
Abstract
Abstract
Introduction:
This article presents a comprehensive and systematic auricular diagnosis protocol that summarizes 14 different and specific ear acupuncture point (EAP) diagnosis routes and covers 165 EAPs distributed on the ear that are organized around the anatomical structure and organ systems of the human body.
Methods:
Strategies used for auricular diagnosis are described, including visual inspection, palpation, auricular electrical detection, and differentiation. In particular, auricular electrical detection is an objective diagnostic method for identifying acupoints by assessing auricular cutaneous resistance. Illustrations related to clinical observations of skin-surface changes in the ear and related body symptoms are presented. This protocol can be used to diagnose and differentiate diseases/symptoms in the corresponding body areas. This article provides valuable information related to auricular diagnosis and disease differentiation.
Conclusions:
Empirical studies will be needed to validate the procedures and diagnostic accuracy for diseases/symptoms. Auriuclar diagnosis is an objective, painless, and noninvasive method, and, if found effective, can be used as a complementary approach by health care professionals in practical applications for screening and treating health problems.
Introduction
A
Paul Nogier, MD, a French neurologist, theorized in 1950 that the ear represents the inverted fetus within the womb and that somatotopic mapping can be found between EAPs and their corresponding body areas. 4 The whole anatomical body relationship to EAPs in Chinese ear medicine has been modified according to Nogier's theory.1,5 The first scheme of standardization of auricular points was approved at the International Conference on the Standardization of Acupoints, held in South Korea in June of 1987. 1 The “Chinese Standard Ear-Acupoints,” including 91 points and represented by zones, was established and widely adopted in China. 6 However, different Chinese and French somatotopic maps have developed. Since the end of the 1980s and the beginning of the 1990s, auricular diagnosis and treatment have become a unique branch of acupuncture and moxibustion around the world.1,5 The World Health Organization considers auricular medicine to be a form of microacupuncture that can affect the whole body. 6
Auricular Diagnosis
Differing from body acupuncture, which works on the meridian basis whereby health is promoted through balancing Yin and Yang, auricular therapy works on a microsystem basis, with the ear as a self-contained microsystem that can affect the whole body. Normal auricular points are flat and have normal skin color. When a person suffers from disease in various parts of the body, the EAPs may show a decrease in auricular cutaneous electrical resistance, a decrease in pain threshold,1,5 discoloration, deformity, papules, or angiosclerosis.1,7 Thus, physical conditions can be identified through auricular examination. Such changes are not usually observed in body acupuncture points. Experimental and clinical scientific studies have accumulated evidence of surface changes of ear skin (e.g., the presence of an ear lobe for coronary heart disease8–11 ), and electrodermal skin-resistance changes (e.g., stomach and duodenal ulcer disease, 12 liver and viral hepatitis, 13 musculoskeletal pain 14 heart disorders 15 ). These neurobiology and pathophysiology studies have provided support for auricular diagnosis.
In addition to ear skin-surface changes, auricular diagnosis is mainly based on changes of electrical resistance. Electrodermal measurement (using an electrical acupoint finder) is an objective diagnostic method for identifying acupoints by assessing the auricular cutaneous resistance.1,5 Lower resistance identifies the acupoint that indicates the corresponding body part with the symptoms/illness. This method of acupoint identification has been validated using functional magnetic resonance imaging. 16 However, body acupuncture points do not always show a pattern of low skin resistance 17 and positive skin-surface changes. 7 The electronic point finder described in this article is manufactured by the Auricular Medicine International Research & Training Center (AMIRTC; Fig. 1). The acupoint locator is connected to two probes, one held by the patient and the other by the examiner (hereafter, referred to at the “detecting” probe). During electronic detection, normal EAPs emit a very low sound (of low tone and frequency) or no sound. When the corresponding part of the body has a symptom or problem, the electrical resistance of the EAP changes, causing the acupoint finder to emit a sound. When a person has pathologic changes in the body, functional-related EAPs can have different positive reactions.

Electronic point finder.
Methods
This article presents comprehensive and systematic auricular diagnosis protocols, including 14 different specific EAP diagnosis routes that cover 165 EAPs distributed on the ear, and organized around the anatomical structure and organ systems of the human body (Fig. 2). The ordered series of 14 diagnosis routes includes: (1) abnormal blood pressure detection; (2) reproductive system; (3) urinary system; (4) liver, gallbladder, and spleen; (5) digestive system; (6) abdominal cavity, (7) cardiovascular system; (8) respiratory system; (9) five sense organs; (10) endocrine system, (11) neurologic system, (12) locomotor system, (13) immunologic system and (14) tumor-specific areas I and II. Following the anatomical structure of the auricle, the detection should proceed as follows: triangular fossa→cymba conchae→helix crus→cavum conchae→tragus→tragic notch→antitragus→earlobe→antihelix→upper antihelix crus→lower antihelix crus→upper antihelix crus→lower antihelix crus→scapha→helix→auricular posterior. Figure 1 presents the 14 routes of detecting procedures.
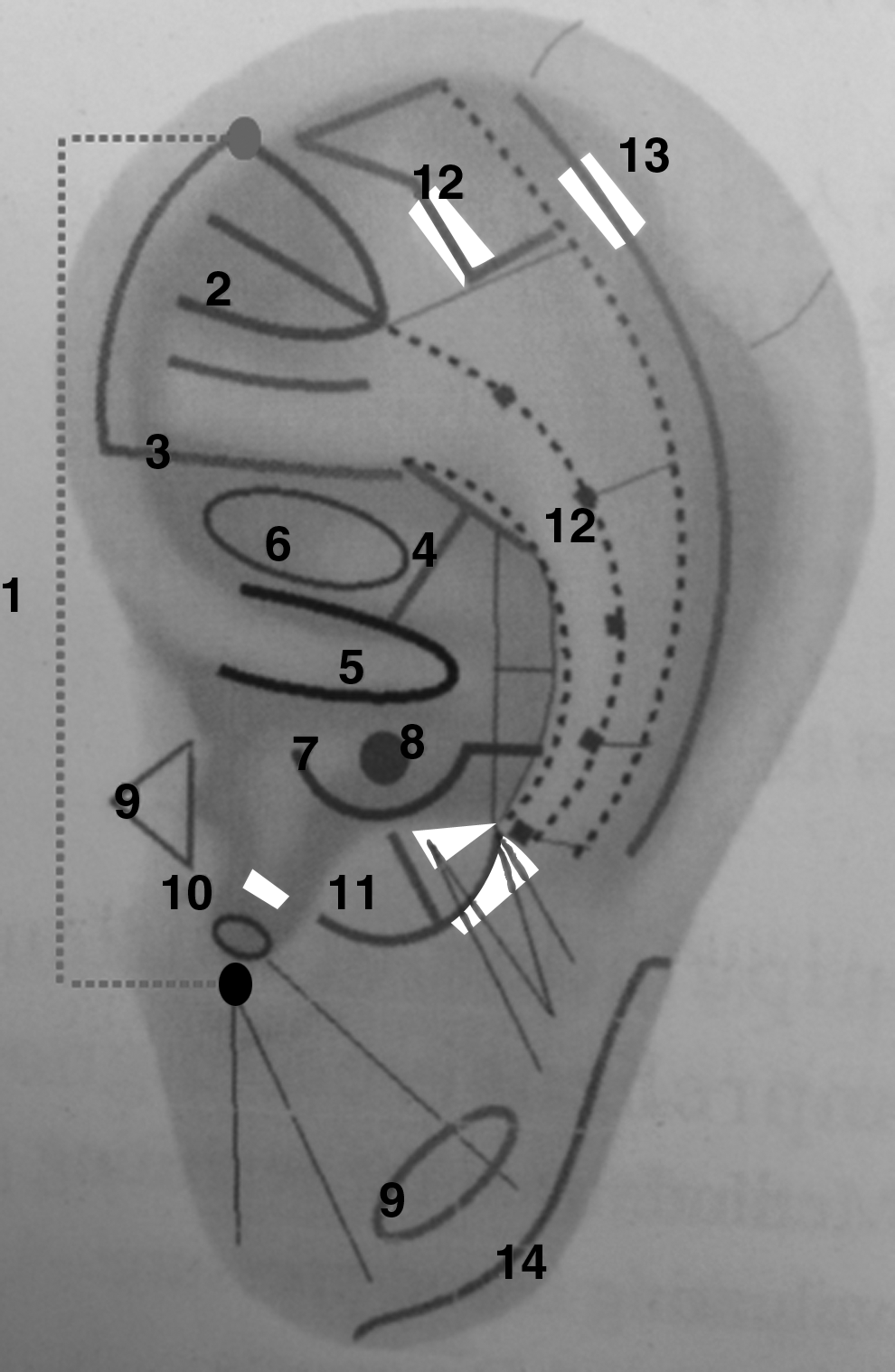
Fourteen routes of systematic auricular diagnosis protocol summarized by Li-Chun Huang: (1) blood-pressure detection; (2) reproductive system; (3) urinary system; (4) liver, gallbladder, and spleen; (5) digestive system; (6) abdominal cavity; (7)cardiovascular system; (8) respiratory system; (9) five sense organs; (10) endocrine system; (11) neurologic system; (12) locomotor system; (13) immunologic system; (14) tumor-specific areas I and II.
