
Abstract
Objectives:
Naturopathic medicine has demonstrated efficacy at reducing risk factors for chronic disease. Targeting health behaviors of parents and caregivers in a group-based setting may improve the behaviors of children in their care. This study sought to assess the feasibility of such a program.
Design:
Participants of a six-session health education series were invited to respond to surveys and participate in a focus group about their health behaviors and their experience in the program.
Subjects:
Caregivers of children aged 0–6 attending publicly funded community centers in Ontario, Canada.
Interventions:
A 6-week group-based naturopathic education program to promote healthy lifestyle behaviors among caregivers.
Outcome measures:
Satisfaction with content and delivery, and frequency of healthy behaviors.
Results:
The majority of responses indicated satisfaction with the program, and an ongoing benefit 6 weeks and more after completion. There was a clear correlation between healthy behaviors of parents and children.
Conclusions:
A group-based naturopathic education program may be a feasible method of delivering primary-prevention education to caregivers, particularly in the domains of practicality and acceptability.
Introduction
Noncommunicable disease (NCD) is the leading cause of mortality worldwide 1 Upward of 75% of health care spending in developed nations is for individuals with chronic disease. 2,3 The top four causes of death—cardiovascular disease, cancer, respiratory disease, and diabetes 1 —are conditions that have modifiable lifestyle determinants, including diet, physical activity, and tobacco use. 3 Inadequate sleep, 4 toxic stress (especially during early life), 5 environmental toxins, 6 and inappropriate use of medications such as antibiotics potentiate the underlying common mechanisms, 7 notably oxidative stress and an inflammatory phenotype. Primary prevention is the most effective means of reducing the prevalence of NCD. 3 Naturopathic approaches have demonstrated efficacy in decreasing risk factors for NCD, effectively reducing health care costs. 8,9
Although behavior change can be difficult to promote and maintain in adulthood, behaviors established in childhood tend to persist throughout the lifespan. 10 –12 There is myriad evidence that prenatal, infant, and childhood health lay the foundation for adult well-being, including the risk of NCD. 13 –16 Maladaptations to suboptimal conditions set the stage for chronic inflammation, oxidative stress, and metabolic dysregulation. 17,18 All four of the top NCD identified by the World Health Organization have determinants originating in childhood, including obesity, 14,19 –22 childhood adversity, 17,23 environmental exposure, 24 –32 suboptimal nutrition, 33,34 and early life antibiotic use. 35 –38 To improve community health, interventions are needed early to reduce the impact of these determinants. Because primary caregivers directly control factors such as nutritional options, emotional bonding, health care approaches, and opportunities for physical activity, targeting caregivers may be beneficial in promoting healthy behaviors in children and reducing the risk of NCD. 17,39,40 The impact of parental modeling has been demonstrated for a wide range of behaviors, including fruit and vegetable consumption, 41 –43 physical activity, 43,44 screen use, 45 smoking, 46,47 and empathy. 48
Strategies other than one-on-one clinical encounters may create opportunities to bridge gaps in health literacy. 49,50 Group programs can facilitate learning and enhance community and social support, more deeply engaging participants in self-care. 51 Group visits have been successfully used for prenatal care, 52,53 to support and educate parents of children with and attention deficit hyperactivity disorder (ADHD), 54 and for primary prevention of pediatric obesity 55,56 including the “Lifestyle Triple P,” trials of which have demonstrated benefit. 57,58
There is a paucity, however, of data on group programs that focus on general wellness promotion in families. Healthy Family, Healthy Kids (HFHK) is a group program designed to deliver evidence-based preventative health education. It aims at facilitating decision making by caregivers with a goal of reducing risk factors for NCD in children. The program was developed and delivered by naturopathic doctors and students; in Ontario, naturopathic doctors are regulated primary health care providers with a broad scope of practice. This study explores the feasibility of the program.
Methods
Intervention
The HFHK program consisted of six 2-h educational sessions offered at provincially funded Early Years Centers (EYCs) in Toronto and Cambridge (Ontario). EYCs provide free health and development programming for families with young children, and they offer childcare during programs for caregivers. We targeted families with at least one child from newborn to 6 years of age (also the target for the EYC). Participants enrolled in one of four iterations of the program between October 2014 and June 2016. The groups were facilitated by naturopathic doctors and students. The content and methods were consistent among iterations, with space for flexibility based on group needs and facilitator style.
