
Abstract
Objectives:
Healthcare organization leaders' support is critical for successful implementation of new practices, including complementary and integrative health (CIH) therapies. Yet little is known about how to garner this support and what motivates leaders to support these therapies. We examined reasons leaders provided or withheld support for CIH therapy implementation, using a multilevel lens to understand motivations influenced by individual, interpersonal, organizational, and system determinants.
Design and setting:
We conducted qualitative interviews with leaders in seven Veterans Health Administration medical centers that offered at least three CIH therapies to Veterans and were identified as early adopters of CIH therapies.
Subjects:
Participants included 12 executive leaders and 34 leaders of key clinical services, including primary care, mental health, physical medicine and rehabilitation, and pain.
Measures:
We used a thematic analysis to examine leaders' narratives of barriers and facilitators to implementation including their attitudes toward CIH therapies, perceptions of evidence, engagement in implementation, and decisions to provide concrete support for CIH therapies. Drawing from Greenhalgh's Diffusion of Innovation framework, we organized themes according to the influence of individual determinants, two levels of inner setting, and outer system context on CIH implementation.
Results:
Leaders' decisions to provide or withhold support were driven by considerations across multiple levels including (1) individual attitudes/knowledge, perceptions of evidence, and personal experiences; (2) interpersonal interactions with trusted brokers, patients, and loved ones/colleagues/staff; (3) organizational concerns surrounding relative priorities, local resources, and metrics/quality/safety; and (4) system-level policy, bureaucracy, and interorganizational networks. These considerations interacted across levels, with components at organizational and system levels sometimes prevailing over individual perceptions and experiences.
Conclusions:
Garnering leaders' support for CIH therapy implementation should address their considerations at multiple levels. Implementation strategies designed to shift individual attitudes alone may be insufficient for securing leaders' support without attention to broader organizational and system-level contextual issues.
Introduction
Healthcare organization leaders, including executive and clinical department leaders, are critical for new health care practice implementation. 1 –5 Leaders provide resources, create cultures of innovation, champion evidence-based practices, and encourage staff engagement, 3,6 –8 thereby creating a positive climate for innovation and practice implementation. 9,10 In safety net settings, such as the US Department of Veterans Affairs healthcare System (VA), this support may additionally help overcome financial and organizational constraints that further challenge implementation. 11
Complementary and integrative health (CIH) therapies, such as acupuncture, yoga, and meditation, 12 are increasingly being incorporated into healthcare policy and systems 13 –16 including the VA. 17 –19 This reflects a growing evidence base and increasing patient demand for nonpharmacologic and nontraditional healthcare options. 20 –24 In 2017–2018, VA medical centers (VAMCs) offered an average of five CIH therapies, 25 and VA policy now mandates coverage for eight evidence-based CIH therapies. 19 Yet, while CIH therapy offerings are expanding within healthcare systems, implementation challenges remain. 26,27
Healthcare leaders' support for CIH therapies is instrumental for successful implementation. 28 –32 However, little is known about how to garner such support and what motivates leaders' provision or withholding of support. In two prior studies, leaders identified individual knowledge/attitudes toward CIH, perceptions of patients, traditional medical culture, champions, and organizational issues as barriers or facilitators to CIH implementation. 28,32 Yet how these barriers/facilitators may influence leaders' decision-making has not been fully explored. Therefore, we sought to examine leaders' reasons for providing or withholding concrete support for CIH in early adopting VAMCs.
Methods
Study design
We conducted semi-structured qualitative interviews at seven VAMCs as part of a larger study on barriers and facilitators to CIH implementation. 26 These sites were selected as early adopters that had successfully implemented at least three CIH therapies, consistent with VA policy during data collection, 33 based on screening interviews with CIH program heads. They varied in geographic location, rural/urban status, and size. The VA Bedford Healthcare System Institutional Review Board determined that this study was consistent with program evaluation for quality improvement purposes.
Participants
This analysis focused exclusively on interviews conducted with 12 executive and 34 leaders of key clinical services. We worked closely with contacts (often CIH providers) at each site to identify at least two local executive and department-level leaders from services that interfaced frequently with CIH, including at least primary care, mental health, physical medicine and rehabilitation, and pain (Table 1). All invited participants agreed to participate and provided verbal consent.
