
Abstract
The recent expansion of antiretroviral treatment (ART) coverage in middle/low-income countries has been associated with increasing prevalence of HIV pre-ART drug resistance (PDR). We assessed PDR prevalence, patterns, and trends in Guatemala. Blood samples from 1,084 ART-naive individuals, enrolled from October 2010 to December 2013 at the Roosevelt Hospital in Guatemala City, were obtained. PDR was evaluated using the WHO mutation list for transmitted drug resistance (TDR) surveillance. An overall PDR prevalence of 7.3% (95% CI 5.8–9.0%) was observed for the whole study period. TDR to nonnucleoside reverse transcriptase inhibitors (NNRTI) was the highest (4.9%, p<0.001), followed by nucleoside RT inhibitors (1.8%) and protease inhibitors (1.0%). No significant trends in PDR prevalence were observed during the study period. However, higher NNRTI PDR levels were found in individuals with >500 and 350–500 CD4+ T cells/μl (7.4% and 8.7%, respectively) compared to individuals with <350 CD4+ T cells/μl (3.7%; p=0.039 and p=0.007, respectively), as well as a tendency of higher levels of NNRTI transmitted drug resistance (DR) in individuals with recent infection determined by HIV incidence tests (9.7%), suggesting increasing trends in time. Clusters of viruses with NNRTI PDR suggesting complex transmission networks were observed. No associations between PDR and demographic variables were found. PDR in Guatemala remains at an intermediate level. Nevertheless, we have shown evidence suggesting increasing trends in NNRTI PDR, which need to be taken into account in national HIV management policies.
Introduction
T
More than 58,000 individuals were estimated to live with HIV in Guatemala by the end of 2012, of which approximately 40% were women. 3,4 The epidemic in Guatemala is typically concentrated in high-risk and vulnerable groups with a prevalence of 0.7% in the general population. 3 –8 Seventeen integral care units for individuals living with HIV exist in the country (15 of them in the public sector). Three of these function as national reference centers: The Infectious Diseases Clinic of the Roosevelt Hospital, the Luis Angel García Clinic of the San Juan de Dios General Hospital, and the Infectology Unit of the Social Security System. Clinical follow-up of patients diagnosed with HIV infection is highly centralized in these three centers. 9
Access to ART in Guatemala has existed since the second half of the 1990s through Social Security centers, starting with single and double ARV drug regimens. Ministry of Health centers implemented access to ART since 2001, starting with triple ARV schemes. 10 Universal access to ART was implemented since 2004 with the intervention of the Global Fund. It is estimated that 53% of eligible adults were receiving ART in the country by the end of 2012. 4 Since 2007, Ministry of Health centers use drug combinations based on tenofovir–emtricitabine or zidovudine–lamivudine backbones in combination mainly with efavirenz or nevirapine in most patients starting ART. This situation differs in centers from the Social Security System, where the number of first-line schemes tends to be higher, impacting national statistics on the number of first-line ART regimens available in Guatemala. 10,11 Nearly 90% of patients under ART are reported to be in first-line regimens 11 and the 12-month retention on ART is 82%. 4 This is consistent with high levels of adherence to ART reported at least for urban Ministry of Health centers. 12
Considering this scenario, there is little information on the trends of HIV PDR in the country. In a recent preliminary study, our group found a global PDR prevalence of 8.3% in individuals starting ART in the country for October 2010–March 2011, with most DR cases associated with NNRTIs. 13 This study showed the importance of continuing PDR surveillance in the country to assess HIV DR trends. We present an updated study assessing HIV PDR in Guatemala for October 2010 to December 2013 in a cohort of 1,084 ART-naive individuals with no previous exposure to ART, the largest cohort gathered so far in the country to assess the prevalence of HIV DR, from the Roosevelt Hospital, one of the three national reference centers for HIV care, managing 25% of HIV-infected individuals under ART in the country.