Detection of EAPs
Two special manipulations assist in detecting EAPs as described in the next two sections.
Finger-exposure method. Auricles are composed of uneven cartilage. EAPs are distributed on these uneven surfaces or embedded into the concave area of the ear. Embedded EAPs in the cartilage require using finger-exposure techniques to locate the positive points. To expose embedded EAPs (using the right ear as an example), the examiner's left thumb and index finger are used to hold the auricle, and the middle figure is used on the posterior of the ear to expose the targeted EAPs. The right hand holds the detecting probe and the left fingers move wherever the probe moves. The EAPs are examined to detect low electrical resistance, tenderness/sensitivity level, and point and morphologic changes.
Points are distributed on the ear as follows:
(1) Triangular fossa—Uterus, Decrease Blood Pressure point, Fallopian Tube
(2) Cymba concha—Kidney, Liver, Gallbladder, Prostate
(3) Tragus—Pharynx, Larynx, Glottis, Internal Nose, Nasopharynx
(4) Antitragus—Brain, Nervous Subcortex, Digestive Subcortex, Cardiovascular Subcortex, Testicle
(5) Antihelix—1, 2, 3, 4 Cervical Vertebrae.
Pressure application. Appropriate pressure on the EPAs may be needed during the examination. In the concave area of the ear, electrical resistance of ear skin is relatively low and is relatively sensitive. There are many nerve branches, sebaceous glands, and sweat glands distributed in the concave areas of the auricles and, thus, it is typical to have low-resistance points in these areas. If a positive EAP is identified in a concave area, then more pressure should be applied to make sure that it is truly positive, while gliding the detecting probe forward and backward 2–3 times. During the diagnosis, if the points are checked according to their distributed anatomical directions, then it is possible to detect whether or not a point is positive; otherwise, it is hard to find positive points. During the detecting process, if a low resistance point is detected, then there is a need to change the examining directions to make sure that the diagnosis will be accurate. During diagnosis, the physiologic low-resistance points must be differentiated from the pathologic low-resistance points.
Special Characteristics of Some EAPs
EAPS based on TCM. According to TCM, some EAPs are one-point, multiple-disease types, especially EAPs of the TCM Zang–Fu theory. These EAPs require a combination of the Western medical theory and the TCM Zang–Fu theory to make an accurate diagnosis. Table 1 lists the differences of diagnostic results between TCM and auricular diagnosis. As distinct from TCM, which is based on tongue or pulse diagnosis, auricular diagnosis provides a more scientifically grounded method for identifying areas of pathology in the body.
Positive EAPs. Some EAPs are continuously active for all 24 hours, such as the Sympathetic, Endocrine, and Uterus EAPs. For these points, physical low-resistance points must be carefully differentiated from pathologic low-resistance points. The following EAPs are physiologically sensitive points, also called normal physiologic low-resistance points or false–positive points. These EAPs include locations at the helix clavicle (Shoulder Joint, Shoulder Elbow, Wrist, Finger), triangular fossa (Uterus, Shenmen), lower helix crus (Mouth, Esophagus), cymba concha (Large Intestine, Bladder, Kidney, Prostate), tragus north (Endocrine), and cavum conchae (Heart, Lung, Sanjiao).
EAPs for treatment only. Based on characteristics/functionalities of EAPs, some points are for treatment only and, thus, it is not necessary to examine them for diagnosis. These EAPs include nerve-system points (i.e., Sympathetic, External Sympathetic, Lesser Occipital Nerve, Large Auricular Nerve, Vagus Nerve Point, Vagus Nerve, Facial Nerve, Stimulation Point of Nasopharyngeal, Hybrid Branch Nerve, Sciatic Nerve, Brain Stem, Thalamus); specific points (Decrease Heart Rate Point, Hungry Point, Exciting Point, Libido Point, Drunk Point, Tumor Specific Area II); endocrine-system points (Endocrine, Gonadotrophin, Adrenal Gland); TCM points (Shenmen, Liver Yang); corresponding points (Buttock, External Ear, External Nose, Parotid Gland, Eye I and Eye II, Larynx, and Teeth); and EAPs that are based on anatomical names (Ear Apex, Helix 1–6, Tragus Apex).
Auricular Diagnosis Strategies
Before diagnosis (using the left ear as an example), the examiner can use the left hand to fix auricles and use the right hand to hold the detecting probe, and vice versa for right ear. The examiner needs to apply appropriate pressure and intensity during the detection. It is important (1) to ensure that the detection time for each EAP is equal and (2) to avoid repeated detection of any EAP. Then, the examiner needs to conduct the detection for each of the 14 different specifically designed detection routes. In auricular diagnosis, the left ear is believed to reflect the medical condition of the left side of the body, while the right ear reflects the medical condition of the right side of the body.
The examiner should note any false–positive points and the points that are normal anatomical points. Four strategies are used for auricular diagnosis.
(1) Visual inspection. This is used to observe the ear skin surface changes, such as discoloration, deformity, desquamation, papules, and angioplerosis on the auricle. If the body diseases are acute, EAPs have a fresh red discoloration. If the body has chronic or organic disease, the skin of the EAPs lacks brightness. Discoloration includes white, dark, and brown spots. When there has been surgery in the body, a surgical scar is visible in the ear.
(2) Palpation. This diagnostic method allows the examiner to observe any subtle abnormalities apart from the natural uniformity of the ear's surface with the detecting probe used to examine EAPs. The morphology of the symptomatic body can cause skin-surface changes, including modules, cord-like protrusions (cords), depressions, and edema. When the detecting probe glides along the auricular skin surface with these morphologic changes, the examiner should be able to feel the different sensations. These reactions form the basis of the clinical auricular diagnosis. During the diagnosis process, three marks may be observed:
(1) Permanent mark—For chronic and organic diseases, a permanent mark remains on the auricular surface after the disease has been cured.
(2) Tenderness—Corresponding EAPs of symptomatic body parts usually reveal a change in tenderness of the ear during the examination. Thus, the patient's reaction during the detecting probe glides along the auricular surface skin should be observed. The more severe the symptoms, the greater the tenderness that will be felt by the patient.
(3) Pressing mark—A press mark is observed when a detecting probe is used to press the auricular surface. Pressing marks differ in depth, coloration, and recovery time. If the body has symptoms or disease, patients feel tenderness when the detecting probe is used to examine the EAPs.
(3) Auricular electrical detection. This is a diagnostic method that measures auricular cutaneous resistance (mainly on detecting low electrical resistance points). Analyzing the auricular points and recording the results can be used as references for diagnosis and serve as a foundation for point selection. Low resistance can be 10–15 times lower than normal value when there are pathologic changes in the body. A high volume of noise at an EAP indicates that the EAP is most likely the one related to the disease. The EAP that has highest volume of noise is the key point for the diagnosis. Low electrical resistance is an important basis for auricular diagnosis.
(4) Differentiation. The changes of EAPs can be multilevel and multiformat. When a human body is normal, the EAP is just a point—a functional point or an anatomical point. It has no positive reactions (surface-skin color change, normal resistance, normal pain threshold). When there are any pathologic changes in the body, EAPs will manifest as auricular skin-surface changes, which may be detected as “areas,” “grooves, or other “shapes” (i.e., modules, cords, depressions, and edema). Clinical observation shows that EAPs can display forms or patterns known as Thread, Groove, Axis, Channels, Triangles, or Rings. These changes are the basis of differentiation for auricular diagnosis.
Fourteen Routes of EAPs Diagnosis
(1) Abnormal blood pressure detection. To detect both decreased and raised Blood Pressure points, the examiner can (1) use the middle finger of the left hand to hold up the decreased Blood Pressure points, and (2) use the right hand to hold the detecting probe and move downward from the upper border of the triangular fossa to the exterior upper crus of the triangular fossa. One should pay attention to the electrical resistance changes of the EAPs and check whether or not there is a cord. If there is a cord, then the diagnosis is most likely to be arteriosclerotic hypertension. For the raised Blood Pressure point, the examiner needs to use the detecting probe to make horizontal linear movements from Eye 2 to Eye 1 at the tragus notch and repeat 2–3 times. The judgment of abnormal blood pressure is based on the change between two points (decreased Blood Pressure point and raised Blood Pressure point). A groove of hypotension can be observed in the earlobe (Fig. 3).
