
Abstract
Abstract
Background:
Success of any medical treatment depends on understanding the true origin of symptom development—this is also naturally true of acupuncture. All therapeutic actions must consist of not only relieving patients' pain but also reinstating the correct working order of the body's defense mechanisms and of the organ whose weakness caused the ailment to develop. Early diagnosis of an internal weakness, which could potentially lead to development of a pathological syndrome—even before any symptom is detected—could be the basis of effective prevention. The aim of Auricular Causative Diagnosis (ACD) is to discover the inner causes of pathologic conditions. ACD is based on visualization and analysis of the pathologic marks in Auricular Points (APs). ACD allows physicians to identify existing illnesses precisely and determine which inner organ is fragile and therefore responsible for the development of a symptom. ACD can even be used to anticipate and reveal developing pathologic processes before their clinical manifestation and therefore can be used to prevent illnesses.
Objective:
The aim of this research is to show correlations between organ pathologies and their corresponding APs in practice, and to improve understanding of the successes and failures in results when using ACD.
Materials and Methods:
This long-term study (ongoing since 1985) has included >10,000 cases, with patients of different ages and different pathologies. First, measurements were performed with an Electric Skin Resistance Test (ESRT) in main APs of healthy individuals at different ages. Then, measurements of the same APs with the ESRT were performed in patients with well-known pathologies, who were undergoing surgery in different hospital departments: cardio-surgery; gynecology; digestive surgery; orthopedic surgery; and respiratory surgery. ESRT measurements were compared in both groups.
Results:
Stimulation of a Causative Auricular Point tremendously increased therapeutic success, led to immediate relief of pathologic symptoms, helped recover organ functions, and helped prevent illnesses.
Conclusions:
Given that different causes can be at the origin of identical symptoms, discovery of true inner problems through ACD, helps physicians treat the roots of pathologies, not only the symptoms, and improves the efficiency of the treatments. To support these clinical case studies, provided by more than 30 years of practice, the current authors believe that evaluations using a double-blind procedure and also animal trials should be performed.
Introduction
T
Unfortunately, learning traditional acupuncture diagnosis techniques, especially pulse diagnosis, is based on the subjective feelings of the therapist, which can only be developed after long experience and requires many years of studying under the guide of a master, which can be difficult in the modern world.
However, Auricular Causative Diagnosis (ACD) is based on objective physical and visible features of auricular points (APs) and allows rapid and reproducible results, which, like X-ray images, can be shared and discussed among different experts. While all medical imagery tests (magnetic resonance imaging [MRI], X-ray, scanning, etc.) can only be used to detect already anatomically modified structures (tumors, calculi, cysts, etc.), which only become detectable after a long time of dysfunction, ACD reveals functional disturbances from the very beginning of their development, reflecting information from the cortical centers about functional changes in the state of each organ. This advantage of ACD helps practitioners be aware of pathologic processes on the functional level, provides an early functional diagnosis, and leads to early treatment of disease and its prevention. 1
APs are traditionally used in acupuncture for both diagnosis and treatment. The specificity of the action of one AP with its corresponding organ is well-known.2–4
Many researches have demonstrated the relationships among the APs, their corresponding organs, and functional areas of the brain cortex.2–4
In the current authors' previous experiments, it was possible to show that stimulation of an AP activates a cortical somesthetic area as well as direct peripheral-nerve stimulation does, as was seen by somatosensory evoked potential (SEP) traces in both, while a nonactive “placebo” point of the ear did not result in this action. Moreover, both of these traces were altered in the same manner in patients with the same pathologic problem of the same corresponding organ. 4 These results indicated a convergence of nervous impulses coming from the organ itself and from the AP corresponding to this organ in the same cortical area. These results also revealed neurologic support for the functional somatotopics of APs, discovered by Paul F.M. Nogier, MD, 2 and described in the microsystem theory of Jean Bossy, MD, et al.3–5
Among the three main tests used for AP detection—Inspection, Pain Pressure Test (PPT), and Electric Skin Resistance Test (ESRT)—the Inspection test has shown the best success rates for identifying patients' symptoms.6,7 However there is, sometimes, a discordance between a classical medical diagnosis and an auricular diagnosis.7,8
It is important to prove this correlation between organ pathology and corresponding APs in practice, and to gain understanding of the successes and failures of ACD results. These are the aims of the current authors' ongoing research.
Materials and Methods
This study has been underway since 1985 until now and has included more than 10,000 cases, involving patients of different ages and with different pathologies.
For a preliminary trial, measurements of ESRT were performed in main APs of healthy individuals at different ages.
After that, measurements with ESRT were performed in the same APs, in patients with well-known pathologies, undergoing surgery in different hospital departments: cardio-surgery, gynecology, digestive surgery, orthopedic surgery, respiratory surgery.
Comparing the results of ESRT in both groups, a statistically significant fall of the ESRT was found in the specific APs associated with diseased organs. Every time, the lower ESRT was found in a specific AP corresponding to a specific organ with the pathologic condition, there was always Visual Ear Skin Mark (VESM). Therefore, it was possible to confirm a perfect coincidence of low electric resistance and VESMs in the APs corresponding to the diseased organs.
Beginning from this, photographs were taken regularly of the ears of all study patients to find the VESMs needed to make diagnoses.
With the development of iPhones, it became possible to take high-quality photos with potential to amplify these images instantly. 1
Results
AP Detection
Only points related to pathology are detectable on the ear.
There is no VESM in a healthy person. Healthy babies have no marks on their APs. The appearance of visible skin marks in an AP results from focal hypersensitization of the central nervous system caused by a pathologic process in its corresponding organ.
From the very beginning of its development, any pathologic process in any part of the body causes modifications of the sensitivity of the neurons in its associated cortical somesthesic area, which leads to the formation of an AP on the specific area of the external ear.3–5
Thus, a specific AP with particular features appears in the correlated area of the external ear, corresponding to the organ with the pathologic condition. This AP has less electrical skin resistance and high thermosensitivity, becomes very painful under the pressure, and a VESM appears on the AP's site.
The more intense the pathologic process is in a patient, the larger the representation will be on that patient's ear. This is why the point location in different auricular maps is so diverse. Indeed, for instance, in the case of acute gynecologic pathology, its corresponding AP will become larger and will extend on to the places of neighboring points, which is why one therapist will place it inside the triangular fossa, while another therapist will find the hypersensitive point on the superior crus of the antihelix (the area, which in other maps, is associated with the lower extremity). This might explain the observations of Marco Romoli, MD, and colleagues, who have shown a different distribution of APs with low ESRT results in patients after hysteroscopy. 6
The explanation seems to be clear: The more intense the gynecologic condition is in a patient, the larger its representation will be in that patient's ear, and, sometimes the representation will even extend to neighboring sectors.