Materials and Methods
Ethics statement
The present study was evaluated and approved by the Ethics Committees of the National Institute of Respiratory Diseases (INER) in Mexico and the Roosevelt Hospital in Guatemala, and was conducted according to the principles of the Declaration of Helsinki. All the participants gave written informed consent before blood sample donation.
Patients
Newly diagnosed and follow-up ART-naive HIV-infected individuals were enrolled from October 2010 to December 2013 at the Infectious Diseases Clinic of the Roosevelt Hospital in Guatemala City in order to assess HIV PDR prevalence and trends in a prospective, observational, cross-sectional study. Inclusion of patients was according to new clinical diagnoses at spontaneous demand to the clinic, also including individuals on follow-up visits, previous to starting ART according to national guidelines. Every eligible person attending the site was offered the opportunity to participate in the study. No exclusion criteria were applied except for known previous exposure to ARV drugs. After giving written, informed consent, participating individuals donated a single peripheral blood sample, collected in EDTA Vacutainer tubes (BD, San Jose, CA) for molecular assays and Cyto-Chex BCT tubes (Streck, Omaha, NE) for flow-cytometry assays. Demographic data were collected through direct application of a questionnaire at the time of sample donation. All blood samples were sent to and processed at the INER in Mexico City, a WHO-designated HIV DR genotyping laboratory, within 48 h of collection. Plasma viral load assays, CD4+ T cell counts, and HIV genotyping and PDR analyses were performed for each patient. Results were sent back to the Roosevelt Hospital for patient clinical follow-up.
HIV plasma viral load and CD4+T cell count estimations
HIV plasma viral load was determined by automated real time polymerase chain reaction (PCR) using the m2000 system (Abbott, Abbott Park, IL). CD4+ T cell counts were obtained by flow cytometry using the Trucount Kit in FACSCanto II instruments (BD Biosciences, San Jose, CA). Both tests are carried out routinely for patient follow-up at the INER.
HIV sequencing
Viral RNA was extracted from 1 ml of plasma (QIAamp Viral RNA Kit; QIAGEN, Valencia, CA). A fragment of the viral pol gene including the whole protease (PR) and 334 codons of the reverse transcriptase (RT) was amplified and bulk-sequenced from plasma HIV RNA using an in-house developed methodology. Briefly, amplification was performed by nested reverse transcriptase (RT)-PCR with primers PR_5′_OUTER 5′-CCCCTAGGAAAAAGGGCTGTTG-3′ (positions 2009–2030 HXB2) and RT_3′_OUTER 5′- GTTTTCAGATTTTTTAAATGGCTCTTG-3′ (3576–3602) for the first round of amplification and PR_5′_INNER 5′-TGAAAGATTGTACTGAGAGACAGG-3′ (2057–2080) and RT_3′_INNER 5′-GGCTCTTGATAAATTTGATATGTCC-3′ (3559–3583) for the second round of amplification. SuperScript III OneStep RT PCR (Invitrogen, Carlsbad, CA) and Platinum Taq DNA polymerase (Invitrogen) were used for the first and second round PCRs, respectively, according to the manufacturer's recommendations, with the following conditions: 50°C for 30 min (first round only); 94°C for 3 min; 35 cycles of 94°C for 30 s, 60°C for 30 s, 72°C for 2 min; and a final extension of 72°C for 5 min. PCR products were purified (QIAquick PCR Purification Kit; QIAGEN), quantified (Nanodrop, Thermo Scientific, Wilmington, DE), and sequenced by capillary electrophoresis using seven sequencing reactions per sample with four forward sequencing primers: POL_A 5′-CCAGAAGAGAGCTTCAGGTCTGGGG-3′ (2164–2288), POL_B 5′-GTTAAACAATGGCCATTGACAGAAG-3′ (2610–2634), POL_C 5′-GGAAAGGATCACCAGCAATATTCCA-3′ (3007–3031), POL_D 5′- CCCTCARATCACTCTTTGGCAACG-3′ (2252–2275), and three reverse sequencing primers: POL_F 5′-CTTTTGGGCCATCCATTCCTGGCTT-3′ (2586–2610), POL_G 5′-CCATCCCTGTGGAAGCACATTGTA-3′ (2985–3008), POL_H 5′-TGCCCCTGCTTCTGTATTTCTGCTA-3′ (3526–3550), using the BigDye Terminator v3.1 chemistry (Life Technologies, Carlsbad, CA). Sequences were obtained with a 3730xl Genetic Analyzer (Life Technologies), assembled, and manually edited using Geneious v6.1 and ViroSeq v2.8. Negative controls were included in all runs and phylogenetic analyses were performed monthly for contamination monitoring.
