
Abstract
To assess the pharmacokinetics of dapivirine in plasma and dapivirine concentrations in cervicovaginal fluids (CVF) and cervicovaginal tissues following vaginal administration of dapivirine microbicide gel in healthy, HIV-negative women for 10 days. A randomized, double-blind, phase I study was conducted at a single research center in South Africa. A total of 18 women used dapivirine gel (0.001%, 0.005%, or 0.02%) once daily on Days 1 and 10 and twice daily on Days 2–9. Pharmacokinetics of dapivirine were assessed in plasma on Days 1 and 10. Dapivirine concentrations were measured in CVF on Days 1 and 10 and in cervicovaginal tissues on Day 10. Safety was evaluated through laboratory tests (hematology, clinical chemistry, and urinalysis), physical examinations, and assessment of adverse events. Plasma concentrations of dapivirine increased over time with gel dose and were greater on Day 10 (Cmax 31 to 471 pg/ml) than Day 1 (Cmax 23 to 80 pg/ml). Tmax was 10–12 h on Day 1, and 9 h on Day 10. Concentrations in CVF generally increased with dose but were highly variable among participants. Mean peak values ranged from 4.6–8.3 × 106 pg/ml on Day 1 and from 2.3–20.7 × 106 pg/ml on Day 10 across dose groups. Dapivirine was detectable in all tissue biopsies on Day 10 at concentrations of 1.0–356 × 103 pg/mg.
Conclusions:
Dapivirine was widely distributed throughout the lower genital tract with low systemic absorption when administered in a vaginal gel formulation for 10 consecutive days. The gel was safe and well tolerated.
Introduction
M
Dapivirine (TMC120), a non-nucleoside reverse transcriptase inhibitor (NNRTI), is a promising microbicide candidate currently in development in multiple vaginal dosage forms for the prevention of HIV transmission to women. 9 –13 Dapivirine is a potent inhibitor of HIV-1 replication in vitro and in vivo 10,14 –16 and exhibits potent antiviral activity against multiple clades of HIV as well as both wild-type virus and strains harboring various resistance-inducing mutations. 15,16 We describe a phase I clinical trial of dapivirine vaginal gel in healthy, HIV-negative women. The trial was designed to evaluate the plasma concentrations and distribution of dapivirine throughout the lower genital tract over a 10-day administration period.
Materials and Methods
Study design
IPM004 was a randomized, double-blind, phase I clinical trial in healthy, HIV-negative women 18–50 years of age, conducted at a single phase I unit (FARMOVS-PAREXEL, Campus of the University of the Free State, Bloemfontein, South Africa).
The objectives of the study were to assess the pharmacokinetics of dapivirine in plasma and dapivirine concentrations in cervicovaginal fluids (CVF) and cervicovaginal tissues following vaginal administration of dapivirine microbicide gel in healthy, HIV-negative women for 10 days. Before study initiation, the study protocol was approved by the U.S. Food and Drug Administration, the South African Medicines Control Council, and the University of the Free State Ethics Committee (Bloemfontein, South Africa). All participants signed an informed consent form (or provided a thumbprint if illiterate) during screening. Screening visits were conducted up to 21 days prior to study entry. Women were advised prior to Day 1 to use condoms in addition to their usual contraceptive method (oral contraceptive, combined injectable, depot-medroxyprogesterone acetate, or intrauterine device). Participants were willing to be sexually abstinent from Day 1 through the end of the gel application period on Day 10.
A total of 18 women were randomized 1:1:1 to one of three concentrations of dapivirine gel (0.001%, 0.005%, or 0.02%) for use once daily on Days 1 and 10 and twice daily on Days 2–9. The date of randomization was to be planned so that menses did not occur during the 10-day gel application period. Pharmacokinetics of dapivirine were assessed in plasma on Days 1 and 10. Dapivirine concentrations were assessed in CVF on Days 1 and 10 and in cervicovaginal tissues on Day 10. Safety was evaluated through laboratory tests (hematology, clinical chemistry, and urinalysis), physical examinations, vital signs, and adverse events.
Investigational products
Dapivirine gel was manufactured and packaged by the International Partnership for Microbicides (Bethlehem, PA) as individual doses of 2.65 g (2.5 ml) in polyethylene vaginal applicators (HTI Plastics, Lincoln, NE). Dapivirine gel contained w/w 35.0% carbowax 300NF, 2.0% Natrosol 250HX Pharm, 0.65% Noveon AA-1 USP, 0.60% carbopol 1382, 0.20% methylparaben NF, 0.05% propylparaben NF, 0.09% sodium hydroxide, dapivirine (0.001%, 0.005%, or 0.02%), and purified water (q.s. to 100%).
