in the University Malaya Medical Centre (UMMC) (Medical Research Ethics Committee Reference Number: 937.11) between the years 2012 and 2017. A total of 40 subjects with CBN were randomized into two groups, acupressure (n = 20) and hypnotherapy (n = 20), using the block randomization method. The sample size estimation was obtained using G*Power© sample size calculation software. Based on the pilot study, the mean and standard deviation of the two groups were 6.90 (0.88) and 7.90 (0.99), respectively. With type I error of 0.05 and power of 0.90, the required sample size was 20 for each group.
Four sessions of clinical hypnotherapy were conducted, 1 week apart in the hypnotherapy group and two sessions fortnightly in the acupressure group, for a duration of 1 month. Subjects were scored 1 month pretreatment (week 0), pretreatment (week 4), mid-treatment (week 6), post-treatment (week 8), and 4 months post-treatment (week 20). Visual Analog Scale (VAS) scores were obtained before treatment as a baseline control (week 0 to 4), where subjects acted as their own control, and subjects were rescored later, in week 6, 8, and 20. The Brief Pain Inventory (BPI) and SF-36v2® Health Survey were used to measure overall health changes and the efficacy of the treatment in terms of improving various aspects of quality of life.
Patients who were diagnosed with brachial plexus injury by a specialist, presenting with CBN with moderate-to-severe pain (VAS 5 to 10), were referred and screened, based on their inclusion and exclusion criteria (Table 1) during the first session. Study selection criteria required that subjects have symptoms for more than 6 months and with persistent pain despite other forms of medical intervention. Patients who were scheduled for surgery within 6 months and those with preexisting psychotic conditions and or cognitive impairment were excluded from this study. Informed and written consent was obtained from all patients. Subjects were also provided with an information sheet explaining acupressure or clinical hypnotherapy.
Inclusion and Exclusion Criteria of the Study
VAS, Visual Analog Scale.
Subjects in the acupressure group were guided by a qualified acupuncturist and were instructed on the protocol to apply the acupressure patches to specific meridian points which resulted in the best response. Subjects were provided with a 2 week supply of acupressure patches to take home and were reviewed at mid treatment (week 6) for progress feedback and for any revision of the meridian point patching protocol. The patches comprised nanoscale nontransdermal organic materials which were said to mildly and continuously stimulate the acupuncture points. The major acupuncture points used in their subjects were the governing vessel 14 (GV14), conception vessel 17 (CV17), triple energizer 14 (TE14), small intestine 11 (SI11), and pericardium 6 (PC6).
The subjects in the hypnotherapy group were referred to a clinical hypnotherapist for 4 weekly hypnotherapy sessions. The assigned clinical hypnotherapist used a standardized pain analgesic protocol for all the sessions with specific analgesia suggestions. At the initial consultation, the hypnotherapist used the Patient Health Questionnaire (PHQ-9) questionnaire to exclude subjects with preexisting psychosis illness. The focus of hypnosis in the treatment of chronic pain also involved teaching the patient self-hypnosis that could be used to reduce pain on a daily basis, outside the face-to-face sessions. The initial appointment lasted approximately for about 2 h, where a full case history was taken, with the subsequent appointments lasting for about one and a half hours.
All data obtained were tested for normality distribution using the normality curve available with the SPSS package (IBM SPSS Statistics, Version 24). The efficacy of both treatments were calculated using the statistical analysis of paired t tests, and comparison of both modalities was analyzed using the independent t test. The effect size estimation was calculated using Cohen's d, to indicate the standardized difference between two means which supplemented the t test values. The SF-36v2 Health Survey© data were manually recorded into the Optum Pro Core Smart Measurement® System Version 1.0.6431.17600 software.
Results
A total of 40 CBN subjects (all male) with the mean age of 35.83 ± 12.52 (range 18–68 years) were recruited into the study, based on the specific inclusion and exclusion criteria. The mean duration of TBPI was 44.78 ± 39.95 months (range 7–183 months). Only 15 (37.5%) of the subjects were currently employed. For the 40 subjects, 24 brachial plexus injuries (60%) were total, while 16 (40%) were partial. Twenty-five subjects (62.5%) reported to have pain over the whole upper limb. Subjects in the acupressure and hypnotherapy groups had similar percentages of complete and incomplete injuries, the percentage being 60% and 65%, respectively.