Topics included nutrition, environmental health, optimizing immune function, psychosocial well-being, and other determinants of health such as physical activity and sleep. The objectives of each session are provided in Appendix Table A1. A variety of teaching methodologies were used to accommodate different styles of learning, including traditional didactic methods, small group discussion, hands-on activities, and social media engagement. Every session incorporated setting goals for behavior change. Appendix Table A2 provides examples of different delivery approaches. HFHK was solely an educational program, and it offered no individual medical care to participants.
Study design and analysis
We used a sequential explanatory mixed-method study design 59 (quantitative surveys with open-text responses, followed by a focus group) to seek cross-validation of results (Fig. 1). 60,61 Questions proposed for feasibility studies by Orsmond and Cohn 62 and Tickle-Degnen 63 were used for guidance; the primary area of focus was acceptability to participants. 64 The good reporting of a mixed-methods study (GRAMMS) guidelines proposed by O'Cathain et al. 65,66 provided structure to our description of methods and results. Semi-structured interviews were also held with the administrators of the EYCs where the program was hosted. This was an open-label design without a control group.
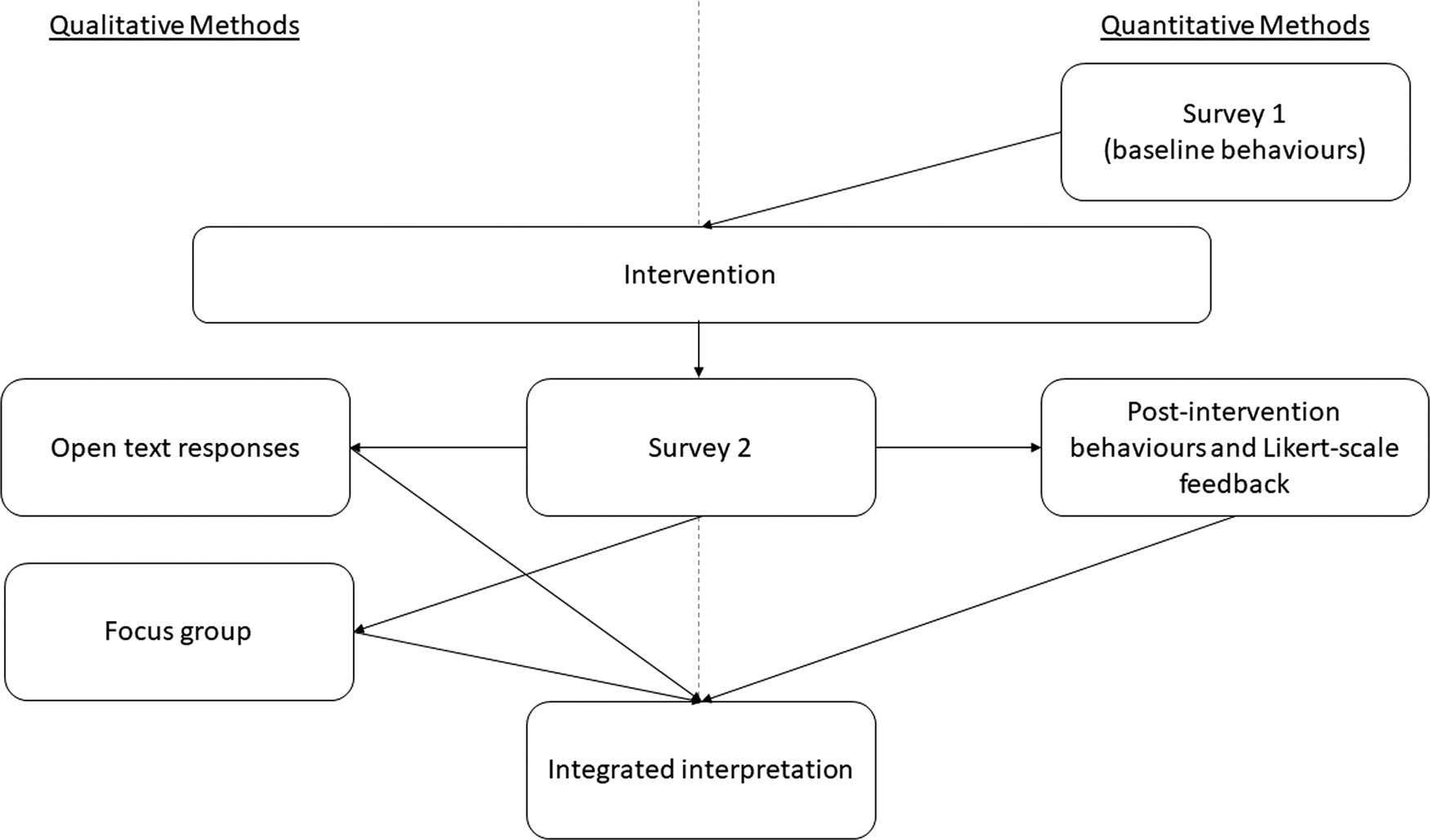
Flow of study design and methodology.