Meanings of Different VESMs
Examples of different VESMs include:
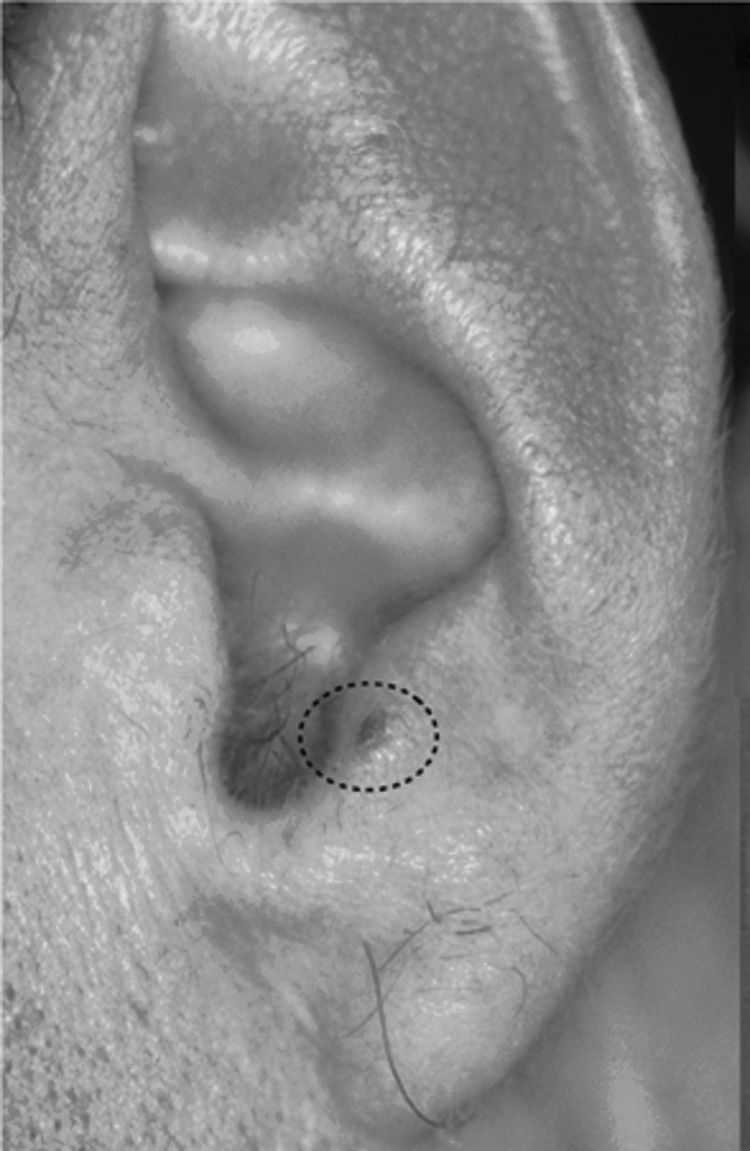
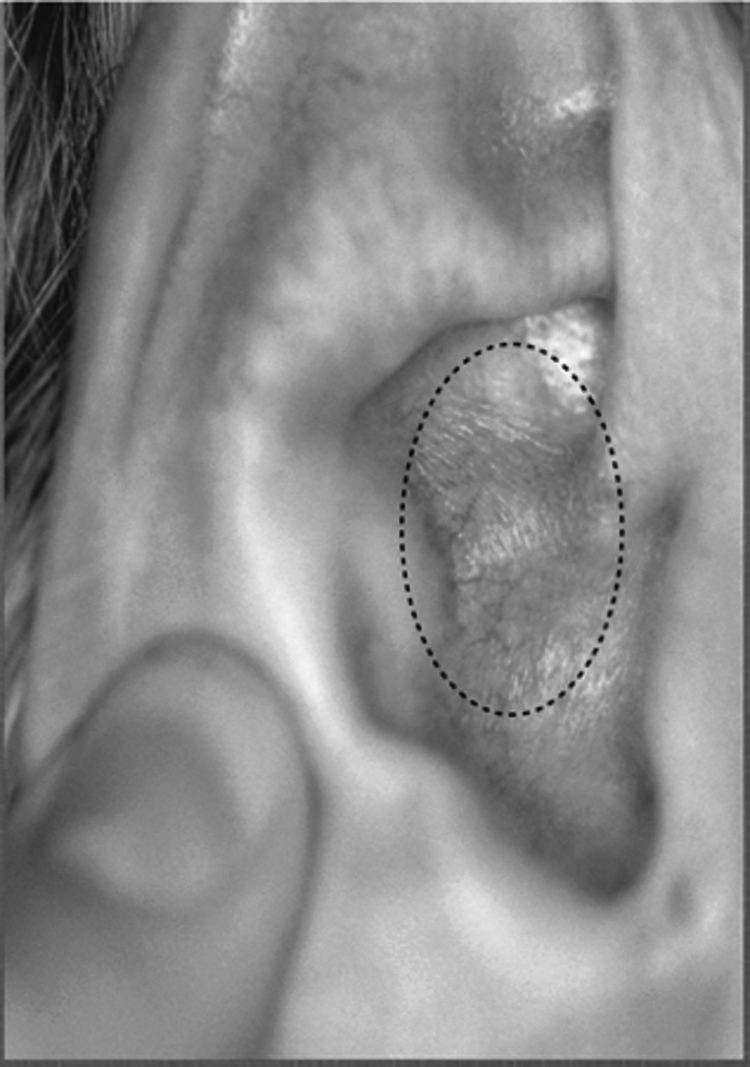
• A red spot means acute inflammation (Fig. 1). • A brown spot means an old or chronic process (Fig. 2). • Hyperemia means intense acute inflammation (Fig. 3). • Hyperemia specifically located in the earlobe means high blood pressure (Fig. 4). • Visible vessels mean Blood Stagnation (Fig. 5). • A pustule means a nodule or tumor (Fig. 6). • Ulceration means ulcer (Fig. 7).
Visual Ear Skin Mark as a red spot (in the Auricular Point corresponding to the forehead in this case) means acute inflammation.

Visual Ear Skin Mark as a brown spot (in the Auricular Point corresponding to the temple area in this case) means chronic or ancient inflammation.
Visual Ear Skin Mark as an area of the hyperemia (in the Auricular Point corresponding to the Stomach in this case) means acute inflammation.
