
Abstract
Objectives:
Available literature highlights the effectiveness of Acupuncture or Acupressure on the Spleen 6 acupoint (Sanyinjiao or SP-6) for pain management in primary dysmenorrhea (PD). The objective of the current systematic review and meta-analysis is to provide an updated assessment of available randomized and non-randomized controlled trials and to compare the effectiveness of acupressure and acupuncture stimulation of Sanyinjiao among patients with PD.
Methods:
We conducted a comprehensive literature search on various electronic databases including Embase, PubMed, and the Cochrane Library from January 1990 to March 2023 to identify the comparative studies (randomized and non-randomized controlled trials) that assessed the effects of acupressure or acupuncture on the Sanyinjiao acupoint in patients with PD. We assessed the studies' risk of bias in accordance with the Cochrane Handbook for Systematic Reviews of Interventions, and certainty of evidence using the Grading of Recommendations Assessment. Subsequently, a fixed-effects meta-analysis was performed using the Der-Simonian and Laird method to combine intervention effects from the included studies. The primary outcome of interest was a reduction in pain.
Results:
We included 19 studies (9 acupressure and 10 acupuncture) with 1171 PD patients. This meta-analysis showed a significant (Standardized Mean Difference, SMD: −0.29, 95% confidence interval −0.41 to −0.17, p < 0.001) reduction in pain, for both acupressure and acupuncture at Sanyinjiao acupoint with considerable heterogeneity. Acupressure was found to be more effective than acupuncture stimulation in reducing pain associated with PD (SMD: −0.52, 95% confidence interval −0.71 to −0.33, p < 0.001).
Conclusion:
The findings of this updated systematic review and meta-analysis suggest that both acupuncture and acupressure on Sanyinjiao acupoint could effectively reduce pain associated with PD. Acupressure stimulation, in particular, was found to be more effective than acupuncture stimulation of the acupoint in reducing pain associated with PD.
BACKGROUND
Primary dysmenorrhea (PD) is a common condition that negatively impacts the quality of life (QOL) in women. 1 It leads to physical pain, with concurrent social and psychological distress, frequently accompanied by other symptoms such as sweating, headache, nausea, vomiting, tiredness, and diarrhea. 2 Globally, about 50–90% of women of reproductive age are affected with dysmenorrhea. 3 Approximately 50% of teenagers, adult women, or adolescent girls have skipped school or work at least once due to PD, which negatively impacts QOL and reduces female productivity. 4 Conventional medicines such as paracetamol, aspirin, and non-steroidal anti-inflammatory drugs are commonly used to manage dysmenorrhea. They work by inhibiting the cyclooxygenase 2 pathway. In addition, oral contraceptives are also used, but less frequently, as they act through the inhibition of ovulation. 5
Lack of appropriate pain relief through conventional medications leads women to adopt self-care strategies. These strategies often involve complementary, non-pharmacological, or traditional medicine approaches. Women can practice self-care techniques, which include physical and psychological lifestyle interventions, such as yoga, exercise, heat therapy, meditation, aromatherapy, self-massage, and acupressure. 6 In addition, non-pharmacological traditional complementary and integrative medicine (TCIM) interventions such as massage, acupuncture, and hydrotherapy are commonly used to manage dysmenorrhea. 6 By incorporating these practices, women may experience relief from menstrual pain, reduce their reliance on analgesics, and improve their overall health-related QOL. 6
Acupuncture is considered one of the TCIM therapies for dysmenorrhea and can be used to reduce the requirement for conventional medicines to reduce pain and thereby minimize adverse effects due to conventional medications. 7 SP-6 (Sanyinjiao) is located three Finger-cun (F-cun) above the medial malleolus behind the posterior border of the tibia. 8 The cause of dysmenorrhea, according to traditional Chinese medicine (TCM), is Cold-Damp stagnation and blood stasis in the Uterus. Sanyinjiao is a crucial point for treating dysmenorrhea due to its anatomical connection to the Uterus, sensitivity during dysmenorrhea, and role in addressing the Cold-Damp Stagnation pattern. As the intersecting point of the SPLEEN, LIVER, and KIDNEY channels, SP-6 regulates and harmonizes Qi and Blood, improving the nourishment of Chong Mai (the Thoroughfare Vessel), Ren Mai (the Conception Vessel), and the Uterus. It is a specific and compelling point for addressing PD.9,10
A previous systematic review and meta-analysis 11 published in 2013, comprising eight studies (four on acupressure and four on acupuncture), reported evidence that “acupressure” at the SP-6 acupoint may be effective in managing pain in PD. However, “acupuncture” at SP-6 was not found to be more effective than the control group, and further clinical studies were recommended. 11 Similarly, another systematic review and meta-analysis 12 published in 2016 reported that acupressure at the SP-6 acupoint, administered by trained acupuncture specialists, could be effective in pain reduction. 12 However, this review included only six studies, and neither of the reviews assessed the certainty of evidence.
The purpose of this systematic review and meta-analysis is to identify, update, and assess any additional studies investigating the effectiveness of the SP-6 acupoint in PD. In addition, our aim is to conduct a subgroup analysis to compare the effectiveness of acupuncture versus acupressure stimulation of the SP-6 acupoint in PD and to assess the certainty of evidence.
METHODS
The current systematic review was registered with The International Prospective Register of Systematic Reviews—PROSPERO (
Search Strategy
Electronic databases, including Embase, PubMed, and the Cochrane Library, were searched with English language restrictions from inception up to March 30, 2023. Medical Subject headings (MeSH terms) were employed, including (“Acupuncture”[Mesh] AND “Acupuncture Therapy”[Mesh] AND “Acupuncture Analgesia”[Mesh] AND “Acupuncture Points”[Mesh] AND “Acupressure”[Mesh] AND “Dysmenorrhea”[Mesh]), and keywords related to PD, such as dysmenorrhea, pain, menstrual, menstrual pain, menstrual pains, pains, menstrual, menstruation, painful menstruations, painful menstruation, painful periods, period pain, and intervention-related terms such as acupressure and acupuncture targeting the Spleen meridian, Sanyinjiao, or Spleen 6 (SP-6) (see Supplementary Table S1).
Inclusion and Exclusion Criteria
Studies that met the following criteria were eligible for inclusion: (1) published in the English language; (2) Randomized controlled trials and non-randomized controlled trials assessing the effect of acupuncture or acupressure at Sanyinjiao (Spleen-6 or SP-6) alone in patients with PD; (3) studies that used visual analog scale (VAS) or numerical rating scale to assess pain severity were included. Observational studies, case reports, reviews, and conference or poster abstracts assessing the effect of Sanyinjiao were excluded.
