
Abstract
Background:
Tai Chi (TC) is a traditional Chinese martial art with demonstrated beneficial effects on physical and mental health. In this study, the authors performed a systematic review to assess the efficiency of TC in different populations' cognitive function improvement.
Design:
The present systematic review utilized the Chinese National Knowledge Infrastructure (1915-), Wanfang (1998-), VIP (1989-), Chinese Biomedicine databases (1978-), PubMed (1950-), Web of Science (1900-), Cochrane Library (1948-), Embase (1974-), EBSCOhost (1922-), and OVID (1996-) databases to search and identify relevant articles published in English and Chinese from the beginning of coverage through October 17, 2020. Randomized controlled trials (RCTs) published from the beginning of coverage through October 17, 2020 in English and Chinese were retrieved from many indexing databases. Selected studies were graded according to the Cochrane Handbook for Systematic Reviews of Intervention 5.1.0. The outcome measures of cognitive function due to traditional TC intervention were obtained. Meta-analysis was conducted by using RevMan 5.4 software. We follow the PRISMA 2020 guidelines.
Results:
Thirty-three RCTs, with a total of 1808 participants, were included. The study showed that TC could progress global cognition when assessed in middle-aged as well as elderly patients suffering from cognitive and executive function impairment. The findings are as follows: Montreal Cognitive Assessment Scale: mean difference (MD) = 3.23, 95% CI = 1.88–4.58, p < 0.00001, Mini-Mental State Exam: MD = 3.69, 95% CI = 0.31–7.08, p = 0.03, Trail Making Test-Part B: MD = −13.69, 95% CI = −21.64 to −5.74, p = 0.0007. The memory function of older adults assessed by the Wechsler Memory Scale was as follows: MD = 23.32, 95% CI = 17.93–28.71, p < 0.00001. The executive function of college students evaluated by E-prime software through the Flanker test was as follows: MD = −16.32, 95% CI = −22.71 to −9.94, p < 0.00001.
Conclusion:
The TC might have a positive effect on the improvement of cognitive function in middle-aged and elderly people with cognitive impairment as well as older adults and college students.
Introduction
The term cognitive function is derived from the word cognition. Cognition denotes the internal mental progressions explained in cognitive psychology, which is a sub-topic of psychology. It comprises numerous mental capacities, such as memory, attention, executive functions, mental processing speed, language, visual-spatial skills, and fine motor dexterity. 1,2 In most healthy individuals, especially in early childhood, the brain can learn new skills to develop personal and individual thoughts about the world. Humans are usually equipped with a capability for cognitive function from birth. This indicates that an individual is capable of learning or memorizing a certain amount of information. Over time, parameters such as aging and illnesses can cause impairment to several cognitive functions, including memory, processing speed, learning, understanding, and decision making. This has posed a serious health concern for the public in recent years. 3 Hence, prevention or therapy for cognitive dysfunction employing highly efficient strategies is extremely imperative and crucial.
The interventions considered to improve cognitive function chiefly comprise intervention for risk aspects, physical exercise, dietary intervention, cognitive training, acupuncture, acupoint massage, repeated transcranial magnetic stimulation, and drug therapy. However, more and more evidence suggests that aerobic exercise positively affects cognition. 4 –6
Tai Chi (TC) is a traditional Chinese martial art and a kind of mind and body coordinated exercise. The TC exercise chiefly comprises various actions such as stretching and relaxation of skeletal muscles and body coordinated movements, regular breathing, and meditation. The TC is very popular; according to incomplete statistics, hundreds of millions of people have practiced TC in more than 150 countries and regions around the world. 7 Several researchers have established that TC has a beneficial effect on health, including physical and mental health. 8 –10 A review published in 2015 included both randomized and non-randomized controlled trials (RCTs) in healthy adults. 11 A systematic assessment of TC intervention on cognition was performed, which focused only on the effect of TC on older adults' cognitive performance, which employed active control groups, and the comparison parameters included western group exercise, stretching, and toning, a combination of resistance and non-resistance training. 12 A review performed in 2018 involved assessing traditional systems of exercises, TC, qigong, Yoga, and/or Pilates on the performance of cognition in elderly patients. 13
A systematic review (2020) assessed the effect of TC intervention on the cognitive function of the elderly with cognitive impairment; another review (2020) included RCTs in determining whether TC is effective in slowing cognitive decline in older populations with mild cognitive impairment (MCI). 14,15 Another systematic review (2020) included RCTs and quasi-experimental studies in older adults with MCI, which focused on the influence of TC and qigong mind–body exercises on both motor and non-motor function and the quality of life. 16
However, all studies in these reviews included only a single specific kind of participants, randomized and/or non-randomized design, and studied TC with other interventions. Therefore, this systematic review aims at evaluating the efficacy of TC on cognition performance among the available data from RCTs. This review also included only studies that assessed the TC group versus the non-TC group (control group) with an anticipation that the outcome of the present review will offer the practitioners with program designs to improve cognitive performance, provide stronger evidence-based medical evidence to fully prove the impact of TC on the cognitive function of adults. Supplementary Material for this article is available online.
Methods
Search strategy
The present systematic review utilized the Chinese National Knowledge Infrastructure (1915-), Wanfang (1998-), VIP (1989-), Chinese Biomedicine databases (1978-), PubMed (1950-), Web of Science (1900-), Cochrane Library (1948-), Embase (1974-), EBSCOhost (1922-), and OVID (1996-) databases to search and identify relevant articles published in English and Chinese from the beginning of coverage through October 17, 2020. The method of retrieval was customized to meet the characteristics of each database mentioned earlier. Moreover, a manual retrospective search was also conducted to detect articles published in rehabilitation medicine and Chinese journals. Search Strategy of two databases show in Supplementary Data.
Inclusion and exclusion criteria
The selection of studies was based on the following criteria.
Inclusion criteria:
(1) RCTs; (2) The participants are adults (including healthy adults and patients); (3) Whether the participants in the experimental group were trained on TC, including different genres; (4) The control group with no intervention or just received usual therapy along with nursing and/or health counseling for the preliminary illness and preserve routine activities; (5) Inclusion of at least one measure of cognitive function, such as global cognition: Montreal Cognitive Assessment Scale (MoCA), Mini-Mental State Exam (MMSE), event-related potential 300 (comprising amplitude, latency, reaction time, and peak value); learning and memory: Wechsler Memory Scale (WMS); executive function: Trail Marking Test (TMT-A and TMT-B), E-prime software (Flanker inhibition function test, N-back refresh function test, More-odd shift conversion function test); (6) Only the TC group and the non-TC group (control group) were selected in case there were multiple comparisons in the study.
