
Abstract
Abstract
Background:
The routine integration of traditional Eastern medicine with modern Western medicine can be of great benefit to providers and patients. Practitioners of Western medicine who are unfamiliar with herbal medicine and acupuncture would benefit from a set of simple guidelines for incorporating these techniques in the treatment for a number of common complaints.
Materials and Methods:
This article introduces a new set of uniquely defined rules (in the form of algorithms) for selection of medicinal herbal preparations and acupoints that can be used by physicians with no prior knowledge of Traditional Chinese Medicine and examines preliminary outcomes in terms of symptom relief after applying these rules for treatment in a group of 987 female patients with headaches, neck/shoulder stiffness, dizziness, low-back pain, or menstrual cramps. Among these patients, 497 were treated with herbal medicine and 490 were treated with acupuncture.
Results:
Overall, the treatments were considered to be highly effective in >80% of cases. Acupuncture was more effective for musculoskeletal complaints (i.e., neck/shoulder stiffness, low-back pain), while herbal medicines had a greater effect on headache, dizziness, and menstrual cramps.
Conclusions:
Acupuncture provided a more-rapid onset of symptom relief than herbal medicine.
Introduction
P
Materials and Methods
A total of 987 female patients seen at a single center in Japan (traditional/Eastern medicine department) from July 2005 to May 2013 were included in this study. The patients were treated for headache, neck/shoulder stiffness, dizziness (including lightheadedness and lightheadedness upon standing), low-back pain, or menstrual cramps according to preset algorithms (Figs. 1 and 2). Underlying medical or surgical causes of symptoms were ruled out by standard laboratory or diagnostic studies in all cases. Of the 987 patients, 497 chose treatment with herbal medicine and 490 chose treatment with acupuncture.
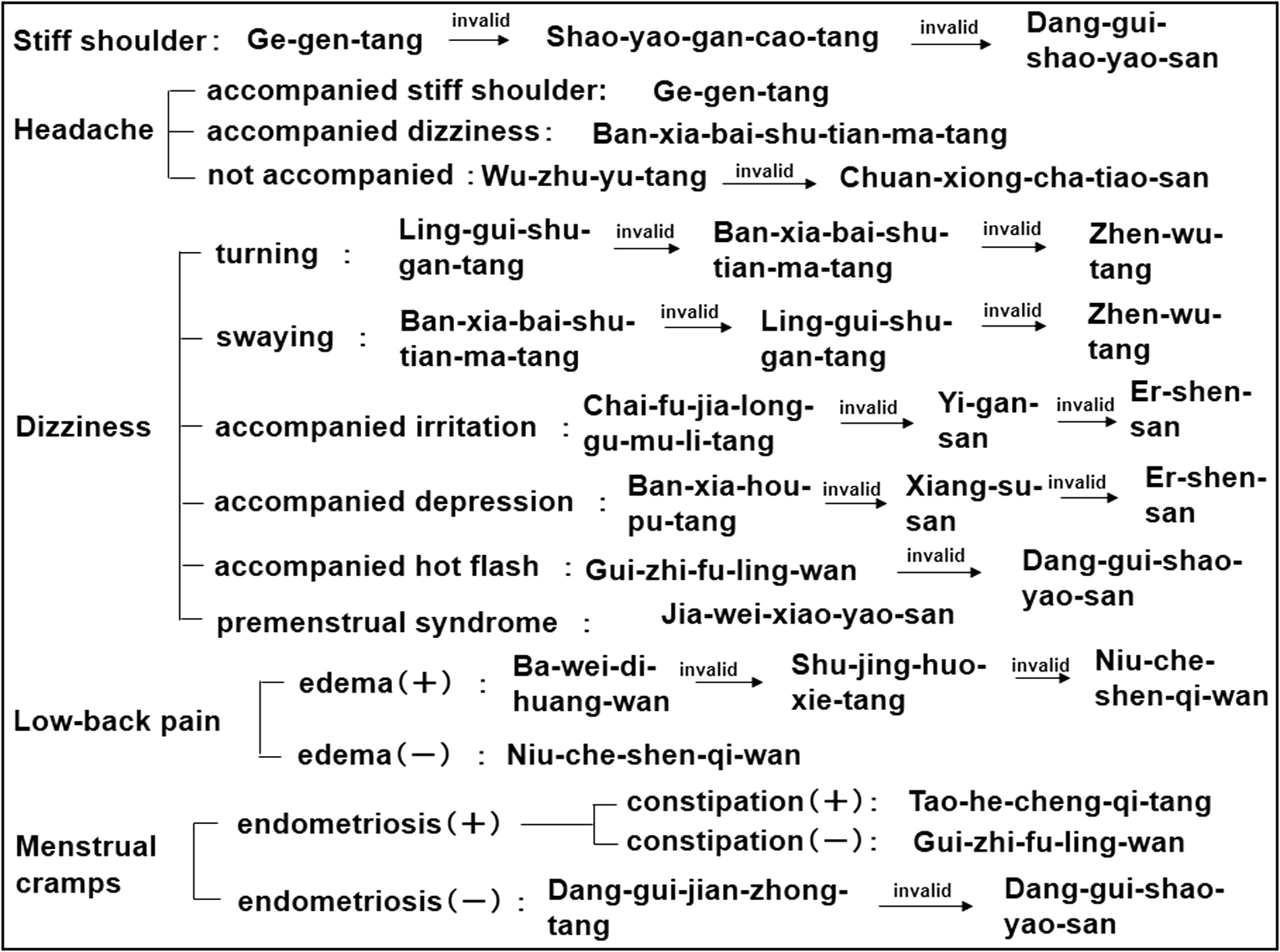
Algorithms for selection of medicinal herbal preparations (Kampo extracts). These treatment algorithms were devised according to original texts (Shanghan-lun, Jinkui-yaolue, Heji-jufang, and Wanbing-huichun) and extant instructions passed down orally by ancient practitioners of herbal medicine.