Sites and Study Participants
Types of leaders represented: aMedical Center Director; Associate Medical Center Director; Chief of Staff; Deputy Chief of Staff; Associate Director of Patient Care Services.
Directors/chiefs/leaders of: Medicine or Medical–Surgical Services; Primary Care Women's Health; Mental Health; Behavioral Health; Psychology or Psychiatry; Social Work; Pain or Integrated Pain; Neurology; Urgent Care; Geriatrics; Extended Care and Rehabilitation; Physical Medicine and Rehabilitation; Recreation and Creative Arts Therapies.
Data collection
Two 2-person teams experienced in qualitative methods conducted in-person interviews using a flexible semi-structured interview guide informed by Greenhalgh's Diffusion of Innovation in Service Organizations model. 34 Like other compilations of implementation determinants, 35 this model encompasses domains that influence implementation including individual characteristics of adopters, aspects of the organizational setting (antecedents, readiness, communication, and influence), and the outer context of the larger system in which the organization exists. As such, the interview guide included questions designed to understand the influence of individual determinants, inner setting, and outer context on CIH implementation. We specifically asked about leaders' awareness of CIH offerings, attitudes toward CIH, perceptions of evidence, leaders' engagement in CIH implementation, and implementation barriers/facilitators. Leaders described their own experiences as well as their perceptions of other leaders at their sites. Interviews lasted up to 1 h, were audio-recorded, and transcribed.
Data analysis
Following data collection, we conducted a thematic analysis 36,37 focused on leaders' support for CIH implementation. Three team members reviewed transcripts to inductively develop emergent codes from the data, followed by an iterative process to refine codes and resolve differences through consensus discussions. Remaining transcripts were independently coded and reviewed using constant comparison to ensure coding consistency, collaboratively developing new codes as needed. We then grouped codes into broader thematic categories that captured leaders' motivations for providing or withholding support for CIH implementation, drawing on Greenhalgh's concepts of individual determinants, inner setting, and outer context to synthesize and interpret our emergent themes.
Results