All program registrants were invited to complete survey 1 online at the outset of the program; questions were related to health-related behaviors. All respondents were invited by e-mail to complete survey 2 6 weeks after finishing the program. Survey 2 inquired about the same behaviors, and it prompted the participants' evaluation of the program (both surveys can be viewed in Appendix 1). Quantitative responses were provided according to a Likert scale, and open-text responses were invited. No structured face validity testing was used to assess the surveys; however, the materials were reviewed by a number of mentors and colleagues and deemed to be relevant to the goals of the study. Survey responses were matched based on the combination of e-mail address and birthday of the child; parents were informed that this was the sole reason for collecting this information. Respondents were sent a $30 honorarium for completing both surveys; no reimbursement was provided for completing only the first.
Count, percentage, and median response values were determined to evaluate acceptability; themes were assessed within the open-text responses. To explore preliminary evidence for efficacy, Spearman rho was used to evaluate the correlation between parent and child behaviors. Wilcoxon signed-rank test was used to determine whether there were significant differences in these behaviors both before and after the program.
All interested respondents were invited to participate in a focus group to further explore the themes that arose from the surveys. The focus group took place in November 2016; all participants had completed the program the previous spring. A 1-h semi-structured conversation focused on strengths and weaknesses of the program; discussion around a particular question continued until no new themes emerged. The focus group was recorded, transcribed, and analyzed by using a content analysis method, and the themes were connected and compared with the quantitative data. 67 Focus group participants received a $50 honorarium for participation.