Safety laboratories and adverse events
Blood samples for hematology and clinical chemistry were collected at screening and on Day 11. Urine dipsticks were done at screening and on Days 1 and 11. Specimen collection, handling, and processing were performed according to the local laboratory's standard operating procedures. Laboratory tests for genital infections (syphilis, trichomonas, gonorrhea, chlamydia, lymphogranuloma venereum, yeast, genital ulcer disease, bacterial vaginosis, and herpes simplex virus type 2) were performed at screening. HIV and serum pregnancy tests were performed at screening and on Days 1 and 11. Participants were monitored for treatment-emergent adverse events (TEAEs) at study visits on Days 1, 2, 10, and 11. Adverse event data were coded using MedDRA System Organ Classes and Preferred Terms. Severity of TEAEs and laboratory abnormalities were graded by the investigator according to the NIH Division of AIDS (DAIDS) Table for Grading the Severity of Adverse Experiences. 17 Causality of TEAEs was assessed by the investigator as related to study gel (definitely, probably, or possibly related) or not related to study gel (probably not related or not related).
Pharmacokinetics of dapivirine in plasma
Venous blood samples were collected for determination of dapivirine concentration in plasma on Day 1 (before gel application and 0.5, 2, 4, 6, 8, 12, and 24 h after) and on Day 10 (before gel application and 2, 4, 6, 8, 12, 24, 36, 48, 72, 96, 108, and 120 h after). Within 1 h of collection, blood samples were centrifuged to separate plasma, which was shipped frozen to the FARMOVS-PAREXEL Bioanalytical Services Division in Bloemfontein for bioanalysis. Dapivirine concentrations in plasma were determined by liquid chromatography with tandem mass spectrometry (LC-MS/MS). The assay method was validated in accordance with FARMOVS-PAREXEL's current standard operating procedures and acceptance criteria. The assay method provided an acceptable degree of accuracy (%Nom, 101–105) and precision (%CV, 5.3–9.0) over the concentration range of 5.00–4050 pg/ml. Variability across seven drug concentrations in intra-batch accuracy and intra-batch precision were %Nominal, 1.0 to 5.7 and CV%, 1.4 to 8.8, respectively.
Internal standard solution (6 ng/ml d4-isotope-labeled TMC120 in water; 100 μl), 500 μl sodium carbonate buffer (250 mM, pH 10.5), and 5 ml hexane:iso-amyl alcohol (98:2 v/v) were added to an 0.8 ml-aliquot of each thawed sample. After mixing and centrifugation, the aqueous phase was frozen in an alcohol bath, and the organic phase was decanted and evaporated to dryness. After adding 300 μl of each a methanol:water solution (10:90, v/v) and phosphate buffer (250 mM, pH 6.0), the sample was mixed and tert-butyl-methyl ether (TBME; 3 ml) was added. After mixing and centrifugation, the aqueous phase was frozen and the organic phase evaporated to dryness. Reconstitution solution (mobile phase:2% formic acid, 3:1 v/v; 150 μl) was added to each vial, samples were mixed and transferred for injection (35 μl) into the chromatographic system. The mobile phase consisted of acetonitrile:methanol:0.2% formic acid (40:20:40 v/v/v). HPLC column temperature was 30°C, and the flow rate was 0.265 ml/min.
Dapivirine concentrations in cervicovaginal fluids
Cervicovaginal fluid samples were collected at the introitus, mid-vagina, and cervix on Tear Flo™ Test Strips (Odyssey Medical, Bartlett, TN) on Day 1 (before gel application, and 0.25, 1, 4, and 8 h after) and on Day 10 (before gel application, and 4, 12, and 24 h after). Samples were collected from all participants at sequential time points on Day 1 and pre-dose on Day 10. For subsequent time points on Day 10, samples were collected from two participants per time point in each dose group according to a randomization schedule. Test strips were placed in the vaginal lumen using forceps and held in place for approximately 1 min. Samples were shipped on dry ice to Analytisch Biochemisch Laboratorium, Assen, The Netherlands (ABL) where they were stored frozen.
Dapivirine concentrations in CVF were determined by LC-MS/MS as follows. Acetonitrile (2 ml) was added to tubes containing sample test strips, samples were mixed and centrifuged, and a 100 μl aliquot of each sample was transferred to a clean vial. Internal standard solution (100 ng/ml TMC125 in methanol; 25 μl) was added, samples were mixed, and dilution buffer (10 mM ammonium formate in Elix water; 100 μl) was added. Samples were mixed, centrifuged, and transferred to an autosampler well plate. A 25 μl aliquot of each sample was injected into the chromatographic system. The mobile phase solutions were [100 mM ammonium formate + 0.5% formic acid in Elix water] (5%), Elix water (15–35%), and acetonitrile (60–80%). Column temperature was 40°C, and flow rate was 1.00 ml/min. The assay method provided an acceptable degree of accuracy (%Nom, 104.5–110.4) and precision (%CV, 6.4–8.0) over the concentration range of 40 to 40,000 pg/strip. Intra-batch precision (CV%) was 7.1 to 7.4, and inter-batch precision (CV%) was 6.3 to 8.0. Test strips were not calibrated for volume of fluid absorbed; therefore, CVF concentrations could not be calculated. However, based on the composition and size of the test strip, the estimated maximum absorption volume is 33 μl.
Dapivirine concentrations in cervicovaginal tissues
Cervicovaginal biopsies were obtained from each participant. Within each dose group, participants were randomized to have biopsies taken at 4, 12, or 24 h post gel application on Day 10 (two participants per time point in each dose group). Three full-thickness biopsies (measuring approximately 2 × 4 mm) were collected under propofol anesthesia from the vagina (near the vulva and near the cervix) and cervix. Samples were shipped on dry ice to ABL and stored frozen.