We found that leaders' were persuaded by considerations across multiple levels of Greenhalgh's model: (1) individual attitudes/knowledge, perceptions of evidence, and personal experiences; two aspects of inner setting including (2) interpersonal interactions with trusted brokers, patients, and loved ones/colleagues/staff; (3) organizational concerns surrounding relative priorities, local resources, and metrics/quality/safety; and (4) outer system context including policy, bureaucracy, and interorganizational networks (Fig. 1). Below, we describe how each level influenced leaders' motivations, with additional quotes in Table 2. We indicate instances in which considerations interacted to influence leaders' support.
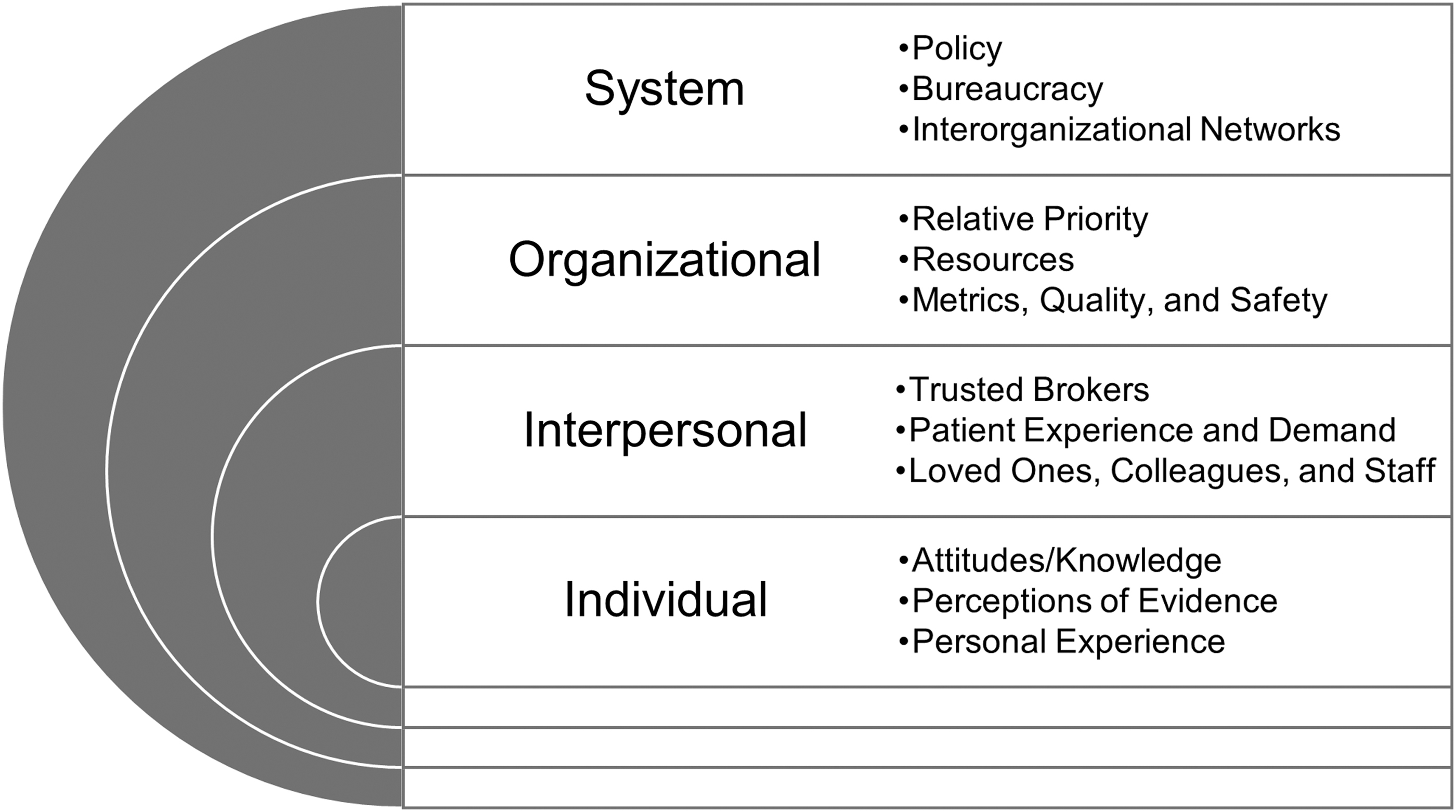
Multilevel considerations influencing leaders' decisions to support CIH implementation. CIH, complementary and integrative health.
Exemplar Quotes of Key Themes Mapped to Multilevel Concepts
CIH, complementary and integrative health.
Individual level
Individual considerations that influenced leaders' decision-making included attitudes/knowledge regarding CIH, perceptions of the evidence, and leaders' own experiences engaging in CIH therapies.
Attitudes/knowledge
Leaders expressed variable knowledge about CIH, ranging from expertise to limited awareness. While several participants had not been exposed to CIH therapies in their past educational or employment experiences, many described themselves as “open-minded” and “believers” of at least some therapies. Skepticism was present but tempered by a belief that CIH would not harm patients: “I think there's probably a spectrum of belief in, and non-belief in, the more Eastern integrative health stuff … we're going to be more skeptical … But as long as it's not hurting our patients … and I don't believe that any of us think this is harmful. (Associate Chief of Medicine, Site 3).” Leaders also described shifting perceptions, sharing sentiments such as “I used to be a skeptic,” while now developing a growing awareness and acceptance of CIH.
Perceptions of the evidence
Empirical evidence for CIH motivated leaders to endorse and actively support implementation. “I think our Chief of Staff would probably respond to more the empirical stuff … they can ground their decisions in those academic things. (Mental Health Director, Site 1)” Yet, while randomized controlled trials were valuable to leaders, they recognized that the evidence for CIH was still growing. Subsequently, evidence from other sources including business case analyses, “n of one” trials, and local utilization were also influential.