Data Collection, Extraction, and Assessment
Two reviewers (DB and PR) independently conducted duplicate screening of all titles and abstracts, excluding studies that did not meet the inclusion criteria. Full texts of selected articles were reviewed by one reviewer (AA) and cross-checked by a second reviewer (YC). Any disagreements were resolved through discussions with senior reviewers (MK, VV, MK, and MV). Data extraction was performed by three reviewers (MV, MK, and DB) using Microsoft Excel. Extracted data included study characteristics (study design, sample size, and location), participant details, intervention specifics, and outcomes.
Assessment of Risk of Bias
The quality of studies included in this review was evaluated using version 1 of the Cochrane Risk of bias assessment tool (RoB 1). The RoB 1 covers all types of bias arising from the randomization process; bias due to deviations from intended interventions; bias due to missing outcome data; bias in the measurement of the outcome; and bias in the selection of the reported result. The evaluations were categorized as “Low,” “High,” or “Unclear.” Any disagreements among the authors were resolved through discussion. A summary of the risk of bias assessment for each included study was provided in the traffic light diagram.
Data Analysis
The data were analyzed using R software version (4.3.0) and RevMen 5.4.1. Efficacy values with 95% confidence intervals (CIs) were reported. Heterogeneity was estimated using the chi-squared test. I2 is expressed as the percentage of total variability due to heterogeneity. Statistical heterogeneity was considered low (I2 < 25%), moderate (I2 25%–49%), or high (I2 > 50%) (3). Given the diversity in interventions, study designs, and other conditions, it was expected that there would be substantial clinical heterogeneity across the included studies. Consequently, a fixed effects model was employed to determine the combined effect sizes of efficacy variables. Publication bias was assessed using funnel plots. 15 In addition, subgroup analysis was conducted based on acupressure and acupuncture, type of stimulation (electrical or manual), and by whom acupressure were applied (researcher or self). The certainty of evidence was assessed using GRADEPro (Grading of Recommendations, Assessment, Development, and Evaluation).
RESULTS
Search Results
Through a search of electronic databases, 1640 studies were identified. After excluding duplicate studies, 349 articles remained. Following screening titles and abstracts, we selected 100 studies to read their full texts. Ultimately, 11 studies were deemed eligible. In addition, we included 8 studies from a previous meta-analysis. 11 In total, 19 studies were incorporated into our current systematic review and meta-analysis (Fig. 1). Of the 19 studies, nine employed acupressure interventions, whereas the remaining 10 utilized acupuncture interventions.
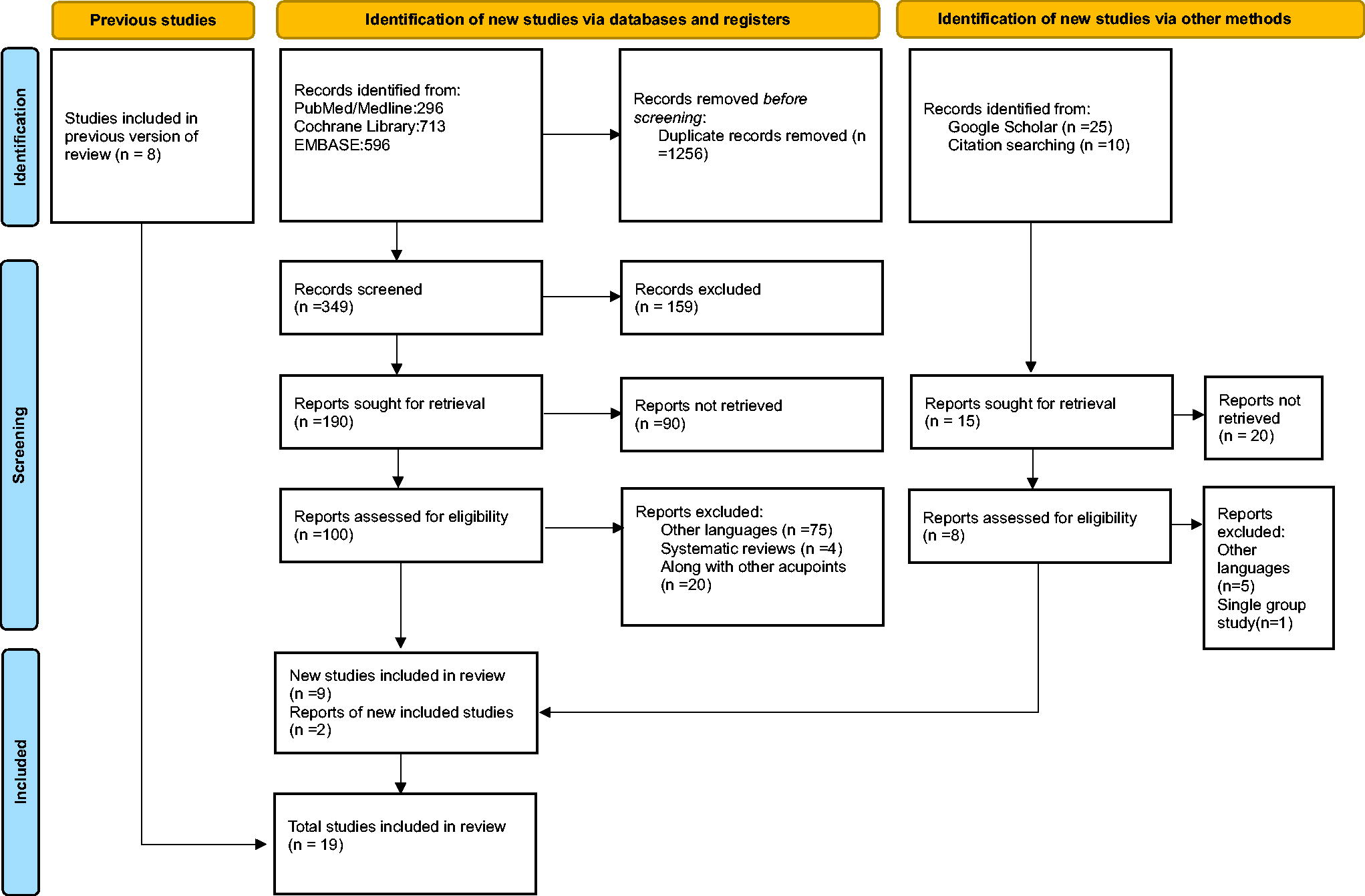
PRISMA flow diagram.