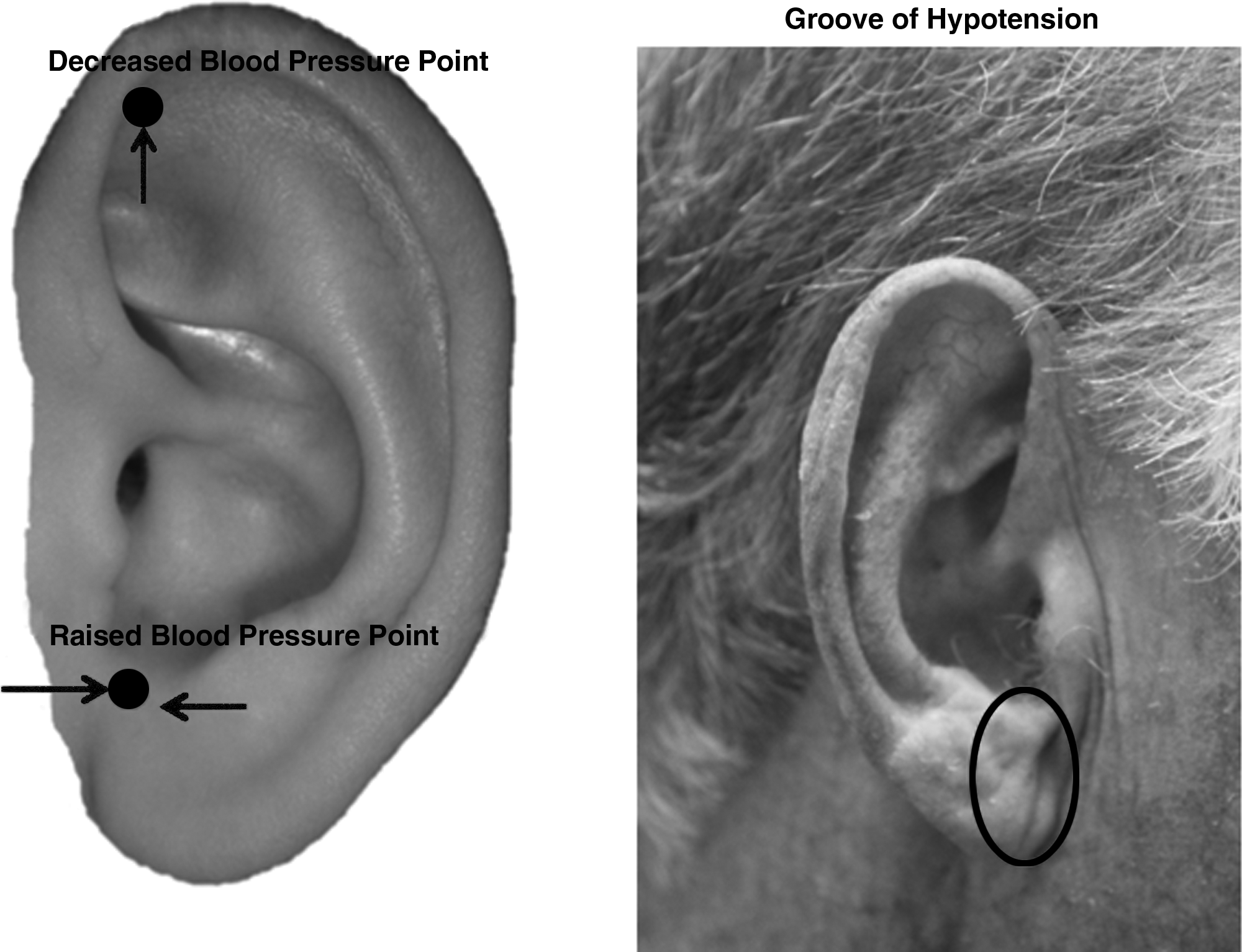
Abnormal blood-pressure detection.
(2) Reproductive system. The detection route is “one-point, three-lines.” The Hepatitis point, located on the upper line, is used to judge liver function. On the upper line, the Fallopian Tube point—which is close to the Hepatitis point and Cervix EAPs—is the main point used to detect problems related to inflammation if the electrical detection is positive without other skin-surface changes; tubal stenosis if electrical detection is positive with a cord in the skin surface; or nodular salpingitis if electrical detection has a positive reaction with a nodule. The middle line is used to detect reproduction problems (i.e., andropathy and gynopathy). The detecting method is to slide the probe from the Pelvic to the Uterus point during the examination. The lower line is used to detect andropathy, including spermatic-vein inflammation, varicocele, and hernia (Fig. 4).
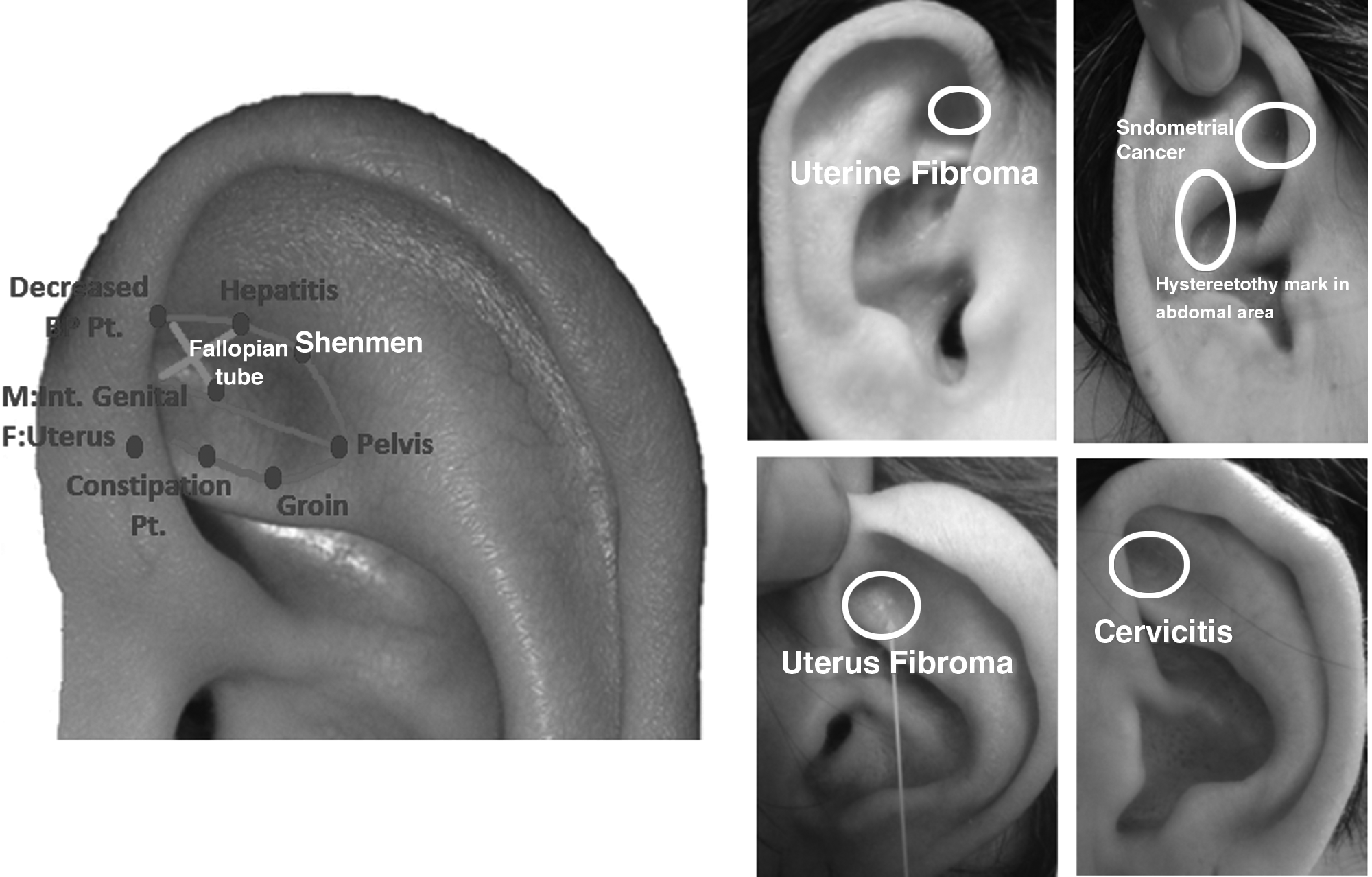
Reproductive system route.