Genotypic antiretroviral drug resistance testing
Genotypic drug resistance was assessed by the presence of any of the drug resistance mutations included in the list for HIV TDR surveillance defined and periodically updated by the WHO. 14 Additionally, genotypic drug resistance analyses were carried out with the Stanford HIV Drug Resistance Database algorithm (Version 7.0), 15,16 using the HIVdb program available on line. 17,18 In this system, a drug-specific penalty score is assigned for each HIV drug resistance mutation. The total score for each of 19 FDA-approved drugs is then estimated by adding the scores of all mutations associated with resistance to that drug. To define the presence of ARV drug resistance, a total score of 15 or higher to any ARV drug was considered.
HIV subtyping
HIV subtyping was carried out using the sequenced PR-RT segment, with REGA HIV subtyping tool v3.0 (University of Leuven, Netherlands). 19 All recombinants and non-B subtypes were confirmed using the RIP tool, available online at the Los Alamos HIV Database, 20 and with phylogenetic analyses using the Los Alamos HIV Database premade subtype reference alignments, 21 as described below.
HIV incidence tests and determination of recent HIV infection
Incidence tests were carried out in order to estimate TDR in recently infected individuals, following a previously described multiassay algorithm. 22 Briefly, the BED HIV-1 Incidence EIA (Sedia, Portland, OR) was applied to all individuals with CD4+ T cell counts >200 cells/μl and <1 year of HIV diagnosis, according to the manufacturer's instructions. Positive tests (OD <1.0) were confirmed with the HIV-1 Lag-Avidity EIA (Sedia) following the manufacturer's specifications. Individuals with <80% avidity and viral load >400 copies/ml were classified as recent infections.
Phylogenetic analyses
Maximum likelihood trees were constructed using MEGA v6.0. 23 Genetic distances were estimated using the general time reversible+Γ +I model using a partial deletion of gaps/missing data treatment with site coverage of at least 85%, and allowing for ambiguous bases. The Γ parameter was estimated for the data as 0.4064, using five categories and 1,302 positions in the final dataset. Significance was tested with 1,000 bootstrap replications. Reference sequences for different subtypes, available at the Los Alamos HIV Sequence Database, 21 were included.
Statistical analyses
STATA/SE (version 12) was used for statistical analyses. Chi-square tests were used for group comparisons. ANOVA, linear, or logistic regressions were employed for univariate and multivariate analysis according to variable type. Odds ratios (OR) with 95% confidence intervals were estimated to determine effect size for each variable; variables with p values less than 0.05 were used for multivariate adjustment.
Results
We prospectively analyzed PDR in a cohort of 1,084 recently diagnosed and follow-up, ART-naive, HIV-1-infected individuals enrolled at the Infectious Diseases Clinic of the Roosevelt Hospital in Guatemala City, from October 2010 to December 2013. Specimens for 100% of the participants were HIV genotyped. Being a national reference center for HIV care, 44.7% of the patients in the cohort came from departments other than Guatemala City. A characteristic late detection of HIV infection was observed with a median CD4+ T cell count of 180 cells/μl (Table 1). More than half of the participants presented with CD4+ T cell counts lower than 200 cells/μl (581/1084, 53.6%) from which nearly a third presented with less than 50 cells/μl (180/581, 31.0%). A 3:2 male-to-female ratio was observed with a high percentage (84.4%) of participants reporting heterosexual sex as the main risk for HIV acquisition (Table 1). One of each four males (24.8%) identified themselves as men who have sex with men (MSM) in the enrollment questionnaire. Low literacy levels and high unemployment were common (Table 1). HIV pol subtyping revealed that 98.0% (1,062/1,084) of the viruses belonged to clade B, 0.8% (9/1,084) to clade C, 1.0% (11/1,084) were BD recombinant forms, and 0.2% (2/1,084) CRF02_AG.