Dapivirine concentrations were determined by LC-MS/MS as follows. Tissues were weighed in dismembrator tubes. Elix water (1 ml) and 1 ml acetonitrile were added to each sample. Samples were homogenized for 2 min and transferred to extraction tubes. Methanol (50 μl) and 50 μl internal standard solution (1.0 μg/ml d4-isotope-labeled TMC120 in methanol) were added to each tube, samples were mixed, and 100 μl of 25% ammonium hydroxide solution were added. After addition of 4 ml TBME, tubes were rotated for 30 min, followed by centrifugation. Aqueous layers were frozen and organic layers were evaporated to dryness. The residue was dissolved in 500 μl TBME, and TBME was evaporated under a nitrogen stream. The final residue was dissolved in 500 μl injection solvent (20 mM ammonium formate in water:acetonitrile, 40:60 v/v). Samples were transferred to an autosampler well plate, and each sample (40 μl) was injected into the same chromatographic system used for analysis of CVF. The assay method provided an acceptable degree of accuracy (%Nom, 98.7–103.3) and precision (%CV, 3.2–6.2) over the concentration range of 250–200,000 pg/sample.
Statistics
The statistical analyses of the pharmacokinetic and safety endpoints were performed by FARMOVS-PAREXEL (Bloemfontein, South Africa) and Quintiles South Africa (Bloemfontein), respectively.
At randomization, each participant was assigned an identification number according to the randomization schedule provided by Quintiles. Participants, as well as clinical and nonclinical staff associated with the trial, were blinded to the randomization code. Participants were randomized in a stratified block design within dose groups in a 1:1:1 ratio to have three biopsies of cervicovaginal tissues taken at 4, 12, or 24 h post gel administration on Day 10 (two participants per time point in each dose group).
Participants with no major protocol violations and defined Cmax and AUC0-last values for dapivirine in plasma on Day 1 were included in the pharmacokinetic population. Pharmacokinetic parameters were calculated using the actual sampling intervals relative to application of study gel. All values below the limit of quantification (BLQ) were substituted with zeroes. Missing pharmacokinetic concentrations were not imputed.
The safety population included all participants who used at least one application of study gel and who had post-baseline safety data. Baseline was defined as the last observation prior to the first administration of study gel. IPM004 was not designed to detect statistically significant differences among the three study arms. The sample size was primarily driven by the intention to provide a descriptive measure of the pharmacokinetics of dapivirine in plasma and dapivirine concentrations in CVF and cervicovaginal tissues following administration of dapivirine gel for 10 days, and to build on an earlier pharmacokinetics study of a different dapivirine gel. A sample size of 18 (six participants per dose group) was considered to be sufficient for these purposes.
Results
Baseline characteristics
Four of six participants (67%) in each of the 0.001%, 0.005%, and 0.02% groups were black, and 33% were white. The mean ages for participants in the three dose groups were 34, 25, and 35 years, respectively. Other baseline characteristics (height, weight, and body mass index) were similar across dose groups.
Exposure and disposition
All randomized participants completed the study. For all participants in both the 0.001% and 0.02% groups, and five of six participants in the 0.005% group, 100% compliance with study gel usage (once daily on Days 1 and 10 and twice daily on Days 2–9) was suggested based on the number of returned, unused gel applicators. One participant in the 0.005% group used one extra dose of study gel during the 10-day study period.
Adverse events and safety laboratories
No serious adverse events occurred during the study. Blood in urine (5/6, 83%; 4/6, 67%; 5/6, 83%) and nitrites in urine (1/6, 17%; 3/6, 50%; 3/6, 50%) were the most common TEAEs in the 0.001%, 0.005%, and 0.02% dose groups, respectively. The day of onset for all but one of these events was Day 11, the day of (or the day after) collection of cervicovaginal tissue biopsies. Most blood-in-urine events (12 of 14) were considered to be probably not related to study gel; 2 of 14 were assessed as possibly related. All nitrites-in-urine events were considered to be possibly related to study gel. All other abnormal urinalysis results reported as TEAEs (bilirubin, protein, or white blood cells in urine) were assessed as possibly related to study gel and occurred in 0 to 2 participants in each dose group. The only other event considered to be possibly related to study gel was a urinary tract infection that occurred in the 0.005% group on Day 15 (5 days after the last gel administration) and was classified as Grade 2. All other events were assessed as not related or probably not related to study gel.