(3) Urinary system. An L-shaped detection route is used to identify possible urinary-system problems. If only weak positive electric resistance in the Kidney point is identified, it is not used for diagnostic analysis. The urinary system points include Kidney, Ureter, Bladder, Prostate (male), or Internal Urethra (female). The Anus point is beside the ear apex. If a nodule is detected, it indicates hemorrhoids (Fig. 5).
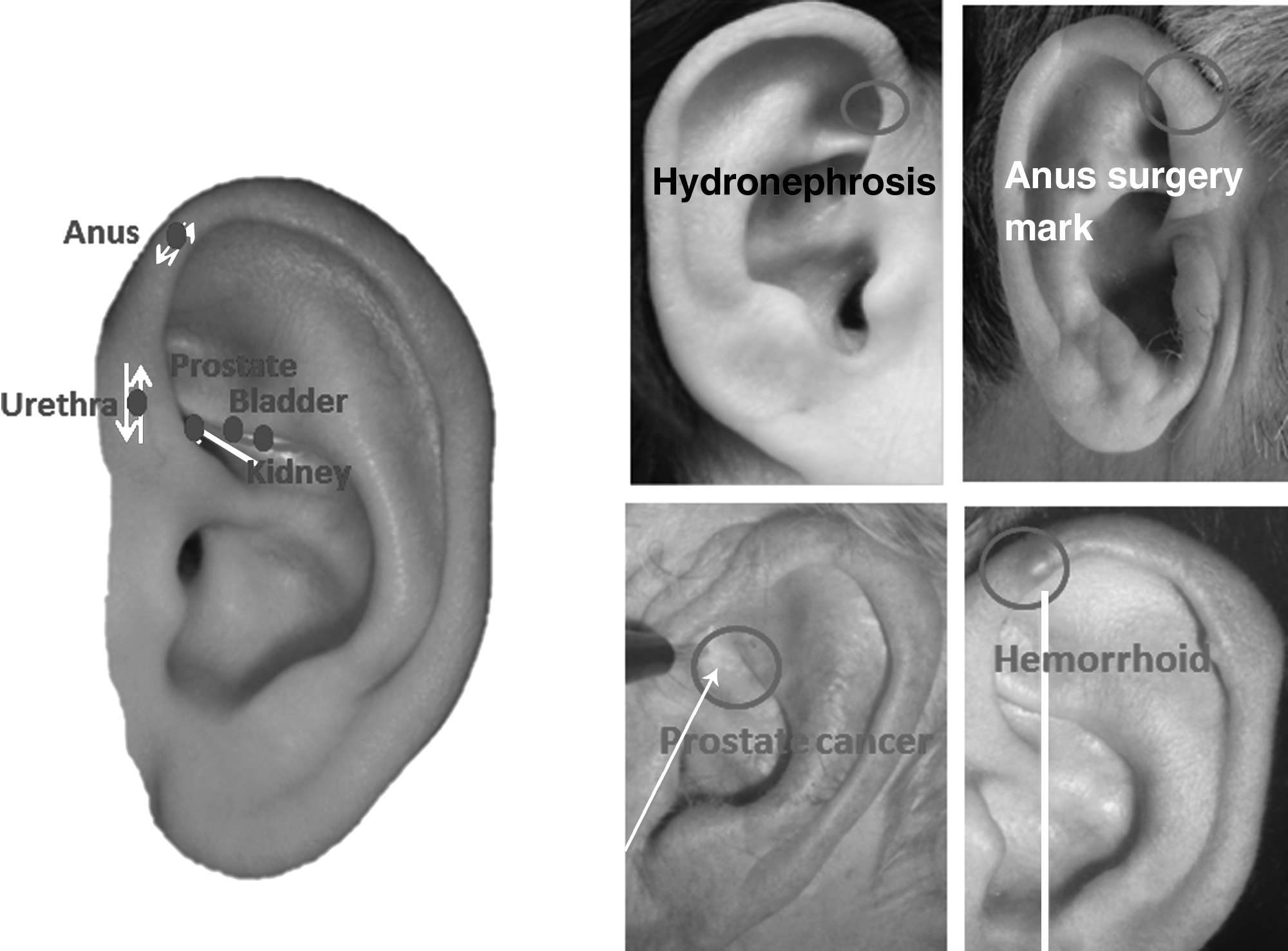
Urinary system.
(4) Liver, gallbladder, pancreas system. A T-shaped route is used to examine the liver and gallbladder system. To reach the Liver, Gallbladder (right ear), and Pancreas (left ear) points, which are embedded in a concave area, the right thumb and index finger are used to hold the auricle, and the middle finger is used to expose the target EAP (Fig. 6). In addition, the Gallbladder area and Duodenum ball points are located on the posterior ear.
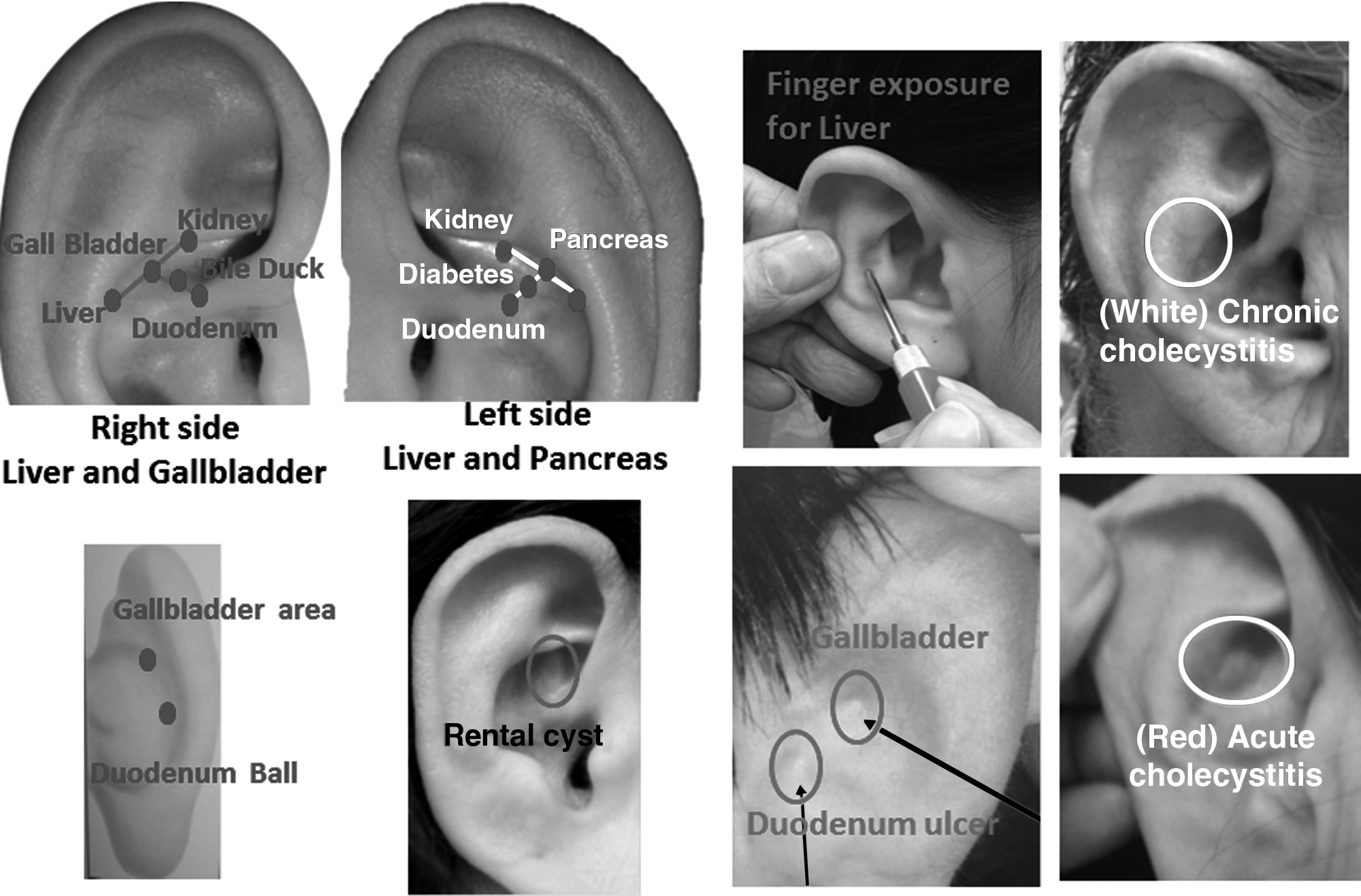
Liver, gallbladder, and pancreas system.
(5) Digestive system. A U-shaped examination route is used, beginning with the Mouth point, followed by Esophagus, Cardia, Stomach, Duodenum, Appendix, Sigmoid, and Large Intestine points (Fig. 7).