There was no observed difference of mean average pain intensity between the two groups during baseline pretreatment week 0 to 4 (Tables 2 and 3). This shows that all of their enrolled subjects were resistant to the first line treatment and were still in pain. There was a significant decrease in pain intensity (p < 0.05) observed between week 4 and 8 in both groups. Subjects in the acupressure group reported a mean average pretreatment week 4 VAS of 7.25 ± 1.29 and mean average post-treatment week 8 VAS of 4.40 ± 2.19 (28.5%), while subjects in the hypnotherapy group reported the mean average pretreatment week 4 VAS as 8.00 ± 1.38 and mean average post-treatment week 8 VAS of 4.95 ± 1.76 (30.5%) (Fig. 1).
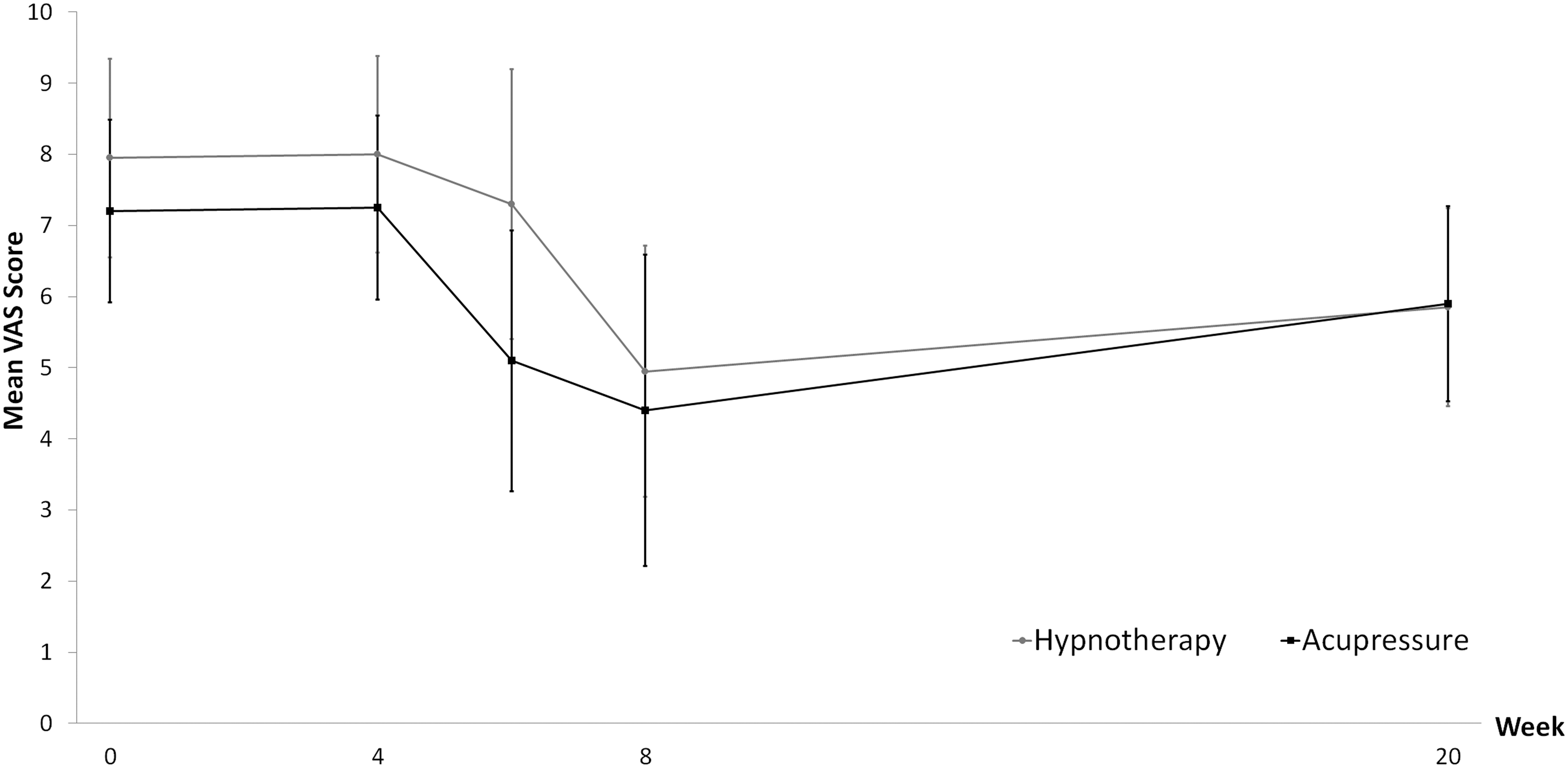
The comparison of VAS scores in both groups from week 0 to 20. VAS, Visual Analog Scale.