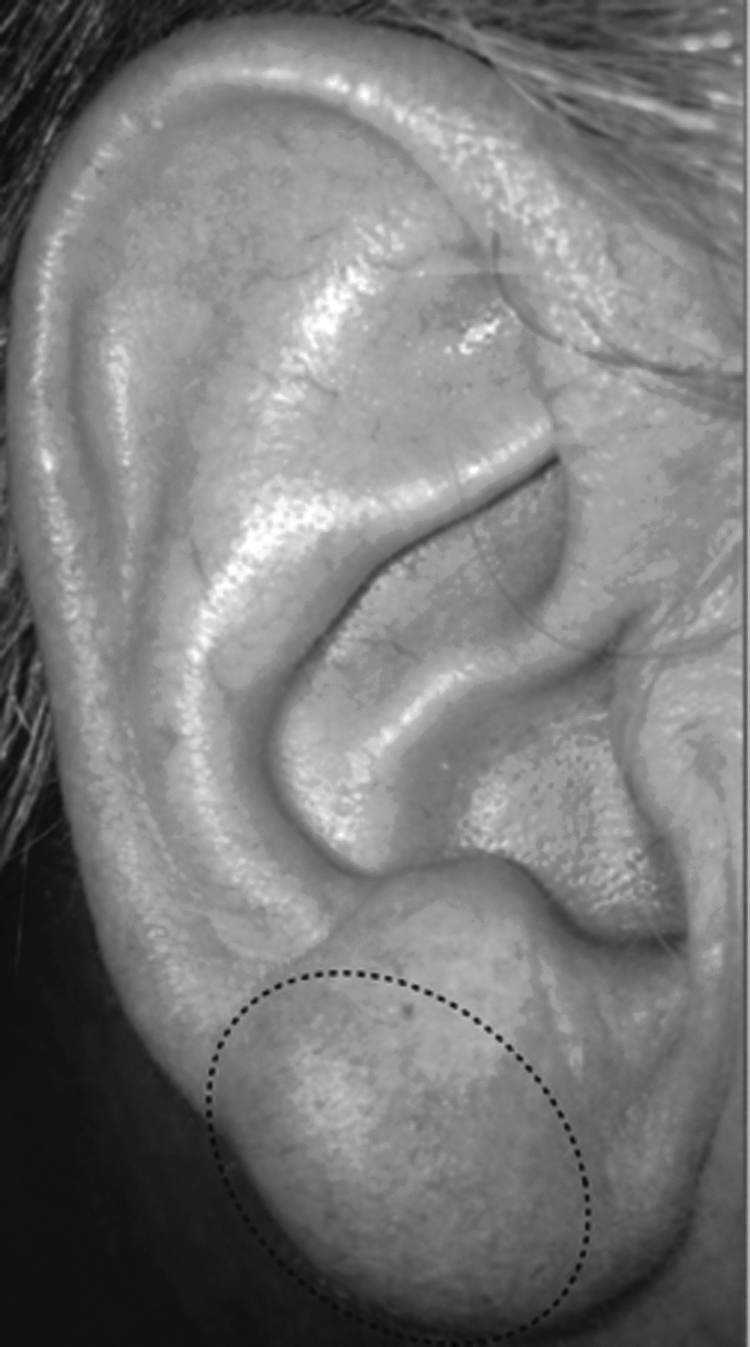
Visual Ear Skin Mark as an area of the hyperemia specifically in the ear lobe, means high blood pressure.
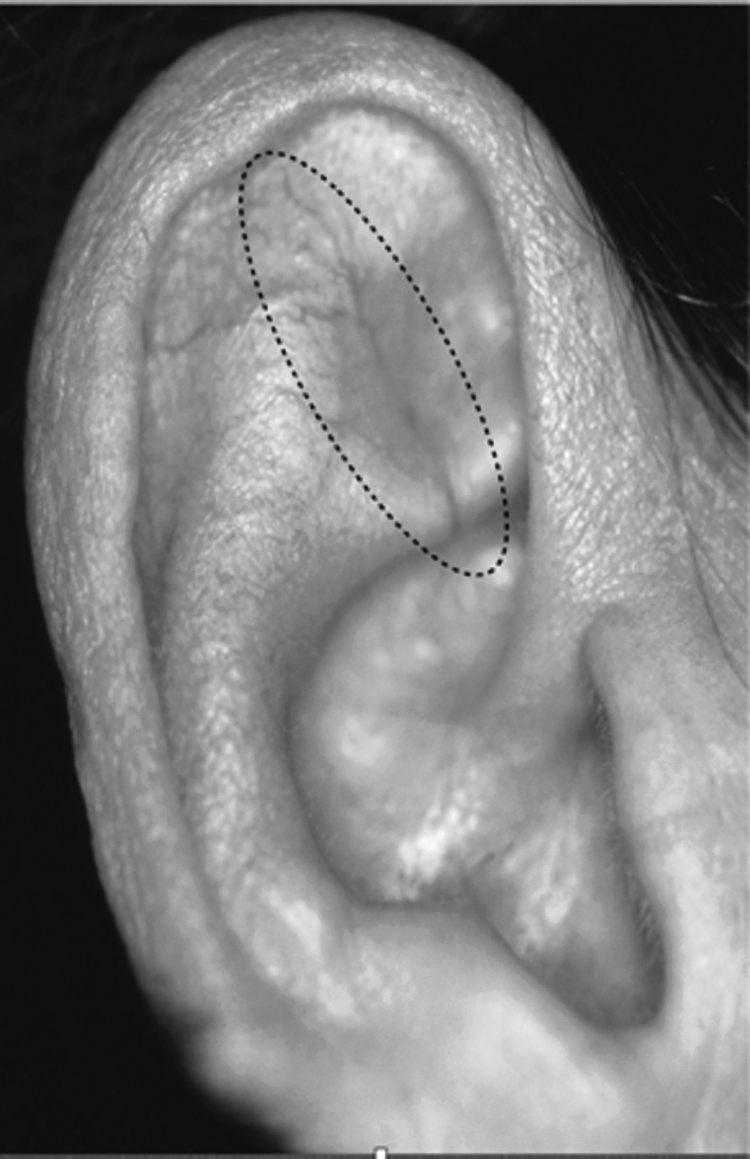
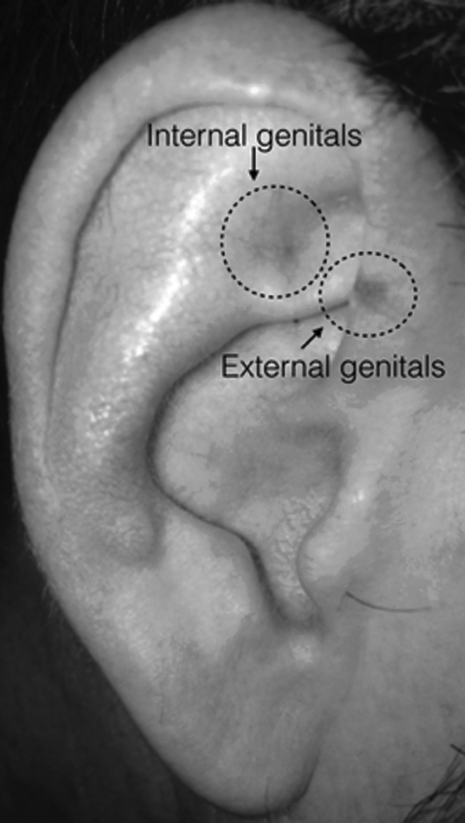
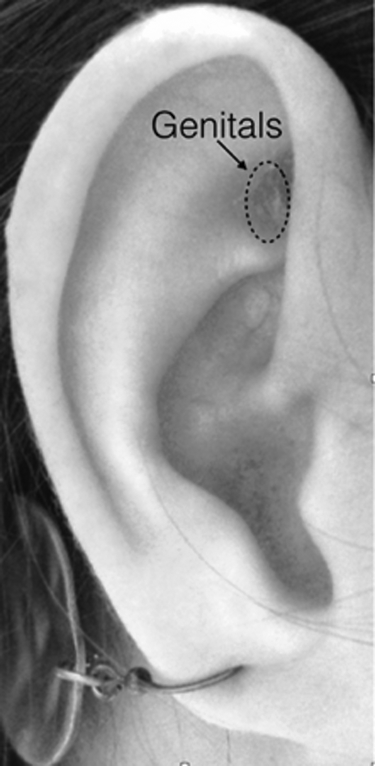
Visual Ear Skin Mark as a visible vessel (in the area corresponding to the Inner Genitals in this case) means Blood Stagnation.
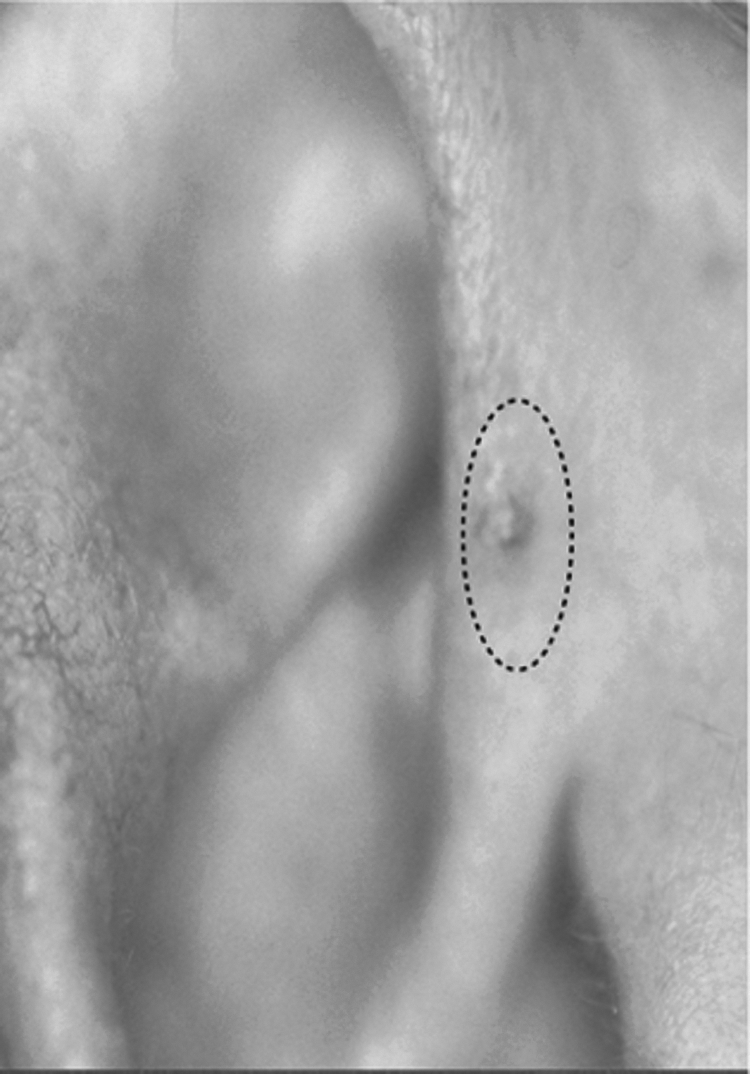
Visual Ear Skin Mark as a pustule (in the area corresponding to the Prostate in this case) means nodule or tumor.

Visual Ear Skin Mark as an ulceration (in the area corresponding to the Duodenum in this case) means ulcer.
The same clinical manifestation, for instance, a gastric pain, resulting from different pathologic processes in different patients, will have different kinds of VESMs, located in the same area of the ear corresponding to the Stomach: A VESM in the ear of a patient suffering from acute gastritis is a hyperemia; a VESM in the ear of the patient with chronic gastritis is a brown spot; a VESM in the ear of the patient with a duodenal ulcer is an ulcer (Fig. 8).