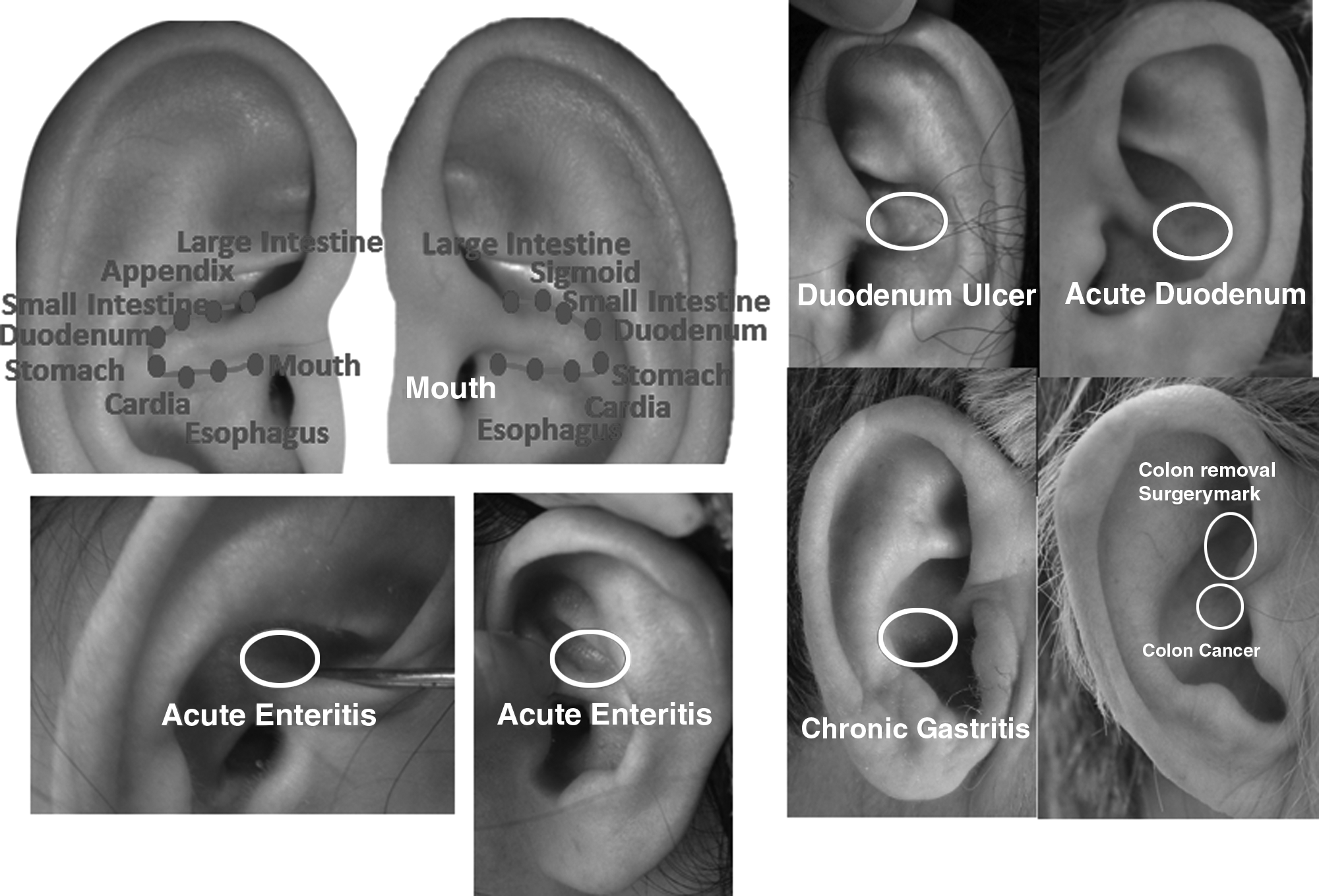
Digestive system.
(6) Abdominal cavity. The abdominal cavity includes Lower Jiao (a Chinese point, including systems of the Small and Large Intestines, the Kidneys, and the Urinary Bladder) and Ascites points (Fig. 8). These points can also be used to judge abdominal distension.
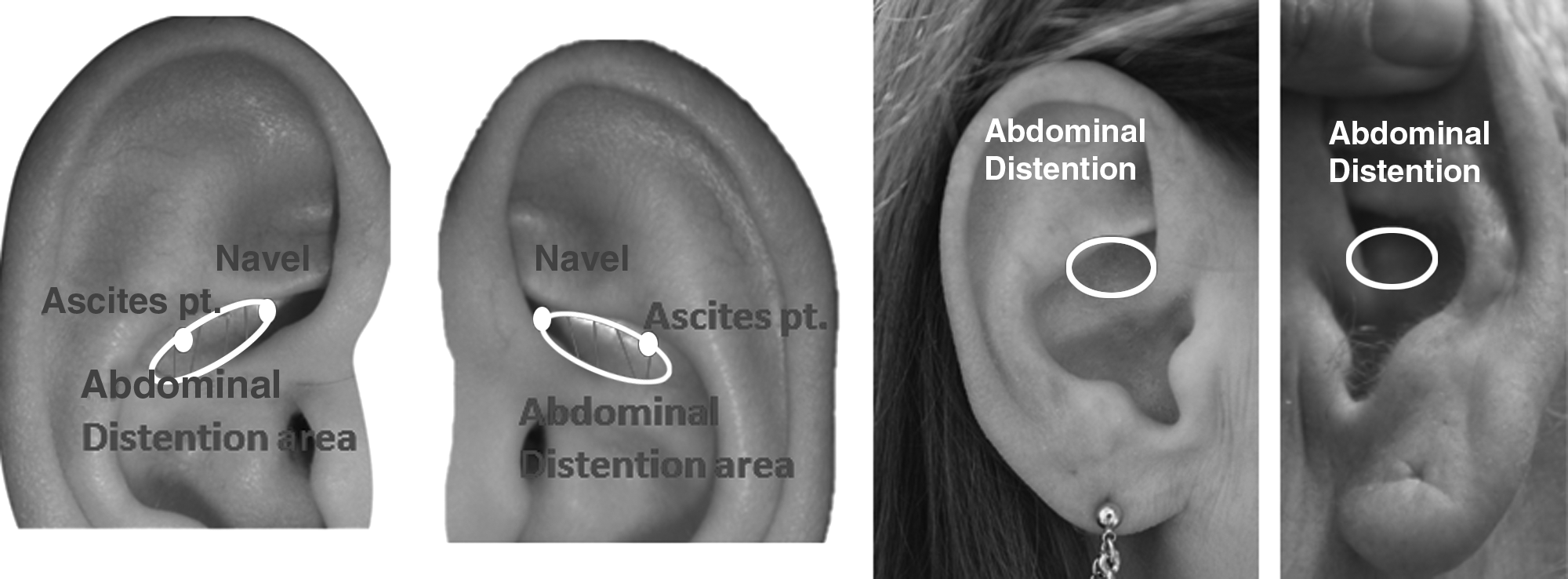
Abdominal cavity.
(7) Cardiovascular system and respiratory system. To check the heart area, the finger-exposure method is needed (Fig. 9). The detecting probe can glide from the Lung to the Heart area. If a depression mark is observed, it refers to edema. In the cavum conchae, the Spleen and Blood points can be used to detect blood-system–related problems.