Statistical Analysis of the Average Pain Intensity in Acupressure and Hypnotherapy Group
CI, confidence interval; SD, standard deviation; SE, standard error.
Statistical Analysis of the Average Pain Intensity Difference in Both Groups
CI, confidence interval; SD, standard deviation; SE, standard error.
The acupressure therapy was observed to provide significantly better pain reduction (p < 0.05) with high effect size estimation (1.36) compared to hypnotherapy at week 6 (0.46). Hypnotherapy was observed to reduce the subject's pain score less at week 6; however, the average pain scores were reported to further decrease at week 8 similar to the pain score change in the acupressure group. The mean average of pain intensity 4 months post-treatment (week 20) for acupressure and hypnotherapy was 5.90 ± 1.37 (range 4–8) and 5.85 ± 1.39 (range 3–8), respectively. There was significant difference in the pain intensity post-treatment (week 8) and 4 months later (week 20) (p < 0.05) indicating that subjects in both treatment groups reported a significant increase of pain intensity 4 months post-treatment. The pain scores in both treatment groups from week 4 to 20 however showed that there was still a significant decrease of pain intensity observed (p < 0.05), implying the positive efficacy of both treatments in managing the chronic pain in the long term.
There was significant difference in comparison of mean change of both groups observed from week 4 to 6 and week 4 to 20 (p < 0.05). The findings were consistent with the paired sample t tests and effect size estimation values where the results suggest that acupressure reduced the pain intensity faster than hypnotherapy from week 4 to 6 (Table 3). However, hypnotherapy had a better effect in reducing pain intensity from week 4 to 20 compared to acupressure.
As for the effect size estimation, the authors noted that both therapies had a large effect size estimation (d > 0.80) of change in mean pain intensity from week 4 to 8 and week 4 to 20 (Table 4). The data reflected that both therapies successfully reduced pain intensity following 4 weeks of therapy. The results also revealed that acupressure had a large effect size estimation of increased pain intensity (0.82) observed from week 8 to 20, while hypnotherapy had a medium effect size estimation (0.57), suggesting that subjects in the acupressure group experienced a larger rebound of pain intensity from week 8 to 20 compared to subjects in hypnotherapy group, although the overall reduction from the beginning to end was favorable.
The Effect Size Estimate, Interpretation, and Statistical Significance