Pharmacokinetics of dapivirine in plasma
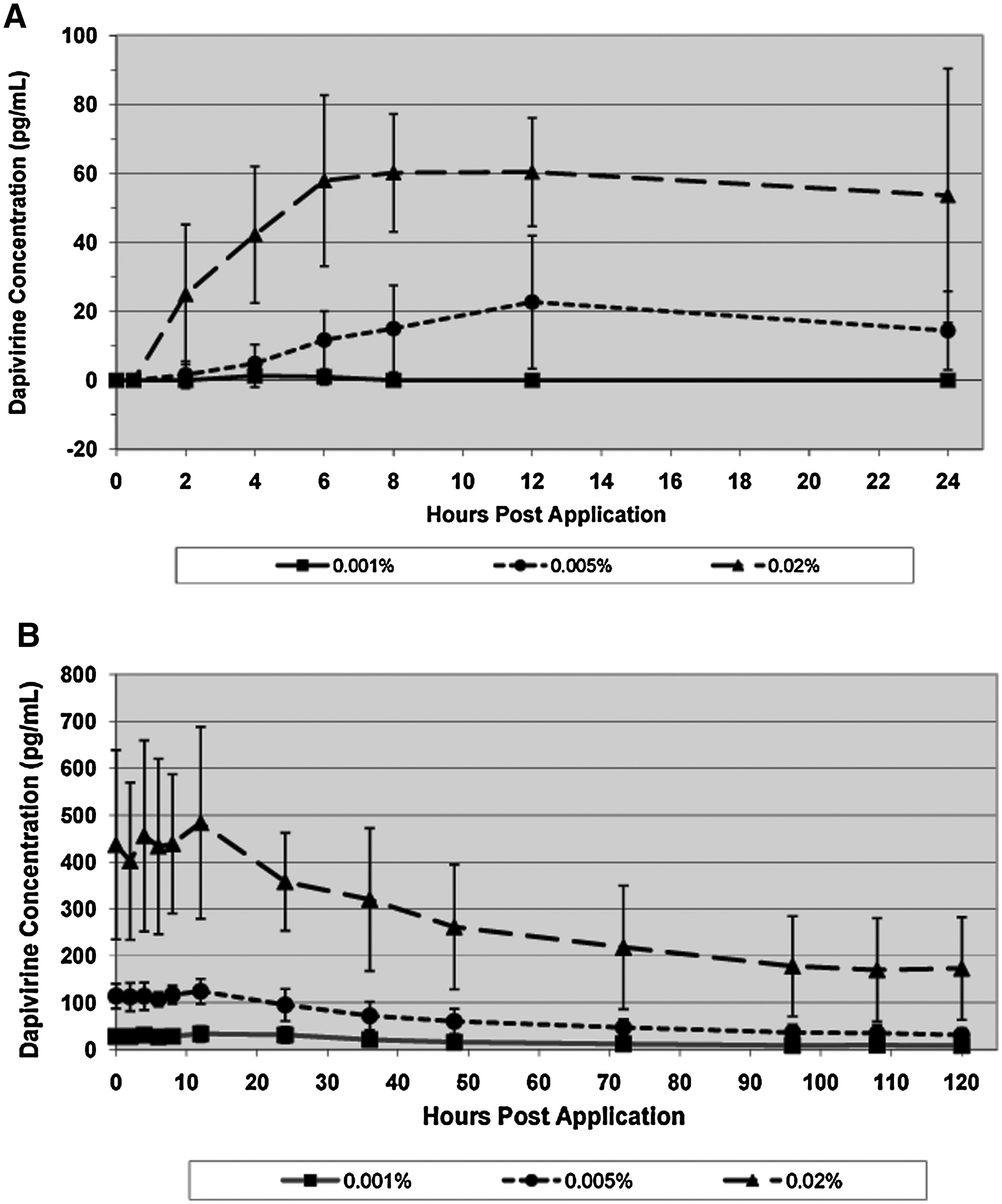
Blood samples were collected sequentially over a 24-h period following administration of study gel on Days 1 and 10, and on Days 11–15. In the 0.001% group on Day 1, all dapivirine concentrations were BLQ and set to zero except for the 4 and 6 h values for one participant (Fig. 1A). After 9 days of dosing, and before administration of the Day-10 dose, mean dapivirine concentration was 27.9 ± 10.3 pg/ml in the 0.001% group (Fig. 1B). Following administration of study gel on Day 10, mean concentration peaked at 12 h (33.7 ± 16.6 pg/ml) and was approximately 50% lower at 48 h (15.7 ± 6.8 pg/mL). Mean concentrations continued to decline throughout the observation period to 25% of the peak value at 120 hr after the Day 10 dose (8.3 ± 4.5 pg/ml).
Dapivirine concentrations in plasma on Day 1 (
In the 0.005% group on Day 1, the mean peak concentration was reached at 12 h post dose (22.7 ± 19.3 pg/ml) then declined to 14.4 ± 11.4 pg/ml at 24 h post dose (Fig. 1A). The mean pre-dose value on Day 10 was 114.2 ± 26.3 pg/ml. Similar to the results obtained in the 0.001% group, the Day 10 mean peak concentration was reached at 12 h post dose (124.4 ± 26.7 pg/ml) and was reduced by approximately 50% at 48 h (60.1 ± 26.6 pg/mlL) (Fig. 1B). Mean concentrations steadily declined during the remainder of the observation period to 31.1 ± 14.8 pg/ml at 120 h after the Day 10 dose (25% of peak value).