The study received research ethics board approval from the Canadian College of Naturopathic Medicine before conduct.
Results
Forty-two individuals registered to participate in one of the four iterations. Thirty-four took part in four different iterations of the 6-week program. Group sizes ranged from 5 to 12 participants. All but one participant were female. Two caregivers were grandparents; the rest were parents. Ethnic diversity represented the wide range typical of the Greater Toronto area. More than half of the participants attended four or more of the six sessions; more than 75% attended three or more.
All program participants were invited to complete survey 1 (some participants started attending later in the series and were not included in the study). There were 24 responses to survey 1 (response rate 70.1%; 11.01% margin of error, 95% confidence interval [CI]) and 18 responses to survey 2 (response rate 52.9%; 16.8% margin of error, 95% CI). The flow of participants through the program and study is illustrated in Figure 2. The ages of the children were between 1 and 7 years. Demographic information of the respondents was not systematically gathered.
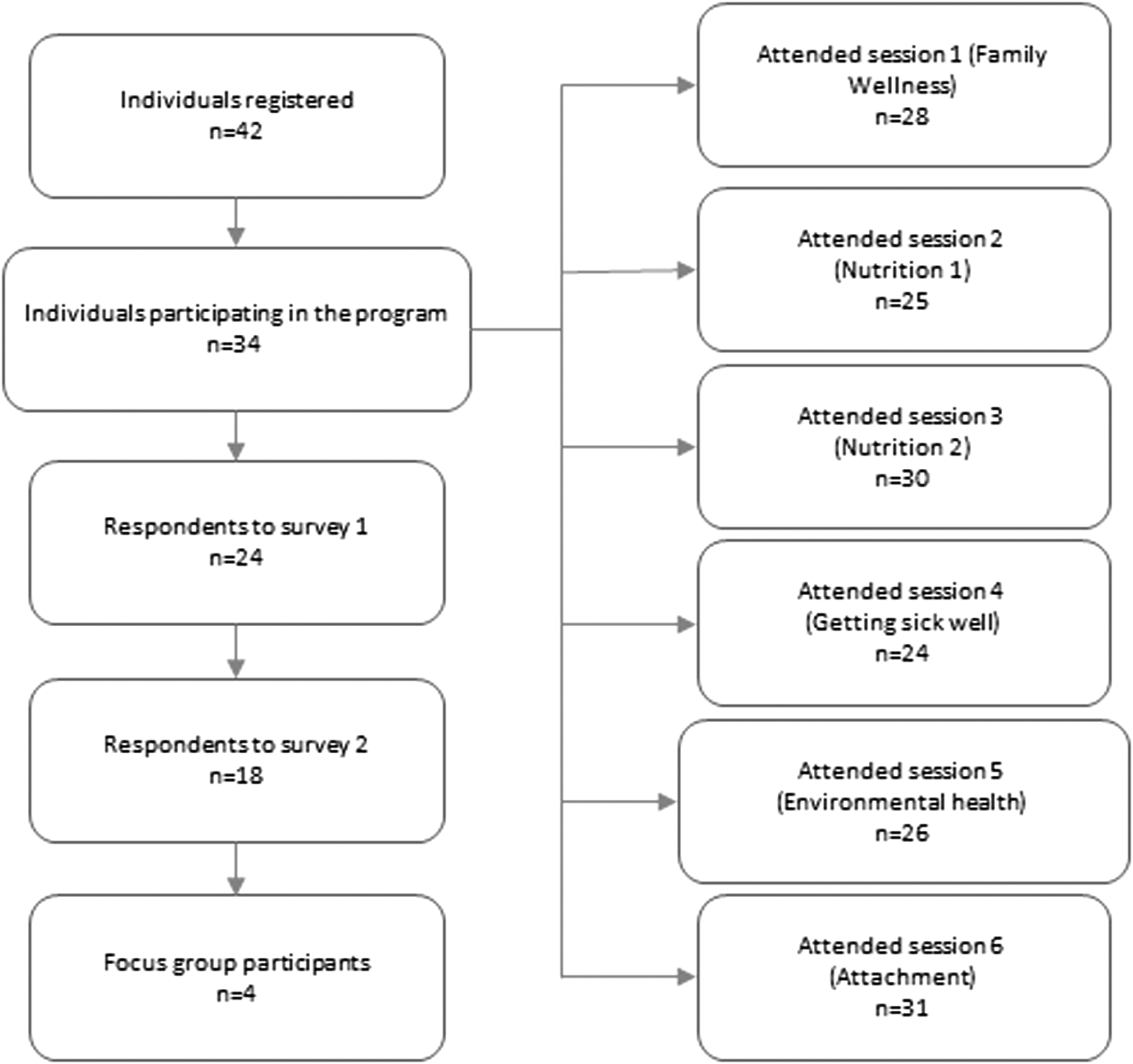
Flow of participants through the intervention and study.
Most respondents to survey 2 had attended all sessions, with only one or two missing any one session. One hundred percent of respondents indicated that they were “satisfied” or “very satisfied” with both the content and the delivery of the program overall. The majority of participants found all sessions helpful; basic nutrition (“Nutrition 1”) and coping with illness (“Getting Sick Well”) were rated as helpful by 100% of the participants who attended (Fig. 3).
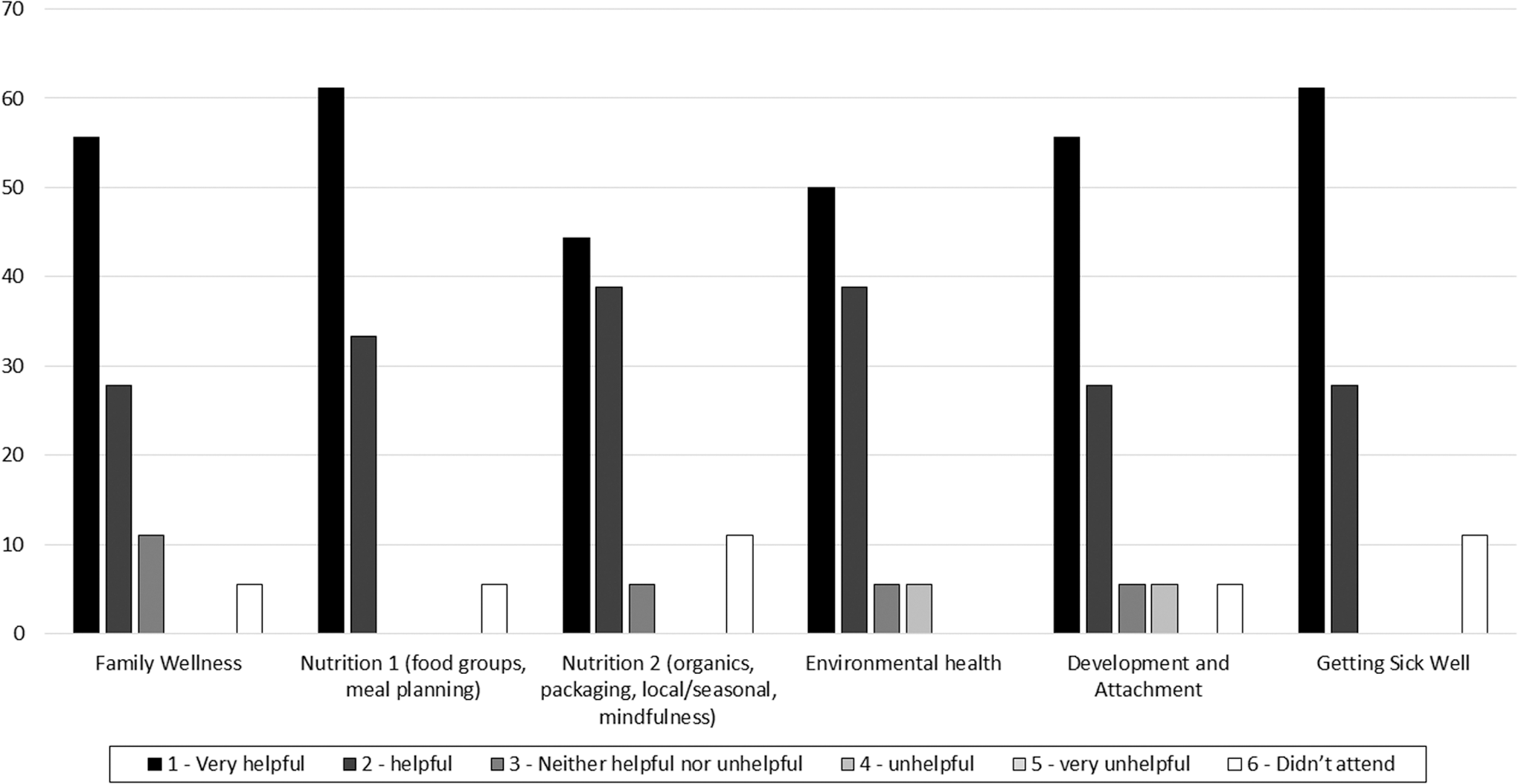