The BPI scores obtained from each time point in both groups showed that all of the observed aspects in the BPI questionnaire were significantly improved over the course of the treatment and 4 months post-treatment (week 4 to 8 and week 4 to 20) (Fig. 2). Results of pain and interference scores in the acupressure and hypnotherapy groups varied from week 8 to 20, with hypnotherapy able to retain several aspects of the pain and interference scores, while this was not observed in acupressure group.
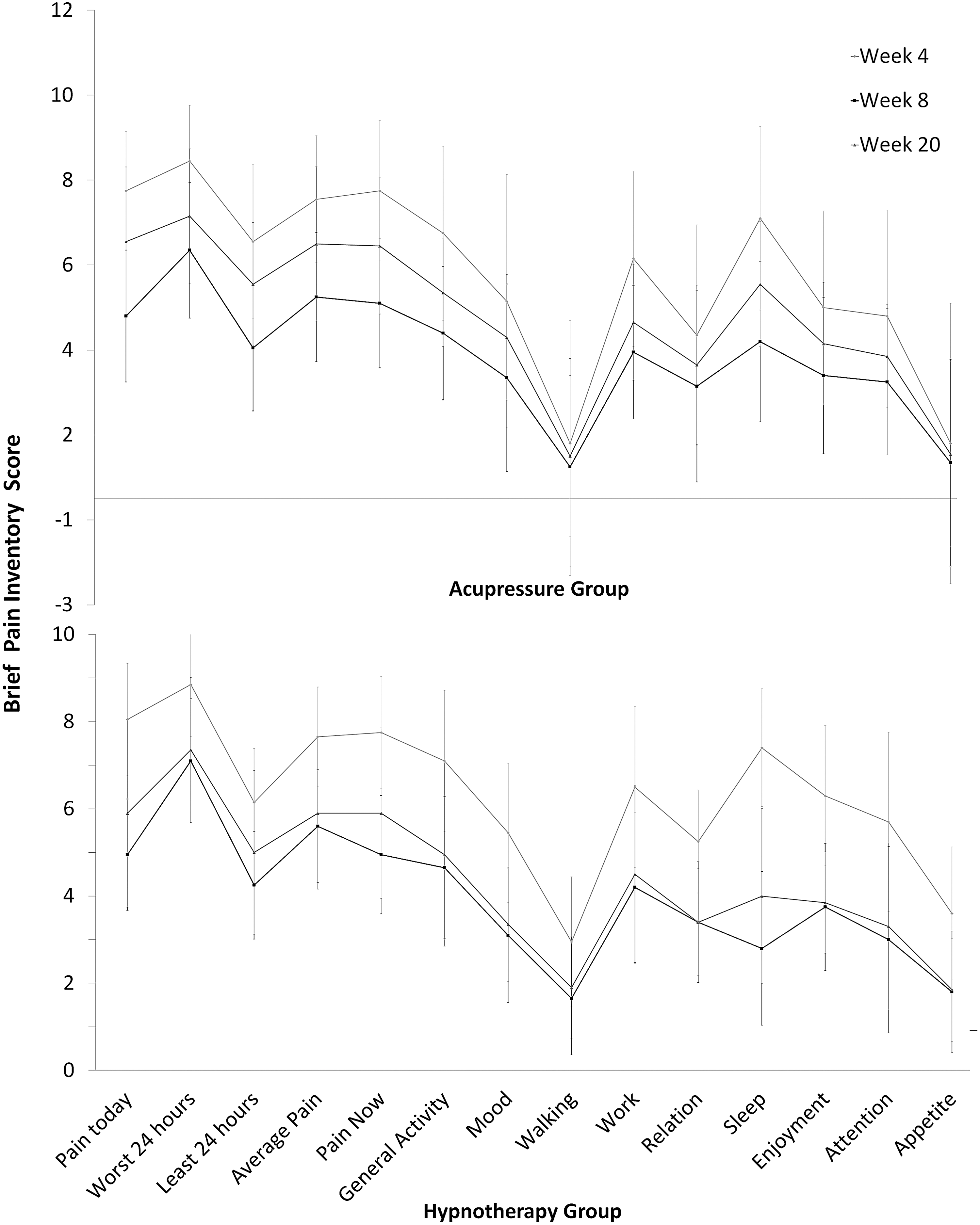
Changes in aspects of Brief Pain Inventory scores at different time points.
With regards to the effect size estimation of both acupressure and hypnotherapy from week 4 to 8 on pain interference with quality of life, the authors noticed that both acupressure and hypnotherapy had a statistically significant large impact (d > 0.80) on improving subjects' sleep, “today's pain score,” and “current pain score.” The effect size estimation of BPI aspects in the hypnotherapy group was observed to be better than the acupressure group, implying that hypnotherapy provides stronger effects in alleviating pain scores and the pain interference associated with quality of life. There were multiple aspects reported to be retained in the hypnotherapy group from week 8 to 20. The aspects were “worst pain in 24 h,” average pain, mood, walking, relations, and enjoyment.
The SF-36v2 Health Survey data quality evaluation report showed satisfactory data quality, ranging from 94.3% to 100%. The survey reported that 55% of the subjects had the risk of first stage positive depression on screening. This is considered to be relatively high, with reported average normal percentage among general population at 18%. All of the physical component scores (PCS) and mental component scores (MCS) during initial screening of week 0 were below the normal score of 50. This indicates that physical and mental conditions were greatly affected by the disease and chronic pain itself.
The SF-36v2 Health Survey demonstrated that both acupressure and hypnotherapy increased the PCS and MCS after the subjects attended 4 weeks of therapy (Fig. 3). However, subjects in the acupressure group reported significantly decreased scores, while subjects in the hypnotherapy group reported similar scores during week 20 compared to scores in week 8. Subjects in both groups however were noted to have a significant improvement of PCS and MCS from week 4 to 20. The authors also found that hypnotherapy further improved the “mental health aspect” up to 4 months post-treatment, with observed increase of scores from week 8 to 20.