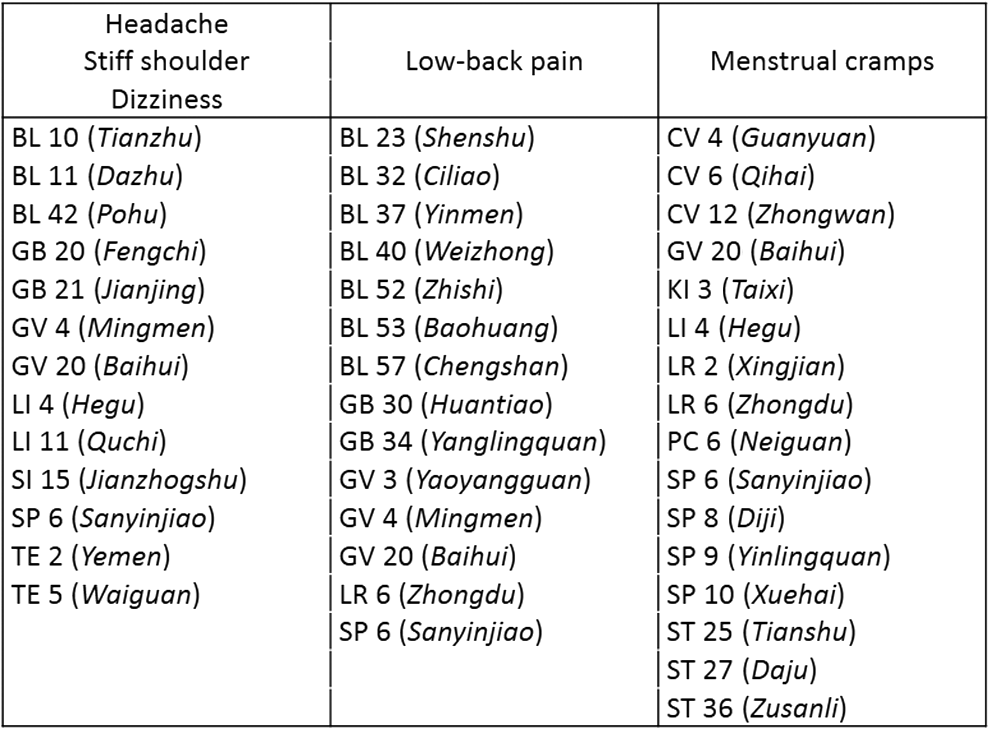
A guide to acupuncture points used to select meridians and acupoints. The selection of acupoints was based on the literature regarding the acupuncture points frequently used to treat the conditions described.
The unique algorithm devised by the current author for the selection of medicinal herbal preparations (Kampo extracts) is shown in Figure 1. Each extract was used for an initial period of 2 weeks to 1 month at a minimum dose of 3 packets per day. If no reduction of symptoms was noted at the 1-month follow-up examination, a new extract, according to the next step of the algorithm, was prescribed; similar steps were followed, when applicable, at the 2-month follow-up examination. Patients who had no reduction of symptoms after 3 months of treatments in accordance with the algorithms were considered nonresponders. In patients who had some, or slight, but not complete, symptom relief, the dose of the Kampo extract was increased to 4 packets per day. Patients who reported complete symptom relief (i.e., those who unhesitatingly responded “yes” when asked “Were your symptoms eased?”) were deemed to be responders. Patients who were prescribed 2 or more daily Kampo extracts were instructed to take the extracts >30 minutes apart. Instructions for taking the extracts did not specify that they be taken before, during, or after meals. Patients were allowed to take extracts with liquids other than water. When taking an extract, patients were allowed to take up to 2 packets each time.