Pre-antiretroviral treatment drug resistance estimated with the WHO list of mutations for HIV transmitted drug resistance surveillance. 14 PDR, pretreatment drug resistance; SD, standard deviation; AVR, antiretroviral; NNRTI, nonnucleoside reverse transcriptase inhibitors; NRTI, nucleoside reverse transcriptase inhibitors; PI, protease inhibitors; MSM, men who have sex with men; IDU, intravenous drug user.
Using the WHO list of mutations for HIV TDR surveillance, a global HIV PDR prevalence of 7.3% (95% CI 5.8–9.0%) was observed in the complete cohort for the whole study period (Table 2). PDR to NNRTI was the highest (4.9%, 95% CI 3.7–6.4%, p<0.001) followed by nucleoside RT inhibitors (NRTI, 1.8%, 95% CI 1.1–2.8%) and protease inhibitors (PI, 1.0%, 95% CI 0.5–1.8%, Table 2). Using the Stanford HIV DR definition, significantly higher levels of PDR to any ARV drug and to NNRTIs were observed compared to using the WHO list of mutations (p=0.012 and p=0.01, respectively). These differences were more evident in the group of individuals with <350 cells/μl and were mainly due to the presence of polymorphisms at RT position 138, associated with rilpivirine resistance.
Recently infected individuals were defined using a previously described multiassay algorithm including HIV incidence tests, as described in Materials and Methods. 22 CD4+ T cell count for one patient is missing.
Pre-antiretroviral treatment drug resistance (PDR) estimated using the WHO HIV transmitted drug resistance surveillance mutation list. 14
PDR estimated with the Stanford algorithm (v7.0), 15,16 with a threshold of ≥15 for at least one antiretroviral drug of the specified class.
AVR, antiretroviral; NNRTI, nonnucleoside reverse transcriptase inhibitors; NRTI, nucleoside reverse transcriptase inhibitors; PI, protease inhibitors.
Nevertheless, DR levels were maintained along the study period when analyzing by year of enrollment with only a slight increase observed for NRTI TDR (p=0.0072; Fig. 1A). Four cases (0.4%) of PDR to two ARV drug families were observed and no cases of PDR to the three ARV drug families were found. No significant variations in time were observed in PDR throughout the study period associated with demographic variables including gender, risk factor for HIV infection, CD4+ T cell count, residence, literacy, marital status, or employment (Fig. 1B–H). PDR cases were observed mainly in Guatemala City, central departments around Guatemala City, and eastern departments bordering El Salvador, namely Alta Verapaz, Quiché, Totonicapan, Sololá, Chimaltenango, Sacatepéquez, Escuintla, Santa Rosa, Jutiapa, Chiquimula, and Zacapa (Fig. 2).