Percentage of respondents reporting individual sessions as being helpful to their family's health. The majority of participants found all sessions helpful.
All delivery methods were evaluated as being used to an appropriate degree, with between 66.7% and 100% of respondents deeming that each method was used “just the right amount” (Fig. 4). The methods that were desired more by most respondents included Facebook posts (27.8%) and shared resources (33.4%).
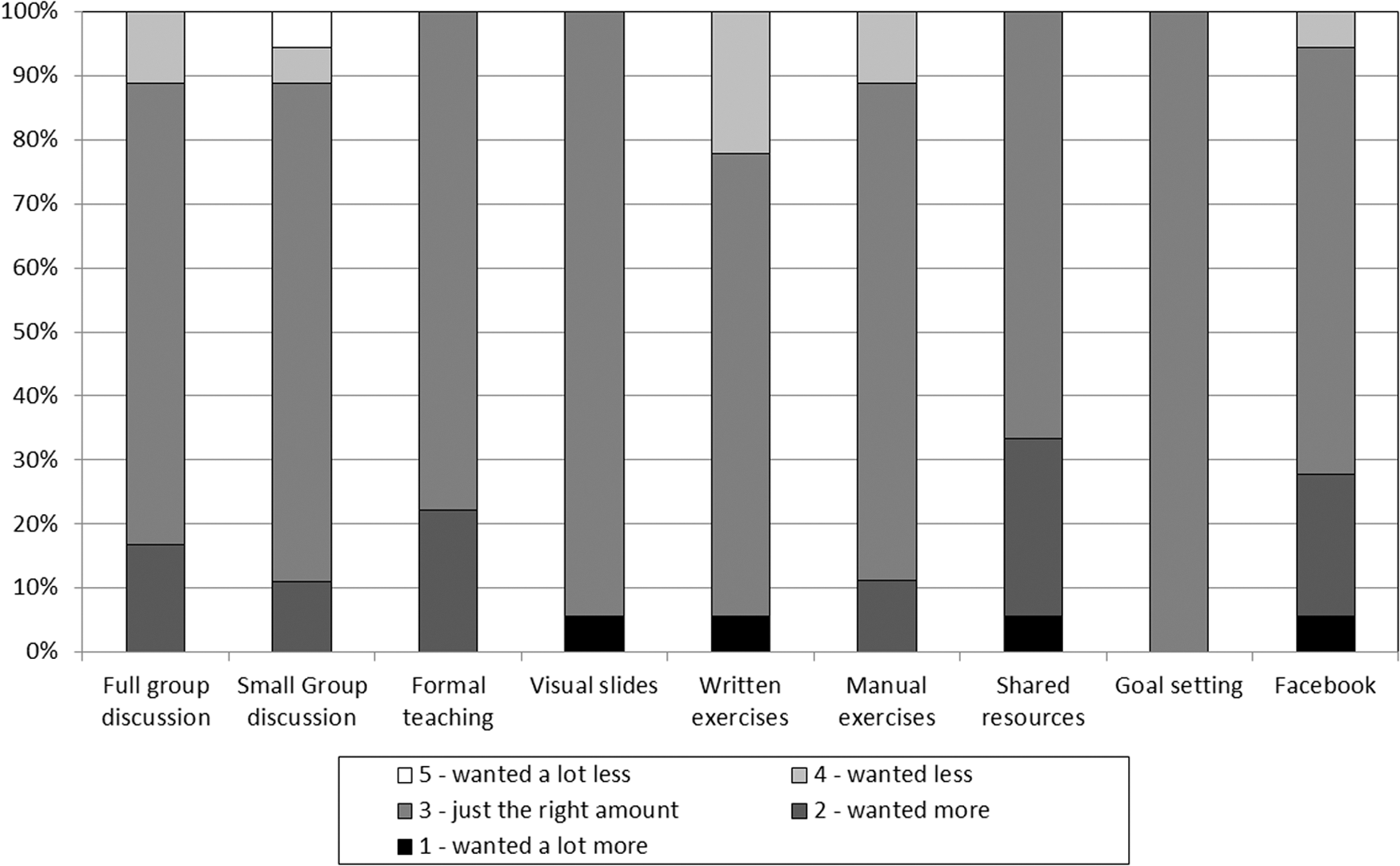
Evaluation of delivery methods by respondents. All delivery methods were evaluated as being used to an appropriate degree.
Most respondents indicated an ongoing benefit of the program at the time of completing survey 2, with 100% indicating a conscious application of concepts learned. Overall, 66.7% of respondents referred back to resources used during the program, and 94.5% agreed that the program was valuable to their family's health. Fourteen of 17 open-text responses received in response to the question “what was most valuable to you” about the program cited various elements of content. The practical nature of the course followed with six mentions, and the group approach with four. Two open-text responses reflected that the program improved their confidence in their ability to care for their children. Ten comments of 12 suggested more hands-on activities and resources such as handouts, electronic information, and Facebook.
We noted a significant correlation between behaviors of caregivers and their children both pre- and postintervention (Table 1). There were no significant differences in behaviors between pre- and postcourse responses for either child or adult.
Correlation Between Health-Promoting Behaviors of Caregivers and Children (Postcourse)