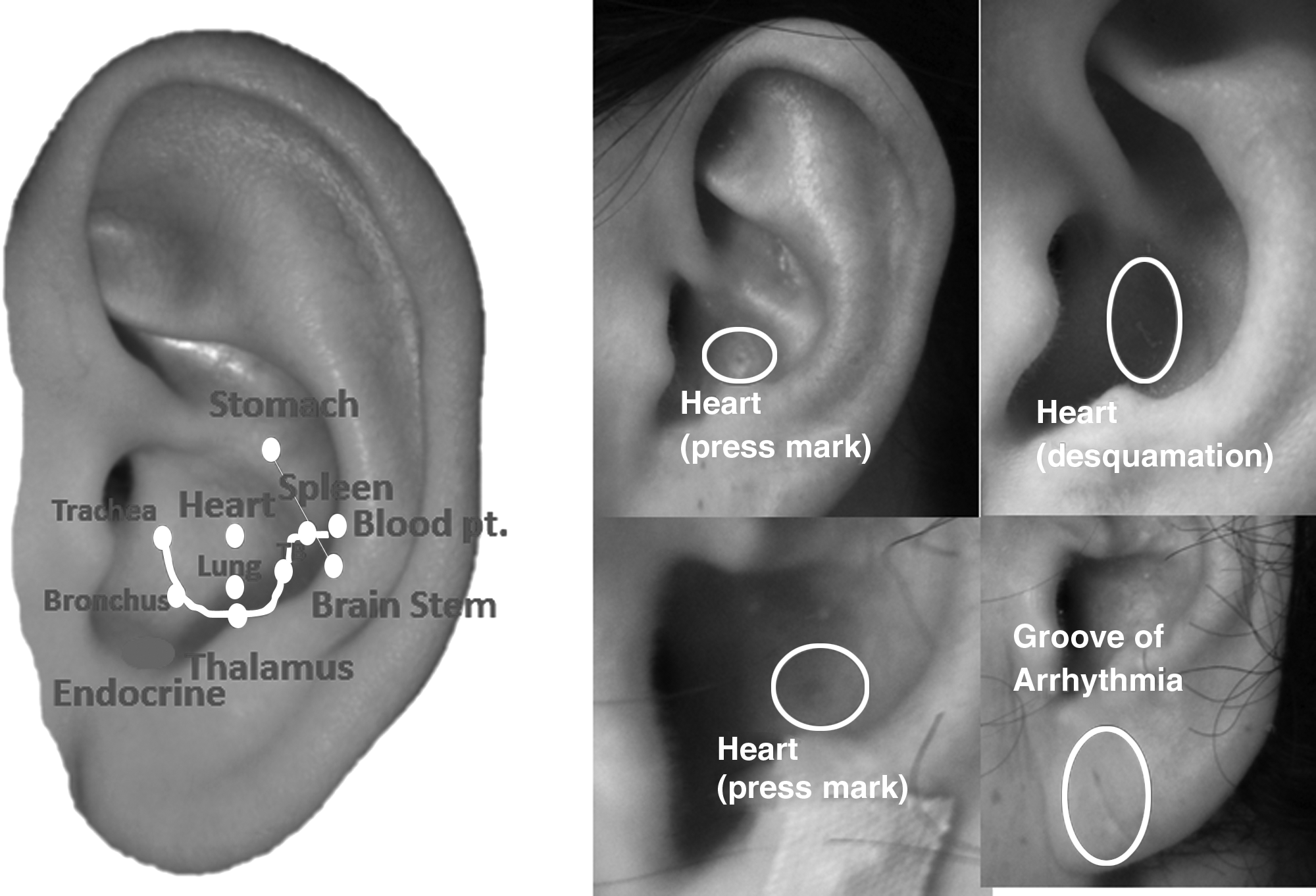
Cardiovascular system.
(8) Respiratory system. Trachea, Bronchus, and Lung are included. The finger-exposure method is needed when checking this system (Fig. 10). Finger exposure is also needed to examine the Bronchus point.
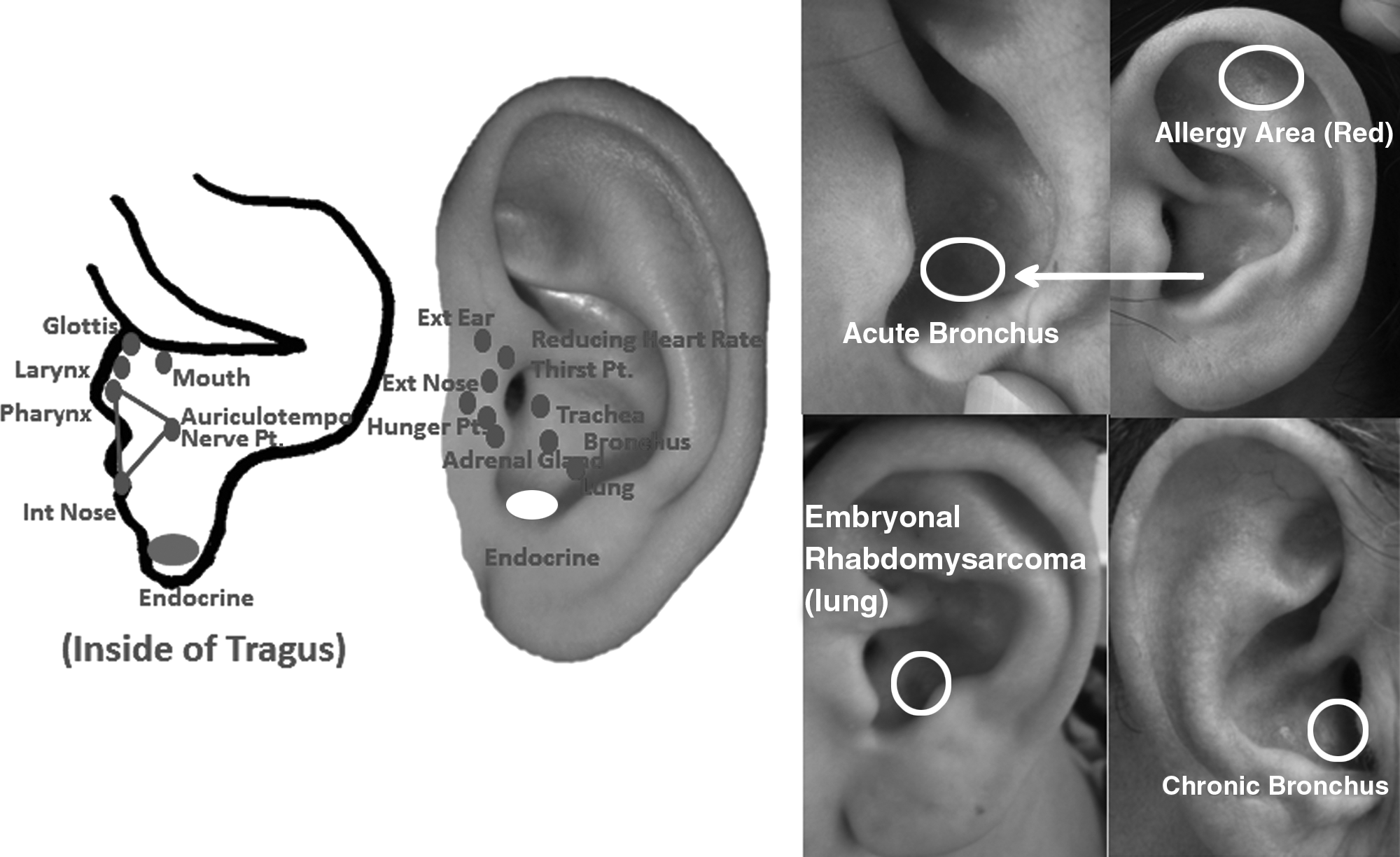
Respiratory system.
(9) Five sense organs. These include internal Nose, Larygopharynx, and Nasopharynx, which are located inside of the apex tragrus (Fig. 11). The Eye and Tongue points are located on the earlobe.
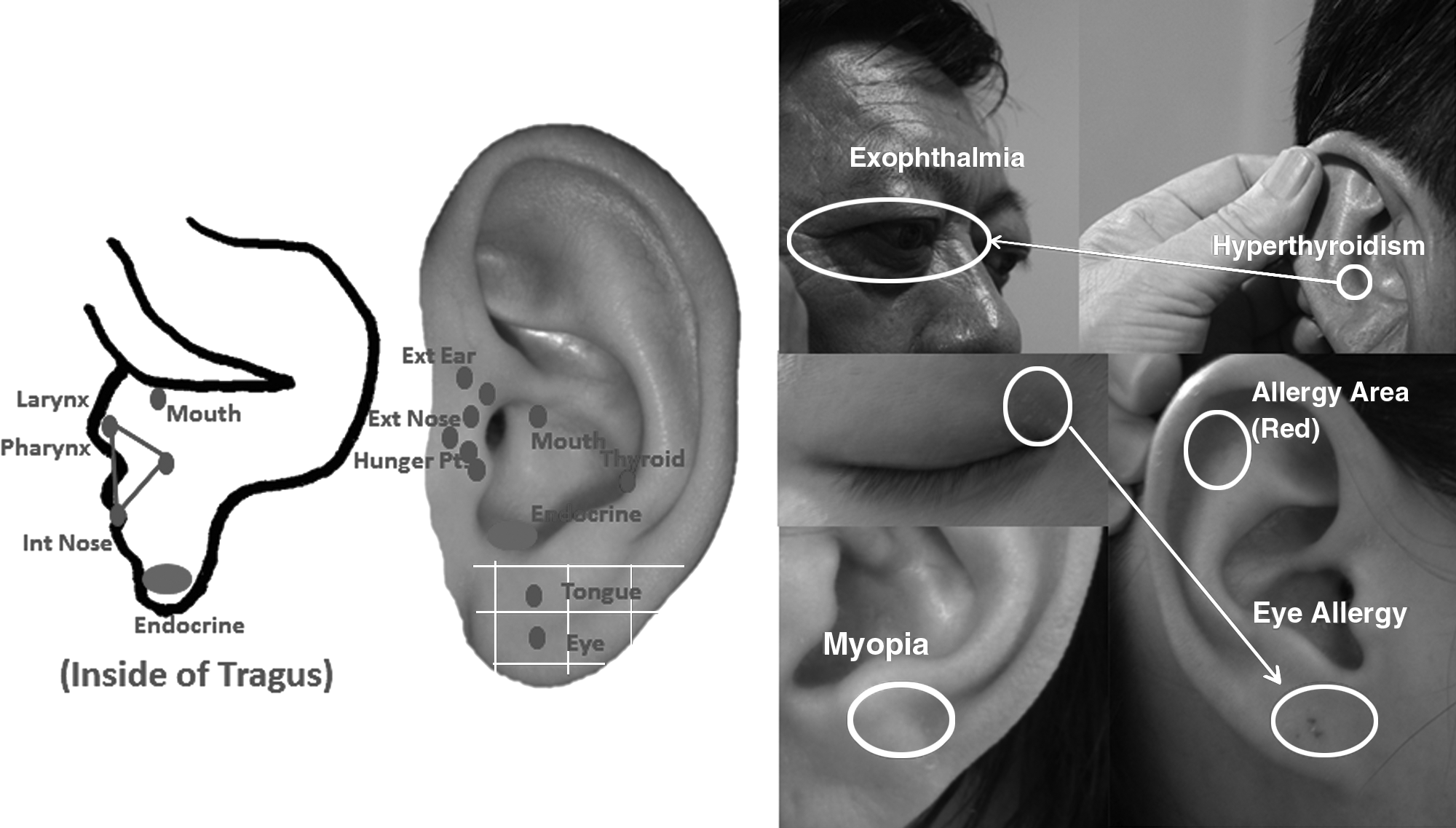
Five sense organ and endocrine system.