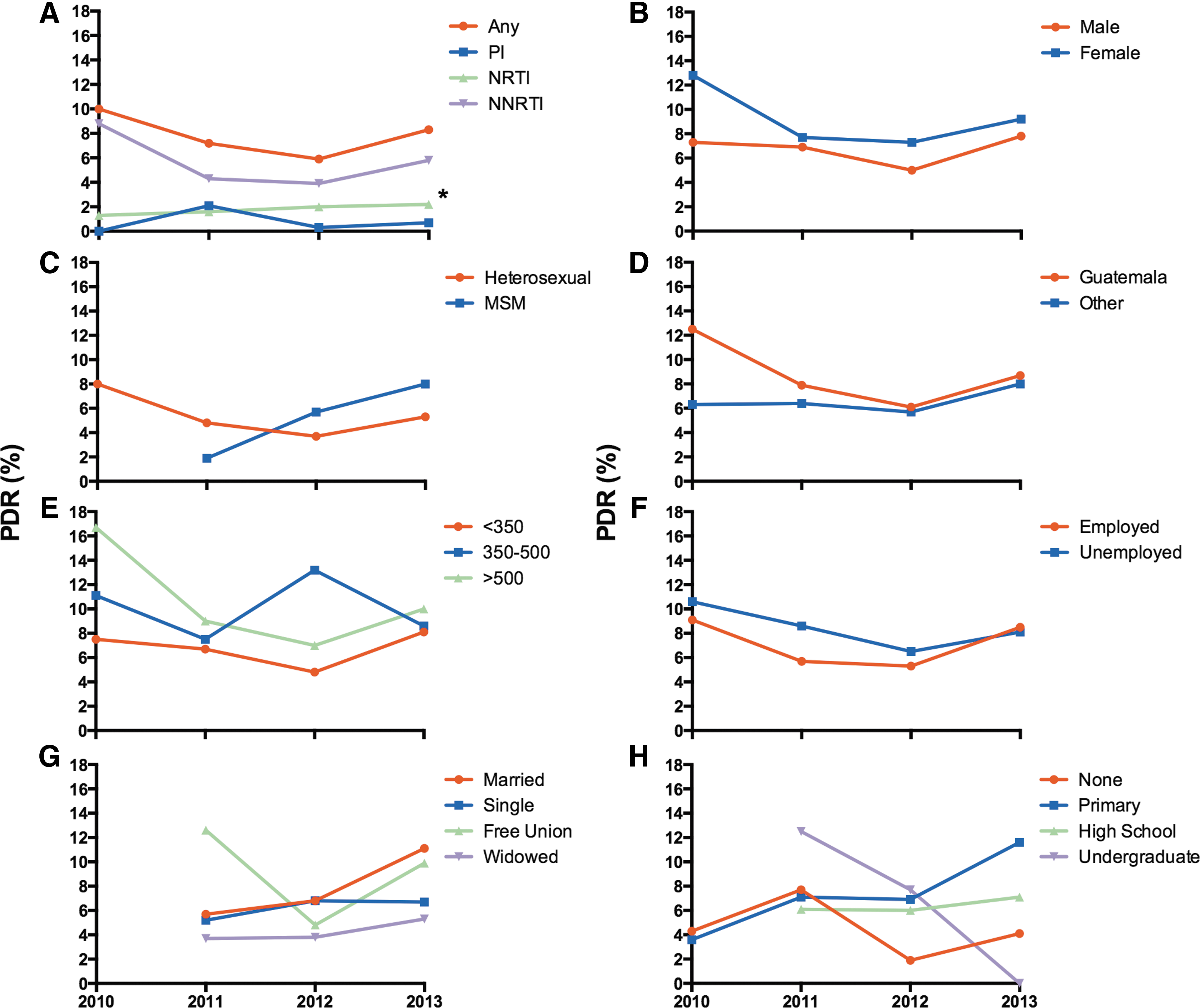
HIV pre-PDR trends in time by demographic variables. PDR was estimated for 1,084 PR-RT HIV sequences from antiretroviral treatment (ART)-naive Guatemalan individuals enrolled at the Roosevelt Hospital in Guatemala City, using the WHO list of mutations for HIV drug resistance surveillance.