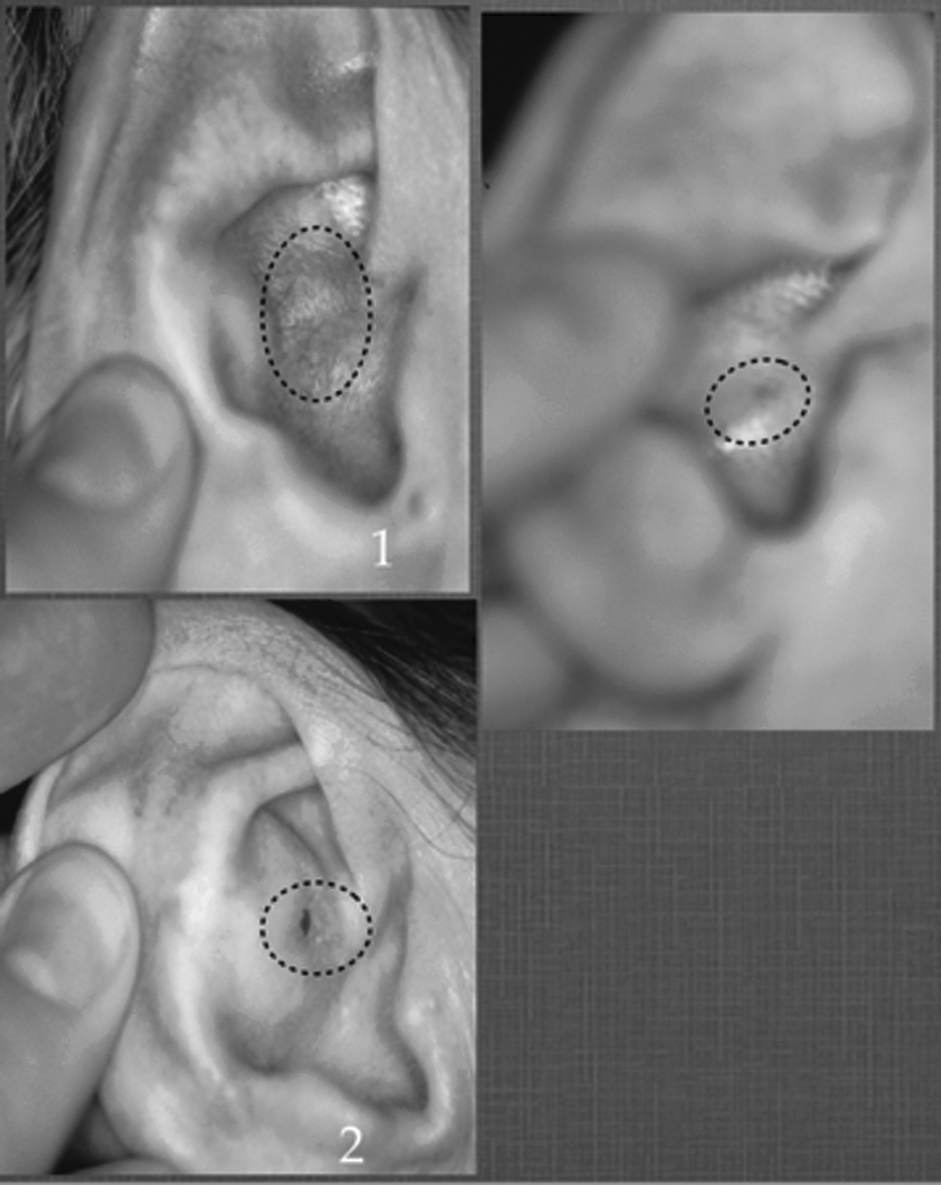
Three patients with gastric pain resulting from different pathologic processes presented different kinds of Visual Ear Skin Marks located in the same area of the ear corresponding to the Stomach:
It might happen very rarely that no anatomical changes are found in the ear and nothing is visually apparent. This is what is termed a “silent ear,” and it means that the vascularization of the external ear is blocked because of a neurovegetative imbalance. In this case, simple pressure or needling of the AP Diaphragm (Point Zero) will reveal visual marks. Given that the brain has to be aware of any pathologic process in any part of the body, this information will inevitably be reflected in the relative AP. Therefore, the active AP will appear with its specific characteristics: hypersensitive under pressure, low electrical resistance, and an apparent VESM. If, however, nothing visual is apparent, the current authors recommend looking for active points based on the patient's medical history or local pain under pressure, or by electrical detection.
When a VESM is in the shape of visible vessels, which means Blood Stagnation (Fig. 5), it is sometimes necessary to determine where this mark begins and ends—where the organ-source of the pathology is situated. One should press this vessel in the middle in order to see, what AP would become full (dark) while the other side of the vessel would become empty (clear). This “full” AP would thus indicate the organ related to the source of the pathology.
Discussion
The main question is: “If the appearance of the AP reflects the information in the corresponding brain center concerning the dysfunction of the correlated organ—and as the brain center is always informed about the state of all parts of the body at any moment—why is there, sometimes, a discordance between the classical medical diagnosis and the auricular diagnosis?”
Even in previous studies, Romoli and Mazzoni, and Terry D. Oleson, MD, et al., did not find 100% correlation between ear diagnoses and classic medical diagnoses.7,8
Understanding the nature of referred pain offered an answer. Referred pain is pain perceived at a location other than the site of the pain stimulus. An example is myocardial infarction, where pain is often felt in the neck, shoulders, and back rather than in the chest, which is the actual site of the injury. Physicians and scientists have known about referred pain since the late 1880s.9,10
Referred pain is a well-known phenomenon that may occur in any pain condition.11–13 It is defined by the International Association for the Study of Pain as “pain perceived at a location that is not the origin of the pain.”14,15
Referred pain can originate in tendons, ligaments, and visceral and skeletal structures, as well as in myofascial structures. 16
According to the segmental organization of the body, inner organs have a common segmental innervation with bones, joints, muscles, and skin located in the area supplied by the same spinal nerve. The concept of convergent projection proposes that afferent nerve fibers from tissues converge onto the same spinal neuron, and explains why referred pain is believed to be segmented in much the same way as the spinal cord. Peripheral and central sensitization of the nervous system can contribute to an expansion of the receptor fields of dorsal-horn neurons. When local pain is intensified, the referred pain is also intensified.
When there is a pathologic condition in one internal organ, this sends an alarm signal to its associated nervous segment. Although the “referred pain” appears in one area of the skin or muscle or joint, it may actually come from a different source. This pain reflects a pathologic process in an internal organ that has the same innervation.
For instance, the shoulders have the same segmental innervation as the pleura. When a pathologic process occurs in the lungs and involves the pleura (for example, an inflammation or a tumor process), it can be felt as a shoulder pain, but this is only a signal.
The most famous example is myocardial infarction, which is often only detected by a pain in the left arm, because the arm and heart have the same innervation.
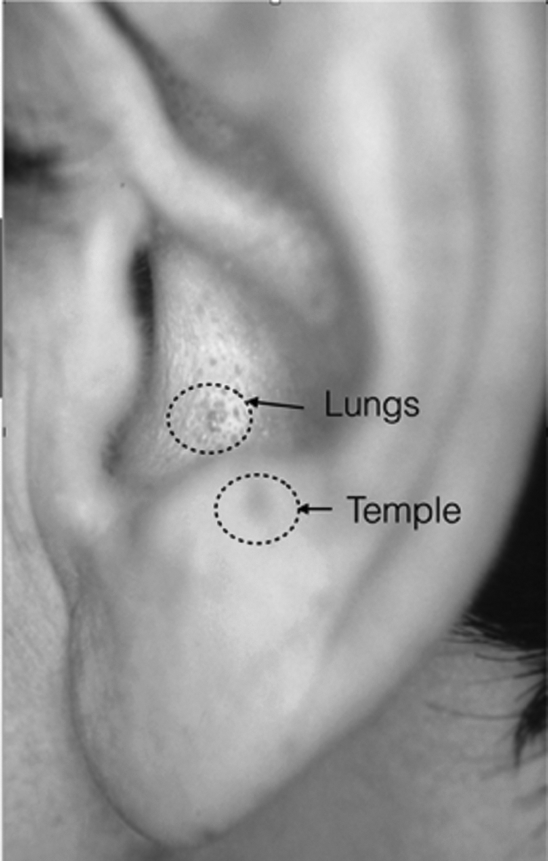
Yet, in these cases, auricular diagnosis will reveal the real source of the pain. In the first example, ACD will show a VESM in the AP Lungs and not in the AP Shoulder, associated with the place where the patient feels the pain. In the second example, a VESM will appear in the AP Heart, even when the pain is perceived in the arm.
