
Abstract
Liver disease in patients with chronic hepatitis C virus (HCV) infection has an accelerated course in the presence of human immunodeficiency virus (HIV) coinfection. Some data suggest that HIV suppression achieved with highly active antiretroviral therapy (HAART) ameliorates HCV-related liver disease progression. The aim of this study was to test if there is overexpression of serum markers of liver inflammation and fibrosis in HIV-HCV-coinfected patients and if the effect is counteracted by HAART. In a pilot, cross-sectional, and comparative study serum markers of liver inflammation (CK-18 and HGF) and fibrosis (HGF, MMP-2, and TIMP-1) were measured via ELISA in HIV-infected patients off and on HAART, HCV monoinfected, HIV-HCV coinfected off and on HAART, and controls (10 per group). HIV-HCV-coinfected off HAART patients with low CD4 counts had higher levels of M30, HGF, and MMP-2 than HIV-HCV-coinfected on HAART. HCV coinfection predicted higher levels of MMP-2 [B 65.82 (95% CI 3.86–127.78); p = 0.04], HGF [B 520.22 (95% CI 123.65–916.78); p = 0.01] and M30 [B 128.02 (95%CI 16.39–239.64); p = 0.03]. HAART use was a predictor of lower levels of MMP2 [B −83.18 (95%CI (−146.8) – (−19.52)); p = 0.01] and M30 [B −112.9 (95% CI (−221.3) – (−4.52)); p = 0.04]. Other factors analyzed including alcohol intake ware not associated with the studied markers. In conclusion, serum markers of hepatic inflammation and fibrosis are overexpressed in HIV-HCV-coinfected patients with advanced immunosuppression, while HAART has a “protective” effect.
Introduction
L
Several serologic markers have been proposed as noninvasive methods to assess liver inflammation and fibrosis. Activation of caspases is up-regulated in HCV-infected liver and correlates with the grade of inflammatory activity. 5,6 Caspase activation can be detected in serum from HCV-infected patients using an ELISA that selectively recognizes a caspase-generated neoepitope of cytokeratin-18 (CK-18), M30, abundantly expressed in hepatocytes. It is associated with liver fibrotic changes, even in patients with normal aminotransferase levels. 7 Liver extracellular matrix is remodeled by the proteolytic enzymes [matrix metalloproteinases (MMPs)] and their specific inhibitors [tissue inhibitors of matrix metalloproteinases (TIMPs)]. Serum MMPs and TIMPs correlate with the development of cirrhosis in HCV-infected patients. 8 –12 In particular, TIMP-1 levels correlate with fibrosis, and MMP-2 with the degree of periportal necrosis and of fibrosis and total histological activity index score. 8,12 MMPs–TIMPs imbalance might lead to excessive matrix apposition and more liver fibrosis. 13
Serum TIMP-1 (but not MMP-1, MMP-2, TIMP-1/MMP-1, and TIMP-1/MMP-2) correlated with liver fibrosis in a cohort of HIV-HCV-coinfected patients. 14 A small study showed higher TIMP-1 levels in HIV-HCV-coinfected patients compared to HIV-monoinfected patients, with no differences in MMP-9 levels. 15 The same study revealed higher TIMP-1 levels in HIV-monoinfected than in healthy volunteers. The gelatinase MMP-2 is also dysregulated in HIV infection. 13 Finally, a correlation has been observed between inflammatory activity and fibrosis in the liver tissue and serum concentration of hepatocyte growth factor (HGF). 16 We hypothesize that the aforementioned markers of liver inflammation/fibrosis are overexpressed in HIV-HCV-coinfected patients compared to those with HCV but not HIV infection.
Retrospective studies suggest that HIV suppression and preservation of CD4 counts using highly active antiretroviral therapy (HAART) slow the progression of hepatic fibrosis and improve survival. 17 –19 A more recent meta-analysis, however, failed to conclusively demonstrate the benefits of HAART for HCV-related adverse outcomes. 20 Brief follow-up and other limitations make these results difficult to interpret. We hypothesize that the immunologic benefit conferred by the suppression of HIV replication using HAART may reverse, at least partially, the overexpression of liver inflammatory/fibrosis markers. The objective of this study was to determine the effect of HIV and of HAART use on markers of hepatic inflammation/fibrosis in the setting of HCV coinfection.
