
Abstract
Objective:
The present study assessed the feasibility of a definitive placebo-controlled trial for evaluating individualized homeopathy (IH) in stage I hypertension (HTN).
Design:
Double-blind, randomized (IH: 34, placebo: 34), placebo-controlled, parallel arms, pilot trial.
Settings/Location:
National Institute of Homoeopathy, India.
Subjects:
Patients suffering from stage I HTN.
Interventions:
IH and identical-looking placebo.
Outcome measures:
Feasibility issues, blood pressure (BP) and Measure Yourself Medical Outcome Profile-2 (MYMOP-2) were assessed for 6 months.
Results:
The recruitment and retention rates were 44.4% and 85.3%, respectively. Group differences were seemingly higher in the IH group than in the placebo group.
Conclusions:
Despite challenges in recruitment, an adequately powered efficacy trial appears feasible in the future.
Introduction
Hypertension (HTN) is a frequently encountered condition in homeopathic practice 1 ; however, no randomized controlled trial (RCT) on HTN qualified for the meta-analysis of double-blind RCTs on individualized homeopathy (IH). 2 A literature review has revealed two crossover studies, 3,4 several studies with non-IH, 5 –9 use of individualized and fixed medicines, 10 one observational study, 11 two double-blind studies, 12,13 and one single-blind RCT. 14
The current trial was undertaken as an external pilot to explore the feasibility of a definitive and adequately powered future trial on IH versus placebo in stage I essential HTN, with simultaneous lifestyle management (LSM). Furthermore, the authors aimed to estimate preliminary indications of treatment effects, if any, and address feasibility issues such as screening, recruitment, and retention rate, as well as the suitability of outcome measures, and to determine the sample size for the main trial.
Materials and Methods
Trial design
This exploratory, double-blind, randomized, placebo-controlled, parallel-arm pilot trial was conducted at the outpatient department of the National Institute of Homoeopathy.
Participants
Patients with stage I HTN (8th Joint National Committee [JNC8] systolic blood pressure [SBP]: 140–159 mm Hg and diastolic blood pressure [DBP]: 90–99 mmHg 15 ; ICD-10-CM code: I10) were screened and suitably enrolled. Further details are provided in Supplementary Table S1.
Intervention
▪ Verum: Intervention involved IH in centesimal potencies at an individualized dosage. Each dose consisted of six to eight medicated globules (no. 10) of cane sugar, administered orally on a clean tongue and an empty stomach; dosage and repetition were decided by consensus among three qualified, experienced, and affiliated homeopaths. The dosage regimen was once daily for 1–2 days, followed by placebo once daily up to reassessment after 1 month. The duration of therapy was 6 months. All medicines were procured from a good manufacturing practice (GMP)-certified firm (Hahnemann Publishing Company Pvt. Ltd.).
▪ Control: This group received nonmedicated placebo globules that were indistinguishable from the verum globules. The duration of therapy was 6 months. Patients were examined by three homeopaths, as in the verum group.
General management
All randomized patients were advised regarding LSM (dietary approach to stop hypertension [DASH] instructions and daily brisk exercise for 30 min). DASH aims to reduce total calories, refined carbohydrates, and fats (not exceeding 20 g/day), with the inclusion of fiber-rich foods (whole grains, legumes, vegetables, and fruits).
Outcomes
In this pilot trial, the outcome measures assessed were feasibility issues, including recruitment, randomization, treatment, assessment of outcomes, follow-up, retention and attrition, estimation of sample size for future efficacy trials, the time needed to collect and analyze data, and short-listing of the most frequently indicated medicines. The authors assumed an a priori recruitment rate of 50% and retention rate of 80% as satisfactory. Outcome measures that would be used in a fully powered efficacy study were tested: SBP and DBP were primary outcomes and the Bengali version of the Measure Yourself Medical Outcome Profile, v.2 (MYMOP-2), questionnaire 16 was employed as the secondary outcome.
SBP and DBP were measured by blinded research assistants at baseline and every month for 6 months at fixed time points at the outpatient department using an aneroid Doctor® sphygmomanometer (SINO-JAPAN D1208) according to the recommendations of the AHA. 17 MYMOP-2 was measured at baseline and every 2 months for 6 months.
Sample size
As the trial by Saha et al. 13 included patients at all HTN stages, it could not be utilized for effect size calculation. Simultaneously, as both groups were highly likely to improve from the combined effects of homeopathic consultations and LSM advice and the nature of the disease itself, a small adjunctive effect (Cohen's d = 0.2) was possible. To detect a statistically significant difference between two independent means (two groups) of blood pressure (BP) after 6 months of intervention using an unpaired t-test, a study with 2 × 394 patients would result in 80% power based on a two-sided significance level of 5%. Achieving at least 8%–10% of this (63–79) seemed feasible.