(10) Endocrine system. This is located in the internal tragus notch. The distribution of the endocrine “EAP” is not a point, but appears as an area (Fig. 12).
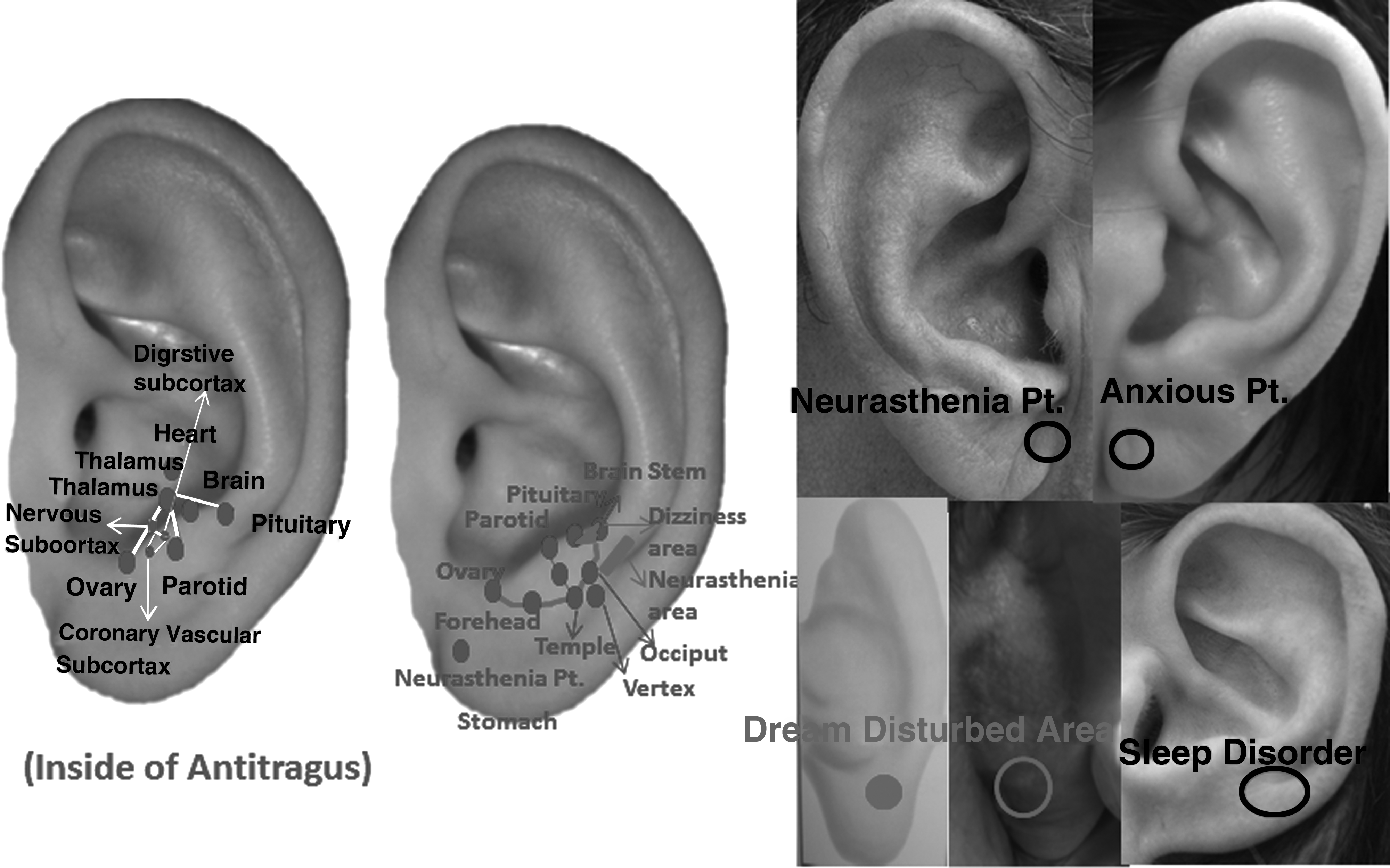
Neurologic system.
(11) Neurologic system. EAPs include the Brain Stem, Digestive Subcortex, Cardiovascular Subcortex, Forehead, Temple, Occipital, and Vertex (Fig. 13). The Neurasthenia point is related to sleep.
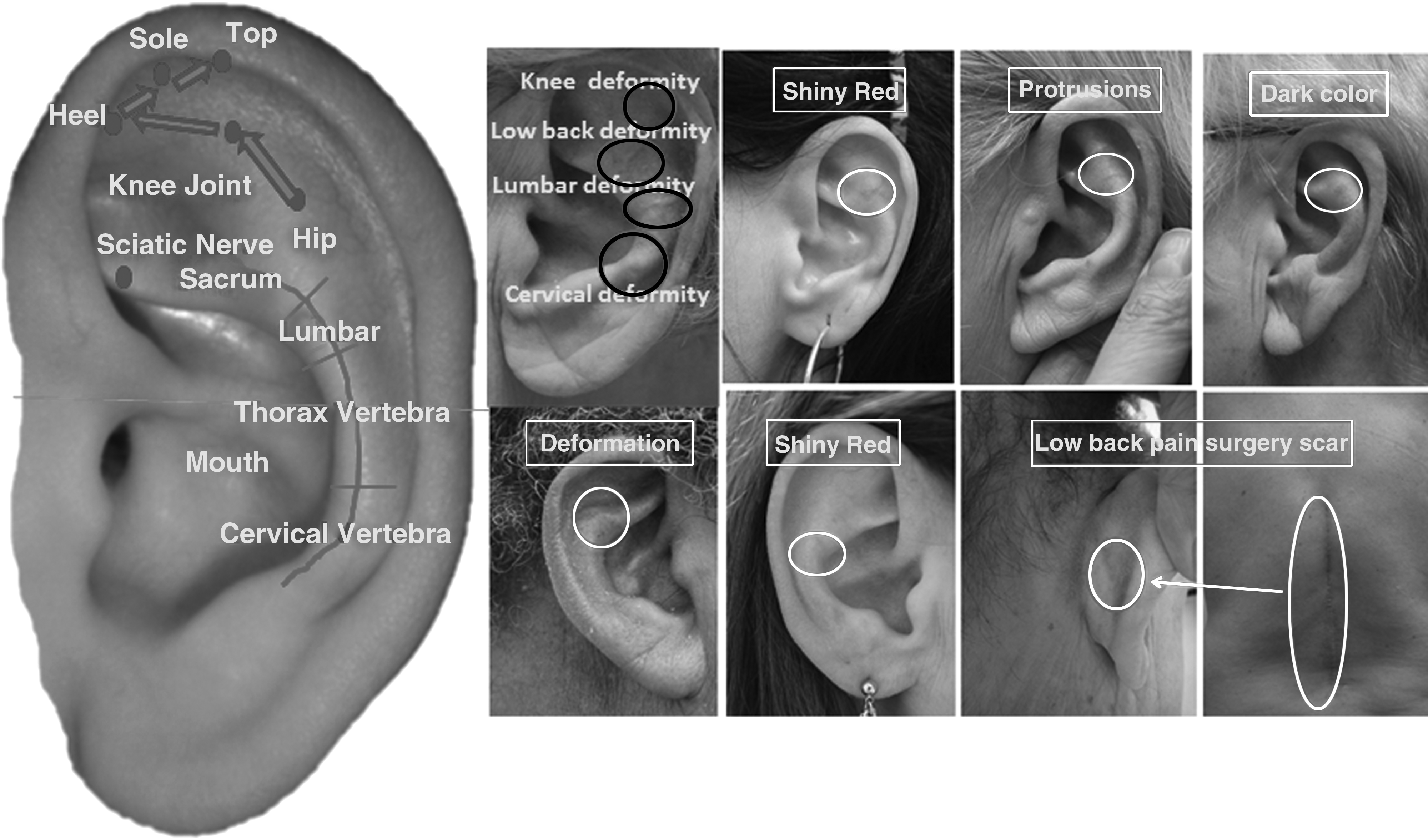
Locomotor system.