The Main Characteristics of Included Studies
The main characteristics of included studies were described in Table 1. A total of 19 studies (17 randomized and two non-randomized controlled trials) were included. Among the 19 included studies, 12 were conducted in China,7,9,16–25 three were from Iran,10,26,27 one was from France, 28 one from Korea, 29 one from Turkey, 30 and one from India. 31 Out of the 10 acupuncture studies, five applied manual stimulation along with acupuncture,7,17,21–23 whereas four applied electrical stimulation along with acupuncture.16,18–20 One study applied acupuncture without any stimulation. 9 Similarly, among the nine acupressure studies, only two28,30 administered self-acupressure application. In five studies, acupressure was applied by the researchers,10,25–27,29 while in one study, both patients and researchers applied acupressure. 24 In one study, details about the intervention application were not reported. 31
Main Characteristics of Included Studies
Biases Among Included Studies
The risk of bias in the included studies is presented in Figures 2 and 3. Fourteen studies described random sequence generation methods such as random.org program, 30 lottery method, 31 computer-based randomization program,7,16,18–21,23,28 centralized telephone randomization procedure, 21 random number table,17,27 random numbers generated with SPSS software, 9 whereas allocation concealment was utilized in 14 studies.7,9,10,16–23,28,30,31 Twelve trials7,9,16,18–23,26,29,30 employed blinding methods, blinding participants and therapists proved impractical. Nine studies were assessor-blinded.7,16,18–23,26 Eighteen studies7,9,10,16–30 showed a low risk of bias concerning incomplete outcome data. In addition, 11 studies7,9,10,18,20–23,29–31 had a low risk of selective reporting, and 10 studies7,9,10,20–23,27,28,30 had a low risk of other biases.
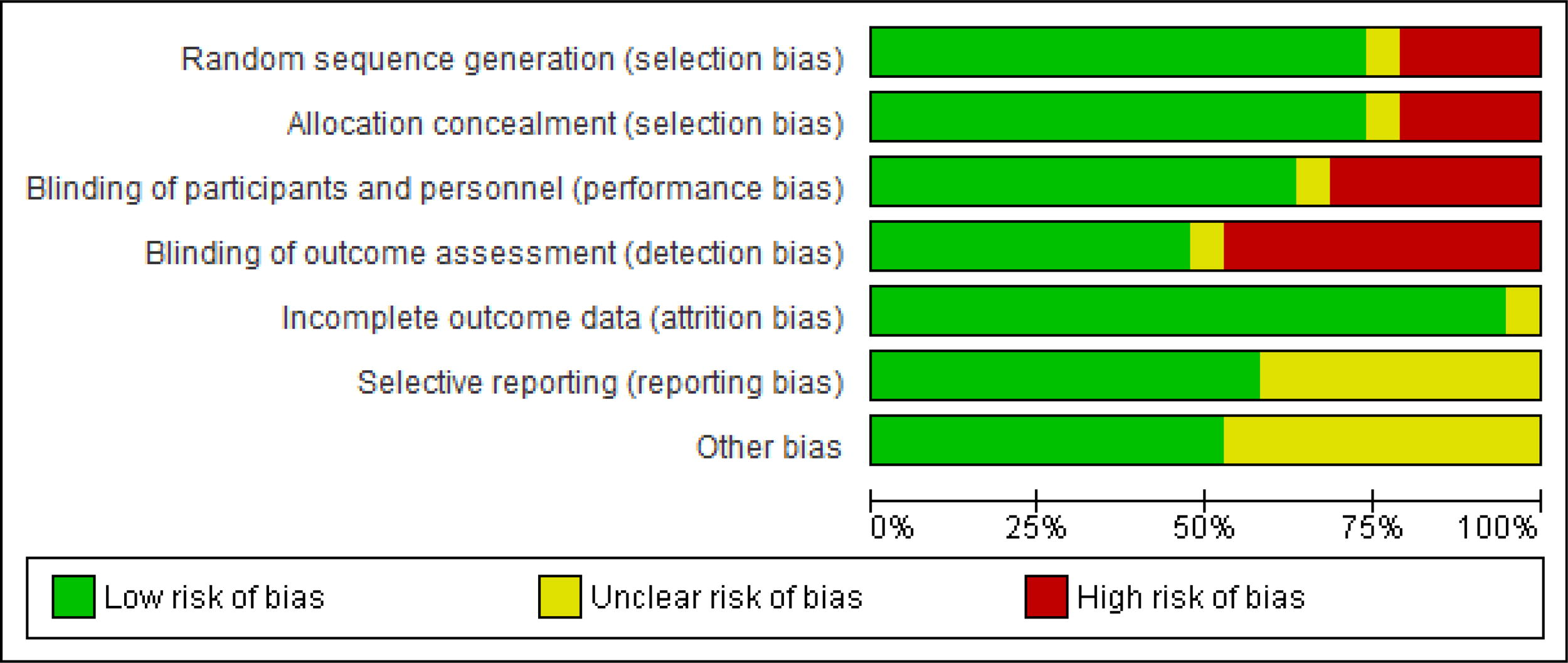
Risk of bias graph.