For the patients who chose acupuncture treatments, needles were placed in accordance with the guideline for selection of acupoints shown in Figure 2. Patients seen for menstrual cramps were evaluated for endometriosis by ultrasound during initial visits. All acupuncture treatments were performed using disposable needles (2-gauge, diameter 0.18×length 40 mm; Seirin Corporation) with a guide tube; needles were inserted to a depth of 4–5 mm and tapped gently into place. Patients with menstrual cramps were treated in a supine position and those with symptoms other than menstrual cramps were treated in a prone position. Needles were left in place for 15 minutes in all patients. Patients were checked for symptom relief 1 week after completion of 6 acupuncture sessions (one session per week). Patients who had no reduction of symptoms whatsoever at the first follow-up visit, 1 week after the six weekly acupuncture sessions (or, in the case of menstrual cramps, at follow-up immediately after the first post-treatment [6 sessions] menstrual period) were considered nonresponders. When any reduction of symptoms was noted during the course of the initial six sessions, the acupuncture treatments were continued, and the patients who unhesitatingly responded “yes” when asked “Were your symptoms eased?” were considered responders. The decision to provide six sessions of acupuncture treatment was based on a previous study 19 reporting that symptoms, such as headaches, dizziness, neck/shoulder stiffness, low-back pain, or tinnitus were reduced as a result of an average of six acupuncture sessions. Responders who completed their first acupuncture trial before June 2012 were evaluated further for symptom recurrence, and recurrence rates for each symptom were calculated.
Treatment results and differences in efficacy between herbal medicine and acupuncture were analyzed by a ratio test with a significance level of 0.05. The ratio test allows comparison of ratios between two groups based on the theory that a difference of ratios obeys a standard normal distribution. The z-value corresponding to p=0.05 in a standard normal distribution is 1.96. A t-test with a significance level of p=0.05 was used to test for significant differences in the time (in days) to symptom relief produced by herbal medicine or acupuncture. The ethics committee of the corporation, where current author is affiliated, approved this study, and informed consent for participation was obtained from the patients. Patient data were carefully retained at this center, and information that could identify individuals was redacted in order to protect private information.
Results
Acupuncture treatments were generally more effective than herbal medicine for addressing common musculoskeletal complaints (i.e., neck/shoulder pain; low-back pain), while the Kampo preparations (herbal medicine) provided greater symptom relief for headache, menstrual cramps, and dizziness. These differences were statistically significant for menstrual cramps and dizziness (Tables 1 and 2).
The rates of effectiveness of acupuncture and herbal medicine for each symptom are shown in Table 1. The results of a comparison of the rates of effectiveness of acupuncture and herbal medicine by a ratio test with z-values are shown in Table 2.
Results of comparisons of the number of acupuncture sessions or the number of days of herbal medicine used until improvement appeared and until symptom relief are shown in Table 3.
Given that the first session took place during each patient's initial visit, the time (in days) to improvement was determined by subtracting 1 from the number of total sessions and multiplying the result by 7. The statistical comparison of the efficacy of acupuncture versus herbal medicine was performed with a t-test based on time (in days) until improvement appeared and until symptom relief. These results are shown in Table 4.
Recurrence rates and the time (in days) from completion of acupuncture until symptom recurrence are shown in Table 5. The number of additional acupuncture sessions required for symptom reduction after recurrence is also shown in Table 5.
Ages (mean and standard deviations) of responders and nonresponders to each treatment type are shown by symptom in Table 6. These data were evaluated for significance by t-test, and the results (p-values) are also shown in Table 6.
SD, standard deviation.
Herbal Medicines
The three Kampo preparations that were most effective for treating neck/shoulder stiffness were Kakkon-to (Gegen-tang in Chinese), Shakuyaku-kanzo-to (Shaoyao-gancao-tang in Chinese), and Toki-shakuyaku-san (Danggui-shao-yao-san in Chinese). Response rates, respectively were 87.5%, 7.5%, and 2.5%. The three preparations that were most effective for headache were Hange-byakujutsu-temma-to (Banxia-baishu-tianma-tang in Chinese), Goshuyu-to (Wu-zhu-yu-tang in Chinese), and Senkyu-chacyo-san (Chuanxiong-chatiaosan in Chinese). The response rates were, respectively, 49.5%, 22.3%, and 18.5%. The three herbal preparations that were most effective for dizziness were Hange-byakujutsu-temma-to, Ryo-kei-jutsu-kan-to (Ling-gui-shu-gan-tang in Chinese), and Shimbu-to (Zhenwu-tang in Chinese). The response rates were, respectively, 53.6%, 33.3%, and 4.4%. The herbal preparations that were most effective for menstrual cramps were Toki-kencyu-to (Danggui-jianzhong-tang in Chinese), Keishi-bukuryo-gan (Guizhi-fuling-wan in Chinese), and Tokaku-joki-to (Tao-he-cheng-qi-tang in Chinese). The response rates were, respectively, 40.7%, 21%, and 12.4%. The herbal preparations that were most effective for low-back pain were Hachimijiogan (Bawei-dihuang-wan in Chinese), Sokei-kakketsu-to (Shujinghuoxie-tang in Chinese), and Gosha-jinki-gan (Niu-che-shen-qi-wan in Chinese). The response rates were, respectively, 72.7%, 15.2%, and 9.1%.