Randomization
A random sequence was generated by permuted block randomization, maintaining 1:1 allocation by a third party using the StatTrek random number generator available to the blinded pharmacist in coded form only for dispensing from coded vials as per prescriptions.
Blinding
Double blinding was adopted; patients, investigators, outcome assessors, and data entry operators remained blinded throughout the trial.
Allocation concealment
This was established by using identically coded containers (coded 1 and 2, either for medicine or placebo, assigned randomly and confidentially by a third party).
Statistical method
Descriptive statistics were used for feasibility evaluation. The intention-to-treat (ITT) approach was adopted by replacing missing values with regression means. The nature of the pilot trial addressing feasibility issues, intragroup changes, and intergroup differences was presented using descriptive statistics only; no p values were reported. Statistical analysis was performed using the Statistical Package for the Social Sciences (version 20.0; IBM Corp., IBM SPSS Statistics for Windows, Armonk, NY, USA). The study was conducted in accordance with the Declaration of Helsinki and adherence to the International Conference on Harmonization Guidelines for Good Clinical Practice. Reporting adhered to the CONSORT extension statement for randomized pilot trials 18 and RedHot 19 guidelines for reporting trials (Supplementary Files S1 and S2).
Adverse events
Patients were instructed to report adverse events either directly or over the phone.
Results
Participant flow
Of 153 hypertensive patients who were screened, 85 were excluded (reasons listed in Fig. 1) and 68 were enrolled and subsequently randomized. Overall, 10 patients dropped out (verum: 6, control: 4) and 58 completed the trial (Fig. 1).
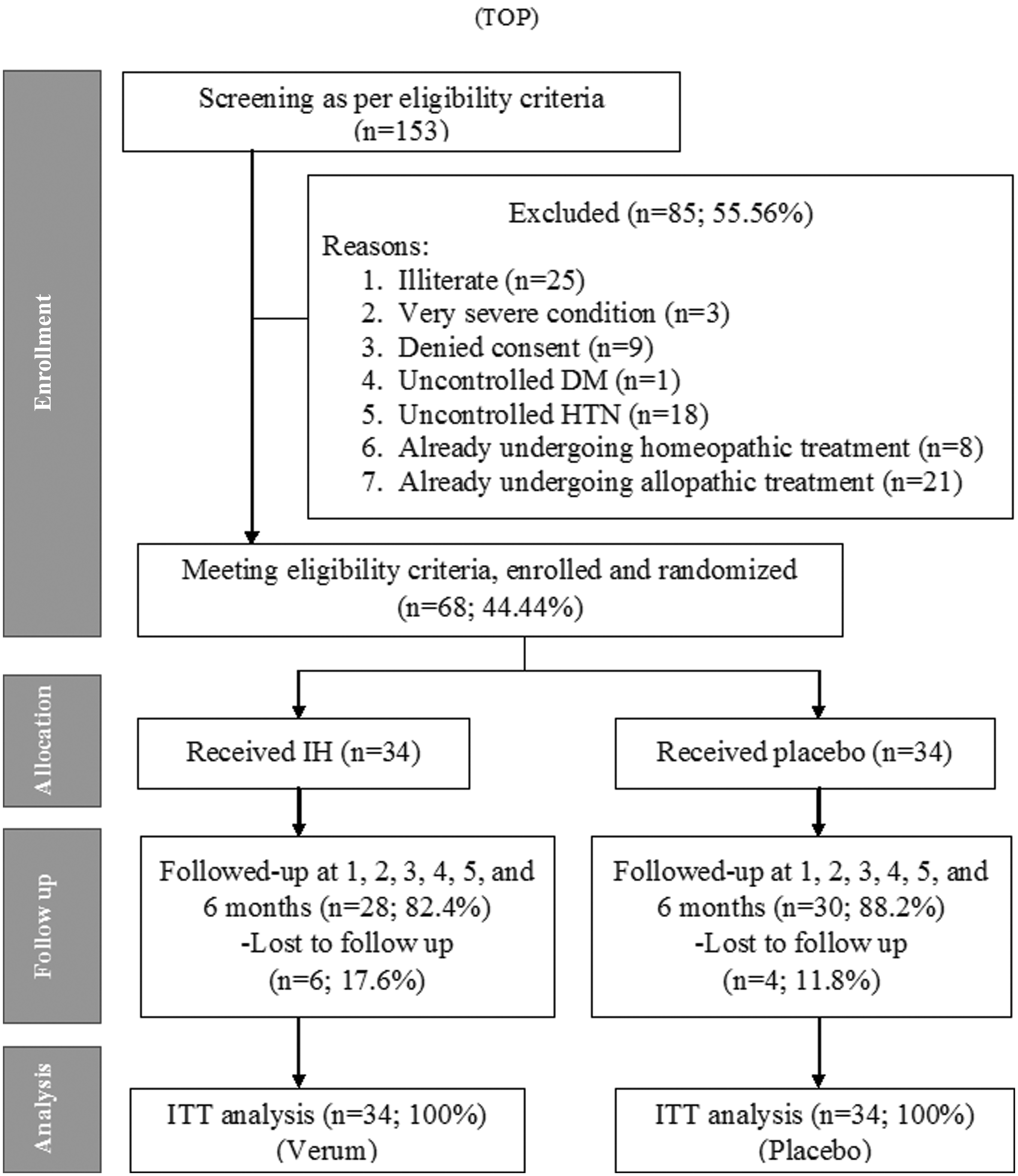
Study flow diagram.