In the 0.02% group on Day 1, mean concentrations steadily increased until 6 h post dose (57.9 ± 24.8 pg/ml), were 60 pg/ml at 8 and 12 h, then decreased slightly to 53.6 ± 36.8 pg/ml at 24 h (Fig. 1A). The pre-dose mean value on Day 10 was 437.0 ± 201.8 pg/ml. Similar to the elimination profiles for the other two dose groups, the Day 10 mean peak value was reached at 12 h post dose (483.7 ± 204.6 pg/ml) and mean concentration decreased by approximately 50% at 48 h (261.5 ± 133.0 pg/ml). Mean concentration continued to decline to a value of 173.1 ± 109.8 pg/ml at 120 h after the Day 10 dose (36% of peak value).
Pharmacokinetic parameters for dapivirine in plasma are shown in Table 1. Geometric mean Cmax values in the 0.005% and 0.02% groups were sixfold greater on Day 10 than Day 1 and were reached earlier (tmax 9 h vs. 10–12 h). Linear regression analysis showed good correlation between Cmax and AUC and dapivirine doses on Day 10 indicating possible dose linearity (Table 2). Values for relative volume of distribution were not dose proportional. These results must be considered in the context of the small sample sizes and the high coefficients of variation for the pharmacokinetic parameters.
Venous blood samples were collected for determination of dapivirine concentrations in plasma on Day 1 (before gel application and at 0.5, 2, 4, 6, 8, 12, and 24 h after) and on Day 10 (before gel application and at 2, 4, 6, 8, 12, 24, 36, 48, 72, 96, 108, and 120 h after). Dapivirine concentrations were determined by liquid chromatography with tandem mass spectrometry. All values below the limit of quantitation were substituted with zeroes. Missing pharmacokinetic concentrations were not imputed. Geometric mean ± SD is shown for each parameter except tmax, for which the median is shown. All Day 1 values in the 0.001% dose group were below the limit of quantitation except for the 4 h and 6 h values for one participant. Therefore, pharmacokinetic parameters were not reportable in this dose group on Day 1.
AUC0-last = area under the concentration-time curve (AUC) from time zero to last quantifiable concentration; AUC0-inf = AUC extrapolated to infinity; AUC0-last,ss = AUC0-last at steady state; AUC0-inf,ss = AUC0-inf at steady state; Cmax = maximum concentration; Cmax,ss = Cmax at steady state; NR = not reportable; tmax = time to reach maximum concentration; SD = standard deviation; tmax,ss = tmax at steady state; Vz/F = relative volume of distribution; Vz/F,ss = Vz/F at steady state.
Using pharmacokinetic parameters for individual participants, a least squares linear regression analysis was performed using the formula y = Ax + B, where y represents natural log transformed Cmax, AUC0-last, AUC0-inf, and Vz/F and x represents natural log transformed dose. An estimate of the slope of the regression line and corresponding 95% confidence interval (CI) was obtained. Dose proportionality was concluded if the 95% CI for the slope contained the value 1.
AUC0-last = area under the concentration-time curve (AUC) from time zero to last quantifiable concentration; AUC0-inf = AUC extrapolated to infinity; Cmax = maximum concentration; Vz/F = relative volume of distribution.
Dapivirine concentrations in cervicovaginal fluids
Cervicovaginal fluids were collected on test strips at the introitus, mid-vagina, and cervix at sequential time points on Days 1 and 10. On Day 1, mean dapivirine concentrations at each time point generally increased with dose, ranging from 0.2–83 × 105 pg/ml, and were highest in fluids collected near the cervix (Table 3). High variability was observed among participants, possibly resulting from the collection of different fluid volumes on each test strip. Alternatively, differences in gel application technique among participants could have been a contributing factor.
Cervicovaginal fluid samples were collected at the introitus, mid-vagina, and cervix on test strips on Day 1 at 0.25, 1, 4, and 8 h after gel application. Dapivirine concentrations were determined by liquid chromatography with tandem mass spectrometry. Raw data in ng/strip were converted to pg/ml based on the estimated maximum absorption volume of each test strip of 33 μl. Arithmetic mean ± SD for 6 participants is shown, including values that were below the limit of quantitation and set to zero.
On Day 10, mean dapivirine concentrations at each time point ranged from 0.4–207 × 105 pg/ml across dose groups and were highest at the mid-vagina (Table 4). Mean dapivirine concentrations in CVF remained elevated at 24 h after administration of the last dose on Day 10 (over 1.5 × 105 pg/ml).
Cervicovaginal fluid samples were collected on test strips at the introitus, mid-vagina, and cervix on Day 10 from each participant before gel application and at 4, 12, or 24 h after gel application from 2 participants per time point in each dose group according to a randomization schedule. Dapivirine concentrations were determined by liquid chromatography with tandem mass spectrometry. Raw data in ng/strip were converted to pg/ml based on the estimated maximum absorption volume of each test strip of 33 μl. For pre-dose values, arithmetic mean ± SD for 6 participants is shown except where indicated. For post-dose values, arithmetic mean ± SD for 2 participants is shown; **N = 5.