Exclusion criteria:
(1) Identical publications; (2) Evaluation of patients with significant dissimilar baseline conditions; (3) Those studies with no outcome indicators or with relevant outcome indicators but still unobtainable even after communicating with the author; (4) Experimental group such as TC in combination with drug treatment and TC in combination with acupuncture; (5) Preclinical studies and experience reports; (6) Abstracts devoid of the full text.
Data extraction
Based on the inclusion criteria, two researchers individually screened the retrieved literature for relevant titles, abstracts, and full texts. The irrelevant RCT reports were eliminated, extracted, as well as cross-verified for the data. In those cases where no mutual agreement was attained for a study, the researchers discussed it together or would take the help of a third-party researcher to assess the credentials of the study. For data extraction, standardized data acquisition tables were employed. The extracted data primarily include (1) Preliminary data of the publication included in the study, such as the name of the first author, date of publication, sampling procedure, and study design; (2) The features of participants, including intervention population group and age; (3) The features of TC intervention, including parameters such as frequency, intensity, and duration; (4) Outcome index.
Risk-of-bias
The Cochrane Handbook for Systematic Reviews of Interventions 5.1.0 was used to assess the selected studies' risk-of-bias. 17 The assessment comprises the production of random sequences, allocation concealment, blindness, the integrity of result data, selective reporting, and other biases. Two researchers self-reliantly assessed the bias risk of the included studies and validated the outcomes. The results were then adjudged for high risk, low risk, and unclear based on individual articles' design and execution in the original literature. When there were variances or divergences in the quality assessment process, and the researchers could not decide, the third-party researchers were included to check and reach a final decision.
This study is a systematic Review and Meta-Analysis so it does not include IRB approval.
Statistical analysis
The Cochrane RevMan software (version 5.4.), The Cochrane Collaboration, 2020 was used for the evaluation of statistical heterogeneity test and data combination analysis. The evaluated data were presented in the form of mean difference (MD). p ≥ 0.1 and I 2 ≤ 50% were considered for all homogeneous studies, and a fixed-effect model was used for meta-analysis. p < 0.1 or I 2 > 50% represented heterogeneity between studies, a random-effects model was adopted in this case, subgroup analysis or sensitivity analysis was performed based on the possible sources of heterogeneity, and the research outcome was sensibly construed. A 95% CI was calculated, and the variance was considered statistically significant when p < 0.05.
Results
A systematic exploration of individual databases gave rise to 4104 studies. Five hundred thirty-three identical studies were eliminated. After thoroughly analyzing the titles and abstracts, 106 studies happened to meet the standards. Subsequently, the full text was carefully read. Thirty-three RCTs were finally included in this review. The precise process is represented in Figure 1.
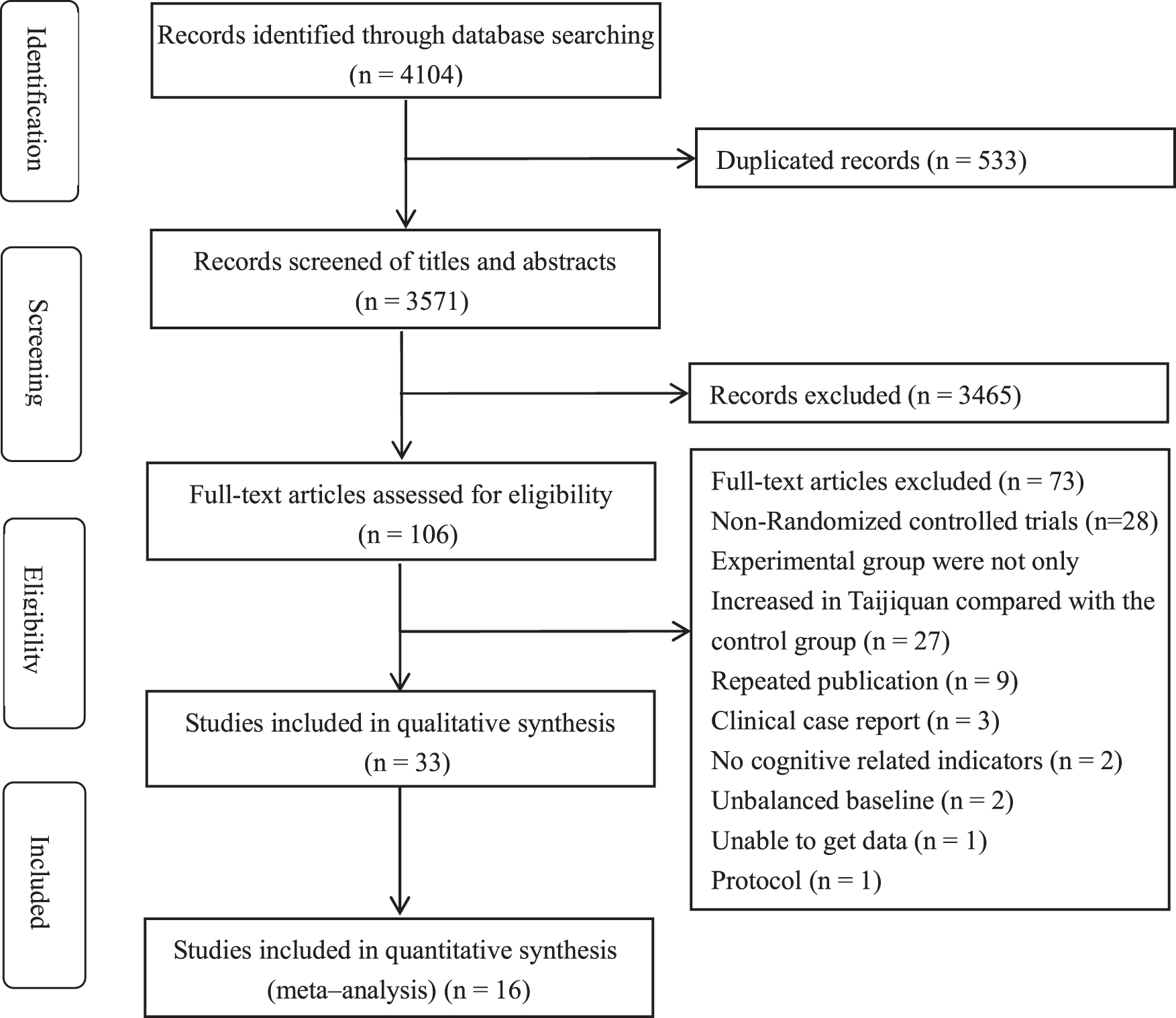
Flow chart for study selection.