Recruitment
This feasibility study included a 10-month recruitment phase from March to December 2018, followed by a 6-month treatment phase.
Baseline data
The distribution of different sociodemographic variables, BP, and MYMOP-2 was assessed at baseline (Supplementary Tables S2 and S3).
Numbers analyzed
All randomized patients (n = 68) were entered into the final analysis.
Outcomes and estimation
A recruitment rate of 44.4% was suboptimal and needed improvement. The major reason was illiteracy; 16.3% of screened individuals were illiterate; thus, completion of the MYMOP-2 questionnaire was impossible. A retention rate of 85.3% was acceptable. Retention rates in the verum and control groups were 82.4% and 88.2%, respectively (Fig. 1), which were statistically nonsignificant (Yates χ 2 = 0.117, p = 0.732). No obstacles were encountered during randomization, double blinding, outcome assessment, and follow-up. Compliance was achieved by providing telephonic reminders. Intragroup changes in mean BP and MYMOP-2 scores were seemingly higher in the IH group than the placebo group (Tables 1 and 2). Furthermore, mean differences in BP and MYMOP-2 scores were higher in the IH group than in the placebo group (Tables 1 and 3).
Systolic Blood Pressure and Diastolic Blood Pressure at Different Time Points in Two Groups and Group Differences (N = 68)
CI, confidence interval; DBP, diastolic blood pressure; SBP, systolic blood pressure; SD, standard deviation; SE, standard error.
Intragroup Changes in Measure Yourself Medical Outcome Profile-2 Measures at Different Points of Time
Group Differences in Measure Yourself Medical Outcome Profile-2 Between Groups Over Different Time Points
MYMOP, Measure Yourself Medical Outcome Profile.
Medicines used
The most frequently used therapeutic agents were Pulsatilla nigricans (n = 11; 16.2%), Natrum muriaticum (n = 10; 14.7%), and Thuja occidentalis (n = 8, 11.8%) (Supplementary Table S4 and Supplementary File S3).
Adverse events
No severe adverse event was reported in either group. A transient rise in BP was reported equally in seven patients in each group after administering the homeopathic medicine, with mild intensification of symptoms 1 and 2 of MYMOP-2 noted in 12 cases in the verum group and 1 case in the placebo group.
Discussion
Herein, the authors performed a double-blind pilot RCT in 68 patients with stage I HTN and compared IH with placebo while undertaking LSM to assess the feasibility of a larger future trial exploring the efficacy of IH against placebo. Group differences in outcomes were seemingly greater in the IH group than in the placebo group, which might be attributed to the mild and autoregressive nature of the disease condition itself, as well as combined effects of medicines or the placebo/context effect along with DASH and LSM measures. These were common in both groups and might have reduced the differences between groups. Although it is difficult to draw more than the relatively limited set of conclusions, an adequately powered definitive trial seemed achievable in the future.
The major strengths of the current trial were double blinding, randomization, ITT analysis, and adherence to classical homeopathic principles. Post hoc power calculation revealed a power compromise of up to 15%, warranting cautious interpretation of results. A run-in period may be maintained before inclusion in future trials, and patients showing spontaneous improvement can be excluded. Compared with the BP at baseline, after 6 months of treatment, SBP values in the verum and control arms were 137.9 ± 16.4 and 142.2 ± 21.3, respectively. The estimated effect size was 0.226. To detect statistically significant differences between two independent means of SBP using the unpaired t-test, a study with 2 × 308 patients will provide 80% power based on a two-sided significance level of 5%. Provision of a 15% attrition rate would further inflate the sample to 708 (2 × 354).