Personal experience
Personally experiencing CIH therapies swayed many leaders' decisions to provide support. “I have always kind of been a skeptic … (until I) actually got to see some of it in action … I started actually going to acupuncture … I was doing yoga twice a week (at a recent federal leadership training) … To change a skeptic, you have to put them in there and show them what it's going to do … it's hard to say ‘Well, I love yoga, I support it,’ if you've never done something like that before. (Associate Director, Site 7)” Many participants described how personal experiences positively shifted their perceptions and underscored their decisions to adopt CIH locally.
Interpersonal level
Interpersonal interactions with others influenced leaders' decision-making by reshaping attitudes, communicating evidence, demonstrating demand, and navigating barriers.
Trusted brokers
Individuals delivering CIH and heading its implementation played a crucial role in leaders' provision of support. Leaders' highlighted these individuals' abilities to develop programs and bridge communication between biomedical and holistic providers, and across different leaders. They were lauded for their business skills, knowledge, and credibility, garnering leaders' support for their CIH programs. One Chief of Staff raved, “I have to tell you that Dr. (CIH contact), she is very special … she is really a most dedicated professional … has really grown the program … (and) is very credible. (Site 6).” Leaders' provision of resources for CIH resulted from these individuals' abilities to communicate evidence, coordinate implementation, present strategic plans, and conduct return on investment analyses. These trusted brokers helped mitigate negative attitudes and navigate barriers: “It seems a little far-fetched … (but) when Dr. (chiropractor) got here he taught us … scientifically what's going on … he can speak intelligently about what he does … it was not hocus pocus. (Rehabilitation Chief, Site 7).”
Patient experience and demand
Patient demand for CIH prompted implementation, with several leaders reporting that “patients were asking for it.” It also helped sustain CIH offerings. Patients at one site successfully “raised a stink” with executive leaders when they considered discontinuing services, whereas another site leader noted, “Once it becomes ingrained and patients really love it, you're not going to be able to take it away. (Chief of Staff, Site 5).” Patient experiences were also persuasive, with one Mental Health Director reporting: “Our (hospital) director … likes hearing the Veteran experience … I think administrators and politicians deal with the ends of the bell curve, those are the stories that they hear … our director responds to ends of the curves. (Site 1).” These positive interpersonal interactions were especially influential when they converged with leaders' perceptions of evidence. “I think the most powerful response is to have a patient who has had a great response … if you can present evidence and if then you can have a patient come in and tell their story. Then you get the emotional side of it. (Chief of Staff, Site 3)” Finally, a desire to keep patients satisfied mitigated skepticism and motivated leaders to support CIH. As one Chief of Staff described, “If you think it's quackery … it doesn't matter … You can dangle a crystal … and if it doesn't do a damn thing, it doesn't matter. What matters is the patient feels better when you're done. (Site 4).”
Loved ones, colleagues, and staff
Leaders' decisions to support CIH were swayed by loved ones, colleagues, and staff. For example, observing positive impacts of CIH in others prompted adoption: “I've seen a lot of the benefits of tai chi and I've seen how the employees really enjoyed it … so why wouldn't we offer it … I just decided that we should try for it. (Chief of Staff, Site 5).” Positive perceptions of CIH and its effects on loved ones also helped diminish skepticism: “I used to be very skeptical. My daughter is a triathlete … she would lose her breath to the point that she could barely finish her race … (then) she went for deep tissue massage … and she hasn't had a problem since … It's curative. (Pain Director, Site 7).”
Organizational level
Organizational considerations, including organizational priorities, availability of resources, and quality/safety metrics, influenced leaders' support for CIH.
Relative priority
Leaders supported CIH when it aligned with organizational priorities, with chronic pain and opiate deprescribing being particularly salient. For others, CIH was appealing when perceived as a mechanism to address other operational priorities such as “employee engagement, operational excellence, and cultural transformation.” Yet leaders had to balance the multiple priorities facing their healthcare organizations and departments, with CIH not always rising to top of the priority list: “I was told, ‘How can we offer yoga when people aren't getting their colonoscopies?’ … the director now has so many eggs in the basket that she can't fry, she's not going to start yoga, or acupuncture. (Women's Health Director, Site 1).”