Another example is pain in the lower back, and/or pain in the knee, which might manifest a pathologic condition in the genital organs or in the intestines, because they have the same innervation. However, the ear map in this case will show a VESM especially in the AP Genitals or AP Large Intestine, indicating the inner pathologic condition in the causative organ.
Knowledge of these patterns can assist in understanding the source of the discordances between the results of auricular diagnosis and classical symptomatic medical diagnosis. Thus, in articles targeting the validation of auricular diagnosis, there was not a 100% concordance between the results of auricular diagnosis and classical symptomatic medical diagnosis, because the researchers could not take into account the cases with referred pain. In fact, the classic orthopedic diagnosis indicated the site of the symptom of the painful manifestation, while auricular diagnosis showed the internal organ whose hidden pathology caused this referred pain.
This consideration enables a tremendous increase of the therapeutic effect, by concentrating all treatments on the causative organ, which is the origin of the pain, and not on the site where the pain is felt.
The Causative Auricular Point (CAP) is the point that corresponds to the original pathology. Stimulation of the CAP inhibits the pathologic hypersensitivity focus in the corresponding nervous center and thus leads to immediate inhibition of the pain in the corresponding organ and the disappearance of the referred pain (i.e., the symptom).
Therefore, ACD defines the whole therapeutic approach, not only the choice of auricular points, but also the acupuncture protocol and all the other kinds of therapeutic methods - all of them should target the original pathology rather than referred symptom.
Auricular Causative Treatment
Because the same spinal segment controls several anatomical layers—skin area muscle, joint or vertebrae, and internal organ—stimulation of one AP will influence all the elements corresponding to the same spinal segment: skin; muscle; bone or joint; and inner organ.
For example, stimulation of the AP Cervical Vertebrae will influence the area of skin; the muscles and bones located on the neck and on the trajectory of the peripheral nerve (upper member), larynx, esophagus, pylorus, bronchus, and lungs, because they have the same segmental innervation. Thus, the same AP Cervical can be used for treatment of neck pathologies, such as a stiff neck, all kinds of neck injuries, and cervical vertebrae conditions (spondylarthritis, hernia, etc.); for all pathologies of the shoulders, elbows, wrists, thumbs, and, elsewhere; and for esophagitis, pylorus reflux, sore throat, laryngitis, bronchitis, pneumonia, etc. Likewise, vice versa, stimulation of AP Shoulder, Elbow, Wrist, can be used to treat neck pain and pathologies of the esophagus, larynx, trachea, bronchus, or lungs. Or, one can use the AP Throat, Lung, Trachea, or Bronchus to treat conditions in the respiratory system as well as neck, shoulder, elbow, wrist, or thumb pathologies.
In the same way, stimulation of the AP Lumbar Vertebrae and Sacrum influences the areas of skin, muscles, and bones located on the lower back and on the trajectory of the peripheral nerve (legs). This AP also influences the function of the kidneys, bladder, large intestine, and genitals, because they have the same segmental innervation.
Thus, the APs Lumbar Vertebrae or Sacrum can be used to treat low-back pain, shingles, muscle contractions, lumbar disc herniation, spondyloarthritis, etc.; hip, knee, ankle, and foot pathologies; and kidney conditions, urinary infections, diarrhea, constipation, Crohn's disease, prostatitis, uterus cramps, ovarian cysts, etc.
In addition, stimulation of AP Hip, Knee, Ankle, Heel, can be used to treat lumbar pain and pathologies of the urinary tract, colon, and genitals, because they have the same segmental innervation. One can also use the APs Large Intestine, Prostate, or Uterus, to treat the conditions in these systems as well as lower-back, hips, knees, ankles, or heels, because they have the same segmental innervation.
These phenomena allow practitioners to multiply the efficiency of auricular therapy dramatically, using several APs corresponding to different structures with the same segmental innervations as the target causative organ. One AP will support and multiply the action of the CAP, because its stimulation will influence the same nervous segment. The main condition for using these APs is that the points should be “active” (i.e., painful under pressure as shown with the PPT).
Thus, auricular causative treatment (ACT) allows a choice of APs as follows: (1) One can use the CAP, and then, other APs corresponding to the parts of the body with the same segmental innervation as the causative organ, when these points are active (they will have a positive PPT). (2) ACT might be combined with body acupuncture and all other kinds of treatments, whose actions are aimed at the causative organs revealed by the ACD.
Clinical Cases
Several clinical cases illustrate how ACD was used within this study.
Clinical case 1 (Fig. 9)
A 17-year-old girl complained of intense headaches and neck pain lasting several months and resistant to anti-inflammatory treatment. ACD revealed a very strong VESM in the form of a pustule in the AP corresponding to the lungs. Stimulation of the AP Lungs stopped this patient's neck pain and headache immediately and completely. Targeted pulmonary investigations revealed that she had tuberculosis.
Clinical case 1: A 17-year-old girl had intense headaches and neck pain for several months that was resistant to anti-inflammatory treatment. She had a very intense Visual Ear Skin Mark—a pustule in the Auricular Point (APs) corresponding to the lungs. Stimulation of the AP Lungs relieved the neck pain and headache immediately and completely. Pulmonary investigations revealed tuberculosis.
Clinical case 2 (Fig. 10)
A 53-year-old female, without any prior medical history, complained of very intense right-shoulder pain that was exacerbated at night. Anti-inflammatory treatment was unsuccessful. MRI of the shoulder showed a small inflammatory process that did not explain the intensity of the patient's pain. ACD did not reveal a Visual Ear Skin Point (VESP) in the AP corresponding to the shoulder. However, ACD revealed a very strong VESP in the ear point corresponding to the lung. Acupuncture of the AP Lung stopped the patient's shoulder pain immediately. Thus, ACD indicated that the pain in her shoulder was a referred pain, caused by underlying lung pathology, as the lung and shoulder have the same segmental innervation. Thoracic scanning was performed and revealed a small cancer tumor developing in the upper lobe of the right lung. This early diagnosis enabled a successful oncologic treatment and complete remission of the cancer.

Clinical case 2. A 53-year-old female had very intense right-shoulder pain that was exacerbated at night. Anti-inflammatory treatment was unsuccessful. Magnetic resonance imaging of the shoulder showed a small inflammatory process that did not explain the intensity of the patient's pain. There was no Visual Ear Skin Point (VESP) in the Auricular Point (AP) corresponding to the shoulder, but revealed a very intense VESP in the AP corresponding to the lung. Acupuncture of the AP Lung stopped the shoulder pain immediately. Auricular Causative Diagnosis indicated that the shoulder pain was referred caused by underlying lung pathology, as lung and shoulder have the same segmental innervation. Thoracic scanning showed a small cancer tumor developing in the upper lobe of the right lung. This early diagnosis enabled successful oncologic treatment and complete remission of the cancer.
Clinical case 3 (Fig. 11)
A 65-year-old female presented with regular and frequent attacks (at least one every week) of a strong pain in the heart area. Analgesics did not relieve the pain. Only a glass of cold water helped to diminish each attack. The patient was hospitalized numerous times in the emergency room, but heart monitoring did not reveal any significant heart pathology. ACD did not reveal a VESP in the AP corresponding to the heart but did reveal a very strong VESP in the AP corresponding to the stomach. Acupuncture of the AP Stomach stopped the pain in the heart area immediately. Application of an Aiguille Semi-Permanent (ASP®) ear needle in the AP Stomach cured this patient's pain attacks completely. Thus, ACD indicated that the pain in the heart area was a referred pain, caused by the underlying stomach pathology, as the stomach and heart have the same segmental innervation. A gastroscopy was performed and revealed a small stomach ulcer.

Clinical case 3. A 65-year-old female had attacks of intense pain often in the heart area, which analgesics did not relieve. A glass of cold water helped to diminish each attack. She was hospitalized numerous times, but heart monitoring did not reveal any significant heart pathology. She did not have a Visual Ear Skin Point (VESP) in the Auricular Point (AP) corresponding to the heart but had a very intense VESP in the AP corresponding to the stomach. Acupuncture of the AP Stomach stopped the pain in the heart area immediately. Application of an Aiguille Semi-Permanent (ASP®) ear needle in the AP Stomach completely cured the painful attacks. Auricular Causative Diagnosis indicated that the pain in the heart area was referred, caused by underlying stomach pathology, because the stomach and heart have the same segmental innervation. Gastroscopy revealed a small stomach ulcer.
Clinical case 4 (Fig. 12)
A 38-year-old male presented with chronic, intense low-back pain of 3 years' duration. His double herniation at L-4–L-5 and L-5–S-1, was treated unsuccessfully by anti-inflammatory medication and numerous infiltrations. ACD revealed a very intense VESP in the AP corresponding to the prostate. Acupuncture of the AP Prostate stopped the pain immediately in patient's lower back. Application of an ASP ear needle in the AP Prostate cured the lower-back pain completely. Thus, ACD indicated that the pain in the patient's lower back was a referred pain caused by underlying pathology in his prostate, as the prostate and lower back have the same segmental innervation. Urologic investigation were conducted and revealed an old chronic inflammation in the patient's prostate.
Clinical case 4. A 38-year-old male had chronic, intense low-back pain for 3 years. His double herniation at L-4–L-5 and L-5–S-1 was treated unsuccessfully by anti-inflammatory medication and numerous infiltrations. He had a very intense Visual Ear Skin Point in the Auricular Point (AP) corresponding to the prostate. Acupuncture of the AP Prostate stopped the low-back immediately. Application of an Aiguille Semi-Permanent (ASP®) ear needle in the AP Prostate cured the low-back pain completely. Auricular Causative Diagnosis indicated that the low-back pain was referred, caused by underlying pathology in the prostate, as the prostate and lower back have the same segmental innervation. Urologic investigations were performed and revealed an old chronic inflammation in the patient's prostate.
Clinical case 5 (Fig. 13)
A 42-year-old male presented with chronic, intense low-back pain for past 8 years. This condition was treated unsuccessfully with anti-inflammatory medication and numerous infiltrations. Scanning investigation revealed that he had arthritis of a few lumbar vertebrae. This patient's pain was exacerbated early in the morning, which would awaken him. ACD revealed a very intense VESP in the AP corresponding to the large intestine. Acupuncture of the AP Large Intestine stopped the pain in the patient's lower back immediately. Application of an ASP ear needle in the AP Large Intestine diminished the early morning attacks of low-back pain significantly and improved the patient's sleep. Thus, ACD indicated that the pain in the patient's lower back was a referred pain caused by underlying pathology in the large intestine, as the large intestine and low back have the same segmental innervation. Endoscopy of the patient's colon was performed and revealed that he had Crohn's disease.

Clinical case 5. A 42-year-old male had chronic, intense low-back pain for 8 years, which was treated unsuccessfully with anti-inflammatory medication and numerous infiltrations. Scanning investigation showed arthritis of a few lumbar vertebrae. The patient's pain was exacerbated early in the morning, which awakened him. Auricular Causative Diagnosis (ACD) revealed very strong Visual Ear Skin Point (VESP) in the Auricular Point (AP) corresponding to the large intestine. Acupuncture of the AP Large Intestine immediately stopped the lower back pain. Application of an Aiguille Semi-Permanent (ASP®) ear needle in the AP Large Intestine diminished the early morning attacks of the low-back pain significantly and improved the patient's sleep. ACD indicated that the pain in the lower back was a referred pain, caused by underlying pathology in the large intestine, as the large intestine and lower back have the same segmental innervation. Endoscopy of the colon revealed Crohn's disease.
Clinical case 6 (Fig. 14)
A 22-year-old female presented with chronic, intense low-back pain and chronic severe diarrhea (10–12 stools per day), which were resistant to all medical treatments for the 5 years prior to her presentation. ACD revealed a very intense VESP in the AP corresponding to the genitals. Acupuncture of the AP Genitals stopped both the pain in the patient's low back and her intestinal cramps immediately. Application of an ASP ear needle in the AP Genitals cured the low back pain completely and diminished the occurrence of diarrhea significantly. Thus, ACD indicated that the pain in the low back as well as the colitis were referred pain, caused by underlying pathology in the genitals, as the genitals, colon, and lower back have the same segmental innervation. The beginning of all the pathologic symptoms coincided with the beginning of the patient's use of oral contraception. The patient was advised to stop using the contraceptive pills and, after a few acupuncture treatments targeting the gynecologic condition, using AP Genitals and Chong Mai Extraordinary Meridian, all of the pathologic symptoms disappeared.