Materials and Methods
Study outline
This is a pilot, cross-sectional study, performed at Wake Forest University Baptist Medical Center in Winston-Salem, North Carolina. Approval was obtained from the Institutional Review Board of our center prior to the performance of the study. Participants provided written informed consent. All procedures followed were in accordance with the Institutional Review Board and with the Helsinki Declaration of 1975, as revised in 2000. Samples were obtained from patients attending the HIV-Infectious Diseases and Hepatitis clinics at our institution. Fifty subjects belonging to five groups (10 patients in each group) were selected: HIV-infected patients off HAART (HIVoff), HIV-infected patients on HAART (HIVon), HCV-monoinfected patients (HCV), HIV-HCV-coinfected off HAART patients (HIVHCVoff), and HIV-HCV-coinfected on HAART patients (HIVHCVon). Samples from 10 healthy volunteers (HVo) were obtained as controls. Serum levels of parameters associated with liver inflammation in HCV infection (M30 and HGF) and fibrosis (MMP-2 and TIMP-1) were measured via ELISA.
Subject selection
Inclusion criteria were age above 18 years old, with available blood sample in storage or able to provide a blood sample. For the HCV-infected groups, patients were required to have active HCV replication (detectable HCV RNA in serum). For the HIV-infected patients they have to meet criteria for one of the following categories: well-controlled HIV infection (undetectable serum HIV RNA) while on HAART for at least 6 months or uncontrolled HIV infection (detectable serum HIV RNA and no HAART over the past 6 months). HAART was defined as a combination of at least three antiretroviral drugs. Exclusion criteria were hepatitis B virus (HBV) coinfection, active opportunistic infection (other than oral candidiasis) or tumor, cirrhosis stages B-C of Child–Pugh, end-stage renal disease, and hemophilia. We included the three non-HCV groups as controls (healthy volunteers, HAART-untreated and HAART-treated HIV-infected subjects) to ensure that changes in serum markers actually reflect HCV-related liver processes.
Clinical variables collected
Clinical data collected include gender, age, risk factors for HCV-HIV infection, duration of HIV infection, use/duration of antiretroviral treatment (HAART), absolute current and nadir CD4 lymphocyte counts, alanine aminotransferase (ALT), aspartate aminotransferase (AST), HIV RNA and HCV RNA levels, HCV genotype, and alcohol use.
Outcome measures
Primary outcome measure were differences in serum HGF, MMP-2, TIMP-1, and M30 levels between groups. Secondary outcome measures include correlations between the serum markers and CD4 counts.
Measurement of serum markers of liver inflammation/fibrosis
The inflammatory/fibrosis markers were measured using commercially available ELISAs. Samples were in storage at −80°C in aliquots. One aliquot of serum from each patient was unfrozen for each of the measurements. Each ELISA was run at the same time for all patients. For MMP-2 Quantikine Human/Mouse/Rat MMP-2 Immunoassay (R&D Systems, Minneapolis, MN) was used. This is a 4.5-h solid phase ELISA designed to measure total MMP-2 (pro- and active MMP-2). It contains CHO cell-expressed, recombinant human pro-MMP-2 and antibodies raised against the recombinant factor. The assay employs the quantitative sandwich enzyme immunoassay technique. The serum samples were diluted 10-fold, as recommended by the manufacturer. M30-Apoptense ELISA (PEVIVA AB, Bromma, Sweden) was used to measure caspase activation. It is a solid phase sandwich enzyme immunoassay designed for the quantitative determination of the apoptosis-associated CK18Asp396 (M30) neoepitope in serum. Quantikine Human HGF (R&D Systems, Minneapolis, MN) was used for HGF determinations. It is a 4.25–4.5 h solid phase ELISA. It contains Sf 21-expressed recombinant human pro-HGF and antibodies raised against the recombinant factor. The assay employs the quantitative sandwich enzyme immunoassay technique. Quantikine Human TIMP-1 Immunoassay (R&D Systems, Minneapolis, MN) was used for TIMP-1 measurement. It is a 3.5-h solid phase ELISA. It contains NS0-expressed recombinant human TIMP-1 and antibodies raised against the recombinant factor. The assay employs the quantitative sandwich enzyme immunoassay technique.