Features of the included studies
In the present review, 33 RCTs with a total of 1808 participants were included. The studies considered for this review were conducted in China, Germany, the United Kingdom, and the United States. There are many genres of TC. Among the 33 RCTs, 22 did not mention specific genres, 8 were Yang styles, 2 were Chen styles, and 1 was Taoist. The incidence of intervention ranged from 2 to 5 days per week. The period of intervention ranged from 6 to 72 weeks. The following five main cognitive function domains were included for evaluating the outcome measures: global cognition, learning and memory, attention, executive function, and language.
Methodological quality of included studies
The results of risk-of-bias (Fig. 2) and risk-of-bias summary (Fig. 3) represent the outcome of each included study's risk-of-bias assessments. The procedure for the generation of the randomization sequence was described in 10 studies. 18 –23,30 –32,50 The procedure for the allocation concealment was reported in only three studies. 18,34,51 Due to the difficulty of blinding participants and personnel during exercise therapy, nearly all the studies included for the review were decided to be comprising unclear risk-of-bias in terms of blinding.
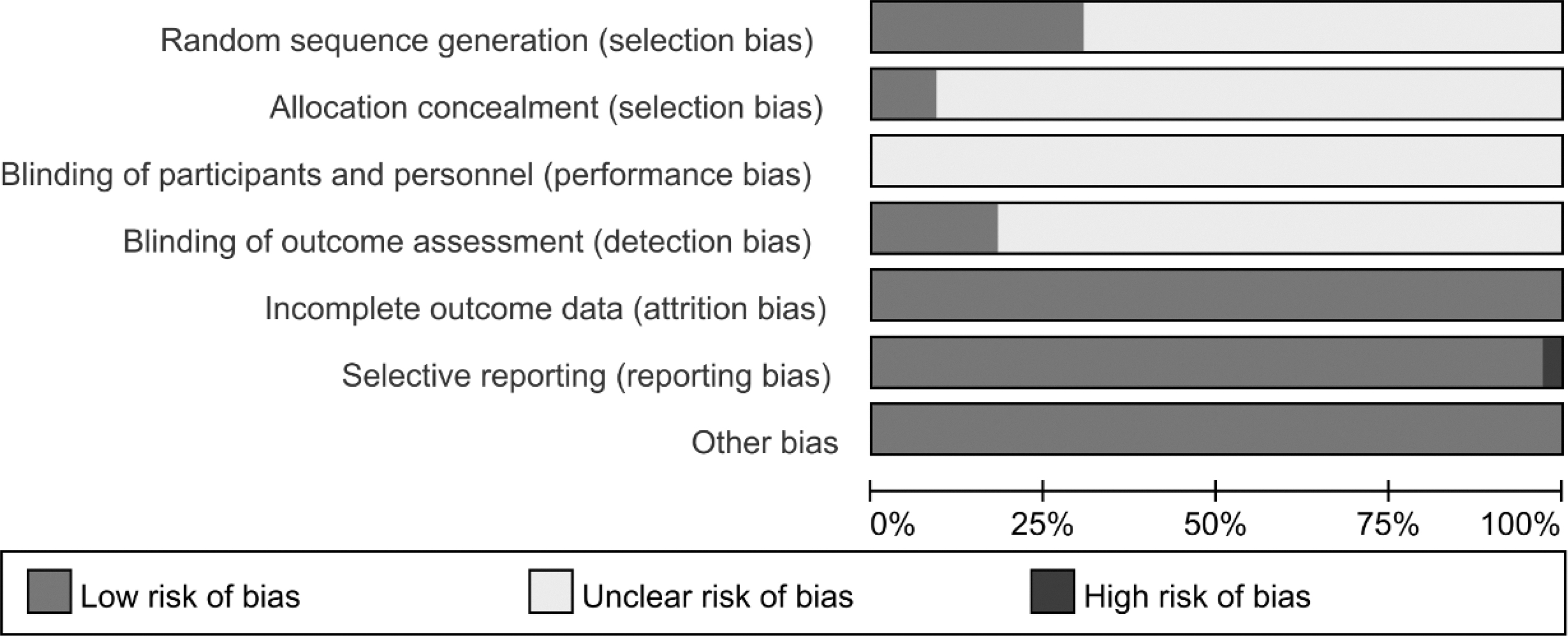
Risk-of-bias.
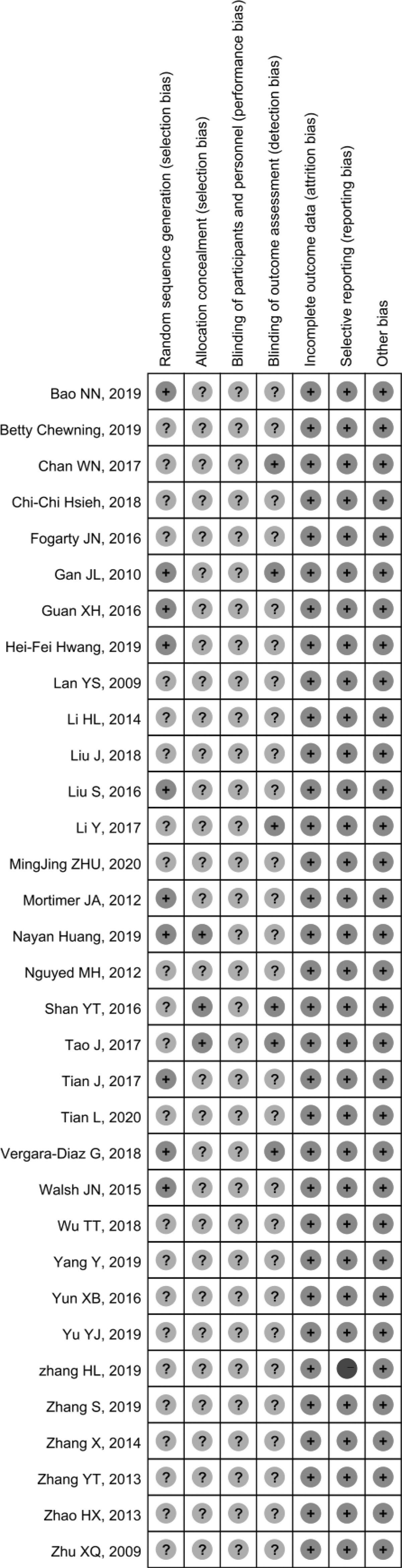
Risk-of-bias summary.