14
PDR trends per year of enrollment are depicted by drug family
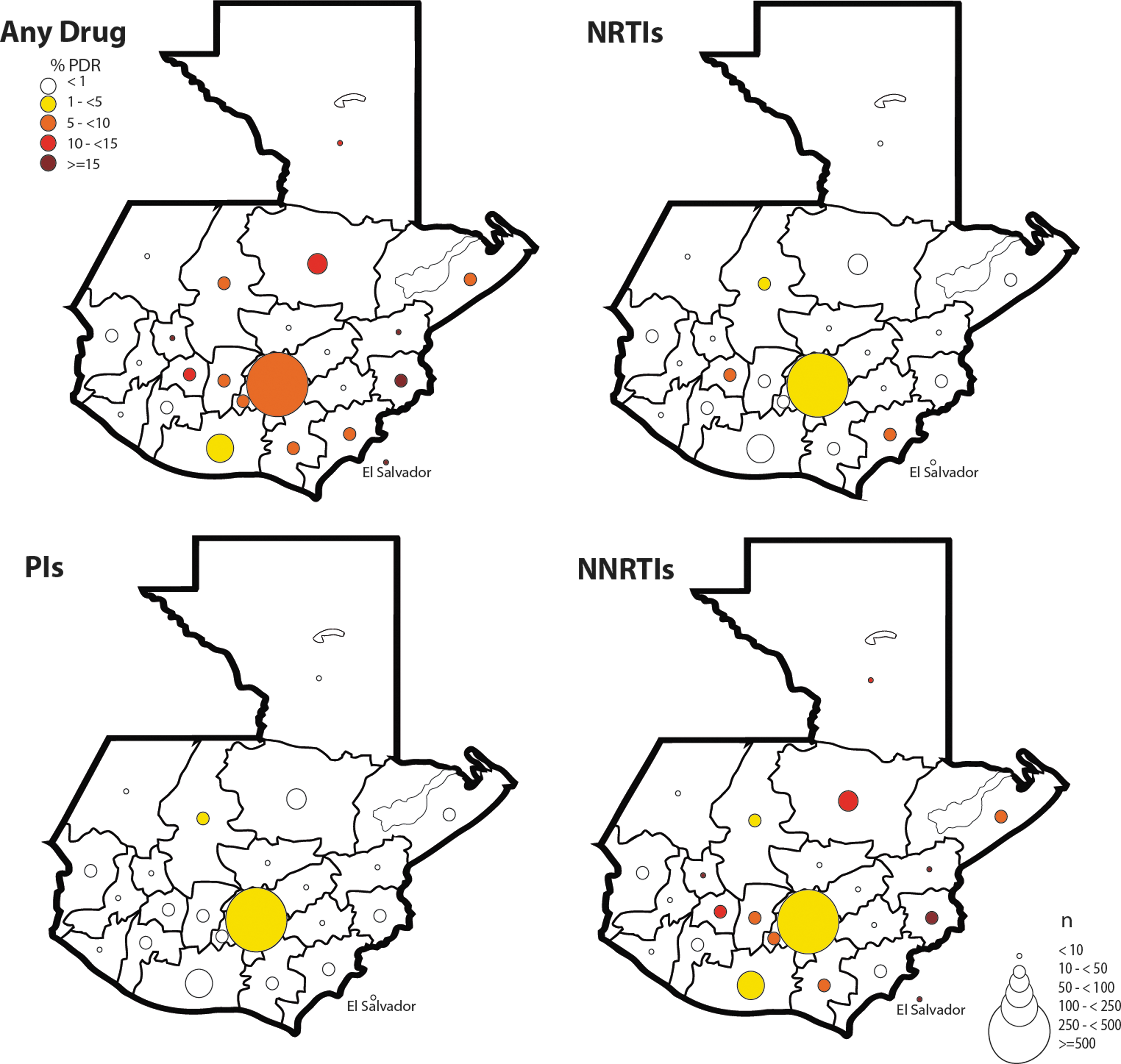
Geographic distribution of HIV PDR cases observed in the study. PDR was estimated for 1,084 PR-RT HIV sequences from antiretroviral treatment (ART)-naive Guatemalan individuals enrolled at the Roosevelt Hospital in Guatemala City, using the WHO list of mutations for HIV drug resistance surveillance. 14 The percentage of PDR cases by department of residence is shown. Circle size reflects the number of patients enrolled for each department; color reflects PDR levels. PDR, pre-antiretroviral treatment drug resistance; NRTI, nucleoside reverse transcriptase inhibitors; NNRTI, nonnucleoside reverse transcriptase inhibitors; PI, protease inhibitors.