Validation of serum parameters as markers of liver inflammation/fibrosis
Correlation tests between the METAVIR histological scores of inflammation and fibrosis and the four selected serum markers were performed in 10 out of the 30 HCV-infected patients who had available liver biopsy (five HCV-monoinfected and five HIV-HCV-coinfected patients). To better validate the serum parameters used as markers of liver inflammation/fibrosis we also analyzed a separate group of HCV-HIV-coinfected subjects. Thus, additional HGF, MMP-2, and M30 ELISAS were run in eight additional HCV-HIV-coinfected subjects with available serum and liver biopsy.
Statistical analyses
Data were reported as percentages for categorical variables and as median and range for continuous variables. Comparisons were made between groups (globally and stratified by CD4 counts <350 and >350 cells/mm3) using nonparametric tests. Correlations were assessed using the Pearson test. Factors predicting levels of liver inflammation and fibrosis were assessed using univariate and multivariate lineal regression analyses. p values <0.05 were considered statistically significant. All analyses were performed using SPSS (version 13.0, SPSS Inc., Chicago, IL).
Results
Subjects' characteristics are displayed in Table 1. HCV-infected patients had higher transaminase levels and were more often ex-intravenous drug users compared to those only infected by HIV. HIV-HCV-coinfected subjects were older and more often African-American compared to the remaining groups. HIV-HCV-coinfected patients off HAART more often admitted to drinking alcohol.
Mean (range).
p = 0.009.
p = 0.05.
p = 0.03.
p = 0.03.
p < 0.0001.
p = 0.001.
There was a positive correlation between the METAVIR fibrosis score and the levels of M30 (r = 0.7; p = 0.02), HGF (r = 0.8; p = 0.003), and TIMP-1 (r = 0.7; p = 0.02). TIMP-1 levels also correlated with the histological inflammation score (r = 0.7; p = 0.03). In the external validation group consisting of eight HCV-HIV-coinfected subjects with available serum and liver biopsy a correlation was found only between the METAVIR fibrosis score and the levels of M30 (r = 0.8; p = 0.02).