If DBP was included in the calculation (verum: 89.9 ± 9.3; control: 88.8 ± 10.1, d = 0.113, α = 0.05, power 80%, and attrition rate 15%), the sample size would be 2816 (2 × 1408). After 6 months, mean reductions achieved in SBP were 15.5% and 9.7% in the verum and placebo groups, respectively. For DBP, mean reductions in the verum and placebo groups were 5.5% and 5.4%, respectively. The minimal clinically important difference (MCID) is a 20 mm reduction in BP. 20 This MCID could not be achieved in the present trial, hence sample size calculation was not based on MCID, but it should be considered in future trials to reach valid conclusions.
Trial recruitment was challenging owing to the inherent problem of illiteracy. Furthermore, even the exclusion of illiterate subjects appeared inadequate. During the recruitment process, it was necessary to specify the restriction of these individuals from trial participation. Future trials need to implement processes to account for this issue, for example, a systematic recruitment strategy, including adequate referrals from colleagues and other outpatient departments, as well as ensuring media presence to publicize the trial. Few patients were dissatisfied with the randomization process that could allocate them to the placebo arm. The authors took additional measures to improve trial recruitment when it was evident that recruitment was slow, including verbal reminders to each referring practitioner, regular WhatsApp group message reminders during clinical hours, and posters in waiting areas and on walls of outpatient departments. As per Lasagna's law, 21 although physicians are overly optimistic regarding patient recruitment, it is a common obstacle to randomized trials. A low recruitment rate and low power raise the challenge of generalizability of findings of any efficacy trial. Underpowered studies are prone to produce false positive results, thus they increase the chance of inflated effect size estimates and reduce the reproducibility of findings. 22
From a practical standpoint, a limited number of 85 homeopathic medicines in three different centesimal potencies (30CH, 200CH, and 1000CH) were available for the trial, although on interviewing subjects, several other medications could have been indicated; however, this was not the case. This was a useful finding in terms of feasibility, but could become an issue in a larger trial. This indicates that the number of medicinal agents could have impacted enrollment.
Furthermore, the outcome of a homeopathic prescription depends largely on the homeopath's skill, hence the consensus method was preferred over assessment by a single homeopath for a more representative appraisal of the homeopathic method employed. The medicines utilized were considerably similar to those employed by Saha et al. 13 and Varanasi et al. 14 Previously, two crossover trials have been reported: both had IH in one arm, with standard therapy 3 or placebo in the other. 4 The former revealed an average reduction of 4.25 mmHg in terms of BP in the homeopathy group versus 8.75 mmHg with standard therapy. Significant improvement was recorded in the homeopathy group when compared with the placebo group.
In a double-blind RCT of 68 patients with mild-to-moderate HTN, homeopathy was successful in 82.2% versus 56.7% in the placebo group. 12 The current study implemented a few improved research methods when compared with the report by Saha et al., 13 including a homogeneous sample of stage I HTN to enhance internal validity, a computerized random number chart to replace a quasi-randomization technique of the coin toss method, blinding by using coded and identical vials in place of pharmacy-controlled randomization, and the use of MYMOP-2 as a possible outcome measure for future trials. The trial by Varanasi et al. 14 was similar, but utilized a single-blind design, which remained unjustified with a poor recruitment rate of only 10.2%.
Overall, the authors assessed feasibility issues of an adequately powered efficacy trial to identify and resolve problems in advance and to ensure that the future trial runs smoothly, maintaining every possible quality aspect and qualifying for meta-analysis.
Conclusion
Although recruitment difficulties were identified, adequately powered trials appear possible in the future.
Ethical Statement
The study protocol was approved by the Institutional Ethics Committee (IEC) [Ref. No. 5-23/NIH/PG/Ethical Comm. 2009/Vol 5/2590 (A/S); dated March 06, 2018] and registered prospectively in the Clinical Trials Registry–India before enrollment of patients and had a secondary identifier—UTN of U1111-1210-5392. The trial protocol (synopsis) and full project report (dissertation) were submitted as the postgraduate thesis of the corresponding author. Each patient was provided with a patient information sheet in local vernacular Bengali, detailing the objectives, methods, risks and benefits of participating, and confidentiality issues. They were enrolled in the study after obtaining written informed consent.
Footnotes
Acknowledgments
The authors are grateful to institutional heads, both academic and hospital sections, for allowing them to conduct the trial. They sincerely thank the fellow postgraduate trainees, staff, pharmacists, and patients for their sincere participation in the study.
Authors' Contributions
S.S. and S. Singh were involved in concept, literature search, clinical study, data acquisition, data interpretation, and preparation of the article; J.M., P.M., M.P., A.N., N.M., N.K., A.B., and S.S.A. were involved in clinical study and data acquisition; and M.K. and S. Saha were involved in design, data interpretation, statistical analysis, and preparation of the article. All authors reviewed and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary File S1
Supplementary File S2
Supplementary File S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.