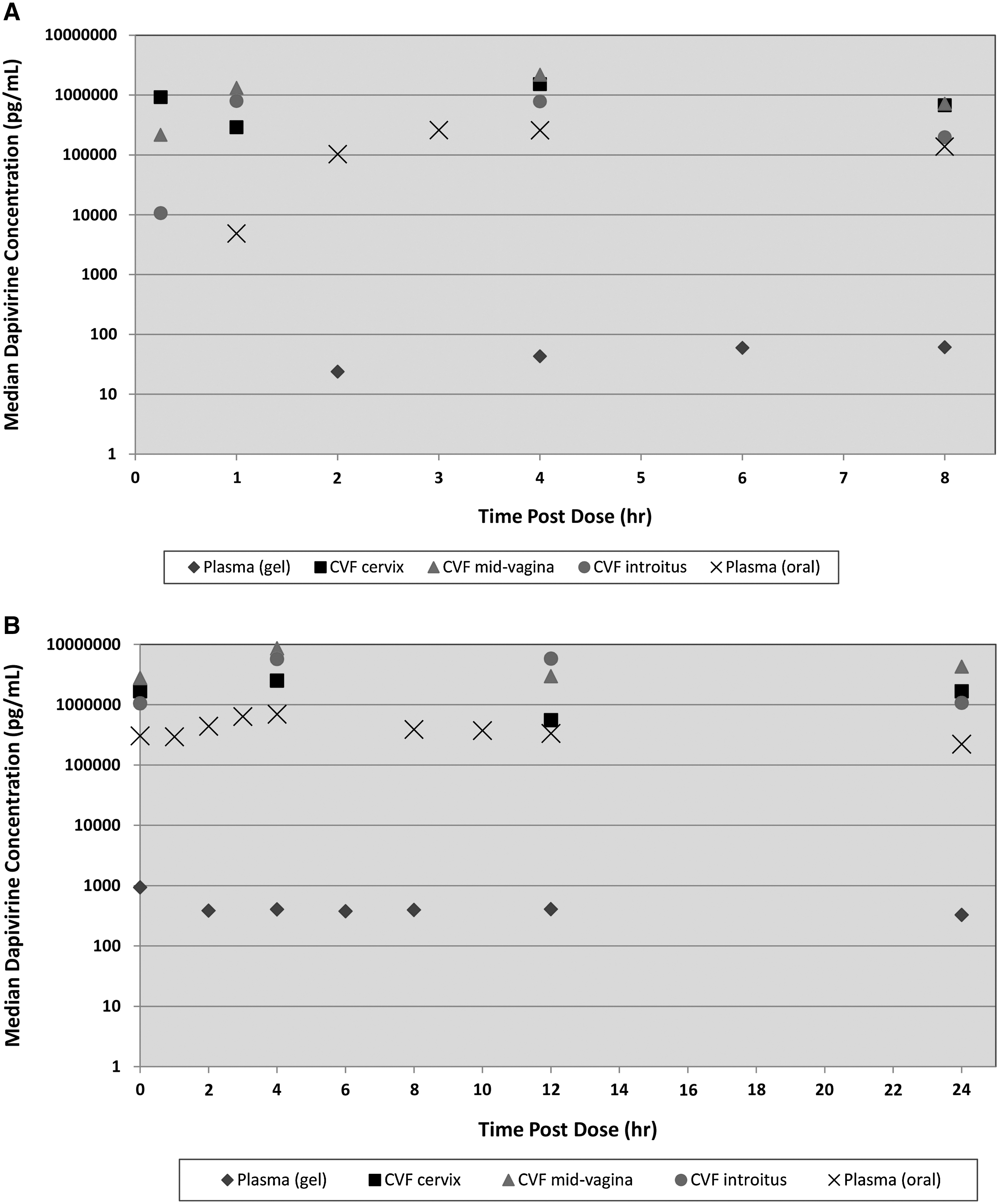
In Fig. 2, dapivirine concentrations in plasma and CVF are compared on Day 1 (Panel A) and Day 10 (Panel B) for the 0.02% dose group. On Day 1, from 1 to 8 h post dose, concentrations in CVF were over 3 logs greater than plasma levels in each dose group. Similarly, from pre-dose to 24 h post dose on Day 10, concentrations in CVF were 3 logs greater than plasma levels. Except for the 1 h time point on Day 1, dapivirine concentrations in CVF were 1–1.5 logs greater than plasma concentrations following 14 days of oral dosing with dapivirine at the therapeutic dose (100 mg BID), shown as exes in both figures. 19
Comparison of dapivirine concentrations in plasma and cervico-vaginal fluid (CVF) on Day 1 (
Dapivirine concentrations in cervicovaginal tissues
Three cervicovaginal tissue samples (vagina near vulva, vagina near cervix, and cervix) were collected from each participant at 4, 12, or 24 h post dose on Day 10 according to a randomization schedule (two participants per time point in each dose group). Absorption of dapivirine was noted in all sampled regions in all dose groups at each time point. The range in values for individual participants across sampling sites and time points was 1.0–43.0 × 103 pg/mg in the 0.001% group, 1.0–190 × 103 pg/mg in the 0.005% group, and 4.3–356 × 103 pg/mg in the 0.02% group. Mean values ± SD at each sampling site are shown in Fig. 3 for participants in the 0.02% dose group.