Serum M30 levels tended to be higher in HIV-HCV-coinfected subjects not receiving HAART compared to HCV-monoinfected patients, and significantly higher compared to HIV-HCV-coinfected subjects treated with HAART (p = 0.02) (Fig. 1A). There was no correlation between M30 levels and CD4 counts.
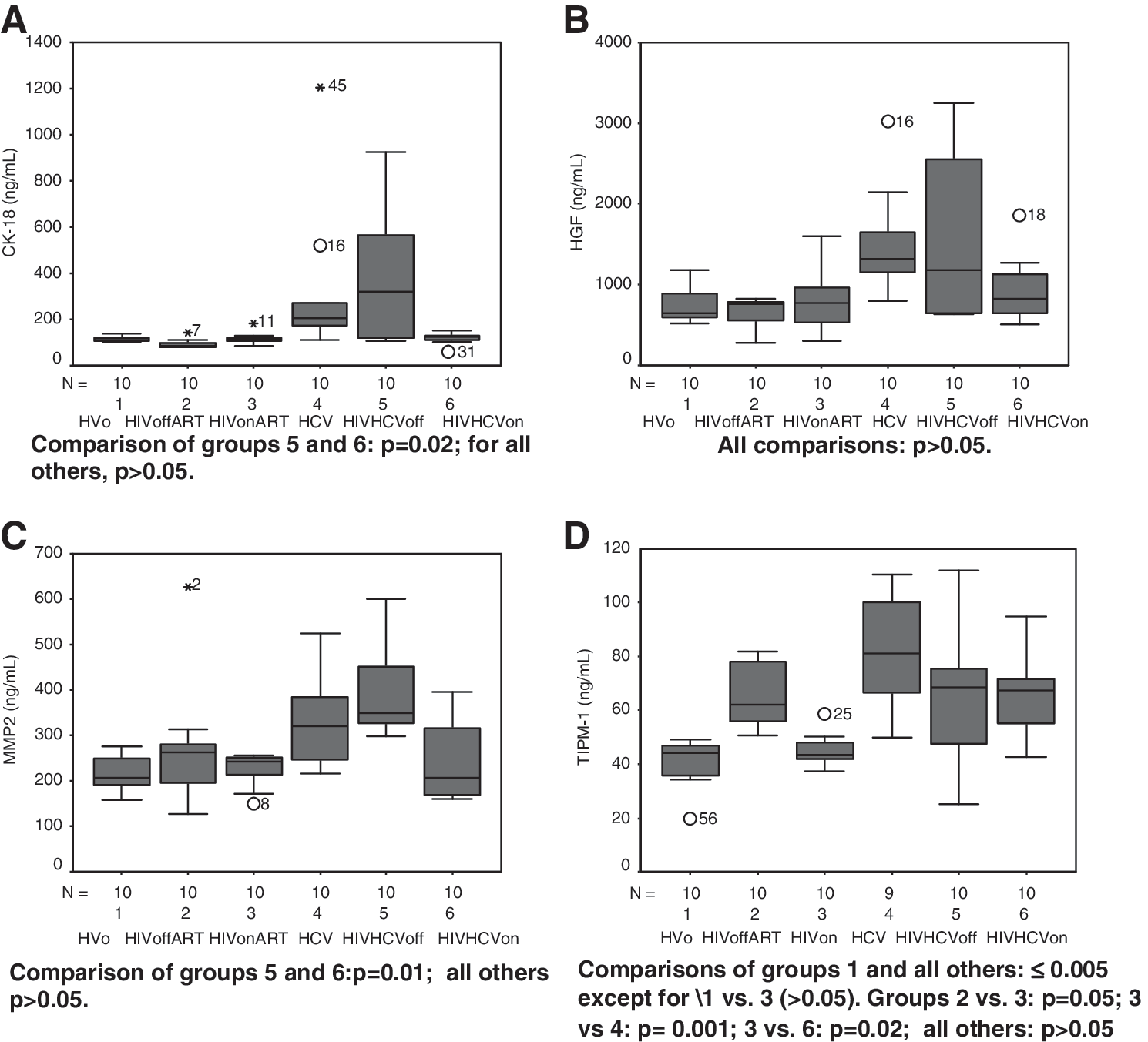
HGF levels tended to be lower among HAART-treated compared to untreated HIV-HCV-coinfected subjects. (Fig. 1B). There was a large dispersion of values among the HCV and the HAART untreated HIV-HCV groups. There were no statistical differences between the three groups with HCV infection despite the apparent disparities in the box-plots. There was a correlation between HGF and M30 levels (r = 0.6; p < 0.0001). Interestingly, there was also a negative correlation between HGF levels and CD4 counts among HIV-HCV-coinfected subjects (r = −0.6; p = 0.008). When analyzed using CD4 counts as a dichotomous variable, those with a CD4 count >350 cells/mm3 had lower HGF mean levels (900.35 ng/ml) than those with CD4 counts <350 cells/mm3 (2238.71 ng/ml) (p = 0.04).
Serum matrix metalloproteinase-2 (MMP-2) tended to be overexpressed among HIV-HCV-coinfected compared to HCV-monoinfected subjects (Fig. 1C). There were statistically significant differences between HIV-HCV-coinfected patients on HAART and off HAART (p = 0.01). We found correlations between MMP-2 and HGF (r = 0.5; p < 0.0001) and between MMP-2 and M30 levels (r = 0.4; p < 0.0001). There was no correlation between MMP-2 and CD4 counts.
TIMP-1 was elevated in HIV-infected patients compared to healthy volunteers (as previously reported), but only in untreated subjects (p = 0.008). However, TIMP-1 levels among HAART-untreated HIV-HCV-coinfected patients did not differ from levels among HAART-untreated HIV- or HCV-monoinfected subjects (Fig. 1D). TIMP-1 levels varied among HAART-treated patients, with higher levels in HIV-HCV-coinfected than in HIV-monoinfected subjects (p = 0.02). We found no correlation between TIMP-1 levels and CD4 counts. The TIMP-1 values obtained were in lower ranges than previously reported, and therefore TIMP-1/MMP-2 ratios were not calculated or analyzed. There were correlations between TIMP-1 levels and MMP-2 (r = 0.5; p < 0.0001), HGF (r = 0.5; p < 0.0001), and M30 (r = 0.3; p = 0.02).