Four focus group participants were drawn from three program iterations in two different centers. They had all attended five or six of the six sessions. Because demographic information was not collected, it is unclear whether the characteristics differed between focus group participants and nonparticipants. One participant attended via telephone. There was strong agreement among participants, and saturation was reached quickly. Participants expressed that the program was manageable in terms of structure and content. They indicated that the content was trustworthy, built on pre-existing knowledge, and gave them the opportunity to apply it without pressure. The delivery approaches catered to different learning preferences. They appreciated having a skilled, knowledgeable facilitator. Resources were appreciated, and more were desired. It was suggested that the lack of cost to participants may have decreased commitment; all indicated that they would have paid for the program. The importance of providing childcare was strongly emphasized. All participants expressed an interest in doing more of this kind of program, a theme that was apparent from open-text responses as well. Key themes that emerged from the focus group are outlined in Table 2 and compared with the findings from the survey.
Key Themes Emerging from Open Text Responses and Focus Group
We did not survey individuals who chose not to participate in the program. However, center administrators cited a range of obstacles to registration or attendance, including poor timing and difficulty with transportation or conflicting obligations. Some were not interested in “natural medicine.” One administrator reported that some participants expressed concern that others were being too dominant. Facilitators also noted that it was occasionally difficult to ensure the needs of the entire group were being met. Some participants already seemed literate on some topics, with others finding them quite novel. Some participants appeared to want more one-on-one personal support that the program was not designed to offer; at times, this pulled the group off track.