NNRTI PDR was significantly higher in individuals with higher CD4+ T cell counts (>500 cells/μl and 350–500 cells/μl vs. <350 cells/μl; p=0.039 and p=0.007, respectively; Table 2), suggesting a possible temporal increase in PDR to this drug family. To further explore PDR variations in time, we assessed TDR by identifying recently infected (RI) individuals using a multiassay algorithm including HIV incidence tests. From 1,084 individuals, 397 eligible individuals (>200 CD4+ T cells/μl and <1 year of HIV diagnosis) were screened with the BED assay. From these, 112 individuals with positive results were reassayed with the Lag-Avidity test, with only 72 (6.6%) individuals in the whole cohort fulfilling the RI criteria. TDR to any ARV drug in RI individuals was 9.7% (7/72) with only NNRTI TDR cases found (Table 2). RI individuals showed a tendency of higher NNRTI DR than the rest of the individuals in the cohort (9.7% vs. 4.5%; p=0.0794). No significant trends in global PDR or PDR to any of the studied ARV drug families were observed when using a moving average approach based on dates of enrollment for the study period (Fig. 3).
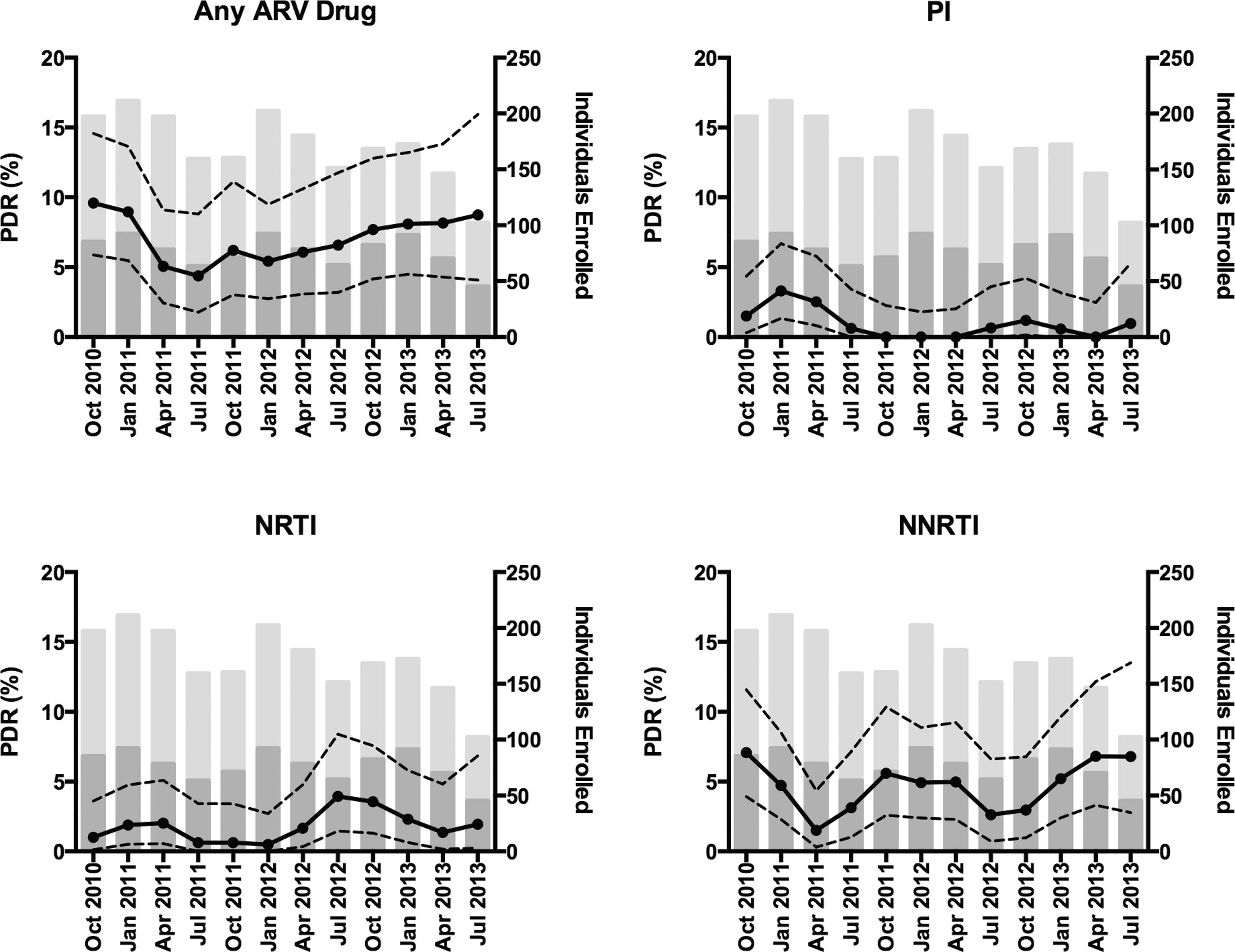
HIV PDR trends in Guatemala 2010–2013. PDR trends by date of enrollment were estimated using a moving average approach, with 6-month windows, moving by 3-month intervals. PDR prevalence and 95% confidence intervals (CI) are shown. The number of individuals enrolled for each estimation is shown: dark gray, individuals coming from Guatemala City; light gray, individuals coming from departments other than Guatemala City. PDR, pre-antiretroviral treatment drug resistance; NRTI, nucleoside reverse transcriptase inhibitors; NNRTI, nonnucleoside reverse transcriptase inhibitors; PI, protease inhibitors.