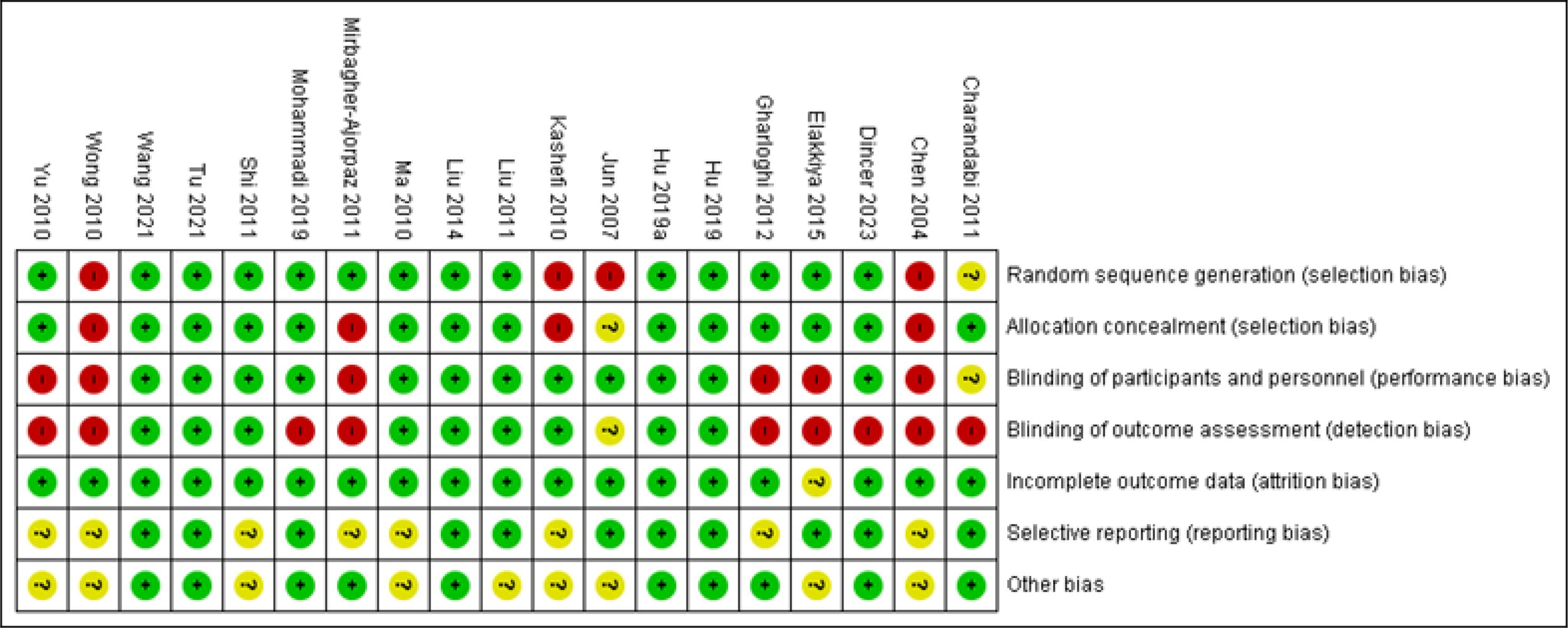
Risk of bias summary.
Efficacy of Acupressure or Acupuncture on Sanyinjiao Acupoint in PD
All the included studies evaluated the efficacy of acupressure or acupuncture on the Sanyinjiao acupoint in patients with primary dysmenorrhea, using the VAS scale. Heterogeneity existed among the studies, as indicated by the I2 statistic (p < 0.0001, I2 = 90%). Therefore, we employed a fixed-effect model to analyze the data (see Fig. 4). The Sanyinjiao acupressure or acupuncture group demonstrated a significant reduction in pain compared to the control group (Standardized Mean Difference, SMD: −0.29, 95% CI −0.41 to −0.17, p < 0.001).
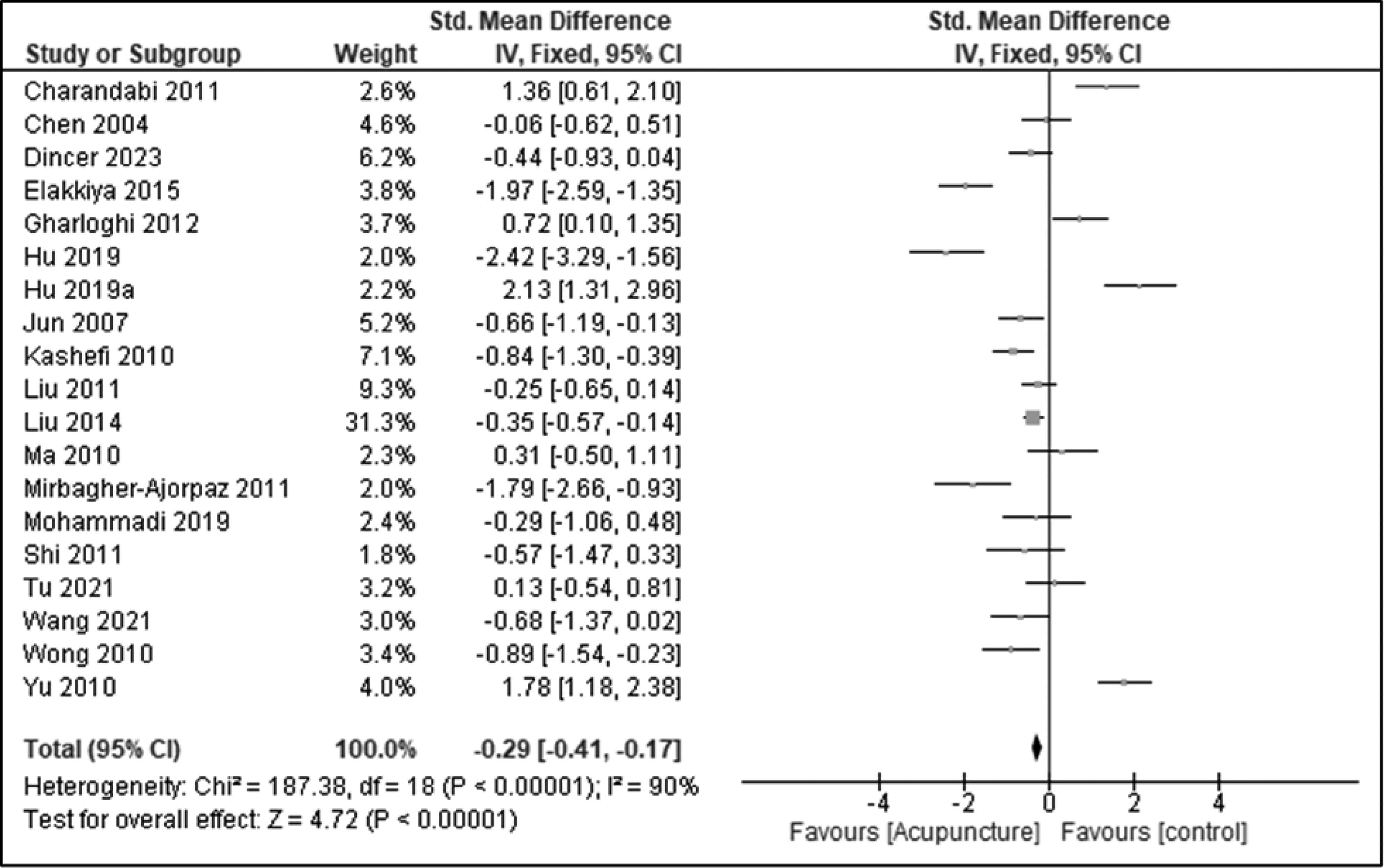
Meta-analysis results of the visual analog scale.
