
Abstract
We report here the novel finding that HIV-negative factor (Nef) protein is present in considerable numbers of peripheral blood mononuclear cells (PBMCs) from viremic HIV-infected patients not on antiretroviral therapy (ART) and also in patients receiving virologically suppressive ART, though to a smaller degree. Interestingly, these Nef-positive PBMCs constitute predominantly uninfected bystander cells. These results may explain systemic pathology in HIV patients, even in those receiving ART.
N
Conduit formation between T cells may present a novel route for HIV transmission, while Nef transfer to B cells was shown to impair antibody class switching. 14 It is our hypothesis that if antiretroviral therapy (ART) reduces HIV virion production but not Nef gene expression as previously described, 15 then the persistence of Nef expression might contribute to the higher risk of Nef-induced pathologies in those on ART. 16 We therefore performed a preliminary investigation to assess the detection of Nef-positive circulating cells from both ART-untreated and ART-treated HIV-infected patients.
Peripheral blood mononuclear cells (PBMCs) were isolated from HIV-infected patients and uninfected controls by standard Ficoll purification. Cells were fixed with 4% paraformaldehyde and then permeabilized with 0.01% Triton X-100 prior to staining for Nef using the monoclonal anti-Nef antibody EH1 (NIH AIDS repository),
17
which we have validated to be suitable for FACS analysis of Nef protein. We found an unexpectedly high mean (SD) 9. 6±8.1% number of PBMCs from HIV-infected untreated viremic patients that stained positive for Nef (Table 1 and Supplementary Fig. S1; Supplementary Data are available online at
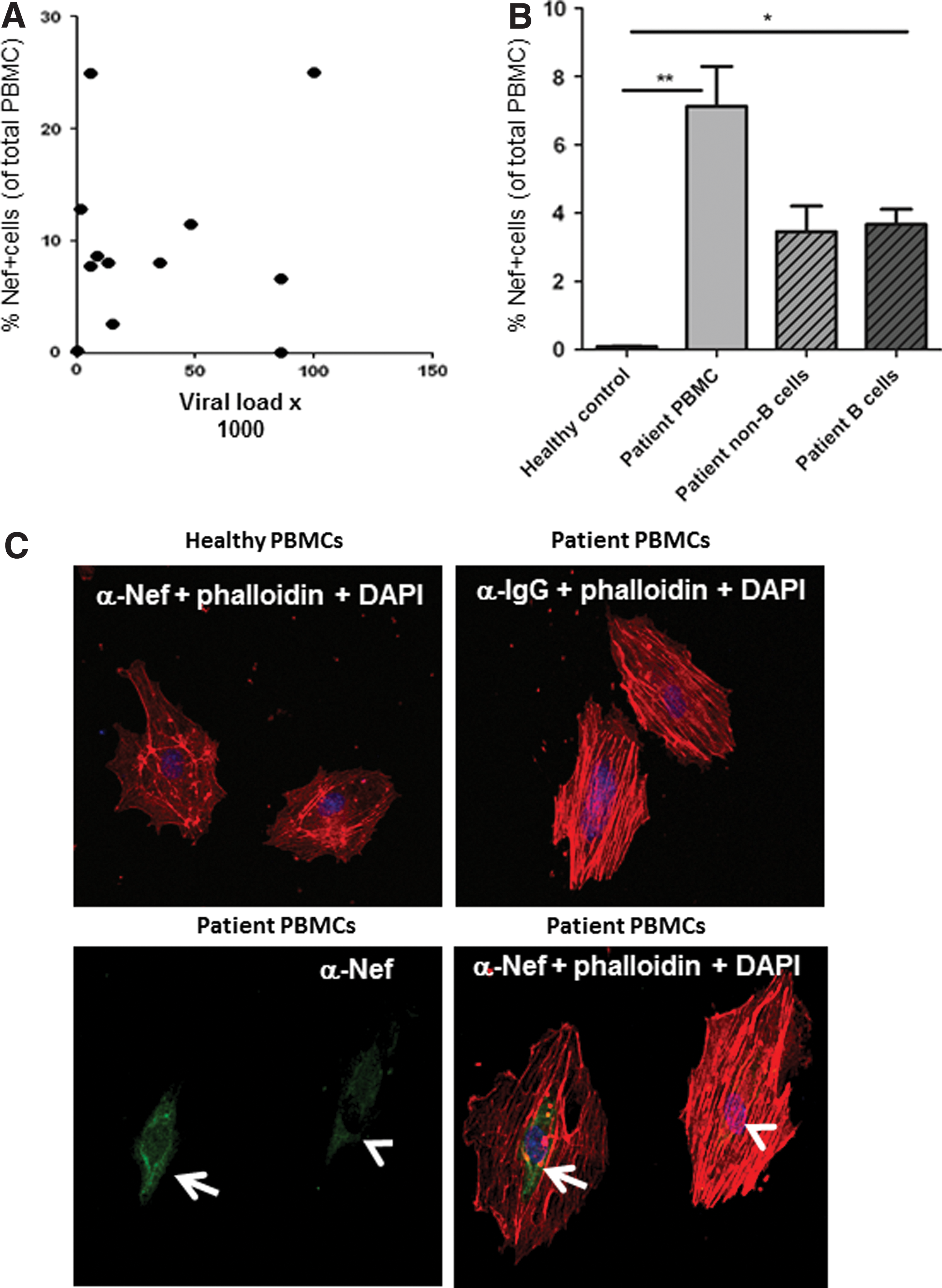
Nef staining does not correlate with viral load, is detectable in B cells and can be transferred to human endothelial cells. (
Percentage of Nef+ peripheral blood mononuclear cells (PBMCs) (stained with Eh1 antibody and analyzed by FACS, see also Supplementary Fig. S1) with clinical parameters in patients without and with antiretroviral therapy (ART) (indicated as ART duration). Patients who had Nef staining confirmed with the Abcam 3D12 antibody are marked with an asterisk (*).