Since alcohol is known to increase the levels of serum inflammatory and fibrotic markers additional tests were performed and no association was found with the parameters studied. Other factors analyzed include age, sex, race, and HIV RNA, current and nadir CD4 count, all of them also with negative results (data no shown).
Subanalyses of more immunosuppressed subjects not on HAART
We performed a subanalysis selecting more immunosuppressed HIV-HCV-coinfected subjects off HAART to assess the role of declining immune function on markers of liver inflammation and fibrosis. HIV-HCV-coinfected subjects off HAART and with CD4 <350 cells/mm3 were selected (N = 5), and comparisons with HCV-only and HAART-treated HIV-HCV-coinfected subjects were made (Table 2). We found that coinfected subjects with a CD4 <350 cells/mm3 and not on HAART had significantly higher levels of M30, HGF, and MMP-2 when compared to coinfected subjects on HAART. Mean levels of these markers were also higher compared to HCV-monoinfected subjects, but the differences did not reach statistical significance.
Off HAART HIV-HCV with <350 cells/mm3 versus HCV monoinfected subjects.
Off HAART HIV-HCV with <350 cells/mm3 versus HIV-HCV coinfected subjects on HAART.
Subanalyses of HIV-infected patients: factors predicting levels of liver inflammation and fibrosis markers
Given that the main differences in serum markers were observed between HIV-HCV-coinfected subjects off and on HAART we performed additional analyses and studied the role of other possible factors determining the levels of inflammation/fibrosis markers among the 40 HIV-infected patients. In particular, we were interested in the effect of HCV infection, HAART, immune status, and alcohol use. Table 3 shows the results of univariate and multivariate linear regression analyses. In multivariate analyses, HCV coinfection was an independent predictor of higher levels of MMP-2 [B 65.82 (95% CI 3.86–127.78); p = 0.04], HGF [B 520.22 (95% CI 123.65–916.78); p = 0.01], and M30 [B 128.02 (95% CI 16.39–239.64); p = 0.03], while HAART use was a predictor of lower levels of MMP2 [B −83.18 (95% CI (−146.8) – (−19.52)); p = 0.01] and M30 [B −112.9 (95% CI (−221.3) – (−4.52)); p = 0.04]. Age, sex, race, alcohol use, HIV load, and nadir and current CD4 counts were other factors analyzed and found not to be associated with levels of the studied markers.
Univariate and multivariate linear regression analyses.
Discussion
Epidemiological studies have shown that HCV-HIV-coinfected patients develop cirrhosis earlier than those with only HCV infection due to an accelerated progression of liver fibrosis presumably due to immune depression. 3,4 For the present study, we selected serum markers that have been shown to correlate with liver inflammation in HCV-monoinfected subjects. 5 –12 In our own analyses, even with a small number of patients M30 was consistently associated with METAVIR fibrosis scores in HIV-HCV-coinfected patients as well. We then searched for the impact of HIV-induced immune deficiency as well as of its reversion by HAART on the dynamic process of HCV-related liver fibrosis. Our data indicate that HGF, M30, and MMP-2 are overexpressed among individuals with HCV infection compared to those with just HIV infection suggesting that they reflect the processes of inflammation and fibrosis occurring in the liver of HCV-infected patients, even in the presence of HIV coinfection.
M30 is a type of protein cytokeratin 18 (CK-18) fragment released during apoptosis of epithelial cells by the action of caspases. M30 is abundantly expressed in hepatocytes, and the levels increase in processes of inflammation such as HCV infection. 6 –8 Serological detection of caspase activation has been associated with accelerated liver fibrosis on biopsy. 5 –7 We observed that caspase activation as measured in serum by the caspase-generated neoepitope cytokeratin-18 M30 tended to be higher among immune-depressed HIV-infected subjects, suggesting increased inflammation and an accelerated fibrosis process compared to HCV. To our knowledge, this is the first report of increased caspase activation in the setting of HIV-HCV coinfection.