Subgroup Analysis
In the current updated systematic review and meta-analysis, we conducted a subgroup analysis based on acupressure and acupuncture. The meta-analysis revealed significant evidence supporting acupressure (Fig. 5) at the SP-6 acupoint (SMD: −0.52, 95% CI −0.71 to −0.33). However, for acupuncture (Fig. 6) at the SP-6 acupoint, the results showed a smaller effect size (SMD: −0.15, 95% CI −0.30 to 0.01). Further subgroup analysis was conducted to examine the application of acupressure by self or researcher. The pooled effects indicated that acupressure on the SP-6 point by the researcher (SMD: −0.45, 95% CI −0.71 to −0.19) significantly reduced the pain associated with PD (Fig. 7). However, no such changes were observed in self-acupressure (SMD: −0.01, 95% CI −0.39 to 0.38) (Fig. 8). Similarly, a subgroup analysis was performed based on the type of stimulation, namely electrical or manual. The pooled effects of the meta-analysis revealed that acupuncture on the SP-6 point with electrical stimulation (SMD: −0.31, 95% CI −0.49 to −0.13) significantly reduced pain in patients with PD (Fig. 9). On the other hand, acupuncture with manual stimulation (SMD: 0.38, 95% CI 0.06 to 0.70) on the SP-6 acupoint did not demonstrate similar beneficial effects (Fig. 10).
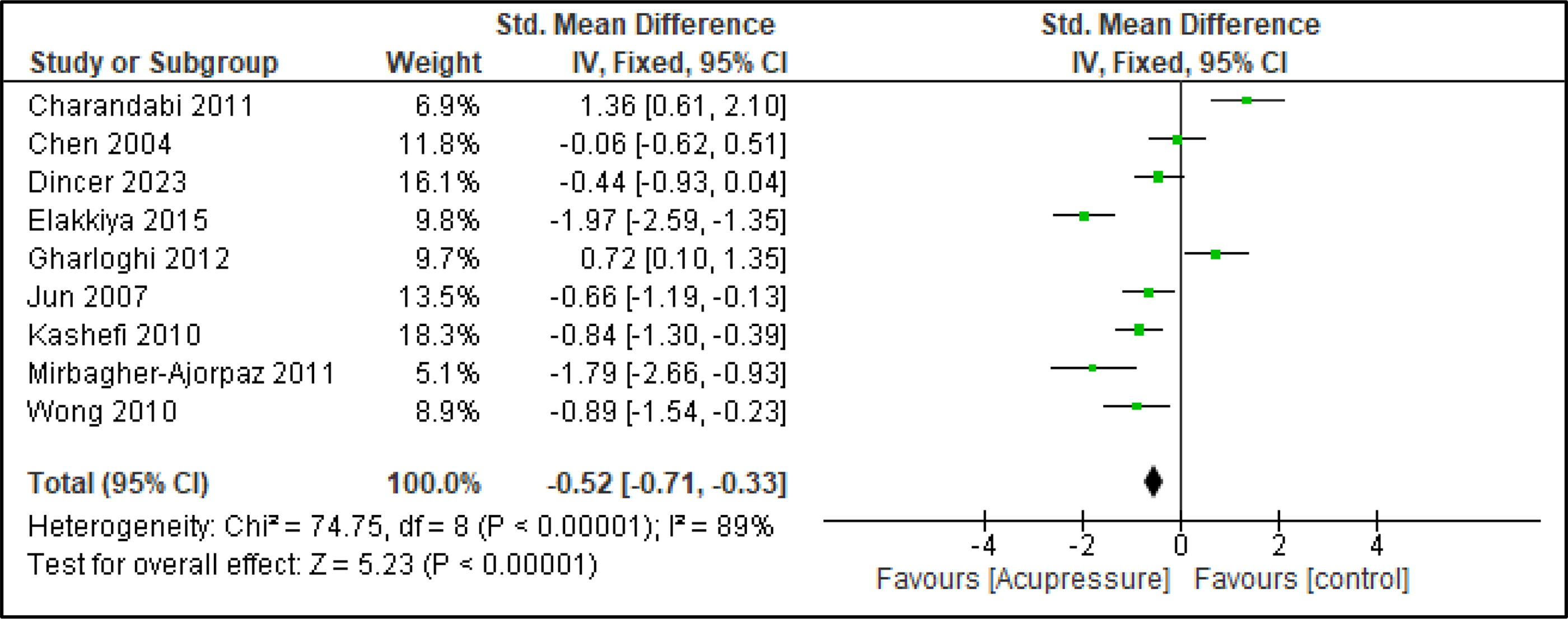
Effect of acupressure at SP-6 on visual analog scale.
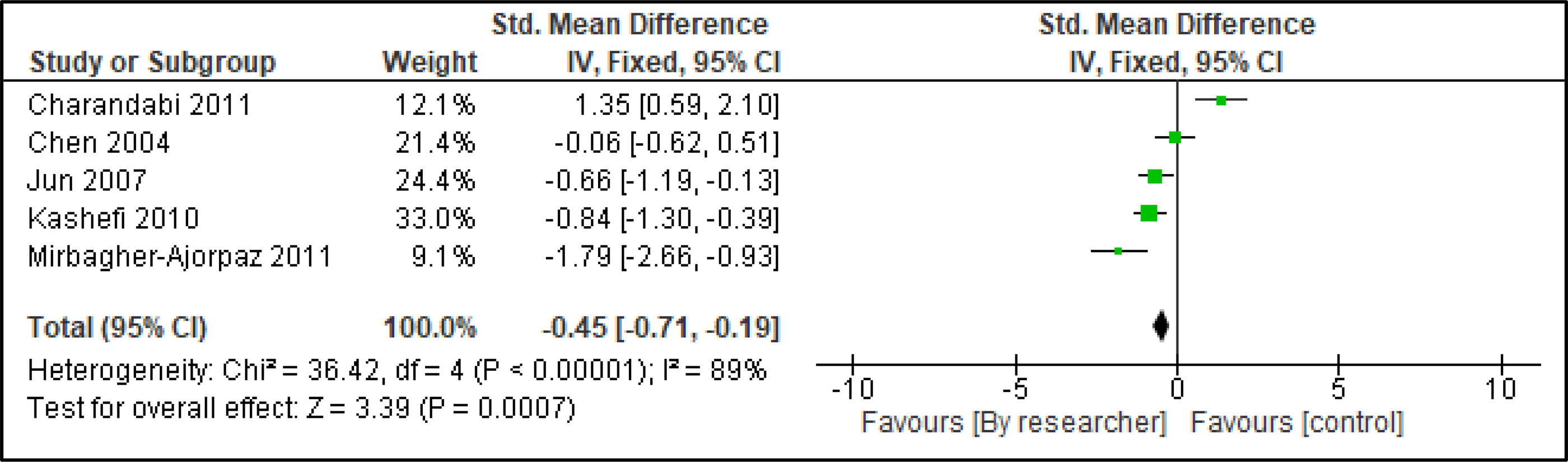
Effect of acupressure at SP-6 by researcher on visual analog scale.