Meta-analysis results
TC in the middle-aged and elderly people with cognitive impairment
This review, including 344 participants in five studies, was evaluated by using the random-effects model for the global cognition, 18,19,28,31,52 employing MoCA after TC. Meta-analysis outcomes revealed that MoCA in the TC group was greater than that of the control group (Fig. 4). The results were as follows: MD = 3.23, 95% CI = 1.88–4.58, p < 0.00001. Taking into account the large heterogeneity, the included studies were divided into groups and subgroup analysis based on the intervention intensity. The results are as follows: TC intervention intensity 20–40 min/time (MD = 1.48, 95% CI = 1.02–1.94, p < 0.00001) (Fig. 5); TC intervention intensity 60 min/time (MD = 5.41, 95% CI = 4.38–6.43, p < 0.00001) (Fig. 5).
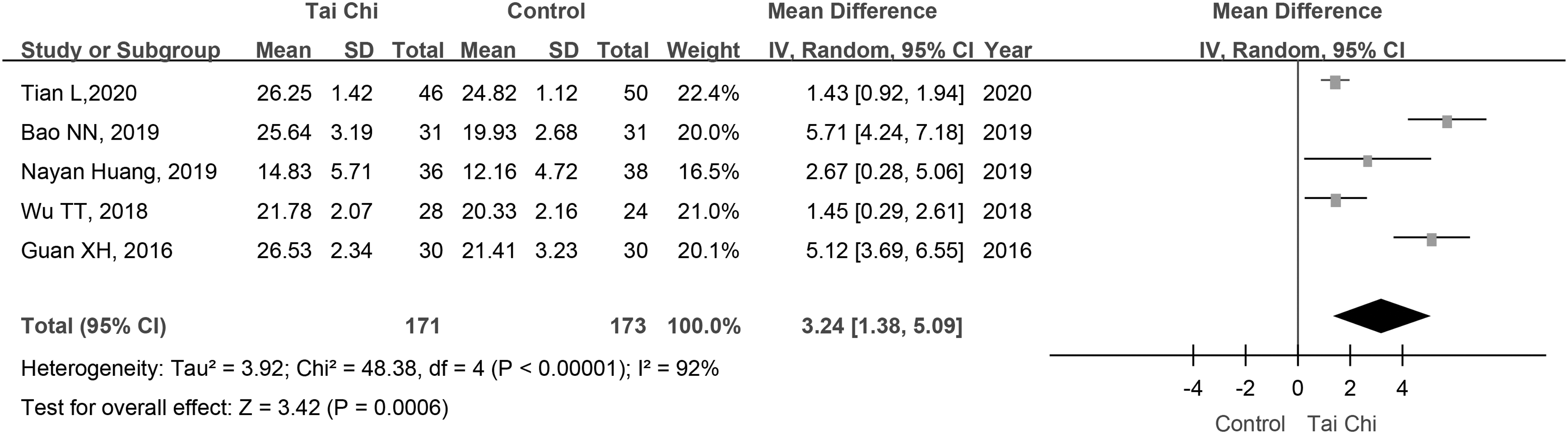
Total scores of MoCA after TC in people with cognitive impairment. MoCA, Montreal Cognitive Assessment Scale; TC, Tai Chi.
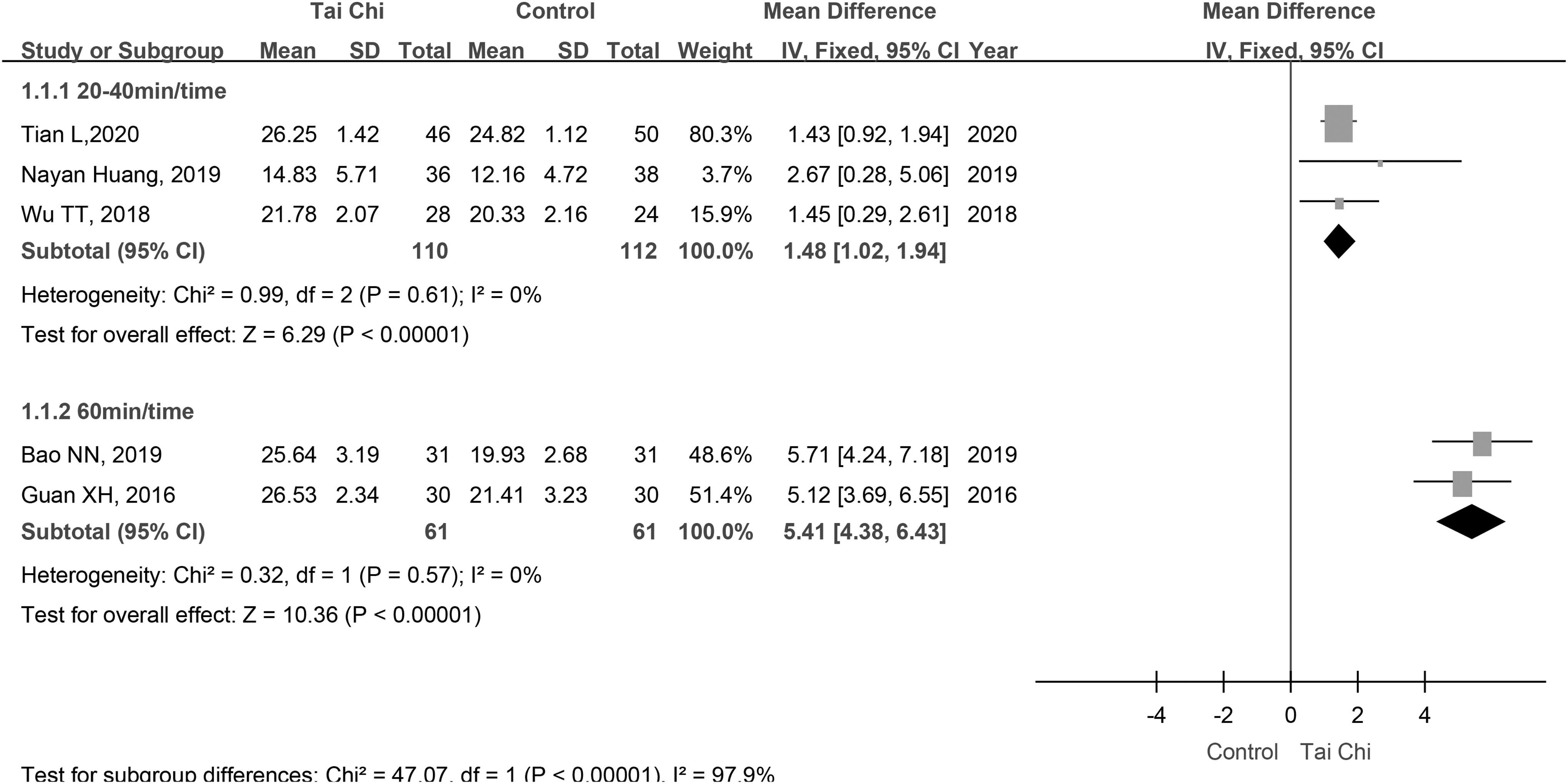
The influence of different intervention intensity on the total score of MoCA in patients with cognitive impairment. MoCA, Montreal Cognitive Assessment Scale.
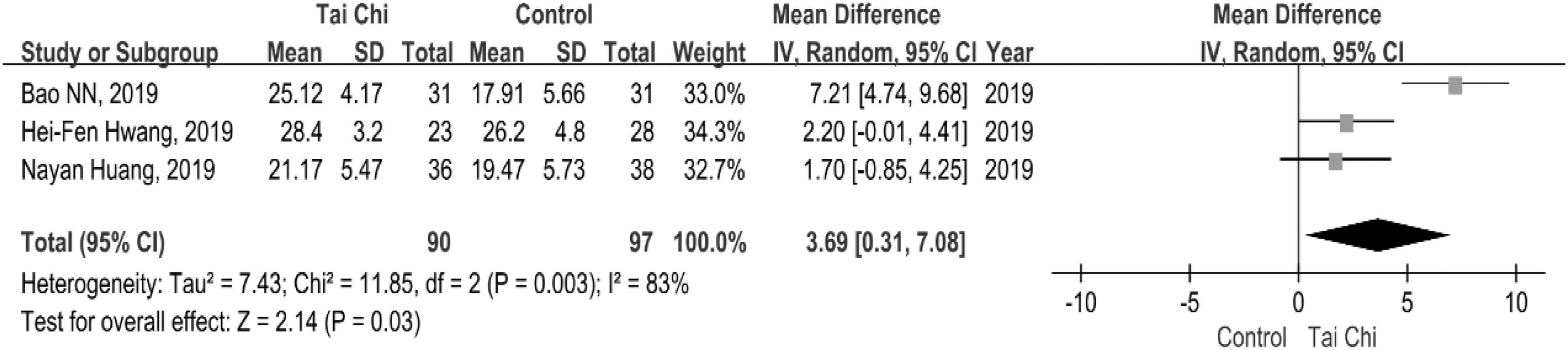
This review, including 187 participants in three studies, was evaluated by using the random-effects model with MMSE after TC. 18,19,30
Meta-analysis outcomes presented that MMSE in the TC group was greater than that of the control group (Fig. 6). The results were as follows: MD = 3.69, 95% CI = 0.31–7.08, p = 0.03 (Fig. 6). A sensitivity analysis of the impact of TC in the middle-aged and elderly people with cognitive impairment was conducted. Before the sensitivity analysis, the I 2 value was 83% (MD = 2.69, 95% CI = 0.31–7.08, p = 0.03). After removing Bao's study, meta-analysis using a fixed-effects model showed that the I 2 value dropped to 0% (MD = 1.99, 95% CI = 0.32–3.66, p = 0.02). These results indicate that TC could benefit the global cognitive function of people with cognitive impairment. Through comparison, it is found that the different forms of TC may be the main reason for the increased heterogeneity (Fig. 7).
Total scores of MMSE after TC in people with cognitive impairment. MMSE, mini-mental state exam; TC, Tai Chi.
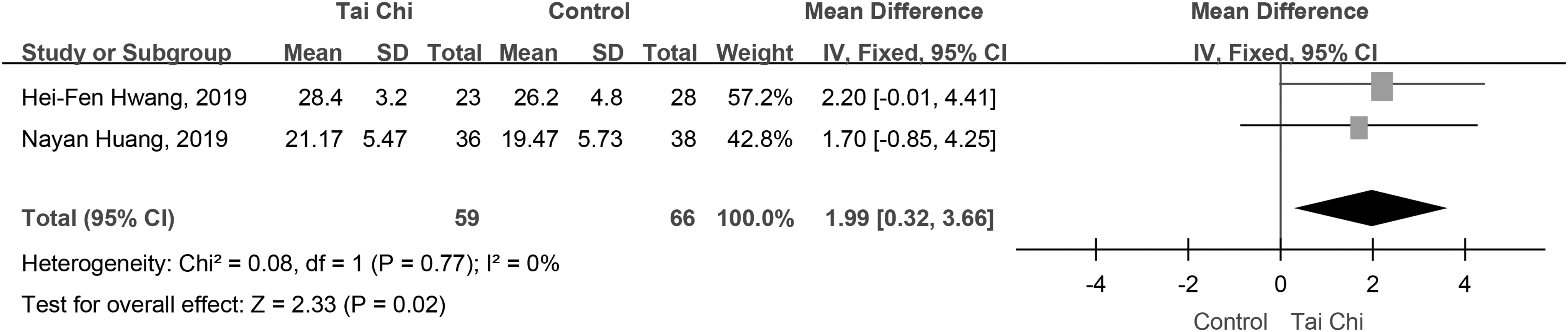
Total scores of MMSE after TC in people with cognitive impairment (sensitivity analysis). MMSE, mini-mental state exam; TC, Tai Chi.
Three studies were assessed for the executive functions with TMT after TC. Among them, one study exhibited the degree of freedom (df) and df error. 29 This review, including 147 participants in two studies, assessed the executive functions with TMT-B after TC by the fixed-effects model. 30,52 Meta-analysis outcomes presented that TMT-B in the TC group was lower than that of the control group (Fig. 8). The results were as follows: MD = −13.69, 95% CI = −21.64 to −5.74, p = 0.0007. The outcomes demonstrated that TC could benefit the executive function of people with MCI.

Descriptive data of TMT-B after TC in participants with MCI. MCI, mild cognitive impairment; TC, Tai Chi; TMT-B, trail making test-part B.
TC in older adults
This review, including 91 participants in two studies, assessed older adults' memory function by fixing the effects model with WMS after TC. 34,51 Meta-analysis outcomes displayed that WMS in the TC group was greater than that of the control group (Fig. 9). The results were as follows: MD = 23.32, 95% CI = 17.93–28.71, p < 0.00001. The results conferred that TC could improve the memory function in older adults.

Total scores of WMS after TC in older adults. TC, Tai Chi; WMS, Wechsler Memory Scale.
This review, including 133 participants in two studies, assessed the TMT-A by using the random-effects model. 21,24 The meta-analysis outcomes displayed TMT-A score with the following results: random-effects model, MD = −3.67, 95% CI = −14.77–7.42, p = 0.52. Three hundred thirty participants in three studies assessed the TMT-B by using the random-effects model (Fig. 10). 21,24,53 The meta-analysis outcomes presented TMT-B score with the following results: Random-effects model, MD = −7.01, 95% CI = −20.82–6.79, p = 0.32. The result exhibited that TC failed to support benefit for executive function in older adults (Table 1).

Total scores of TMT after TC in older adults. TC, Tai Chi; TMT, trail making test.
Characteristics of Randomized Controlled Trials
Outcomes: (1) Global cognition: MoCA; MMSE; P300; CASI; P50; MDRS; N400; SECF; (2) Learning and memory: WMS; RBMT II; DS; HVLT; AVLT; COWAT; Rey-O; CAVL; Boston Naming Test; (3) Attention: TEA; CAARS-S: L; TAP; Elimination test; AEP; (4) Executive function: TMT; Executive function by E-prime software; WAIS-III; Stroop test; Executive control capability; CDT; (5) Language: CVFT.
AEP, Auditory evoked potential; AVLT, Auditory Verbal Learning Test; C, Control group; CAARS-S: L, the Conners Adult ADHD Rating Scales self-report long version; CASI, the Cognitive Abilities Screening Instrument; CAVL, Chinese Auditory Verbal Learning Test; CDT, Clock-Drawing Test; CNLBP, Chronic Non-specific Low Back Pain; COPD-OSAHS, Chronic obstructive pulmonary disease-obstructive sleep apnea hypopnea syndrome; COWAT, Controlled Oral Word Association Test; CVFT, Category Verbal Fluency Tests; df, degree of freedom; DS, Digit Span; F, Female; HVLT, Hopkins Verbal Learning Test; M, Male; MCI, mild cognitive impairment; MDRS, Mattis Dementia Rating Scale; MMSE, mini-mental state exam; MoCA, Montreal Cognitive Assessment scale; N400, event-related potential N400; P50, event-related potential 50; PD, Parkinson's Disease; RBMT II, Rivermead Behavioral Memory Test; Rey-O, Rey-Osterrieth Complex Figure; SECF, scale of elderly cognitive function; TAP, Test of Attentional Performance; TC, Tai Chi group; TEA, Test of Everyday Attention; TICS-M, Modified Telephone Interview of Cognitive Status; TMT, Trail Marking Test; WAIS-III, Wechsler Adult Intelligence Scale, Third Edition; WMS, Wechsler memory scale; VR, Virtual Reality.
TC in college students
P300
This review included five studies that evaluated the global cognition with P300. 25,33,35,36,40 This review, including four studies, evaluated P300 amplitude, 33,35,36,40 of which one study showed 12 electrode points for comparing the P300 amplitude of the individual brain areas. 36 This review, including three studies, evaluated P300 latency. 25,35,40 Two studies evaluated P300 reaction time. 35,40
This review, including 57 participants in three studies, assessed P300 amplitude with the random-effects model. 33,35,40 The meta-analysis outcomes revealed the following results: MD = 1.61, 95% CI = 2.91–6.13, p = 0.48. This review, including 64 participants in three studies, assessed P300 latency with the random-effects model. 25,35,40 The meta-analysis outcomes displayed the following result: MD = −15.94, 95% CI = −49.07–17.19, p = 0.35. This review, including 40 participants in two studies, assessed P300 reaction time with the random-effects model (Fig. 11). 35,40 The meta-analysis outcomes exhibited the following results: MD = −45.16, 95% CI = −90.33–0.01, p = 0.05. These results showed no variance between the TC group and the control group in college students.
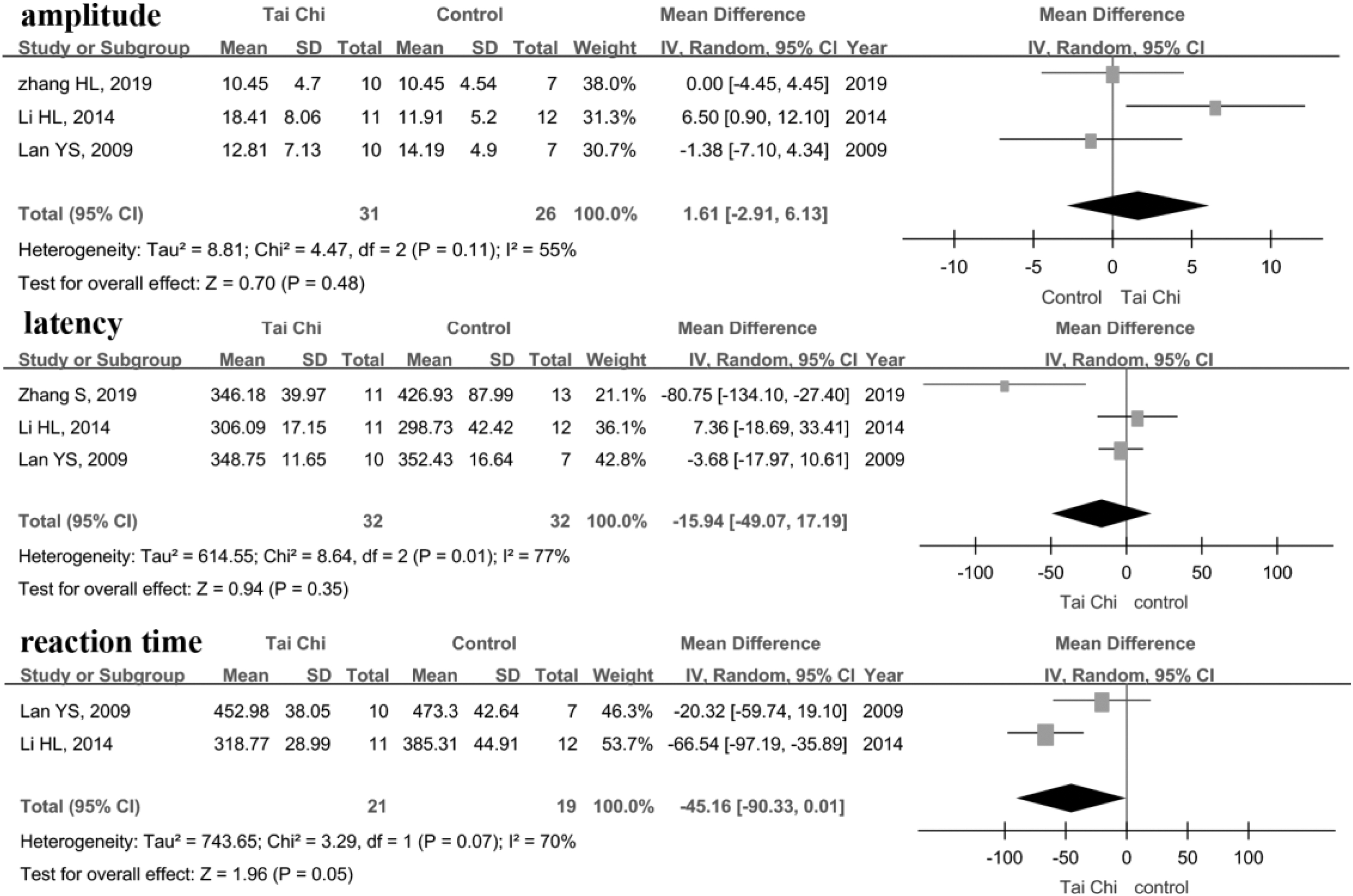
Total scores of P300 after TC in college students. TC, Tai Chi.
Executive function by E-prime software
This review, including two studies, used E-prime software to evaluate the executive function. 25,37 This review, including 72 participants in two studies, assessed the executive function test scores in three dimensions by using the fixed-effects model. 25,37 The Flanker test was used to determine the inhibitory function. Meta-analysis revealed the following results: MD = −16.32, 95% CI = −22.71 to −9.94, p < 0.00001. More-odd shift test conversion function was evaluated by the fixed-effects model, and the results were as follows: MD = −140.73, 95% CI = −184.64 to −96.81, p < 0.00001. The N-back test was performed to evaluate the refresh function by using the random-effects model (Fig. 12). The results were as follows: MD = −248.06, 95% CI = −497.65–1.53, p = 0.05. The results exhibited that TC could benefit the executive function of college students.
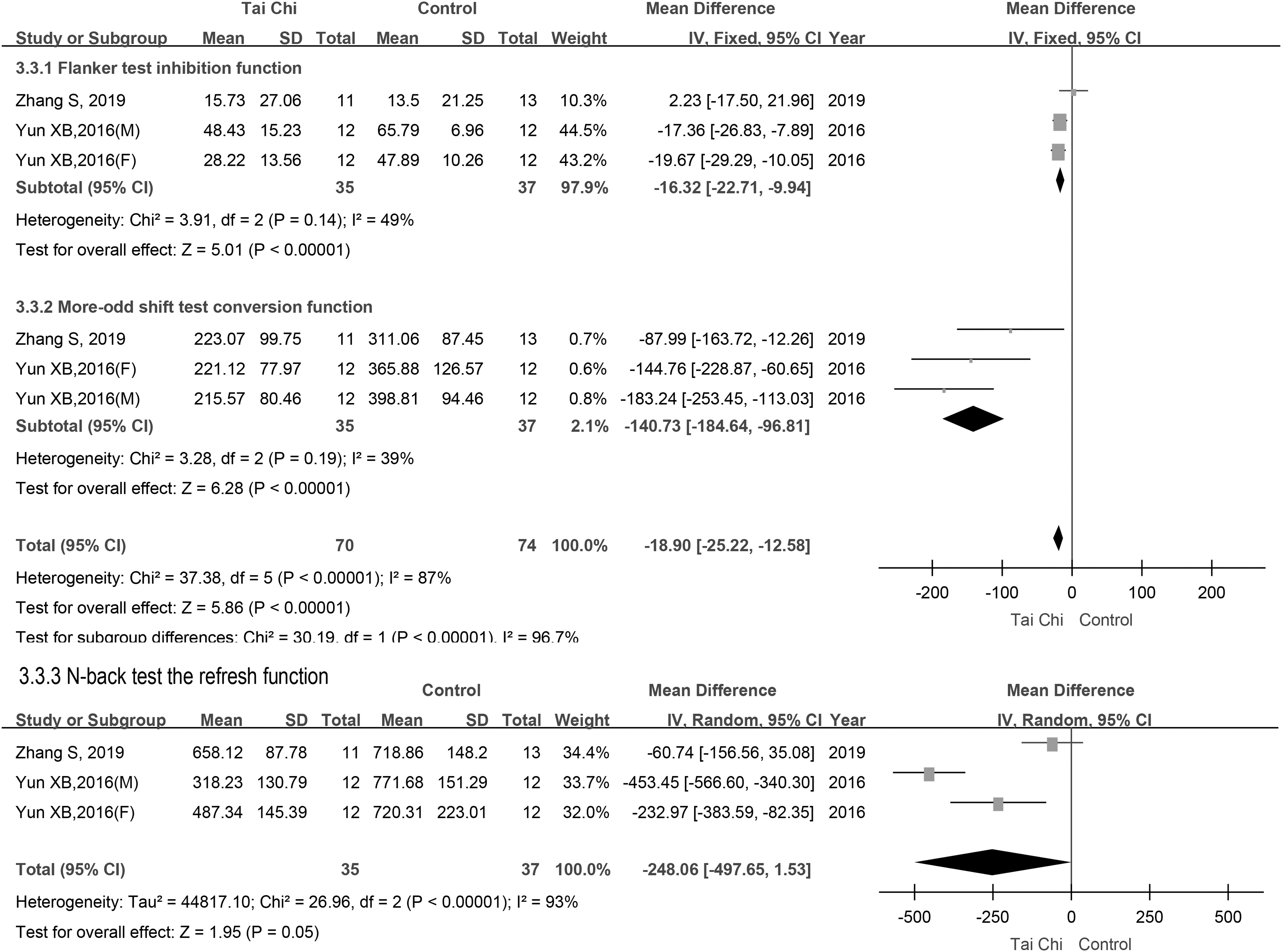
Total scores of executive function after TC in college students. TC, Tai Chi.
Descriptive analysis
In the current review, except for six studies, all the other studies revealed that TC training positively affects cognitive function. Two studies compared differences in cognitive function among long-term TC expert practitioners and age-matched and gender-matched TC-naïve adults. 21,40 The TC experts exhibited significant results on all cognitive measures. This demonstrates that long-term TC positively affects cognitive function, but there is no significant variance from the short term.
Most of the trials that were included in the review did not report any adverse events. One study with five TC group participants reported minor fatigue or slight ache in their limbs in the first week of exercise. 30 Another study reported two adverse events, 21 among which minor musculoskeletal injuries (one wrist and one ankle) were diagnosed. One study reported that two participants from the TC group experienced fatigue and dizziness, 38 and one participant had muscle cramps. These minor adverse events suggest that TC is likely to be safe. However, most of the RCTs included in this study did not report any data on the nonoccurrence of adverse events, and the safety needs to be further studied.
Discussion
Due to the large difference in the included population, our review is divided into different groups of participants to summarize the evidence on the impact of TC on the cognitive function of different participants. The overall conclusions from the current review are analogous to the other reported reviews. However, the present review also included updated evidence and differed significantly in the methods employed. This review gathered evidence with respect to the effects of TC on cognitive function in participants of different RCTs and compared it with the control group. This meta-analysis showed that TC had acceptable beneficial results on global cognition and executive functions in middle-aged and elderly people with cognitive impairment. Similarly, the result showed that TC could improve older adults' memory function, and TC could improve college students' executive function.
The current review results correspond to one of the studies that included four kinds of participants, RCTs and observed the treatment effect among middle-aged and elderly people with cognitive impairment, community elderly, college students, and different patients without cognitive impairment. The present review also indicated that the effect of TC on cognitive function assessed with P300 in college students and TMT in the middle-aged community as well as elderly adults, without MCI was not statistically significant. However, this result was based on two small studies. The reason for the ineffectiveness may be related to the time-frequency of intervention, because the period of training in college students was restricted for 6–10 weeks, which was shorter than 12–40 weeks in the middle-aged and to that of elderly people with cognitive impairment and 6–72 weeks in older adults. This indicates that the influence of TC on cognitive function may be linked to the total number of training sessions or treatment period. This meta-analysis analyzed only the effects of TC on cognition but not the effects of different treatment durations. Follow-up studies can be considered by using different durations of intervention to compare the effects of different frequencies and durations of treatment on TC's efficacy.
Aerobic exercise is distinguished for its positive effects on cognitive performance. 39 Aerobic exercises increase trophic factors such as brain-derived neurotrophic factor that affect cell birth and brain development. 41,54 Brain development includes neural stem cell proliferation, neuronal survival, dendritic arborization, and synaptic plasticity. These activities consequently enhance neural transmission and improve learning and memory. 26,55
The TC is a typical mind–body and low-intensity aerobic exercise involving breathing, body coordination, and visual perception meditation. This has positive associations with physiological and psychological conditions. 56 Certain studies showed that TC training improved the connection of the prefrontal cortex, the motor cortex, and the occipital cortex in myogenic activity, sympathetic nervous system, and endothelial cell metabolic activities; this resulted in enhanced brain functional connections and relayed TC's ability to improve cognition and the anti-memory decline potential. 27,57
Conclusion
The TC might have a positive effect on the improvement of cognitive function in middle-aged and elderly people with cognitive impairment as well as older adults and college students.
Limitations and suggestions for future research
There are several limitations to this study. First, the analysis was restricted to studies in English and Chinese languages only. The inclusion of studies in other languages would have represented the evidence to date and also cover, in whole, the general population who have gained benefits after TC. Second, since TC is represented by several styles (e.g., Chen, Yang, or Wu styles of TC) and within each style, there are different training durations with some training regimens developed explicitly for research purposes; most of the studies did not mention specific genres, and due to different outcome indicators, the meta-analysis was not performed according to the TC genre.
The training time for middle-aged and elderly people ranges from 20 to 90 min, and for college students, it ranges from 30 to 12 min. The frequency is at least two times a week and up to six times a week. In the future, we can further study the impact of different frequencies and different durations on specific groups of people to provide a basis for formulating TC practice programs. Moreover, owing to the limited number of studies available for evaluating TC in different groups and the heterogeneity of populations evaluated across studies, the meta-analyses in the present study were limited to only the most commonly measured outcomes. Until more studies are available with common outcomes reflecting other domains mentioned earlier, it will be challenging to evaluate TC and cognitive function more broadly. As the outcomes of larger-scale trials become available, future studies should contemplate single-group data meta-analyses that can evaluate the impact of the training regimen while controlling for a certain group of people (e.g., MCI and college students). In addition, we did not register and publish the protocol in consideration of time and funding. We will make improvements in follow-up research.
Footnotes
Authors' Contributions
Study concept and design: F.L.; Acquisition of data: P.N., F.L., L.Y., and J.C.; Analysis and interpretation of data: S.L., X.C., and J.G.; Drafting of the article: F.L., P.N., and X.C.; Critical revision of the article for important intellectual content: F.L., L.Y., and P.N.; Statistical analysis: F.Liu, L.Y., S.L., X.C., and J.G.; and Study supervision: F.L.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors disclose the receipt of the following financial support for the research, authorship, and/or publication of this article: Open Project of Nursing Discipline of Fujian University of Traditional Chinese Medicine (X2019044-Discipline); 2020 Fujian Provincial College Student Innovation and Entrepreneurship Training Program (202010393042).
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.