Local resources
Limited resources influenced leaders' support: “With the budget situation … we can't really expand CIH … when you've got a king-sized bed and a queen-sized sheet and you pull the covers one place, somebody is going to get cold in the middle of the night. (Director, Site 5).” Leaders also contended with limited staff time: “I want to incorporate acupuncture … (but) if I have (my two anesthesiologists) do acupuncture, who's going to run the operating room? (Pain Chief, Site 1).” Concerns about limited resources led some leaders to express concerns about offering CIH, particularly for hands-on therapies: “We can't pay for it forever for you to get your back rubbed. (Rehabilitation Chief, Site 7).” Yet, patient demand helped assuage these concerns even when budgets were tight: “The facility … said, ‘Okay, yeah. You've proven that you have the patient demand. There's the medical benefit … We will support a chiropractor position for you.’ (Rehabilitation Administrative Officer, Site 4).” Furthermore, while many leaders perceived CIH as competing for available resources, some leaders considered how CIH could generate revenue. As such, return on investment and business case analyses motivated leaders to adopt/expand CIH. “(If) we can eventually demonstrate if we actually approved all the (non-VA service) requests, that's what it would cost you, and then eventually you can say, is it worth (paying for service in the community) when you can build capacity (internally)? (Pain Chief, Site 1).”
Metrics, quality, and safety
The ability to meet facility metrics, quality standards, and to safely deliver CIH was critically important to many leaders. “There was a question of infection control with the acupuncture needles. And all of a sudden it hit me … I'm supposed to be in charge of (acupuncture), but I don't even know what they do with the needles …. That sounds stupid, but how would I know that (the needles were disposable)? (Primary Care Chief, Site 7)” Access metrics were of particular concern due to “insatiable demand” and insufficient resources. “You start (CIH) … and then all of a sudden, wait, people really like this … and then we get the report … ‘you have this delinquent program that exists.’ (Primary Care Chief, Site 7)” While leaders could resolve access concerns by referring patients to community-based CIH, they were also concerned that CIH therapies outside the VA were not delivered in a high quality and safe manner: “It really hurts when one of my biggest back log clinics is therapeutic massage … (but) I'm not sure that it's a good thing to … let (patients) go (into the community) … when I have real questions about the quality of care. (Chief of Staff, Site 3).”
System level
System-level policy, bureaucracy, and interorganizational networks comprised outer context considerations that influenced leaders' decision-making.
Policy
For some leaders, legislation, VA policy, and initiatives arising from policy prompted CIH implementation and facilitated buy-in. According to one Chief of Staff, “The demand for the integrative health services has dramatically grown … directly related to the opioid safety (policy) and trying to reduce the use of long-term opioid therapy. (Site 3).” Others noted that once CIH becomes a priority for VA Central Office, then sites will be “scurrying around” to implement it. Finally, a few participants mentioned that “if there's enough interest on Capitol Hill,” then CIH would be prioritized.
Bureaucracy
Bureaucratic barriers disincentivized CIH implementation. Leaders lamented challenges related to hiring, credentialing, and reimbursement requirements in the VA, which stymied implementation even when leaders were otherwise motivated to provide support. A Mental Health Chief noted, “We didn't have a lot of success with that because … it's the government … we could buy a tank probably, but we can't get pencils. So that sort of hit a dead end (with yoga). (Site 4).”
Interorganizational networks
CIH implementation occurring in other VAMCs also encouraged buy-in for CIH. A Rehabilitation Chief noted that executive leaders at his facility took notice of CIH after receiving a letter from another facility that had implemented CIH. Leaders also looked to other organizations for examples of how best to implement CIH, visited other organizations to learn from them, and used CIH as an opportunity to positively distinguish their VAMC from others: “This facility sees itself as being special … we're a little rural place. There are no major universities nearby, so we're not gonna be a big research facility. We're not gonna be doing heart transplants. (CIH is) a way to be a little different and distinguish ourselves. (Mental Health Chief, Site 4).”