Clinical Case 6. A 22-year-old female had chronic, intense low-back pain and chronic severe diarrhea for 5 years. Both conditions were resistant to all medical treatments. Auricular Causative Diagnosis revealed a very intense VESP in the Auricular Point (AP) corresponding to the genitals. Acupuncture of the AP Genitals stopped the low-back pain and intestinal cramps immediately. Application of an Aiguille Semi-Permanent (ASP®) ear needle in the AP Genitals cured the low-back pain completely and diminished the patient's diarrhea significantly. ACD indicated that the low-back pain and the colitis were referred, caused by underlying pathology in the genitals, as the genitals, colon, and lower back have the same segmental innervation. The beginning of all this patient's pathologic symptoms coincided with her beginning to use oral contraception. She was advised to stop taking the contraceptive pills. After a few acupuncture treatments targeting the gynecologic condition, using AP Genitals and the Chong Mai Extraordinary Meridian, all of the patient's symptoms disappeared.
Clinical case 7 (Fig. 15)
A 20-year-old female presented with acute, intense low-back pain after a trip to China. ACD revealed very strong VESP in the AP corresponding to the large intestine. Acupuncture of the AP Large Intestine stopped the low-back pain immediately. Application of an ASP ear needle in the AP Large Intestine cured the low-back pain completely. Thus, ACD indicated that the pain in the low back was a referred pain caused by an underlying pathology in the large intestine, because the large intestine and low back have the same segmental innervation. Laboratory investigations revealed amoeba invasion of the patient's large intestine and she received a specific treatment for it. Thus, because of ACD, this patient was not only completely healed from the acute low-back pain but was also prevented from developing a potentially chronic intestinal infection.

Clinical case 7. A 20-year-old had acute, intense low-back pain after traveling abroad. She had an intense Visual Ear Skin Point (VESP) in the Auricular Point (AP) corresponding to the large intestine. Acupuncture of the AP Large Intestine stopped the low-back pain immediately. Application of an Aiguille Semi-Permanent (ASP®) ear needle in the AP Large Intestine cured the low-back pain completely. Auricular Causative Diagnosis (ACD) indicated that the low-back pain was referred, caused by underlying pathology in the large intestine, because the large intestine and lower back have the same segmental innervation. Laboratory investigations revealed amoeba invasion of the large intestine. The patent received a specific treatment for this infection. ACD enabled this patient to be completely healed of her acute low-back pain and prevented her intestinal infection from becoming chronic.
Clinical case 8 (Fig. 16)
A 14-year-old female presented with chronic, intense low-back pain that was considered by an orthopedist to be “growing pains.” All orthopedic treatments were unsuccessful. ACD revealed very strong VESP in the AP corresponding to the kidneys. Acupuncture of the AP Kidneys stopped the low-back pain immediately. Application of an ASP ear needle in the AP Kidneys cured the low-back pain completely. Thus, ACD indicated that the pain in the low back was a referred pain caused by underlying pathology in the kidneys, because the kidneys and the low back have the same segmental innervation. A scan of the patient's kidneys was performed and a 2-cm lithiasis was found in the left kidney. The patient received a specific treatment for this. Thus, because of the ACD, she was not only completely healed from the chronic low-back pain, but also a potentially chronic kidney disease was also prevented.
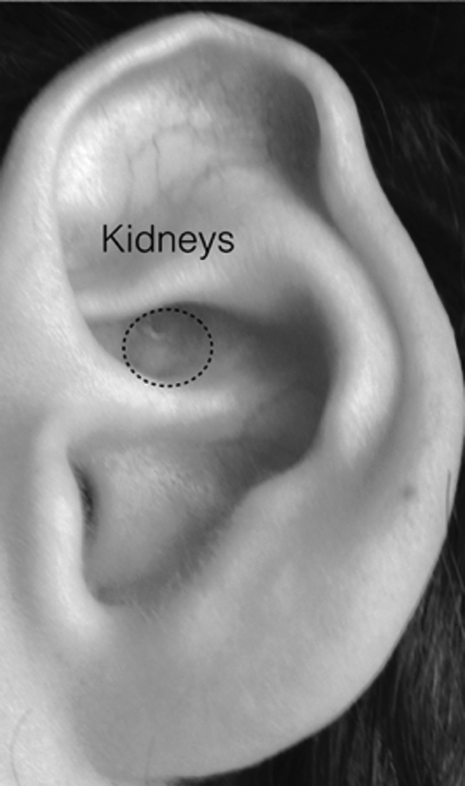
Clinical case 8. A 14-year-old female had chronic, intense low-back pain that was considered by an orthopedist to be “growing pains.” All orthopedic treatments were unsuccessful. She had an intense Visual Ear Skin Point in the Auricular Point (AP) corresponding to the kidneys. Acupuncture of the AP Kidneys stopped the low-back pain immediately. Application of an Aiguille Semi-Permanent (ASP®) ear needle in the AP Kidneys cured the low-back pain completely. Auricular Causative Diagnosis indicated that the low-back pain was referred, caused by underlying pathology in the kidneys, because the kidneys and lower back have the same segmental innervation. A scan of the patient's kidneys showed a 2-cm lithiasis in the left kidney. She received a specific treatment for it. ACD completely healed this patient's chronic low-back pain and prevented the development of a potentially chronic kidney disease.
Conclusions
Classical acupuncture, since ancient times, was based on the consideration of “the root and the branches”—the finding of the inner reason of the development of the symptom, which is specific to each patient. 17
“The normal physician sees the symptom and relieves it.”
“The better physician finds the inner cause of the pathological condition and treats the illness”
“The greatest physician discovers the fragility of the body before the symptom appears and prevents the illness.” 18
The ACD approach allows visualization of the status of all organs, provides the functional diagnosis, shows the origin of the pathology, and helps follow its evolution to determine a global therapeutic approach and to orient prevention. The ACT, based on the ACD tremendously increases the efficacy of auricular therapy, and of acupuncture in general, and allows immediate release of patients' suffering.
To support this study of clinical cases, provided by >30 years of practice, the current authors believe that evaluations using a double-blinded procedure and animal trials should be performed.
Footnotes
Author Disclosure Statement
There are no competing financial interests to declare.