Discussion
The HFHK program appears to be an acceptable way to deliver lifestyle education to caregivers of children aged 0–6. Collaborating with the Ontario EYC enhanced our ability to recruit participants in our target population, and offer the physical resources needed for the program (such as administrative support, childcare, consumable materials, space); access to childcare services was highly valued by participants. Respondents communicated appreciation for the topics explored in the program; it may be beneficial in the future to assess baseline knowledge and interest of participants, placing more emphasis on topics that are unfamiliar or that are in higher demand.
There was particular appreciation for the sharing of resources and practical application. Although all respondents reported a conscious application of concepts in the weeks or months after the program, offering additional resources as suggested may have further supported these participants in their efforts.
Focus group responses acknowledge the reassurance of hearing other parents' stories and experiences. Previous studies support the findings that group-based education improves parental confidence, reducing stress in the home and promoting attachment between parent and child. 68 –71 However, it is important that facilitators have sufficient training and support engaging in this method so that the needs of all group members are met.
All focus group participants indicated that they would have willingly paid for the program, and they suggested that not charging a fee may have decreased accountability. Previous research suggests that patients would pay for a valuable program 71 ; however, it may be difficult to determine the ideal fee for this program while maintaining its accessibility, especially for lower income families. The publicly funded EYCs are mandated to provide early childhood programming free of charge; it would be challenging to find another partnership so ideally suited to the needs of the program. Given the network and funding of these centers across the province of Ontario, it offers an excellent opportunity to deliver the program in a variety of communities with a range of participant characteristics (with the common feature of children aged 0–6). However, funding is necessary to adequately compensate facilitators for their time and expertise.
Although the design and power of our study were insufficient to make any conclusions about efficacy, a variety of studies have demonstrated the effectiveness of group-based programs directed at parents. Dickin et al. demonstrated positive trends in healthy behavior change among parents and children participating in group-based educational workshops focused on nutrition and parenting practices. 72 Davison et al. found that providing parents with education and resources to increase physical activity with their children was effective at increasing outdoor play time and reducing indoor sedentary time compared with controls. 73 A Cochrane review found that the behavior of children with ADHD can be positively influenced after parental training intervention with the added benefits of a decrease in parental stress levels and improvements in the confidence of parents. 41 It seems evident that this kind of approach can be effective at delivering parental education.
Our results showed a positive correlation between all caregiver and child behaviors, a relationship that is supported by other studies. 41 –46,68 When parents improve their own diet, 74 –76 sleep, 77 and physical activity, 78,79 their children benefit as well. A number of studies have shown a positive correlation between parental and child weight loss in particular. 80,81 A positive change in parental body composition was found to be a significant predictor of an improvement in the child's body mass index, showing a benefit to youth when parents are actively involved in interventions related to weight loss. 81 Encouraging caregivers to make healthy choices for themselves may promote healthy behaviors in their children. Continued application of concepts by participants of the HFHK program 6 weeks or more postdelivery suggests that this program has the potential for long-term impact on healthy behaviors.
Although the “natural” focus of our program may have deterred some potential participants, it was a draw for others. Given the common use of complementary health approaches by families in North America, 82 it is wise for public initiatives such as the Ontario EYCs to collaborate with experts in these strategies, including naturopathic doctors. Naturopathic medicine is defined by principles that favor patient-centered, whole-systems, preventative, and low-force interventions (such as dietary guidance, stress management counseling, nature exposure, and herbs generally recognized as safe). 83 These values are strongly aligned with the benefits of group-based approaches. When informed by best evidence for health promotion, group visits facilitated by naturopathic doctors have great potential to improve the health of children and their families.
Strengths
The data collected represented multiple iterations of the program with different facilitators and locations, allowing for evaluation of the program independent of these other factors. The anonymity of the surveys encouraged honesty by respondents. A mixed-methods approach allowed deeper exploration of themes. Holding the focus group allowed us to query further about ways the program could be improved and made more acceptable to participants.
Limitations
There was selection bias at every stage, from those who registered, attended sessions, and participated in the survey and focus group. The response rate for the second survey and the focus group increases the risk of bias. Valuable information may have been gleaned by surveying individuals who did not participate in the program, or those who attended fewer than half the sessions. Invitations to complete survey 2 were disseminated 6 weeks postcompletion, but some responded as long as 6 months later. It is possible that too much time had passed, distorting respondents' memory of their experience. A fully iterative process 84 was not done because of a limited capacity to continue offering the program. Given that we held only one focus group, it is questionable whether saturation truly occurred. 85 Holding additional groups with purposeful sampling may have allowed for an opportunity to test emerging themes for new concepts to manifest. Demographic information was not collected, and this limits the generalizability of the study; future iterations and pilots should collect this information so that the effects on different populations are well understood. The primary investigator (L.S.) was also the developer and core facilitator of the program. This undoubtedly increased the risk of bias in the interpretation of results from both the survey tools and the focus group. The focus group was run by V.K., who was new to participants, thus reducing potential inhibition of honesty.