MMP-2 and HGF, other serum markers of liver inflammation-fibrosis measured, were not significantly higher in HIV-coinfected subjects, which might be explained by the small sample and great dispersion of values. MMP-2, also named gelatinase A, is expressed in mesenchymal cells (mainly fibroblasts) during tissue regeneration. It degrades several types of collagens, elastin, and fibronectin. It therefore participates in the development of fibrosis in the liver in patients with HCV hepatitis. 9,10,12 HGF is a growth factor with marked and varied effects on hepatocytes and other epithelial cells, being elevated in the serum of individuals with a variety of liver disorders including chronic hepatitis C. 16 To our knowledge, HGF has never been examined in HIV-HCV-coinfected subjects and MMP-2 has been measured only in HAART-treated HIV-HCV-coinfected subjects, but never compared with HCV-monoinfected or HAART-untreated HIV-HCV-coinfected subjects. Additional studies using larger samples are needed to further investigate the effect of HIV immunosuppression on the expression of these markers in HCV-related liver disease.
Contrary to previous studies, we did not find an additional increase in TIMP-1 levels by HCV in HIV-infected subjects. 15 Our results suggest an elevation of TIMP-1 derived from both the HIV and HCV infections, which is reversed by HAART in HIV-monoinfected subjects, but not in those with HIV-HCV coinfection.
The most remarkable finding of our study was the significantly lower expression of markers of liver inflammation and fibrosis among HIV-HCV-coinfected patients with well controlled HIV on treatment compared to those coinfected without HIV treatment, especially the more immunosuppressed. The association is very suggestive and calls for additional studies to prove that control of the HIV replication by effective HAART counteracts the HCV-driven overexpression of the studied markers. The correlation between CD4 counts and HGF and the higher M30 and MMP-2 levels in HAART-untreated, HIV-HCV-coinfected individuals (especially those with CD4 <350 cells/mm3) compared to HIV-HCV-coinfected subjects successfully treated for their HIV infection suggest a correlation between immunosuppression and expression of liver inflammation-fibrosis markers.
Our study has some limitations such as the small size of the sample. Therefore, additional studies with a larger sample and inclusion of patients representing a broader range of ages, CD4 counts, and of other characteristics are needed. We found good correlation between M30 and the fibrosis stage in liver biopsies but with the limited number of patients with available biopsy we cannot draw conclusions regarding the other parameters. Nevertheless, our results are in agreement with previous reports suggesting a negative effect from immunosuppression and a positive effect from HAART, and pave the way for additional research. Studies including liver biopsy would be of great interest to confirm our findings. In addition, longitudinal studies are needed to assess the counteracting role of HAART on HCV-related liver fibrosis in an individual basis.
Our results have several clinical implications. If the control of HIV replication with CD4 restoration can ameliorate the course of HCV-related liver disease, it would strongly suggest that patients with HIV and HCV coinfection would benefit from antiretroviral treatment. In this small study, the benefit was clearer for patients with <350 CD4 cells/mm3. Additional studies are needed to better determine if that holds also true for higher CD4 thresholds. Second, these serologic markers could help to identify patients at higher risk of liver disease progression and intervene early by treating the HCV infection or starting HAART early. Finally, if we can identify which inflammation-fibrosis parameters are overexpressed in the setting of HIV-HCV coinfection, new avenues could be opened to better understand the pathogenic pathways and to develop new therapeutic targets.
In summary, serum markers of hepatic inflammation and fibrosis are overexpressed in HIV-HCV-coinfected patients with advanced immunosuppression, while HAART has a “protective” effect. Our data further support a relationship between HIV-related immunodeficiency and inflammation/fibrosis in HIV-HCV coinfection as well as the use of HAART in this population.
Footnotes
Acknowledgments
The results of these studies were presented at the 60th Annual meeting of the American Association for the Study of Liver Diseases (Boston, October 30–November 3, 2009) and at the 17th Conference on Retroviruses and Opportunistic Infections (San Francisco, February 16–19, 2010).
We thank Dr. Kevin High for his continuous support throughout this work.
Author Disclosure Statement
No competing financial interests exist.