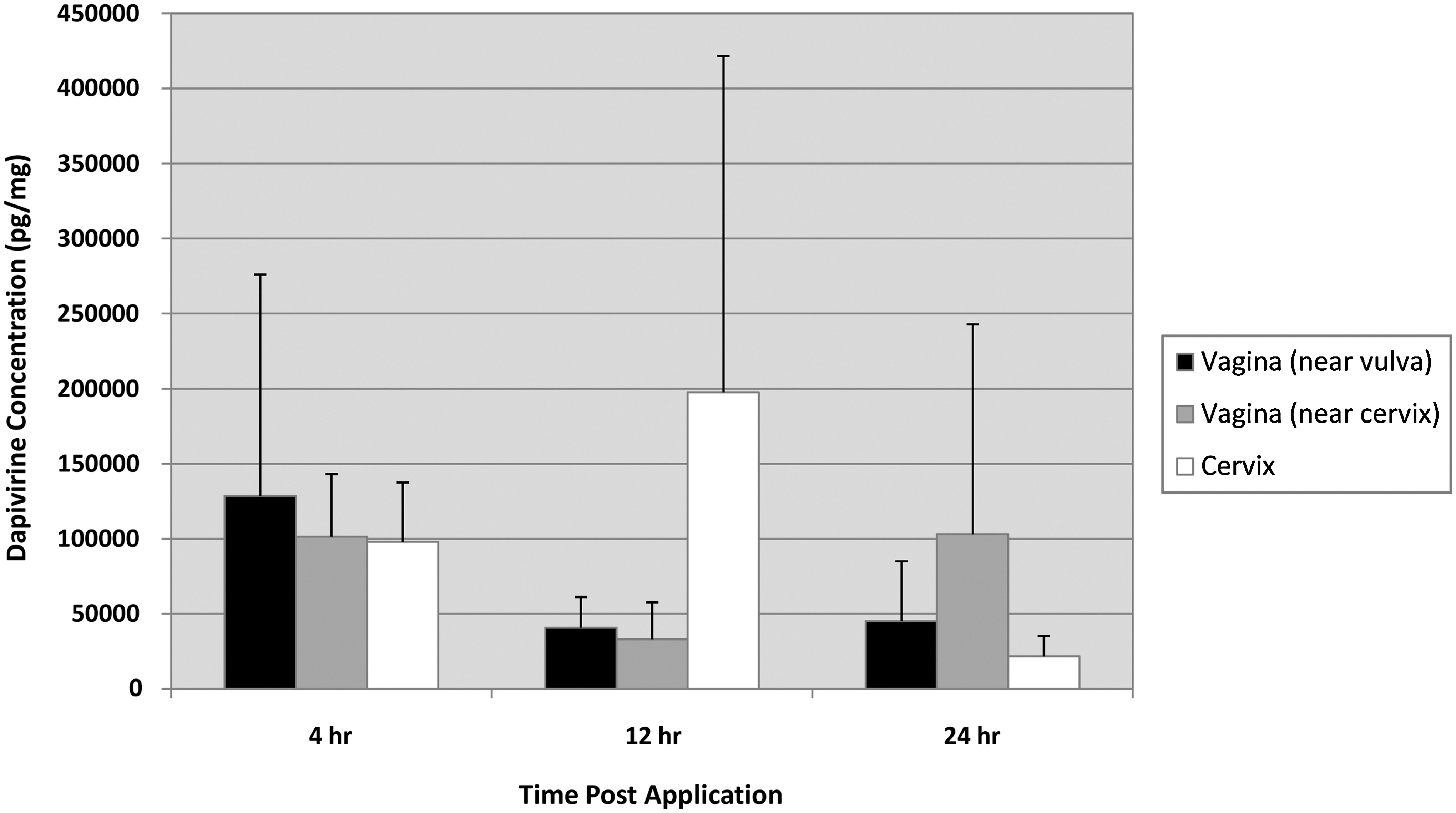
Dapivirine concentrations in cervicovaginal tissues on Day 10 in the 0.02% dose group. Tissue biopsies from the vagina (near vulva, near cervix) and cervix were obtained from each participant under propofol anesthesia at 4, 12, or 24 h post gel administration on Day 10 (2 participants per time point in each dose group) according to a randomization schedule. Dapivirine concentrations in tissues were determined by liquid chromatography with tandem mass spectrometry. Each bar represents the arithmetic mean ± SD for 2 participants.
Discussion
Administration of dapivirine vaginal microbicide gel to healthy, HIV-negative adult women for 10 days at doses of 0.001%, 0.005%, or 0.02% resulted in wide distribution of dapivirine in the lower genital tract with low systemic absorption and minimal side effects.
Blood in urine (67%–83%) and nitrites in urine (17%–50%) were the most common TEAEs. These events could have resulted from a number of causes, including improper collection and handling of urine samples, collection of tissue biopsies, menses or intermenstrual spotting, or trauma associated with application of the study gel.
Urinalysis was not performed in previously published studies with similar dapivirine gels; 4 however, in a recent study with two new dapivirine gel formulations, 18 blood in urine was noted for 14/24 (58%) dapivirine gel users and 8/12 (67%) universal placebo gel users. For 5/14 (36%) dapivirine gel users and 4/8 (50%) placebo users with the event, the observation corresponded with the time of cervicovaginal tissue biopsy, as reported here. Nitrites were not detected in urine specimens.