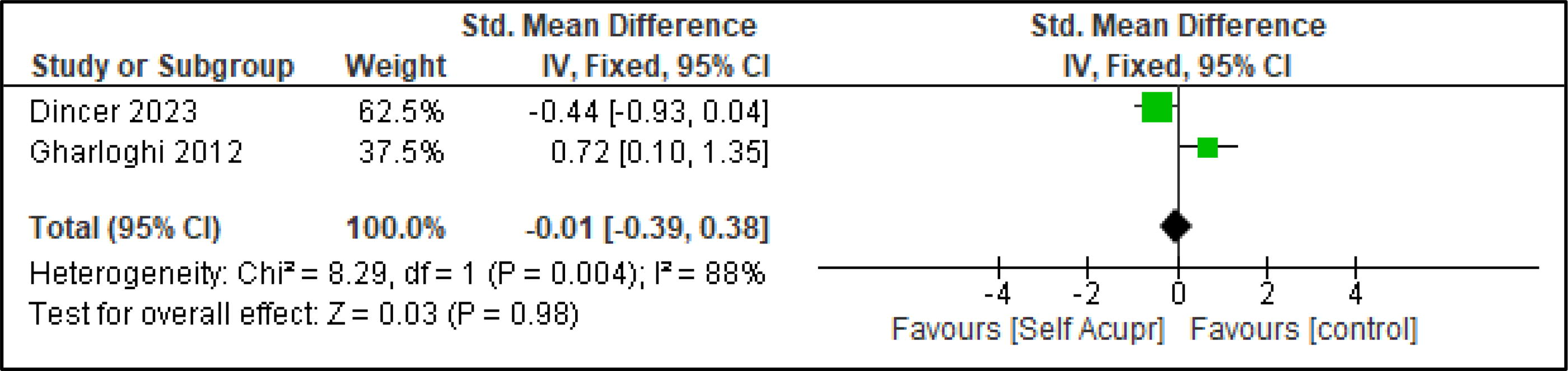
Effect of self-acupressure at SP-6 on visual analog scale.
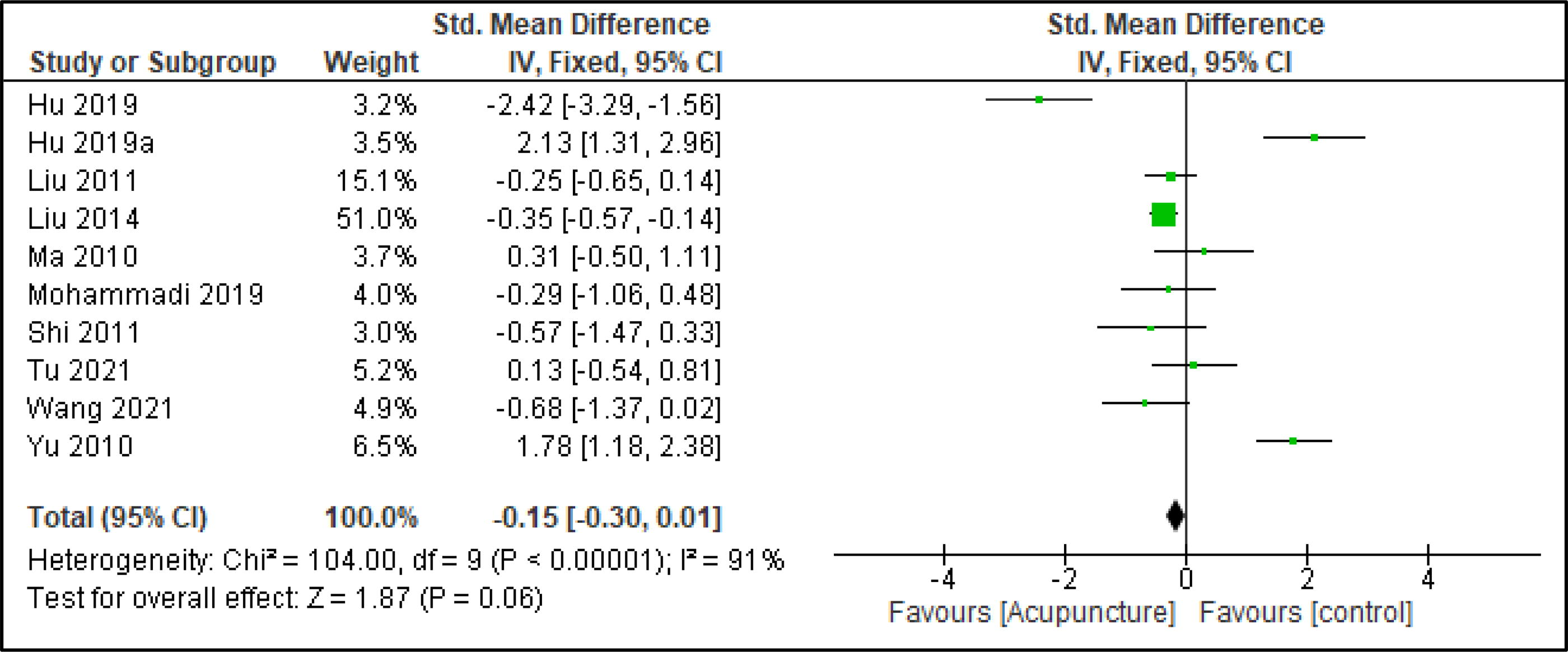
Effect of acupuncture at SP-6 on visual analog scale.