Next steps
Future research should focus on the efficacy of such programs in modifying behaviors. The ultimate outcome measures would include longitudinal and cohort-controlled assessment of incidence or risk of NCD, such as blood pressure, elevated body composition, glucose intolerance, or inflammatory markers in both parents and children as they get older. 86 Given the emergence of these conditions at younger ages, observing these values over time would be a helpful indicator of program effectiveness. Given the correlation between parental health and child health, assessing these values in parents may act as a proxy for children. It would be useful to determine whether this program is equally feasible and effective for participants who are not self-selected, or whether charging for the program affects engagement and/or outcome. Determining the influence of varying demographic factors may be possible with a larger sample of participants. These investigations would be comparison-controlled to accurately determine effects. Completion of a structured facilitators' manual and training program is necessary to enable skilled delivery.
Conclusion
The Healthy Family Healthy Kids program may be a feasible method of delivering primary-prevention education to caregivers, particularly in the domains of practicality and acceptability. Programs that target caregivers of young children have the potential to alter behaviors that contribute to NCD, reducing morbidity and mortality and lowering health care costs. A group-based, family-centered program such as the HFHK program may be a cost-effective means of achieving these goals, and it may prove to be a successful component of a broader public health approach to pediatric and community wellness. Future well-designed studies are needed to accurately assess the impact of the HFHK program on measurable health behaviors and outcomes in various populations.
Footnotes
Acknowledgments
The research for this article was financially supported by the Naturopathic Medical Students Association MacIntosh Junior Investigator Award, made possible by funding from Naturopathic Physicians Licensing Examinations (NPLEX). The authors greatly appreciate the input and engagement from the following individuals in the development, refinement, and delivery of the Healthy Families, Healthy Kids Program: Jennifer Keller, Alex Keller, Jiwoon Min, Emily Casey, Ana Candia, Mollie Brennan, Kaitlyn Zorn, Janine Buisman Wilcox, Samina Mitha, Vishaala Singh, Polina Kapoustina, Alexsia Priolo, Amy de Oliveira, Natalie Mulligan, and any others whom they may have overlooked. Sincere thanks are due to the staff and volunteers of the Scarborough East and Cambridge Early Years Centers, and the Boys and Girls Club of East Scarborough. Appreciation to Kieran Cooley and Paul Saunders for ongoing guidance and support. The sequence-determines-credit approach was used to determine the sequence of authors.
Author Disclosure Statement
No competing financial interests exist.
Appendix
Appendix 1
These surveys allow us to evaluate the usefulness of the Healthy Families, Healthy Kids program. All responses will be anonymous—please be as honest as you can. Please complete the survey only once—if you have more than one child, please select one child to think about for the purposes of these questions.
0–1 2–3 4–5 6 or more
0–1 2–3 4–5 6 or more My child does not have a persistent health condition
0–1 2–3 4–5 6 or more
0–1 2–3 4–5 6 or more
0–1 2–3 4–5 6 or more
0–1 2–3 4–5 6 or more
0–20 20–40 40–60 60–90 >90 My child is not independently mobile
0–20 20–40 40–60 60–90 >90
0–20 20–40 40–60 60–90 >90
0–20 20–40 40–60 60–90 >90
0–20 20–40 40–60 60–90 >90
0–20 20–40 40–60 60–90 >90
0–1 2–3 4–5 6–7 8 or more My child does not yet eat solid food
0–1 2–3 4–5 6–7 8 or more
0–1 2–3 4–5 6–7 8 or more My child does not yet eat solid food
0–1 2–3 4–5 6–7 8 or more
0–1 2–3 4–5 6–7 8 or more
0–1 2–3 4–5 6–7 8 or more
Strongly disagree Disagree Agree Strongly agree
Very satisfied Satisfied Neither satisfied nor dissatisfied Dissatisfied Very dissatisfied
Comments:
Very satisfied Satisfied Neither satisfied nor dissatisfied Dissatisfied Very dissatisfied
Comments:
Very helpful Helpful Neither helpful nor unhelpful Unhelpful Very unhelpful
Comments: