
Abstract
Background:
Dietary supplements promoted for brain health and enhanced cognitive performance are widely available. Claims made for these products are directed not only to the elderly wishing to prevent or mitigate cognitive decline, but also young healthy populations looking to boost their cognitive performance. It is unclear whether these claims made on product bottles and through advertising match the science.
Objectives:
To explore the evidence on the efficacy and safety of single dietary supplement ingredients frequently marketed with claims of enhanced cognitive performance among healthy adults.
Design:
A systematic review.
Results:
Nine of 54 dietary supplement ingredients identified through a scoping review met the eligibility criteria with at least 3 published studies identified per ingredient, yielding 69 unique publications. Ingredients evaluated included Bacopa monnieri, choline, creatine, omega-3 fatty acids, Ginkgo biloba, ginseng, Rhodiola rosea, tyrosine, and valerian root, all in supplement form and compared with a placebo, at various serving sizes and durations of use.
Conclusions:
The low level of certainty in the state of the science, coupled with not always knowing what is in a dietary supplement product, make weighing risks and benefits difficult; these data hinder the ability to develop recommendations about using such ingredients for consumers interested in boosting their cognitive performance. Whereas certain trends regarding promising serving sizes or duration for use, are pointed to in this synthesis, when combined, studies are inconsistent and imprecise, and many are methodologically flawed. Potential solutions to address research gaps are offered, for future research next steps, which is needed to strengthen the evidence and inform decisions.
Introduction
Dietary supplements promoted for brain health and cognitive performance have quickly become a multibillion dollar market, with more than a quarter of Americans aged 50 and older reportedly regularly consuming supplements for brain health. 1 These products are widely available and often advertised with claims for enhanced cognitive performance, including improved memory, attention, focus, energy, and motivation. This massive market not only targets an elderly population that may wish to prevent or mitigate cognitive decline, but also young, healthy population(s) looking to optimize their cognitive performance. In fact, elite performers who strive to gain and maintain a high level of performance are likely a prime target for this market. 2
Research in this area has primarily focused on prevention or mitigation of cognitive health decrements in elderly and impaired populations, 3 –8 rather than enhancement of cognitive performance in otherwise healthy, young populations. However, many of the claims displayed on dietary supplement packaging suggest performance enhancement. It is unclear whether the claims advertised accurately reflect the science. This review summarizes the evidence on the efficacy and safety of single dietary supplement ingredients frequently marketed with claims of enhanced cognitive performance in healthy adults. The primary goal of the evidence synthesis is to rely on the knowledge gained to assist consumers with making informed decisions about the use of various ingredients commonly listed on dietary supplement product labels. A secondary goal is to use the evidence to drive recommendations and possible solutions for next steps in research, based upon the scientific gaps discovered.
Methods
Scoping review
A scoping review was conducted to identify (a) dietary supplement products marketed for brain health and cognitive performance and their associated claims, (b) ingredients most frequently listed among products, and (c) the extent of systematic review research investigating the impact of those ingredients on any cognition outcomes and across various populations. This exercise allowed the authors to refine the focus and scope for this systematic review. These methods are reported in a separate publication. 9
Search strategy
Seventy-two frequently included dietary supplement ingredients were identified across 650 products found on the market. 9 After evaluating the systematic reviews reported upon previously, 54 ingredients were considered for evaluation. The authors searched PubMed, Embase, PsycInfo, and the Computer Access to Research on Dietary Supplements (CARDS), which houses federally funded research projects, from database inception to June 2019. Limits were applied to identify Randomized Clinical Trials (RCTs) published in the English language involving adult humans, where applicable. Natural Medicines database as well as all relevant systematic reviews (identified through the scoping review) were crosschecked, to identify any missing studies meeting eligibility criteria or published reviews that might overlap with this initiative. This search strategy was executed for each of the 54 dietary supplement ingredients (their specific ingredients names coupled with their scientific and common names, and applying mapping strategies where available in databases), coupled with keywords to identify outcomes relating to cognitive performance. Terms specifically used in PubMed included Mesh and other common terms (Example: mental processes OR cognitive dysfunction OR “brain health” OR “cognitive health” OR mental health OR “brain function” OR “cognitive function” OR executive function OR “mental clarity” OR “cognitive ability” OR “cognitive performance” OR “mental performance” OR reaction time OR memory OR problem-solving OR “energy” OR “alert” OR “focus” OR attention OR concentration) (Supplementary Tables S1 and S2).
Study selection
Two investigators (C.C. and C.B.) independently screened titles and abstracts of all citations retrieved from the literature searches, in duplicate and according to predefined eligibility criteria (Supplementary Table S1). Randomized clinical trials were eligible if: (a) the population(s) was healthy adults, 18–60 years of age, without clinically diagnosed disease or signs of cognitive impairment; (b) the ingredient was administered as a monotherapy dietary supplement and compared with placebo, with no restriction on the serving size or time of administration; and (c) participants were subjected to task-based cognitive performance assessment tests, at both a baseline and after consumption or follow-up time of administration. Dietary supplement ingredients with less than three potentially eligible trials were excluded from data extraction and quality assessment, and labeled as “insufficient evidence” to evaluate (Supplementary Table S2).
Data extraction and quality assessment
Data were extracted from each included study to describe the study design, the participants' engagement, intervention(s), all cognitive performance tests performed and associated metrics for assessment at various time points, funding sources, and any noted adverse events reported. Risk of bias was assessed independently by two reviewers (C.C. and C.B.) using the Scottish Intercollegiate Guidelines Network (SIGN 50) checklist for RCTs. 10 Reviewers met to discuss and resolve any discrepancies.
Data synthesis and analysis
Evidence for efficacy
Objective, task-based cognitive performance was the primary outcome assessed through systematic review. Cognitive domain categories for grouping cognitive performance tests and associated metrics were devised as attention/working memory, executive function, memory/learning, and psychomotor performance/reaction time. All self-reported measures relating to mood (in terms of feeling alert, calm, content, stressed, anxious, and mentally fatigued), were considered as secondary outcomes and categorized separately. The authors acknowledge the considerable overlap among tests and domains, and discovered that researchers not only used various different performance tests but also reported test results in varying ways that challenged the ability to perform meta-analysis (Supplementary Table S3). Instead, this systematic review reports cognitive test results by direction of effect/whether it reached statistical significance as compared with placebo at all serving sizes and across every time point measured.
The strength of the evidence was evaluated by using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach: cognitive performance was used as the main outcome. 11 The authors first considered each time point and serving sizes evaluated at those time points. If less than three studies were available, the strength of evidence was labeled as “insufficient data” to evaluate the dietary ingredient in terms of a specific serving size or duration for administration. Each dietary supplement ingredient, regardless of serving size and time point, was then evaluated as a collective body of evidence to determine the ingredient's overall strength of evidence, according to cognitive performance. In both cases, the certainty of the evidence was graded by using criterion of risk of bias across studies, inconsistency, indirectness, and imprecision.
Evidence for safety
In addition to extracting data from included studies reporting on adverse events, the authors conducted additional searches in an attempt to capture adverse events reporting. The authors searched PubMed for published case reports, examined Natural Medicines database “adverse effects” sections of dietary ingredient professional monographs, and searched the Center for Food Safety and Applied Nutrition Adverse Event Reporting System (CAERS) database (2014 to March, 2020), which contains information on adverse events submitted to the Food and Drug Administration (FDA).
Results
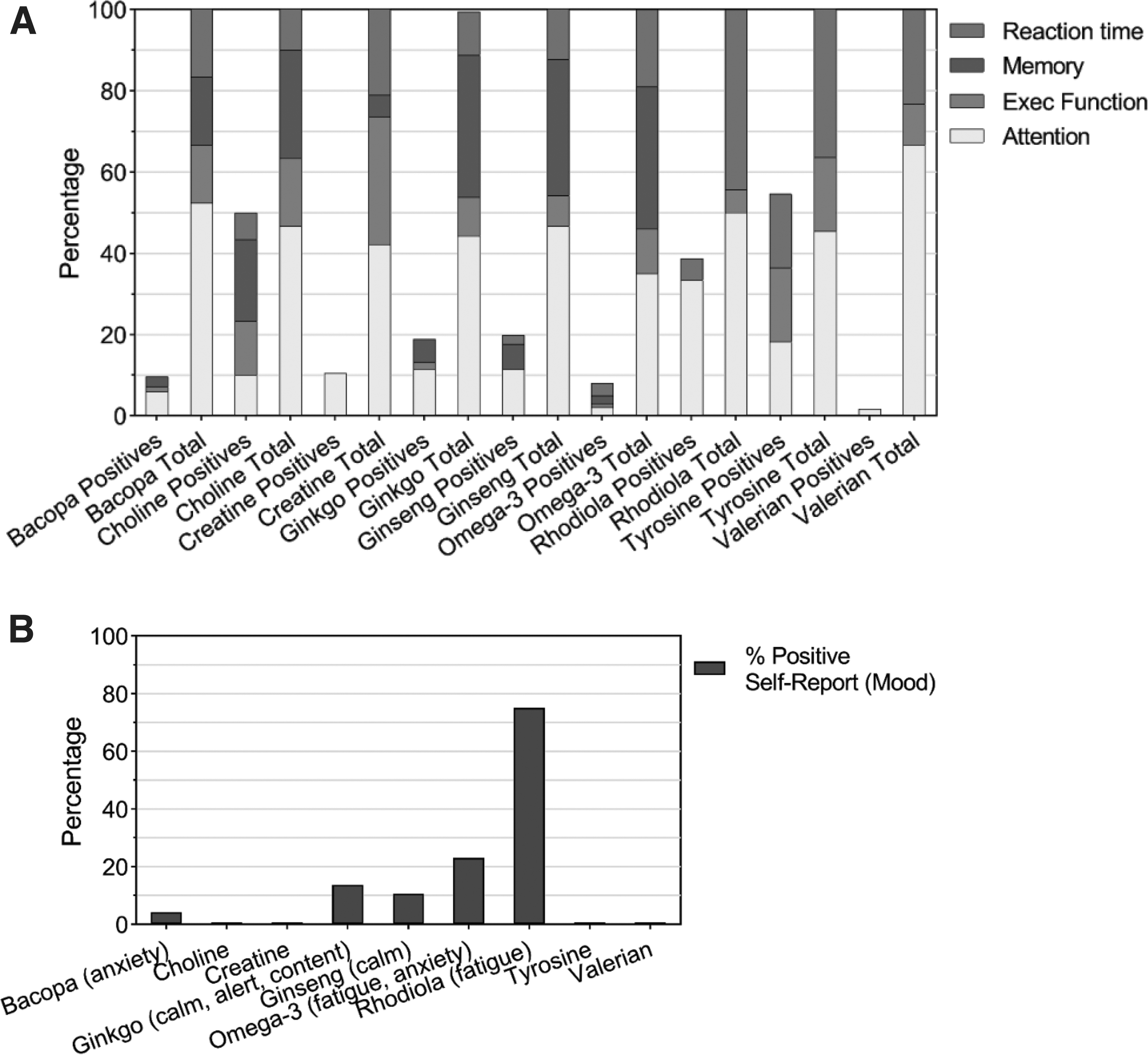
Nine of the 54 dietary supplement ingredients met the eligibility criteria with at least 3 published studies identified per ingredient, which yielded 69 unique publications. Ingredients included Bacopa monnieri, choline, creatine, omega-3 fatty acids, Ginkgo biloba, ginseng, Rhodiola rosea, tyrosine, and valerian root, all in supplement form and compared with a placebo. Cognitive performance tests most prevalent were within the attention/working memory domain, followed by psychomotor performance/reaction time, memory/learning, and executive function (Supplementary Table S3). Figure 1A shows the distribution of tests according to outcome domains across the ingredients studied and the percentage reaching statistical significance in favor of the ingredient as compared with placebo, regardless of serving size or time point within the domains. Figure 1B shows the percent of positive tests for self-report mood-related secondary outcomes.
Characteristics of included studies are detailed in Supplementary Table S4. The number of trial participants ranged from as small as 8 to as large as 305 participants, 18–60 years of age. In all studies, participants were subjected to a variety of cognitive tests before and postadministration of the dietary supplement ingredient being evaluated—from immediately after administration and up to a total duration of 6 months. Most (n = 37; 54%) of the studies were designed to allow for practice tests before starting the trial to familiarize participants with the cognitive performance tasks and minimize the impact of a possible learning effect. The majority (n = 48; 70%) reported instructing participants to abstain from certain practices (e.g., smoking, nicotine, alcohol, caffeine, drugs/specific medications) before study commencement and/or specified a specific diet to follow leading up to the study (e.g., fasting overnight, having a light breakfast).
Some studies (n = 24; 35%) did not report a funding source; aside from companies donating products to the researchers conducting the studies, 20 (43%) reported at least partial funding from industry. Most publications (n = 42; 61%) identified the specific product or extract name used in the study; most (n = 46; 67%) named the manufacturer of the product and detailed characteristics of the product (n = 43; 62%), such as the parts of the plant used, the type of product, or the concentration or weight of the components. Only a few (n = 16; 23%) mentioned a qualitative/quantitative purity test of the product's chemical fingerprints to confirm that the ingredients named on the label were what the participants actually ingested as part of the study.
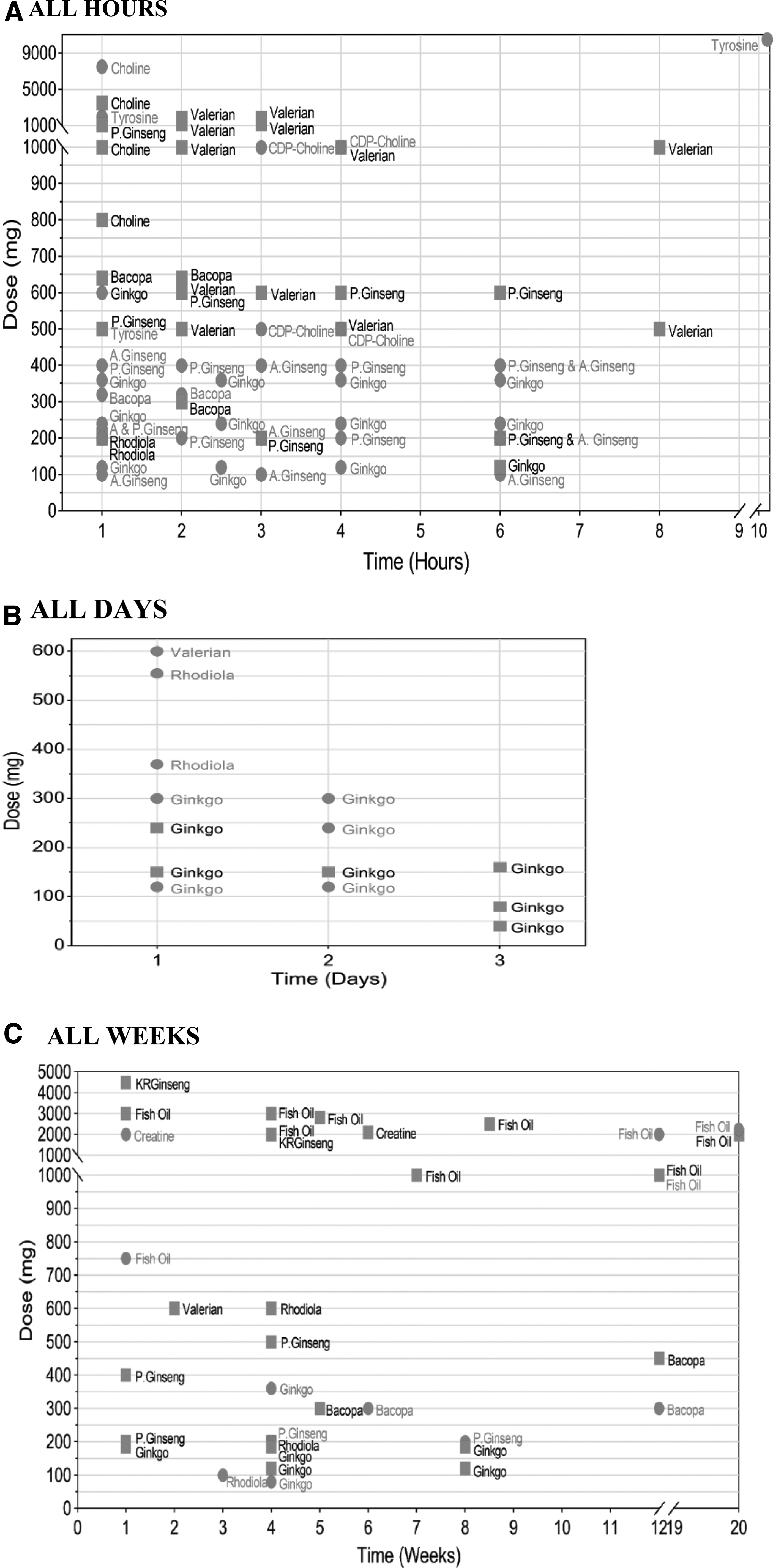
Supplementary Table S5 details the risk of bias across all studies for each ingredient, and the percentage of studies that adequately addressed each criteria. Among all ingredients, reports suffered methodologically across noticeable areas, including adequate descriptions of the randomization process for the assignment of subjects to treatment groups and adequate concealment methods detailed in reports. In addition, few studies reported on power calculations to ensure the detection of meaningful differences for the various tests performed and whether intention-to-treat analyses were considered. Results below describe each ingredient separately for overall strength of evidence and according to specific cognitive performance test outcomes assessed across various serving sizes and time points of administration. Table 1 details an overall summary of findings collectively, relevant gaps, and potential solutions to address gaps for each ingredient evaluated. Figure 2A–C graphically maps each ingredient, at each time point and serving size, compared with placebo, whether there was an effect on cognitive performance. Supplementary Tables S6–S8 detail all data analyzed; Supplementary Table S9 details adverse events.
Summary of Findings for Individual Ingredients
For full detail of GRADE assessment and certainty of evidence table, see Supplementary Table S8.
See Supplementary Tables S5, S7, and S8 for more detail. Supplementary Table S9 details AE noted from several data sources researched.
This represents a “roll-up” of results to display overall cognitive performance as an outcome according to the number of tests performed across various serving sizes and time points assessed (across all studies). The numbers represent the number of tests that reached statistical significance in favor of the dietary ingredient as compared with placebo at every serving size and time point assessed. The Supplementary File breaks this information down across various categories of analysis and per study.
A panel of experts convened and prioritized a set of identified gaps and offered potential solutions for future research.
Inconsistency: Time points of evaluation varied across studies, preventing the ability to gather meaningful evidence about the effect on duration of administration. In addition, different serving sizes were examined across various measures/metrics. Studies did not consistently report benefit within or across these variations.
Imprecision: Results could be impacted because of the enrollment of a small number of participants in each study (and across studies) for each serving size and time point according to outcomes. A threshold of 400 or less is concerning, and less than 100 very concerning.
The strength of evidence is evaluated using the GRADE approach taking into account methodologic flaws, inconsistency, imprecision, and indirectness.
Risk of bias: The majority of studies were rated as suffering methodological flaws.
The available evidence with regard to the populations included may have differing proportions of omega-3 fatty acid blood levels and varying different dietary habits within and across studies that may or may not reflect the otherwise healthy population at large.
Risk of bias: All studies were rated as suffering methodological flaws.
AE, adverse events; CDP, cytidine diphosphate-choline; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; GRADE, Grading of Recommendations, Assessment, Development, and Evaluation.
Bacopa monnieri
Bacopa, a well-known herb in India and used in traditional Ayurvedic medicine, is common in dietary supplements advertised for improving memory and learning retention, concentration and focus, and maintaining overall cognitive function. Seven studies have examined such effects, one judged as low quality. 12 These studies involved a total of 361 healthy volunteers, 18–60 years of age, allocated to either Bacopa or a corresponding placebo, at various serving sizes ranging from 300 to 640 mg/day, taken over the course of 1 day (measured at 1 h) and up to 12 weeks duration. KeenMind was used in five trials, 13 –17 whereas Bacozine 12 and BacoMind 18 were administered in the remaining studies. The most recent study was published in 2016. 12
In single studies, participants who consumed 320 mg Bacopa outperformed those in the placebo arm on tests of a multitasking framework—letter search 13 (n = 17) and a serial three subtraction task 14 (n = 24) at 1 and 2 h after consumption. Higher serving sizes at these same time points did not show any statistical differences between Bacopa and placebo for any test. A single low-quality study of 300 mg Bacozine, taken over the course of 6 weeks and compared with placebo reported significant results in two (digit span, logical memory) of nine tests (n = 60). 12 The largest study included 107 healthy participants taking KeenMind at 300 mg/day over 12 weeks. Results indicated that working memory was significantly enhanced in the Bacopa arm relative to the placebo. 16 Separately, a smaller study (n = 46) showed a statistically significant difference in inspection time and auditory verbal learning test at the same serving size and time points. 17 No other amount or time point revealed any statistically significant cognitive performance effects. Only one study (n = 46) reported a statistically significant change in mood scores (anxiety) after 12 weeks administration of 300 mg KeenMind. 17 For any specific amount or duration of administration or within any specific cognitive domain, the available data are insufficient to evaluate the efficacy of Bacopa as compared with placebo on cognitive performance (Supplementary Table S7). The authors graded the strength of evidence on Bacopa for enhancing cognitive performance as low, overall (Supplementary Table S8 and Table 1).
Two studies, both using KeenMind 300 mg/day over a 12-week duration, reported on adverse events. Other studies did not report on adverse events/safety (K = 2) or reported that none occurred (K = 3). Reported events included dry mouth, nausea, diarrhea, and fatigue. Natural Medicines database reports that Bacopa is “possibly safe” when used orally and appropriately, short term (Supplementary Table S9). 19
Choline
Choline is an essential nutrient that should be included in one's diet to maintain optimal health. 20 Citicoline is a molecule formed in the body as an intermediate in the synthesis of phosphatidylcholine from choline. 21 As a dietary supplement, labels may read as choline chloride, choline bitartrate, or choline citrate. This is different from citicoline or cytidine diphosphate-choline (CDP), which tends to be higher in choline content per unit weight and more easily absorbed than otherwise choline. 22 In fact, in other countries such as Europe, CDP-choline is a prescription drug for cognitive impairment related to chronic cerebrovascular disease. 23 In the United States, CDP-choline is considered a dietary supplement along with choline.
Five publications (1978–2015) met the review's eligibility criteria involving 169 participants 18–38 years of age. All except one 24 were of low methodological quality. Three studies examined the immediate effects of choline in amounts ranging from 50 mg of choline per kilogram body weight, 24 2–2.5 g choline bitartrate, 25 and up to 10 g choline chloride elixir per day. 26 The remaining two studies published by the same author, examined 500 and 1000 mg CPD-choline at 3 and 4 h after consumption. 27,28 Preparations were equivalent to serving sizes ranging from ∼100 to 7500 mg of choline per day based on the information provided.
Taking 50 mg/kg body weight choline (about 3.5 g/day of choline for a 70 kg person) before exhaustive load carrying did not improve any measures of cognitive performance. 24 Two to 2.5 g choline bitartrate (800 mg to 1.0 g of choline/day) also showed no effects on any measures of memory performance. 25 A study from 1978 involving 10 participants showed that taking 10 g choline chloride elixir (about 7.5 g of choline/day) improved serial learning and a selective reminding task for low imagery words but not high imagery words. 26 Studies by Knott et al. 27,28 tested 500 and 1000 mg CPD-choline (about 100 and 200 mg of choline, respectively). The earlier study showed that “low performers” at baseline with 500 mg relative to placebo scored better on the Groton maze task, whereas medium and high performers did not. A similar but not significant trend was found for the 1000 mg amount. 28 The 2015 study showed that low performers again performed better than medium and high performers using both 500 and 1000 mg as compared with placebo. 27 In this study, the high performers actually did worse whereas the low performers did statistically better than placebo. For any specific amount or duration of administration or within any specific cognitive domain, data available to evaluate the efficacy of the different variations of choline as compared with placebo on cognitive performance are insufficient (Supplementary Table S7). The authors graded the strength of evidence on choline or CDP-choline for enhancing cognitive performance as very low, overall (Supplementary Table S8 and Table 1).
Three studies reported that no serious adverse events occurred and two did not describe safety. Choline chloride and choline bitartrate are listed in the Code of Federal Regulations as nutrients and/or dietary supplements that are generally recognized as safe (GRAS) (Federation of American Societies for Experimental Biology, 1975). 29 Natural Medicines database reports that choline is “likely safe” when used orally and appropriately in adults below 3.5 g/day. 30 Citicoline is reported as “possibly safe” when used orally and appropriately, short term, up to 1000–2000 mg and up to 90 days. 31 The most common side effects are nausea, abdominal pain, and diarrhea in either formulation in small amounts (Supplementary Table S9).
Creatine
Creatine is a compound found naturally in skeletal, brain, and cardiac muscles, in the form of phosphocreatine. 32 It serves as an energy source for exercise and during heavy lifting. As a dietary supplement, creatine is popular among athletes and body builders to help gain weight, muscle, strength, and improve performance. Some products are advertised not only to enhance physical but also mental performance. Although different “types” of creatine products are sold, creatine monohydrate seems to be studied more than other types in clinical trials. 33
Four studies published from 2002 to 2015 met eligibility criteria for creatine 34 –37 ; only three had sufficient data reported for the outcomes as compared with placebo. 34 –36 These studies, involving 158 participants (∼21–55 years of age), were not directly related to each other and had varying main objectives. All three were of low methodological quality. Turner et al. 36 investigated creatine monohydrate supplementation during acute oxygen deprivation; those supplemented with 20 g performed statistically better in complex attention and continuous performance tasks than a placebo group. Tests of executive function only trended toward statistical significance. 36 Benton and Donohoe 34 compared creatine with placebo on cognitive functioning of vegetarians versus omnivores; vegetarians supplemented with 20 g performed better on memory tests than omnivores, however, no test reached statistical significance when compared with placebo. Both studies reported similar duration (5–7 days). The third study 35 examined the effect of creatine supplementation over 6 weeks duration of 0.03 g of encapsulated creatine per kilogram of body weight per day (about 2.1 g/day); results showed no improvements over the course of 6 weeks' duration. 35 For any specific amount or duration of administration or within any specific cognitive domain, there were insufficient data available to evaluate the efficacy of creatine supplementation as compared with placebo on cognitive performance (Supplementary Table S7). The authors graded the strength of evidence on creatine for enhancing cognitive performance as very low, overall. It is important to note that existing physical performance research demonstrates likely effective short term (Supplementary Table S8 and Table 1). 38 –40
One study reported minor adverse events, including bloating and headache in both the creatine and placebo group. Other studies did not report on adverse events. Natural Medicines database reports creatine is “likely safe” when used orally and appropriately, short term. Studies have shown that amounts up to 25 g daily up to 14 days in healthy adults to be safe. 41 Case reports have reported rash, dehydration, renal dysfunction, and arrhythmia, but none of these cases has shown up as adverse events in controlled trials. 42 –45 A recent systematic review examined the risk of adverse outcomes in females taking creatine monohydrate and confirmed no serious adverse events associated with this ingredient (Supplementary Table S9). 46
Ginkgo biloba
Ginkgo, one of the most popular dietary supplements, is used for dementia, cognitive decline/memory loss, mood disturbances (e.g., depression, anxiety), attentional issues (e.g., concentration difficulties), and vertigo. Sixteen publications on Ginkgo met eligibility criteria for review, involving 708 participants, 18–59 years of age. Participants were allocated to either Ginkgo or a placebo, in varying amounts ranging from 40 mg/day up and to 600 mg/day, administered on 1 day and for as long as 12 weeks. Ten studies published before 2006 were of low methodological quality. 47 –56 The more recent studies were of adequate to high quality, with the latest published in 2016. 57 –62 Extracts or products named as G. biloba GK 501 (in 4 studies), Egb 761 (2) Ginkgoforte (2), Ginkyo (1), GBE24/6 (1), and LI 1370 (1); the extract or product name was unclear in the remaining 5 studies.
There is low certainty of the evidence for serving sizes of 120–360 mg on cognitive performance assessments as short as 1 and up to 6 h. Statistically significant improvements in favor of Ginkgo were reported for attention/working memory (memory scanning, working memory, digit vigilance, serial three and seven subtraction tasks, speed of attention), memory/learning (quality of memory, secondary memory, delayed word recall, memory tasks), and executive function (card sorting, Stroop task) in single studies. However, this was not consistent across studies, serving sizes, or time measured at 1 to 6 h after administration. Some studies showed that lower amounts (120 mg) had a detrimental effect on speed of attention at these acute time periods, 59 whereas the higher amounts (240–360 mg) showed positive effects over 6 h. Only one study, judged as low quality (n = 36), showed statistically significant effects of Ginkgo 120–300 mg/day for up to 1 week duration on short term memory tasks and those effects were more pronounced in 120 mg and among the older group rather than the younger. 50
Studies over the course of 4–8 weeks, in amounts of 80–360 mg/day, are inconsistent and of low methodological quality. One study, at 80 mg, reported statistically significant improvements on tests of memory (n = 60). 54 Another study (n = 61) reported that participants improved on measures of attention/memory (working memory, digit span), executive function (inspection time), and a verbal learning test at 360 mg/day. 51 The largest, acceptable quality study (n = 104), measured performance at 8–12 weeks; no statistical significance was reported for 120 mg/day. 57 The Bond–Lader VAS was commonly reported. As a self-report measure, participants indicated improved alertness, contentedness, and calmness in studies measuring immediate effects, but not longer term studies (Supplementary Table S7). The authors graded the strength of evidence on Ginkgo for enhancing cognitive performance as low, overall. It is important to note the largest published Ginkgo trial [not eligible for the current systematic review] involving 3069 volunteers, 75 years of age and older, with either normal cognition or mild cognitive impairment, studied over the course of 8 years, showed no effect of Ginkgo at 120 mg twice a day on preventing decline (Supplementary Table S8 and Table 1). 63
One study reported minor adverse events (headache and nausea) occurring equally in the Ginkgo compared with placebo group; 2 studies reported that no adverse events occurred and 13 did not describe adverse events. There have been reports of unexplained hemorrhaging, mood dysregulation, and atrial arrhythmias from case reports. 64 –68 G. biloba leaf extract was recently classified as a possible human carcinogen based on studies in animal models. 69 This does not seem to be the case in humans. 70 Natural Medicine database reports Ginkgo as “likely safe” when used orally and appropriately (Supplementary Table S9). 71
Ginseng
Ginseng is widely used to boost energy levels. There are two main varieties, including Panax ginseng (Korean ginseng) and Panax quinquefolius (American ginseng). Both contain ginsenosides, considered the active constituents of the root but differ in terms of chemical makeup. 72 Sixteen studies met eligibility criteria involving 548 participants, 18–60 years of age. Eight studies included college students. 56,60,62,73 –77 Participants were allocated to American ginseng (known as Cereboost in two studies), 78,79 P. ginseng G115 (nine studies), 56,60,74 –77,80 –82 and LAX-101 (one study) 83 ; the remaining studies either reported Korean red ginseng 84 or P. ginseng. 61,62,73 Serving sizes ranged from 100 mg/day of Cereboost and up to 4500 mg/day of Korean Red Ginseng, administered on 1 day and for as long as 12 weeks' duration; the most commonly studied amount ranged from 200 to 600 mg/day. The majority of studies were adequate to high methodological quality with five low methodological quality studies. 56,73,74,82,84
At 200 and 400 mg of P. ginseng G115 and 100 mg Cereboost, significant acute effects (up to 6 h) of calmness were noted in studies, but this was not consistent across trials or time points. Only one trial showed similar results at 4 weeks or greater for 200 mg G115 on calmness and alertness. 80 There is a low strength of evidence, for P. ginseng G115 in amounts of 200–400 mg to acutely effect measures of performance in domains of attention/working memory (Serial three and seven, N-back, quality and speed of attention factor, rapid visual information processing and digit vigilance tasks, numeric working memory) and memory/learning (tests of speed, quality and secondary memory factors, sentence verification, word recognition, immediate and delayed word recall, spatial memory). Although at least three separate trials have examined these amounts and time points, the results and metrics used are not consistent. Two trials showed a decrement in performance at the 200 mg. 56,81 Two studies examined the effect of Cereboost (100–400 mg), with similar effects noted for attention and memory domains. 78,79 Both showed some effect on reaction time. Effects were not evident in any amount greater than 400 mg, up to 6 h after consumption in any trials. Only one acceptable quality study examining 8 weeks' administration of ginseng showed that 200 mg G115 affected working memory on Corsi block and 3-back tasks. 80 No other acceptable quality studies on the chronic administration of ginseng showed significant effects favoring ginseng (Supplementary Table S7). The authors graded ginseng's overall strength of evidence for enhancing cognitive performance as moderate overall (Supplementary Table S8 and Table 1).
Two studies noted no adverse events occurred. The remaining 14 studies did not describe safety or adverse events. Natural Medicines database reports P. ginseng as “likely safe” when used orally and appropriately, short term; it is “possibly unsafe” when used long term due to “potential hormone-like effects.” 85,86 Common side effects seem to be insomnia, headache, and gastrointestinal upset. Severe effects appear to be more common with combination products, where it is challenging to know what ingredients cause such an effect. 87 Case reports have noted inflammatory papules, perioperative bleeding, pulmonary embolism, manic psychosis, but these seem to reflect single cases and are rare. 88 –91 Natural Medicines report that American ginseng is “likely safe” in adults when used orally and appropriately, short term. American ginseng 100–3000 mg daily has been safely used for up to 12 weeks, with rare cases of reported headache (Supplementary Table S9). 92
Omega-3 fatty acids
Omega-3 fatty acids are a type of polyunsaturated fats found in seafood (e.g., salmon, trout, herring, tuna, mackerel), flax seeds, and walnuts. Eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are long-chain n-3 fatty acids found in seafood and commonly touted for heart and brain health. The Dietary Guidelines for Americans recommends adults consume 8 oz. or more of seafood per week. 93 Despite these recommendations, surveys show consumption of omega-3 fatty acids remains low. 94,95 In 1997, GRAS status was granted for up to 3 g/day of EPA and DHA from fish oil. The FDA recommends not exceeding 2 g/day in healthy people wishing to support their diet through dietary supplements. 96 Recently, an omega-3 index (O3I) was developed, as an evidence-based marker of EPA and DHA intake. It is used to assess cardiovascular risk; a risk zone suggests individuals as high risk with an O3I of less than 4%, intermediate risk between 4% and 8%, and low risk greater than 8% O3I. 97,98
Eleven studies published from 2005 to 2019 met eligibility criteria; one study did not have sufficient data on outcomes for treatment compared with placebo. 99 The remaining 10 studies involved 1276 healthy participants, 18–54 years of age. The largest study involved 305 participants. 100 Six studies detailed eligibility criteria, including participants who consumed fish an average of one time or less per week 101 –105 or “who consumed 300 mg/day of LCn-3FAs or less.” 106 Five studies required participants to track their intake through a diet record or self-assessment questionnaire. 102,104 –107 Five studies evaluated fatty acid composition of EPA and DHA, and/or reported an O3I through baseline and post-treatment blood testing and analysis. 101,102,105,106,108 Three studies did not report anything about either consumption or baseline levels. 99,100,109 The highest O3I reported at the start of the trials was a mean of 5.89%, 105 whereas other studies hovered around 2%–3.5%. All studies testing blood levels reported nearly 100% change post-trial, with the highest index mean of 8.72105 and the remaining hovering around 4%–7%. Amounts ranged from 1 to 3 g/day fish oil containing 90–1740 mg/day EPA and 250–1160 mg/day DHA, in varying ratios of DHA/EPA. Studies spanned 5 days and up to 6 months' duration. Three studies were judged as low quality, 99,100,109 with the remaining studies overall rated as acceptable or high.
One low-quality study reported that 20 healthy medical students consuming 750 mg omega-3 fatty acids (EPA/DHA ratio not specified) over 5 days performed statistically better than placebo on psychomotor performance/reaction time tests; participant baseline values were not reported. 109 Three acceptable quality studies demonstrated at least some effect of supplementation as compared with placebo. Jackson et al. 102 found that those supplemented with a 1 g DHA-rich fatty acid performed faster on the Stroop task but worse on names-to-faces task, as compared with placebo after 12 weeks of supplementation. In another study by the same author, 2 g of a DHA-rich fish oil resulted in a statistically significant difference from that of placebo on a rapid visual information processing task after subjects were supplemented for 12 weeks. 103
Stonehouse et al. 105 were the only ones to report an O3I as high as 8% by the end of the trial. A total of 228 healthy adults with low intake of fish who consumed 2250 mg (1.16 g DHA +0.17 g EPA) fish oil over the course of 6 months had a 2.82%-point increase in O3I (5.89–8.72) and had greater statistically significant improvement in both memory and reaction time than the placebo group. It is important to note that a study involving 78 deployed U.S. soldiers consuming 2.5 g DHA+EPA over the course of 60 days revealed that omega-3 fatty acids significantly increased from 3.5 to 6.7 on the O3I; this increase was not associated with improved cognitive performance but was rather inversely correlated with daytime sleepiness. 108 Through exploratory analysis, Leckie et al. 106 found that participants with low baseline DHA who consumed 2000 mg/day of fish oil improved more than those with higher DHA levels (consuming the same amount) on executive function tasks over 18 weeks. No other studies showed improvements on cognitive tasks. The data available are insufficient with regard to any specific amount/formulation or duration of administration within any specific cognitive domain, to evaluate the efficacy of omega-3 fatty acid supplementation as compared with placebo on cognitive performance (Supplementary Table S7). The authors graded the strength of evidence for omega-3 fatty acids as low, overall (Supplementary Table S8 and Table 1).
Four studies reported adverse events among participants in both the placebo and treatment arms. All were minor adverse events to include burping, a fishy aftertaste, queasiness or upset stomach, headaches, rash, or flu-like symptoms. These studies ranged from 4 weeks up to 6 months in duration at various levels and ratios of DHA/EPA. One study reported no adverse events occurred, whereas the remaining six studies did not describe adverse events. Natural Medicines database reports that fish oil is likely safe when used orally and appropriately. 110 Some reports suggest that extremely high amounts (more than 20 g/day) taken over a long time might reduce immune function or lead to increased risk of bleeding or potential stroke when used in combination with certain medications (Supplementary Table S9). 111 –113
Rhodiola rosea
Rhodiola is a plant considered an adaptogen because it helps the body's natural ability to cope with stress. 114 Its root has traditionally been used as medicine, and is commonly used today in dietary supplements to increase energy, reduce fatigue and anxiety, as well as improve athletic performance and mental clarity. Six studies met eligibility criteria for review; one study was excluded from analysis because no statistical data on primary outcomes between Rhodiola and placebo were reported. 115 The remaining studies (three considered of low quality 116 –118 ) involved 209 participants 17–25 years of age. One adequate quality study included young cadets (n = 121) 119 ; the remaining studies (each less than 30) included students who were either physically active 116,117,120 or undergoing examinations. 118 Serving sizes ranged from 100 mg up to 600 mg/day across 1 day and up to 4 weeks duration. Two studies reported using R. rosea extract SHR-5, 115,119 whereas the other three mentioned only the product manufacturer.
One low-quality study showed improvements on a maze test as compared with a placebo when participants consumed 100 mg Rhodiola over the course of 20 days. 118 The largest adequate quality study (n = 121) compared two different amounts (370 and 555 mg/day) to placebo; results showed improved performance with regard to speed and quality of symbol task, short-term memory, and a number arranging tasks at both serving sizes over 1 day. 119 The remaining studies did not show statistically significant improvements compared with placebo, but were overall smaller studies and in amounts lower than 370 mg/day. Evidence for any specific amount or time duration to evaluate the efficacy of Rhodiola on cognitive performance is insufficient at this time (Supplementary Table S7). The authors graded the strength of evidence on Rhodiola for enhancing cognitive performance as very low, overall (Supplementary Table S8 and Table 1).
Two studies reported no adverse events occurred, two did not describe adverse events, and two reported adverse events, including “feeling worse,” headache, and insomnia. Natural Medicines database reports Rhodiola as “possibly safe” when used orally and appropriately, short term. 121 Reports of dizziness and dry mouth have been reported in other studies (Supplementary Table S9). 122
Tyrosine
Tyrosine is a nonessential amino acid; our bodies make tyrosine from phenylalanine, another amino acid. It is commonly used as a dietary supplement with a promise of improving cognitive performance, especially under stressful conditions. Five studies met the review's eligibility criteria, all judged as low methodological quality. One study was excluded from the final analysis as it did not report statistical results compared with placebo on the primary outcomes of interest.
123
The remaining studies
124
–127
included 80 healthy volunteers (some of which were exposed to physical and/or mental stressors), 18–35 years of age. Participants were allocated to either
In single studies, participants who consumed 2 g outperformed those in the placebo arm on tests of stop-signal measuring response inhibition (n = 22) 124 and a task-switching performance reaction time task (n = 22) 127 at 1 h. Single studies at 500 mg and 150 mg/kg showed favorable results for Stroop and digit span (n = 16) 125 and a vigilance and compensation tracking task (n = 20), 126 respectively. For any specific amount or duration of administration or within any specific cognitive domain, the data available to evaluate the efficacy of tyrosine compared with placebo on cognitive performance are insufficient (Supplementary Table S7). The authors graded the strength of evidence on tyrosine for enhancing cognitive performance as very low, overall. It is important to note there are crossover studies that did not meet eligibility under the current review, where participants are exposed to cold stress and show preliminary evidence for improved memory and cognitive performance not combined into this evidence (Supplementary Table S8 and Table 1). 128 –131
None of the five eligible studies reported on any adverse events or safety. Tyrosine used orally in amounts commonly found in foods has received GRAS status in the United States. 132 Natural Medicines database reports that Tyrosine is “possibly safe” when used orally and appropriately in medicinal amounts (up to 150 mg/kg), short term up to 3 months. 133 Reported adverse events include nausea, headache, and fatigue, but mostly at higher amounts (Supplementary Table S9).
Valerian root
Valerian is an herbaceous perennial plant; as a dietary supplement, its root has been advertised as a sleep aid to reduce anxiety and restlessness. Preliminary evidence suggests that valerian root may be effective in reducing insomnia although systematic reviews indicate conflicting results or no statistically significant differences between valerian and placebo. 134 –136 Valerian has been compared with various drugs in an attempt to determine whether valerian is as effective as prescription sleep aids, and could be used in place of drugs to avoid potential side effects, such as impaired cognitive abilities and reaction time. Advertisements suggest that with improved sleep comes better mental alertness.
Three studies published from 1999 to 2004 met eligibility criteria; all were judged low methodological quality. 137 –139 In total, 121 healthy volunteers, 19–60 years of age, were allocated to receive valerian root, a prescription drug (Triazolam, flunitrazepam, or diazepam), or placebo, in varying amounts ranging from 500 to 1800 mg/day; cognitive performance testing took place as short as 2 h after consumption and up to 14 days following administration. The largest study included 102 participants. 139 All studies investigated whether valerian root would alter the ability of performing.
None of the studies showed that consuming valerian produced a negative effect on cognitive performance. If valerian proves to be an effective sleep aid, it could be considered an alternative to other drugs shown to alter cognitive performance. Whereas there is insufficient evidence to evaluate the efficacy of valerian at any specific time point or amount, the largest study conducted, using 600 mg Valerian (LI 156), showed that cognitive performance was not negatively or positively altered at day 1 and after 14 days of administration (Supplementary Table S7). 139 The authors graded the strength of evidence on valerian for enhancing cognitive performance as very low, overall (Supplementary Table S8 and Table 1).
Only one of the three studies discussed safety and adverse events of dizziness, headache, and weakness. Natural Medicines database reports that Valerian is “possibly safe” when used orally and appropriately, short term. The consequences of long-term use are unknown. 140 A few reports suggest that valerian may affect the liver and should not be taken if liver disease is possible. 141,142 A recent case report reports delirium after withdrawal of valerian (Supplementary Table S9). 143
Discussion
The purpose of this review was to evaluate the evidence on the efficacy and safety of single dietary supplement ingredients frequently marketed with claims for enhanced cognitive performance in otherwise healthy adults. Nine of the 54 ingredients had at least 3 publications meeting eligibility criteria for systematic review across 69 publications. The quality of the evidence is low across the majority of ingredients evaluated. Our confidence in any effect is limited for enhancing cognitive performance when assessing any specific serving size, time point, or duration of administration.
The authors attempted to evaluate safety of these specific ingredients. Although reported adverse events are documented in Supplementary Table S9, these may not be directly related or may not translate to the adverse events or severity of any one particular product someone might purchase. Unknown variability in the quality and formulation from product to product is common. In fact, the authors analyzed 24 products marketed for brain health and cognitive performance and found that the majority of product labels appeared as misbranded and some found to contain prohibited ingredients and drugs. 2,9,144
The low level of certainty in the state of the science, coupled with not knowing what is in the product bottle, makes weighing risks and benefits difficult; these data also hinder the ability to develop recommendations about using such ingredients for consumers interested in boosting their cognitive performance. Whereas certain trends regarding promising serving sizes or duration of use have been pointed out, when combined, studies are inconsistent and imprecise, and many are methodologically flawed.
Limitations
The authors acknowledge the limitation of only including randomized clinical studies in the current review. The primary objective was to evaluate efficacy of the ingredient compared with placebo; since dietary supplements are standardly administered in capsule or tablet form, these studies should be comparable to the methods required of drug trials, which are upheld to the standard RCT study design to avoid bias from selection and confounding factors. 145 The challenge with these studies, however, is a lack of sufficient funding to conduct robust, large-scale trials to yield definitive answers regarding efficacy. In addition, dietary supplements are not upheld to the same regulations as drugs and therefore manufacturers are not required to conduct RCT trials.
To yield definitive answers, research needs to be reproducible, which means the product under investigation must be reproducible. This is sometimes unknown with supplement trials and most have undergone no trials whatsoever. Research into bioavailability, and which parts of plants are bioactive is ongoing. Some ingredients are standardized extracts, such as in the case of Ginkgo Egb761 or P. ginseng G115. Even with these standardized extracts, however, one does not know if the product contains any additional or contaminated elements. 146 –148 This should cause concern regarding heterogeneity and would affect the consistency across trials when grouped for systematic review.
In addition, this review only looked at ingredients considered as monotherapies, not combination products, which are typical of products on the market. The challenge with studying combination products is the uniqueness of every product—this does not allow for combining various ingredients in and across products in a systematic review to develop definitive answers concerning efficacy. To understand whether an ingredient should first even be present on a dietary supplement label, some evidence for efficacy and safety as a monotherapy should exist before combined with other ingredients, to perhaps “bolster” any claimed effects. This remains a serious concern.
Research gaps
Research gaps, identified by the authors through the systematic review and spanning across all ingredients, were examined with an expert panel. Using a modified Delphi process, panelists prioritized research gaps, and recommended potential solutions to address the gaps, as detailed in a separate article (under review). Gaps related to dietary supplements research included the need for quality testing of products used in research, the question of bioavailability and absorption of ingredients, as well as the optimal composition or standardization of supplements under investigation. Other gaps related to the populations studied; in general, there seemed to be a current bias toward focusing on diseased populations, rather than maintaining or optimizing performance in a healthy population. The lack of uniform cognitive performance measures and metrics used across research is a gap, as well as whether these are accurate representations of or even generalizable to “real-life” participants wishing to optimize their performance. Methodological quality and ethical concerns in the conduct and reporting of science encompass all of these. Gaps specific to each ingredient, priorities, and potential research directions are detailed in Table 1.
Applicability to practice
The authors found 650 products on the market with claims of enhanced cognitive performance, such as improved memory, attention, focus, energy, and motivation. These claims require scientific backing, often in the form of reproducible clinical trials, with the specific claim in mind. 149 However, peer-reviewed published clinical evidence is not required of a manufacturer before entering the market. In addition, they are considered safe until proven otherwise. Multiple reports of labels not matching what is contained in the product and some containing ingredients that are actually drugs are available. Some products or advertisements contain scientific-sounding claims such as “clinically proven” or “research suggests it works the first time you take it.” The research to support these claims is rarely cited; if language is available on a website, it is often questionable how such research translates to a “trusted” claim for the specific product advertised. Much remains to be investigated.
Conclusions
The claims made on product bottles and through advertising do not match the science as conclusive evidence that these ingredients work for healthy adults wishing to enhance their cognitive performance. Until future research addressing gaps in the research field are resolved, it will continue to be a challenge in weighing any risk to benefit for many of these ingredients to inform decision making about their use.
Footnotes
Authors' Contributions
P.A.D. and C.C. designed research; C.C. and C.B. conducted research; C.C., C.B., and P.A.D. analyzed data; C.C., C.B., and P.A.D. wrote and edited the article; and C.C. and P.A.D. had primary responsibility for final content. All authors read and approved the final article.
Acknowledgments
The authors would like to acknowledge Ms. Andrea T. Lindsey, Director of Operation Supplement Safety (
Author Disclosure Statement
The authors have no financial interests or relationships to disclose.
The opinions and assertions expressed herein are those of the author(s) and do not reflect the official policy or position of the Uniformed Services University, U.S. Special Operations Command, or the Department of Defense. The contents of this publication are the sole responsibility of the author(s) and do not reflect the views, opinions, or policies of The Henry M. Jackson Foundation for the Advancement of Military Medicine.
Funding Information
Funding for this work was provided by the Preservation of the Force and Family Behavioral Health Program, Uniformed Services University award number HU0001-15-2-0053, and the Consortium for Health and Military Performance.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Table S9
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.