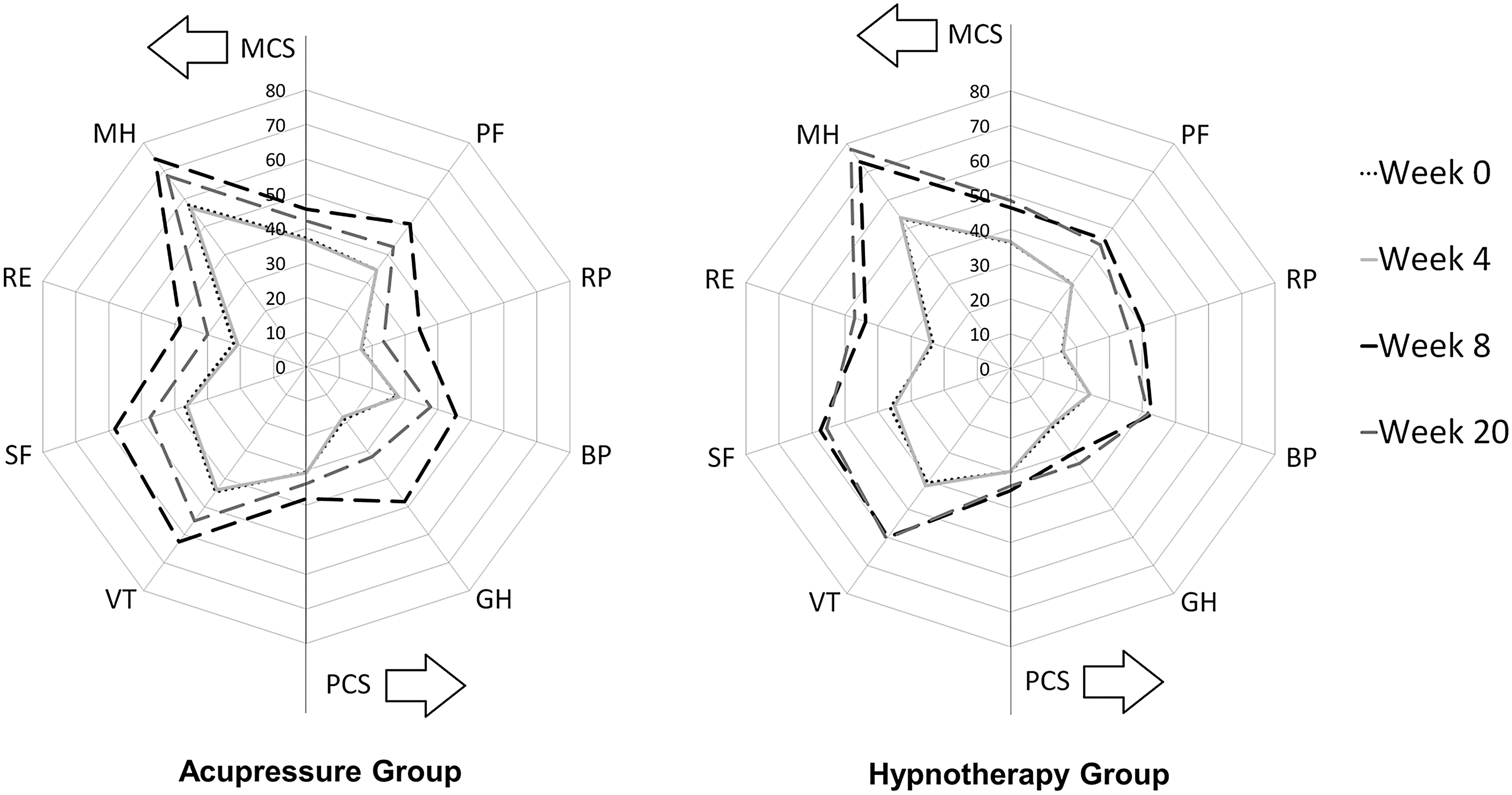
Comparison of SF-36v2® scores. This shows better retention of improvement in the hypnotherapy group. MCS, mental component score; PCS, physical component score.
The results suggest that hypnotherapy was superior in maintaining most aspects in the SF-36v2 Health Survey compared to acupressure. The independent t test revealed that hypnotherapy was better than acupressure in terms of keeping scores of “role physical,” “social functioning,” “role emotion,” mental health, and MCS in week 20, similar to the scores in week 8. Findings also suggested that acupressure was seen to provide better scores in general health during week 8, compared to the hypnotherapy group.
Both modalities were considered safe, with no reported adverse effects. However, there were two subjects in the acupressure group who experienced local redness on their skin. The symptoms did not worsen and disappeared within 1 day of the removal of patches. Sixty-five percent of the subjects reported a positive impression and would have liked to continue the therapy, while 35% of subjects responded as neutral or with no comments.