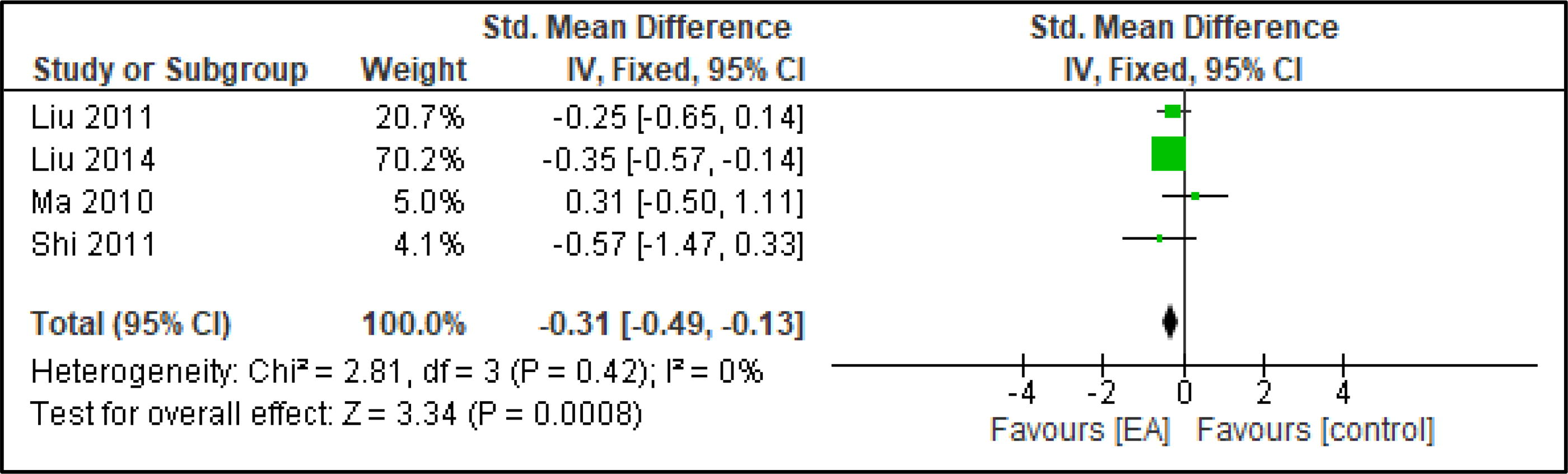
Effect of acupuncture with electrical stimulation on visual analog scale.
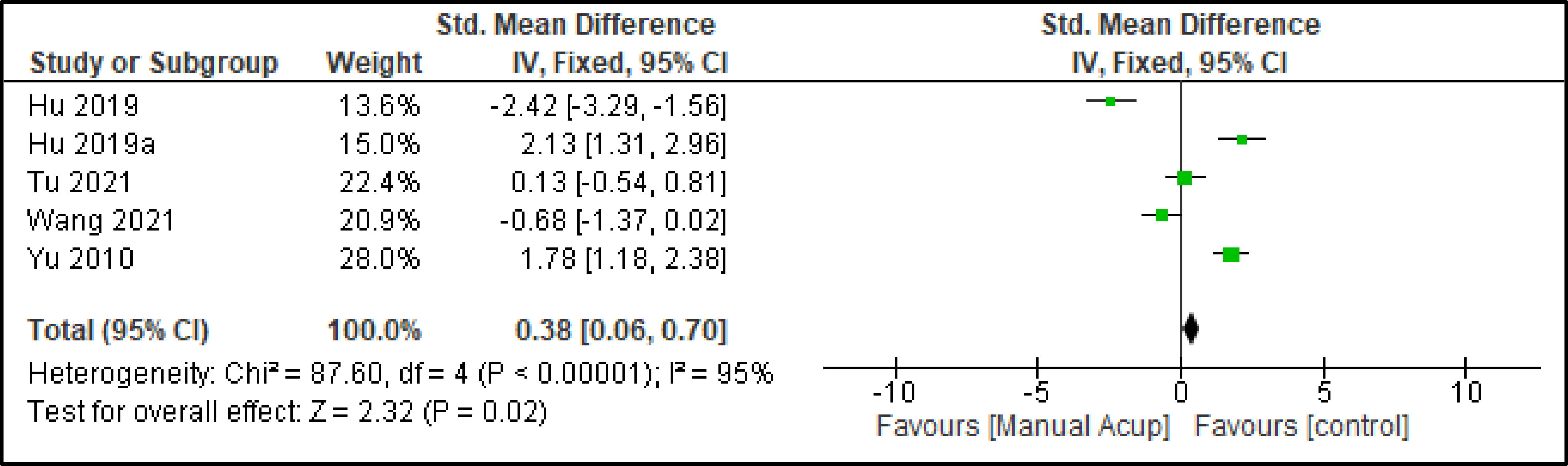
Effect of acupuncture with manual stimulation on visual analog scale.
Publication bias
The funnel plot (Fig. 11) and the results of Egger’s test (p = 0.78) and Begg’s test (p = 0.79) revealed no significant publication bias in these studies.