(12) Locomotor system. A three-line pattern route is used to check the locomotor system (Fig. 13). In the middle line, the Vertebrae line is divided into 5 equal segments, and the probe is moved from up to down. In the uppermost 1/5 of the middle line, points are checked for Caudal Sacral 5 to Sacral 1. On the external side of the upper 1/5, points are checked for the Sacroiliac Joint and Lumbar Muscle. On the internal side of the upper 1/5, points are checked for Soft Tissue of the Lumbar Muscle. The upper 2/5 of the middle line is used to check Lumbar 5–Lumbar 1. The external side of the upper 2/5, is used to check Lumbar Muscle and External Abdomen points (it is also called Kidney Reflex area). The internal side of the upper 2/5 can be used to check points for the Lumbar Muscle and Lumbar Soft Tissue.
In the 3/5 of the middle line, points are checked for Thoracic Vertebra 12–7 and in the 4/5 of the middle line points are checked for Thoracic Vertebra 6–1. The pattern of detection begins from the antihelix and moves downward; if there is a nodule or cord, bone symptoms are indicated. On the external side of the 3/5 segment, the Thoracic Vertebra 1–2 has a Rib Rim area and a Breast point. To examine the Breast point, the probe is moved up and down to do palpation diagnosis. On the internal side of the 4/5 segment are points for the chest. In the bottom 1/5 of the middle line are points for Cervical Vertebrae 7–1. The internal side has Thyroid and Neck points, and the external side has Shoulder and Back points.
The primary detecting technique of Cervical Vertebrae is based on the discernment cords. Because the point for Cervical Vertebrae 1–2 is embedded inside the Occipital area, two hands are used to expose the Cervical Vertebrae point by tightening the skin; diagnosis is then based on the morphologic changes.
(13) Immunologic system. This system includes Allergic Area and Rheumatism Line (Fig. 14). If the Allergic Area has piecelike and white swelling, or a pointlike red or pressing mark, the person has an allergic constitution.
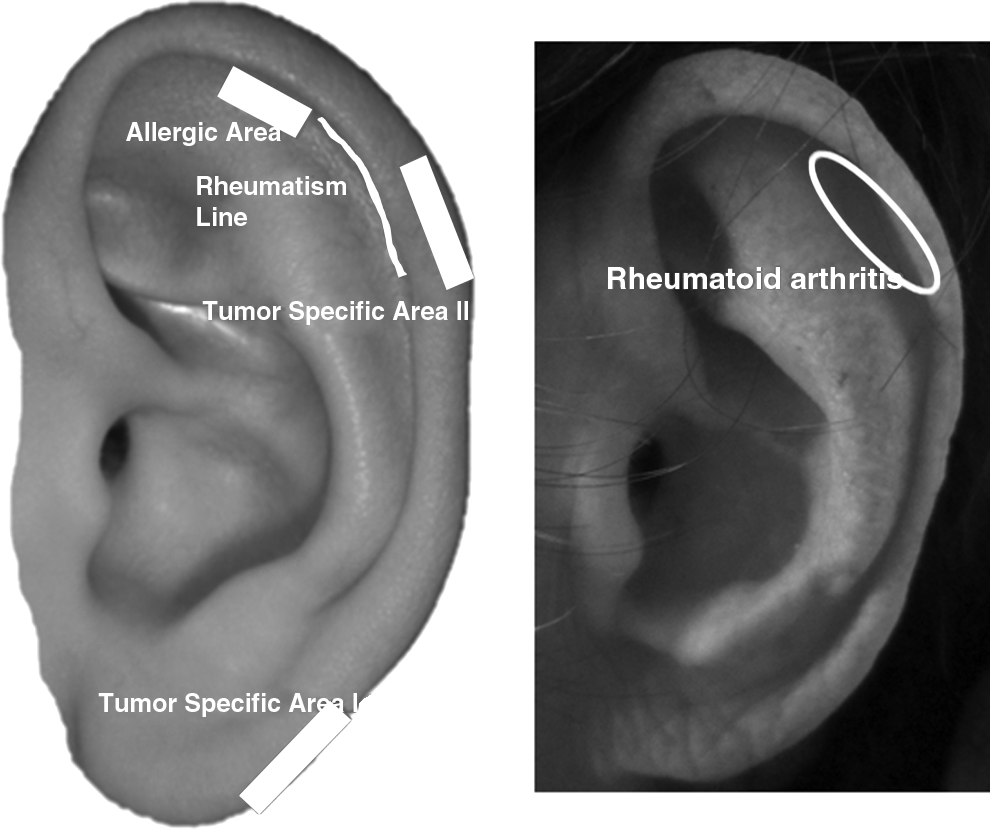
Immunologic system and tumor areas.
(14) Tumor-Specific areas I and II. Tumor-Specific area I is located on the edge of the ear lobe and Tumor-Specific area II is located between Helix 1 and Helix 2 (Fig. 14). The combination of positive reaction of tumor-specific areas (e.g., positive and tenderness at both posterior and anteriors) and corresponding EAPs can be used to identify tumors.
Discussion
This article has presented indepth coverage of comprehensive, and systematic methods of auricular diagnosis that include visual diagnosis, palpation, and electrical diagnosis and differentiation. Diseases/symptoms can be identified and differentiated in clinical practice by following 14 routes that cover 165 EAPs, while applying appropriate manipulation methods. EAPs in the posterior ear are also included. According to this comprehensive diagnosis protocol, diseases can be diagnosed, as well as possible causes of diseases. Based on such information, differentiation diagnosis is possible.
This article has provided valuable information related to auricular diagnosis and disease differentiation. After auricular diagnosis, therapists can administer auricular therapy (for example, auricular acupuncture or acupressure) to manage related symptoms. Auricular therapy is well-suited to the current challenges of primary health care, which emphasizes that care should be available, affordable, and accessible to patients. Health care professionals without formal training in acupuncture and TCM can be taught to incorporate auricular therapy (especially auricular acupressure) into their practices to provide pain relief and augment the effects of other pain-related interventions. Auricular acupressure is similar in effect to acupuncture, but is performed without the use of needles. Auricular therapy has been used to address a variety of health conditions, including anxiety and pain,18–20 tobacco abuse,21–25 substance abuse, 26 insomnia,27,28 nausea and vomiting in early pregnancy 29 or caused by chemotherapy, 30 menopausal hot flashes, 31 dysmenorrhea,32,33 myopia,34,35 pain after lumbar-spine surgery, 36 overweight and obesity,37–40 and low-back pain.41–44
Conclusions
The auricular acupuncture diagnosis protocol presented in this article included systematic approaches to identify specific auricular acupoints related to body symptoms in expected areas, based on maps of the anatomy as displayed on the ear. Empirical studies are needed to validate the procedures and the diagnostic accuracy of detecting diseases/symptoms. Auricular diagnosis is an objective, painless, and noninvasive method, and, if found effective, can be used as a complementary approach by health care professionals in practical applications for health-problem screening. Application of auricular therapy in clinical practice could significantly affect the cost-effective provision of services and contribute to a shift from conventional disease-based biomedical models to a broader integrative medicine paradigm in primary care.
Footnotes
Acknowledgments
This study was supported by grants given to Dr. Yeh from the Center for Research and Evaluation Pilot/Feasibility Study Program, School of Nursing, and Aging Institute, University of Pittsburgh.
Disclosure Statement
Dr. Yeh has no competing financial interests. Dr. Huang is the cofounder of AMIRTC and has a financial in AMIRTC.