Discussion
We found that leaders' provision of support for CIH in early adopting health care facilities was driven by considerations at multiple levels of health care organizations, including individual perceptions and experiences, interpersonal interactions, organizational concerns, and system-level influences external to the site. Multilevel concepts have been incorporated in prior frameworks to understand implementation, with leaders' support often identified as an inner setting concept in these models. 34,35,38,39 Yet, individual leaders in our study supported CIH therapies for reasons beyond just inner setting considerations. These findings provide a more nuanced understanding of leaders' role in implementation and their motives for providing or withholding support for new practices. As health care organizations, researchers, and practitioners seek to implement new practices, they should consider the multifaceted and multilevel nature of leaders' considerations and how these inform implementation. Such understandings can provide insight into sources of leverage to garner support.
While factors within different levels informed leaders' perceptions of CIH and support, we also found important interactions between levels, with considerations at organizational and system levels often overriding individual-level skepticism of CIH. Leaders' positive or negative beliefs about CIH did not always prevail in their decisions. While empirical evidence was important to leaders in our study, unwavering belief in CIH was not necessary for their provision of support. In fact, several leaders in our study expressed reservations about some CIH therapies, yet still supported overall implementation efforts when CIH was linked with hospital priorities, championed by others, or demanded by patients. These organizational-level considerations and interpersonal interactions helped shift buy-in and garner support from leaders. Alternately, even when leaders endorsed CIH, they had to weigh the adoption of new therapies or expansion of existing offerings with hospital policies and other priorities competing for resources. These findings have important implications for implementation initiatives. While individual perceptions of CIH inform support, leaders act within the context of an organization that has its own priorities and strategies. As such, implementation strategies designed to promote buy-in by shifting attitudes may be insufficient in settings where concerns about competing priorities and resources prevail, and unnecessary in settings where the practices being implemented are aligned with existing priorities and stakeholder demand.
Leaders in our study were particularly influenced by individuals responsible for CIH implementation in their facilities. These dynamic individuals served as trusted brokers who were business-minded, respected, and spanned boundaries between traditional providers and holistic services. As a result, leaders entrusted them with CIH implementation, provided needed resources, and engaged with them to develop sustainable CIH programs. As healthcare organizations develop CIH programs, selecting respected individuals to lead implementation can raise legitimacy. This finding reflects the importance of organizational context in influencing leader support of implementation.
Limitations
Sites included in this study had all experienced success implementing at least three CIH therapies. While participant narratives provided insight into why leaders support CIH therapies, as well as barriers encountered that precluded their support, there may be additional reasons for not supporting CIH among leaders at sites that have not successfully implemented any therapies. Furthermore, within the organizations we studied, we predominantly spoke with leaders who had some involvement in implementation, limiting our understanding of leaders who do not support CIH implementation. Finally, the VA context is unique, with bureaucratic challenges not always faced by private healthcare organizations, and policy supporting CIH provision that private healthcare systems and payers are only beginning to consider.
Conclusions
Highlighted in multiple implementation frameworks, 34,35,40 –42 leaders' support is critical for the successful implementation of new practices, including CIH. Our study extends existing understandings of leaders' support for implementation and provides insight into factors that influence their decision-making to provide support. Importantly, as healthcare systems continue to seek leaders' support for CIH, implementation strategies must attend to broader organizational priorities and system-level challenges beyond individual characteristics alone. Anchoring implementation efforts in what matters most to leaders can foster their provision of support.
Footnotes
Authors' Contributions
R.E.B. had full access to all aspects of this study and takes full responsibility for this article. Concept and design: S.L.T., B.G.B., A.R.E., and R.E.B. Data collection: S.L.T., R.E.B., and K.D. Data analysis: R.E.B., K.D., and J.W. Data interpretation: R.E.B., K.D., J.W., B.G.B., A.R.E., M.C., and S.L.T. Drafting of the article: R.E.B., K.D., and J.W. Critical revision of the article for important intellectual content: R.E.B., K.D., B.G.B., M.C., A.R.E., and S.L.T. All the authors reviewed and approved the final article.
Disclaimer
The views expressed in this article are those of the authors and do not represent the views of the U.S. Department of Veterans Affairs or the United States Government.
Acknowledgment
We thank Dr. Alexis Huynh for her contributions to data collection.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Funding for this work was provided by the U.S. Department of Veterans Affairs Office of Patient-Centered Care and Cultural Transformation, and the Quality Enhancement Research Initiative, grant no.: PEC 13-001.