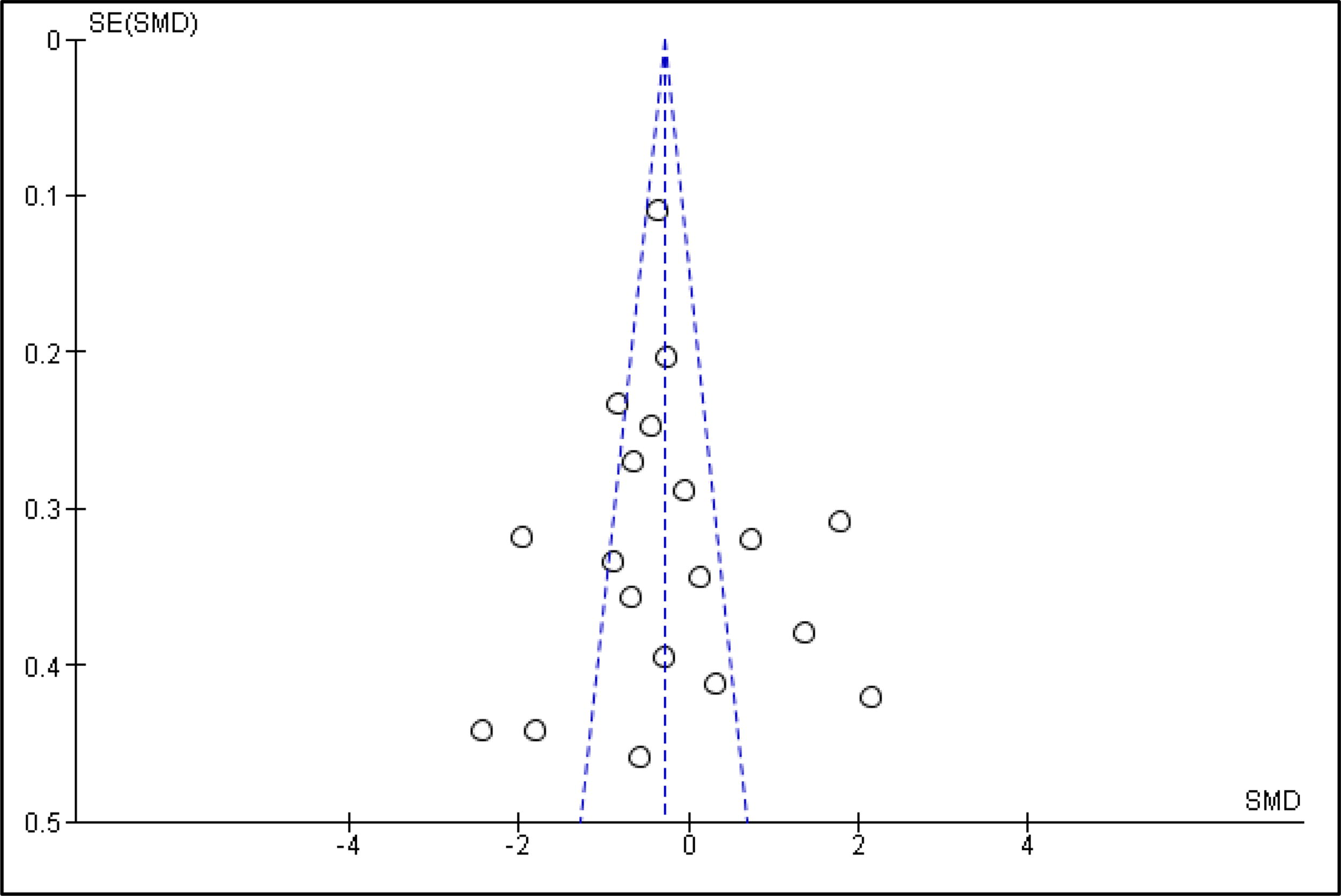
Funnel plot results of the visual analog scale.
Certainty of evidence
The certainty of evidence (see Supplementary Table 2) for the primary outcome was low to moderate (SMD: 0.29).
DISCUSSION
Acupressure or acupuncture on the SP-6 acupoint has been found to be effective in managing pain associated with PD. This current updated systematic review and meta-analysis aim to provide the most recent evidence available in the scientific literature. The results of the current review demonstrate that both acupuncture and acupressure stimulation on the SP-6 acupoint could significantly reduce pain associated with PD, with better results obtained using acupressure stimulation. Likewise, in acupuncture, electrical stimulation was found to be better than manual stimulation of the acupoint in providing better results. However, the certainty of evidence is lower for the primary outcome.
Previous systematic reviews and meta-analyses 11 results indicated that acupressure at SP-6 could be effective in reducing pain in PD. Consistent with this, the current review findings also showed a significant reduction in pain associated with PD. In addition, the current review found that acupressure administered by researchers is more effective than self-acupressure. On the other hand, acupuncture did not show a significant effect, which aligns with the findings of the previous review. Another systematic review and meta-analysis 12 investigating the effectiveness of SP-6 acupressure in managing PD symptoms also reported a significant reduction in pain intensity when delivered by trained personnel (SMD: = −0.72; CI = −0.95 to −0.58; p = 0.000). Consistent with these results, our current study demonstrated that acupressure administered by the researcher (trained by an acupuncture specialist) effectively reduced pain (SMD: −0.45, 95% CI −0.71 to −0.19) in PD patients.
Dysmenorrhea is classified as primary if there is no underlying pelvic or hormonal pathology and as secondary when it is associated with one or more pathological conditions. 32 PD is caused by producing uterine ischemia in response to elevated levels of prostaglandin E2 and F2 alpha (PGF2) released from shedding endometrium. The PGF2 alpha activity is twice as high in dysmenorrhea patients when compared to eumenorrhoeic women. In addition, elevated levels of leukotrienes are also noted in dysmenorrhoeic patients, which may be related to the inflammatory response during PD. 33 The uterine basal tone is elevated, and the uterine contractions are increased and found non-rhythmic in PD patients. These abnormalities cause the uterus to receive inadequate oxygen and blood flow, resulting in pain.33,34 PD is usually classified into spasmodic and congestive types. The spasmodic type is acute and confined to body parts innervated by uterine and ovarian nerves and usually occurs in the first 2–3 days of menstruation, whereas the congestive type is related to premenstrual syndrome. 35 According to TCM, dysmenorrhea is usually classified into two types, 1. Xu type (Spasmodic) due to Qi and blood deficiency, particularly in the LIVER and KIDNEY, and 2. Shi type (congestive) due to stagnation of blood in the uterus. 36 SP-6 is the intersection of three meridians, namely SPLEEN, LIVER, and KIDNEY. According to TCM, dysmenorrhea is caused mainly by deficiency of Qi and blood in kidney and liver elements or stagnation of blood in elements related to the reproductive system (mainly LIVER, SPLEEN, and KIDNEY). Thus, treating PD patients by SP-6 nourishes Qi and blood and removes stagnation of blood in LIVER, KIDNEY, and SPLEEN . 10
One major strength of the meta-analyses is that, instead of limiting ourselves only to finding the efficacy of SP-6 on pain in PD, we conducted a subgroup analysis on the most effective ways to stimulate the acupoint as well. Our meta-analyses have a few limitations as well, which we would like to highlight. Firstly, we limited our literature search to only English, potentially missing relevant trials in other languages. Secondly, the studies identified showed significant heterogeneity, possibly impacting the meta-analyses’ outcomes. Thirdly, none of the included studies, particularly those involving acupuncture as an intervention, reported any adverse events. Healthcare practitioners should consider integrating acupuncture and acupressure on the SP-6 acupoint for effective PD pain management, with acupressure demonstrating potential advantages. Future research should focus on optimal protocols, long-term effects, and combination therapies involving acupuncture and acupressure for PD.
CONCLUSION
The evidence from the current updated systematic review suggests that both acupressure and acupuncture on SP-6 may be effective TCIM treatment modalities to reduce the pain associated with PD. Acupressure stimulation, in particular, was found to be more effective than acupuncture stimulation of the acupoint in reducing pain associated with PD.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.