The unexpectedly high levels of Nef-positive PBMCs cannot be explained by direct HIV infection of cells. In fact, Nef antibody staining was significantly more prominent in uninfected HIV-p24-negative cells than in p24-positive cells (Supplementary Fig. S2). Furthermore, the strongest Nef signal was detected in p24-positive cells, which is in line with our hypothesis that Nef protein from infected cells is transferred to bystander cells and thus diluted. Moreover, when we isolated B cells and non-B cells from patient PBMCs using the Miltenyi anti-PE multisort kit and CD19 antibody and stained them for Nef, almost 50% of Nef-positive cells appear to be B cells (Fig. 1B). These data are in line with previous in vitro studies showing that Nef can be transferred from HIV-infected monocytes to B cells. 14
Nef is one of the three immediate early HIV genes, which are still transcribed in HIV-infected cells even in those receiving ART. 15 Interestingly, we also found significant levels of Nef-positive PBMCs [mean (SD), 1.15±0.178%, p=0.001 compared to noninfected controls] in ART-treated patients with HIV RNA viral loads <50 copies/ml (Table 1). This finding could be explained by transfer of Nef from infected cells located in lymphatic tissues, a major HIV reservoir. 18,19 High endothelial venules enable lymphocyte circulation between blood and lymph nodes 20 and are most likely in prolonged direct contact with Nef-containing mononuclear cells. 21 To test if Nef from lymphatic or blood-derived mononuclear cells could also transfer to venous endothelial cells, we cocultured human umbilical cord vein endothelial cells (HUVEC) with PBMCs from viremic untreated HIV-infected patients for 24 h.
As shown in Fig. 1C (left lower panel), this experiment resulted in strongly (arrow) and less strongly (arrowhead) Nef-positive endothelial cells, which is likely due to different levels of Nef transfer. Of note, these endothelial cells are not leukocytes based on characteristic cytoskeletal morphology as determined by staining with phalloidin-Cy5 (Fig. 1C, right lower panel). Together, our findings suggest that Nef protein may be widely transferred from HIV-infected cells to uninfected blood cells and bystander tissue cells, thus providing a means of pathogenic Nef activity even when virus replication is controlled.
In conclusion, the novel findings of this report are the detection of HIV Nef protein in circulating uninfected bystander PBMCs from HIV-infected patients not on ART and the establishment that Nef is still detectable, albeit at significantly lower levels, in patients receiving virologically suppressive ART. Although beyond the scope of this report, it will be necessary to show that these remaining Nef-positive PBMCs exhibit an altered phenotype; if so, these findings might explain why HIV patients are still at increased risk for HIV complications even in the absence of detectable viral loads in the blood. Given that the power of our study was low and the distribution of Nef in PBMCs demands further characterization by FACS including FACS sorting, additional studies need to address whether determining levels of Nef dissemination in PBMCs could potentially be utilized as a predictor for vascular or other HIV-related end organ diseases.
Footnotes
Acknowledgments
This study was supported by the NIH-NHLBI, contract Grants R01 HL095149 (M.C. and S.G.), R01 HL083491 (S.C.F.), T32HL079995 (L.G.), R21 HL120390 (M.C.), and AHA 13PRE14780025 (T.W.). The project described was also supported by the Indiana University Health–Indiana University School of Medicine Strategic Research Initiative and by the Indiana Clinical and Translational Sciences Institute funded in part by Grant TR000006 from the National Institutes of Health, National Center for Advancing Translational Sciences, Clinical and Translational Sciences Award. The following reagent was obtained through the NIH AIDS Reagent Program, Division of AIDS, NIAID, NIH: HIV-1 Nef monoclonal antibody (EH1) from Dr. James Hoxie. Ting Wang and Linden A. Green contributed equally to this article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.