Low systemic absorption is a desirable characteristic for an antiretroviral drug (ARV)-based vaginal microbicide gel because of the potential for selection of resistant virus in women who seroconvert unknowingly while using the gel. In this study, geometric mean Cmax values in plasma after 10 days of dapivirine gel use were 31, 130, and 471 pg/ml in the 0.001%, 0.005%, and 0.02% groups, respectively. These values are over 3 logs lower than the mean Cmax value in plasma after 14 days of oral dapivirine at 100 mg BID (6.6 × 105 pg/ml). 19
Some systemic absorption of tenofovir, an NRTI in development as a microbicide, was reported following 14-day administration of 0.3% or 1.0% vaginal microbicide gel. Tenofovir was detected in the sera of 56% of tested women with maximum concentrations in the range of 3.0–25.8 ng/ml. 20 Median Cmax values of 4.0 and 3.4 ng/ml were reported following single or multiple doses, respectively, of 1% tenofovir gel. 21 Although these levels are higher than what was reported here with dapivirine, a direct comparison is not meaningful because tenofovir and dapivirine have very different physical and chemical properties and different mechanisms of action.
Since the evolution and transmission of drug-resistant virus has important public health implications for ARV therapy, 22 and because the lower threshold for systemic concentrations of ARVs resulting in drug resistance is unknown, further study of the potential impact of ARV-based microbicides on HIV drug resistance is warranted. 23 We intend to investigate the potential emergence of drug-resistant virus in appropriately designed future clinical trials with ARV-based microbicides. IPM004 is the first study to report drug levels in CVF and cervicovaginal tissues following administration of an NNRTI-based vaginal microbicide gel. Dapivirine was detected in the CVF of each participant on Day 1 and Day 10, and in cervicovaginal tissue samples collected from each participant on Day 10.
The local concentration of dapivirine needed to protect women against HIV infection is unknown. However, on Day 10 pre-dose, all participants had dapivirine concentrations in CVF at least twofold greater than the inhibitory concentrations reported in in vitro studies (0.3–2.0 × 103 pg/ml). 15 Ranges in individual values across sampling sites were 8.4–2010 × 103 pg/ml in the 0.001% group, 4.4–19968 × 103 pg/ml in the 0.005% group, and 397 to >26937 × 103 pg/ml in the 0.02% group. Three of 6 (50%) participants in the 0.001% group, 5 of 6 (83%) in the 0.005% group, and 6 of 6 (100%) in the 0.02% group had CVF concentrations on Day 10 pre-dose that were greater than individual plasma concentrations after 14 days of oral dosing at the therapeutic dose (100 mg BID), which ranged from 240–388 × 103 pg/ml. 19
On Day 10, dapivirine concentrations in cervicovaginal tissue biopsies increased with gel dose and were in the range of 1.3–356 × 103 pg/mg for individual participants. The IC50 for dapivirine in a human ectocervical explants model was 66 pg/ml. 15
Maintaining high local levels of dapivirine is desirable for protection against HIV transmission because genital mucosa is the presumed site of infection. 24,25 Dapivirine levels in CVF and cervicovaginal tissues remained elevated at 24 h post dose, suggesting that once-daily dosing may be a viable option for microbicide gels. Dapivirine concentrations in CVF and cervicovaginal tissues are being evaluated in more detail in ongoing clinical trials with dapivirine vaginal gels and rings.
In conclusion, dapivirine gel at concentrations of 0.001%, 0.005%, and 0.02% was safe and distributed throughout the lower genital tract with low systemic absorption when administered for 10 days. Pharmacodynamic data and drug concentrations in CVF and cervicovaginal tissues following vaginal gel use are important for the future evaluation of ARV-based microbicides.
Footnotes
Acknowledgments
Z. Rosenberg and P. Coplan designed the study. The principal investigator (M. Ferreira) and co-investigators (F. Burger, A. Coetzee, P. Jordan, N. Mbenenge, A. Mostert, J. Potgieter, J. Terblanché, A. van der Bijl, H. Cronjé, and T. Khoale) of the University of the Free State, Bloemfontein, South Africa, oversaw the study at the research center. S. Smythe was responsible for study supervision, site coordination, and study monitoring. The integrity of the data and accuracy of the data analyses were monitored by S. Smythe and A. Nel. Data interpretation was supported by A. Nel and J. Romano. All authors critically reviewed the manuscript. We are grateful to the study team at the Campus of the University of the Free State in Bloemfontein, to ABL and FARMOVS-PAREXEL for bioanalysis and pharmacokinetic analyses, and to the CROs (Triclinium and Quintiles) for study monitoring, statistical analyses, data management, and report writing. Tibotec Pharmaceuticals has provided a royalty-free license to IPM to develop, manufacture, and distribute TMC120 (dapivirine) as a microbicide in resource poor countries. This study was funded by the International Partnership for Microbicides, Silver Spring, Maryland.
Author Disclosure Statement
No competing financial interests exist for any of the authors.