Discussion
Despite being used widely and practised as an alternative tool to attenuate pain, 9,10 the efficacy of acupuncture in treating neuropathic pain remains unclear. Most literature refers to acupuncture rather than acupressure. Although this is a separate modality, it is based on the same principals and meridians. The role of acupuncture in decreasing pain intensity in CBN has proven to be effective in the rat model, 11 while several studies reported that there was insufficient evidence to support or negate the use of acupuncture for chronic neuropathic pain conditions. 7,12 In their study, acupressure was noted to provide 10% improvement in pain intensity reduction from week 4 to 8 in their complete brachial plexus injury subjects, especially in the subjects with high VAS score of 8 to 10. These effects were consistent with a clinical study by Nayak et al. where they concluded that spinal cord injury patients with incomplete nerve injuries responded to acupuncture treatment better than patients with complete injuries. 8,13 The authors suggested that acupuncture was shown in musculoskeletal and central nervous system pain to be more effective in reducing moderate pain rather than in severe pain. The study also revealed that subjects with moderate pain reported to have longer carry over effects of therapy compared to those with severe pain.
In other studies, hypnotherapy was reported to constantly produce a significant decrease in various types of chronic pain. 14 Hypnotic analgesia was able to target multiple brain sites, specific brain locations, and address issues beyond pain reduction alone. 15 Theoretically the effects denote its ability to promote overall tissue healing and inflammation. In their study, the recorded psychologic aspects of the subjects in the hypnotherapy group following treatment were observed to be better than in the acupressure group. This was most likely contributed to by the relationship and trust established during the hypnotherapy sessions. 16 Subjects in the hypnotherapy group received longer contact time (1.5 to 2 h of intensive therapy per session, total of four sessions, 6 to 8 h) than those in the acupressure therapy group. Acupressure therapy focused on application of the patches to the best meridian points, with shorter contact duration and number of sessions.
Generally, the results suggest that both therapies demonstrated significant improvements in alleviating pain intensity and improving quality of life aspects in the subjects across week 4 to 20. The changes occurring in this study were a minimum average of VAS 28.5 mm on the scale. This is definitely clinically significant. A study by Todd et al. suggested that even a change of 13 mm is significant and noticeable clinically. 17 Acupressure was observed to provide quick and subtle pain relief following its application (as early as 30 min) but with some loss of relief over week 8 to 20. The authors concluded that subjects in the hypnotherapy group were able to remain positive, with the aid of self-hypnosis, which may have boosted the emotional and mental aspects of the subjects. In the literature, patient's hypnotizability scores, openness, belief, and trust were associated with better outcomes in pain relief. 18
The possible reasons for changes of scores across time points in their subjects may be, in part, resulting from the subject's adherence to the protocol, such as compliance to patching protocol among subjects in acupressure group and self-hypnosis homework practice in hypnotherapy group. The placebo effect could also have led to the fast pain reduction rate observed among subjects in acupressure group in week 6. The nocebo effect then could have contributed to increased pain intensity from week 8 to 20. The use of self-hypnosis as a tool was also undeniably beneficial in managing the pain, but it may not have been practised by all of the subjects.
The authors encountered several limitations in their study. The number of subjects enrolled in this study reached the number just sufficient for analysis. The limited number of recruited subjects was due to the strict study inclusion and exclusion criteria, with several subjects who declined to be enrolled in the study and drop outs. Nevertheless, the use of Cohen's d value supported the significance of the results, as it provided consistent and meaningful conclusive data on the effectiveness of both treatment outcomes. There was no recorded belief rating or susceptibility scoring; thus, the authors were unable to correlate between the perception, susceptibility score, and effectiveness of the therapies. Subjects were not requested to keep a diary to record their compliance. Future study is needed to assess the trend of the carryover effect of both therapies for a longer period of time.
Conclusion
Both acupressure and hypnotherapy provided significant reduction of mean average pain intensity in chronic brachial plexus injury. There was increased mean average pain intensity rebound post-treatment in both groups; however, the overall reduction of pain intensity was still significant. Most subjects in the hypnotherapy group were able to maintain improvements in most components in the BPI and SF-36v2 Health Survey 4 months post-treatment, less so with acupressure. Hypnotherapy continued to improve the mental health of subjects up to 4 months post-treatment. Acupressure, on the other hand, provided faster pain relief but with lesser carryover effects.
Footnotes
Acknowledgments
The research was funded by the University Malaya Research Grant (UMRG) and LifeWave, Inc. The authors thank the London College of Clinical Hypnosis (LCCH), Dr. Abdul Hanan Soh, Dr. Sivashanmuganathan Sagathavan, Mr. Ko Teik Yen, and Mr. Ong Hean Kheng for their valuable contribution toward the completion of the research project.
Author Disclosure Statement
No competing financial interests exist.