Acupuncture Treatments
Overall, patients who chose acupuncture had shorter times to symptom relief than those who used the Kampo preparations (Table 3 and 4), and when the acupuncture-treated patients were assessed for recurrence of symptoms, >80% of these patients remained symptom-free for ≥1 year (Table 5). In the event of symptom recurrence, all symptoms were reduced with 1–2 additional sessions of acupuncture. Acupuncture was found to be perennially more effective than herbal medicine.
Discussion
Although the physiologic mechanisms of patient responses to acupuncture and herbal medicine have not been clarified scientifically, the fact that these treatments have survived for centuries and handed down from generation to generation by written and oral traditions, should stand as evidence of their efficacy. In recent years, practitioners and patients of “modern” Western medicine have shown increasing interest in the benefits of these traditional Eastern medicines. Western physicians who wish add the time-honored tools of Eastern medicine to their practices would benefit from a set of simple guidelines to traditional Eastern treatment approaches to such commonly reported symptoms as headache, shoulder and neck pain/stiffness, low-back pain, dizziness, and menstrual cramps, particularly for patients in whom no specific underlying surgical or medical disease has been found.
The current author prepared a set of simple guidelines for using herbal medicine and acupuncture for practitioners who have little or no previous knowledge of these techniques. These treatment algorithms were tested in a group of 987 female patients treated over a period of several years at a single center in Japan. The results of this study indicated that, overall, these treatments provided effective symptom relief in ≥80% of cases. The current author's algorithms can guide practitioners in providing Eastern medicine therapies for their patients, and the comparison of the efficacy of herbal medicine versus acupuncture may help clinicians and their patients chose the best course of treatment depending on the patients' symptoms.
As noted above, patients who chose acupuncture had shorter times to symptom relief than those who used the Kampo preparations (Table 3 and 4), and >80% of these patients were symptom-free for ≥1 year (Table 5). When symptoms recurred, 1 to 2 additional sessions of acupuncture provided symptom relief. Acupuncture was found to be perennially more effective than herbal medicine.
There were no statistically significant differences in the ages of patients in terms of response and nonresponse to either treatment method (Table 6), except among those treated with acupuncture for low-back pain (there were a greater number of responders among older patients) and patients treated with herbal medicine for headache and stiff neck/shoulder (there were a greater number of nonresponders among older patients).
Taken together, the results indicate that headaches, neck/shoulder stiffness, dizziness, low-back pain, and menstrual cramps can be treated successfully using the simple guidelines for Eastern medicine presented here, even when applied by a physician with little or no prior knowledge of these traditional methods. The guidelines include algorithms for treatment using herbal medicines (Kampo extracts) as well as rules for selection of acupoints. As acupuncture had a more immediate effect than herbal medicine, it may be the treatment of choice for patients who can make weekly visits, while herbal medicine is a preferred treatment for patients who are unable to do so. The method of acupuncture used in this study is a pain-free treatment involving needles inserted to a depth of 4–5 mm, and it is a practical and effective treatment that can be provided in a relatively brief office visit.
An ideal number of weekly acupuncture sessions has not been established. The treatment guideline presented here involves one session weekly over a 6-week period, because this schedule is reasonable for most patients, and because the author has previously found 19 that acupuncture treatments given according to this schedule have reduced symptoms, including headaches and others. However, the possibility that patients who were found to be nonresponders may have had relief with a different frequency of treatments, or with additional treatments, cannot be excluded. The establishment of ideal treatment schedules for acupuncture should be the topic of a future study, and the continued improvement of simple treatment algorithms for acupuncture and herbal medicine that can be used effectively across medical disciplines should always be sought.
Conclusions
Simple guidelines to assist practitioners of modern Western medicine who wish to provide integrative treatments, including acupuncture and herbal medicine, will be of benefit to both patients and practitioners. In the present preliminary observational study, simple treatment algorithms for acupuncture and herbal medicine were applied in a large group of female patients, and both approaches were found to provide relief from common symptoms including headaches, neck/shoulder stiffness, dizziness, menstrual cramps, and low-back pain. Overall, acupuncture had more immediate action than herbal medicine.
Footnotes
Disclosure Statement
No competing financial interests exist.