Over half of the NNRTI PDR cases could be explained by the presence of the K103N mutation, while nearly a third was associated with K101E (Table 3). Other major NNRTI PDR mutations observed at low frequencies included V106M, Y188H, G190A/E, and P225H. All DR cases among RI individuals were associated with the K103N mutation (data not shown). Interestingly, 2.3% of viruses showed polymorphisms at position 138, associated with resistance to rilpivirine, which occurred mainly in individuals with <350 CD4+ T cells/μl. These polymorphisms are not considered in the WHO list of mutations for HIV drug resistance surveillance and increase the prevalence of viruses with resistance using the Stanford definition (Table 2). A fifth of NRTI PDR cases were associated with M41L and another fifth with T215 revertants (T215D/E). Other NRTI mutations observed at lower frequencies included D67E, T69D, L74V, V75T/M, F77L, M184V, L210W, and K219Q (Table 3). Most cases of PI PDR could be explained by the presence of L24I, M46I/L, or L90M. Other PI mutations found at lower frequency included L23I, I54V, V82M, and N83D (Table 3).
Frequency in individuals with pre-ART drug resistance (PDR; defined with the WHO list of mutations for HIV drug resistance surveillance) to the corresponding drug class. Mutations included in the WHO list of mutations for transmitted drug resistance surveillance are shown in bold. Other mutations contribute with drug resistance penalty scores in the Stanford algorithm. Only mutations found in the cohort are shown. Mutations considered for the analysis are as follows (WHO mutations are shown in bold):
NRTIs:
NNRTIs: V90I, A98G,
PIs: L10F, K20I,
Clusters of viruses with NNRTI PDR and high bootstrap support (>80%) were observed (Fig. 4), including one from two heterosexual males from Alta Verapaz and Guatemala City (bootstrap 88%), one from a female and a heterosexual male from Quiché and Guatemala City (99%), one from three heterosexual/MSM males from Guatemala City (90%), all with NNRTI PDR; one from two MSM from Guatemala City (100%) with PDR to two drug families; and a cluster of 12 sequences combining seven females and five males (two MSM) from Alta Verapaz, Guatemala City, Chiquimula, Sololá, Escuintla, and Izabal with NNRTI PDR (98%, Fig. 4).
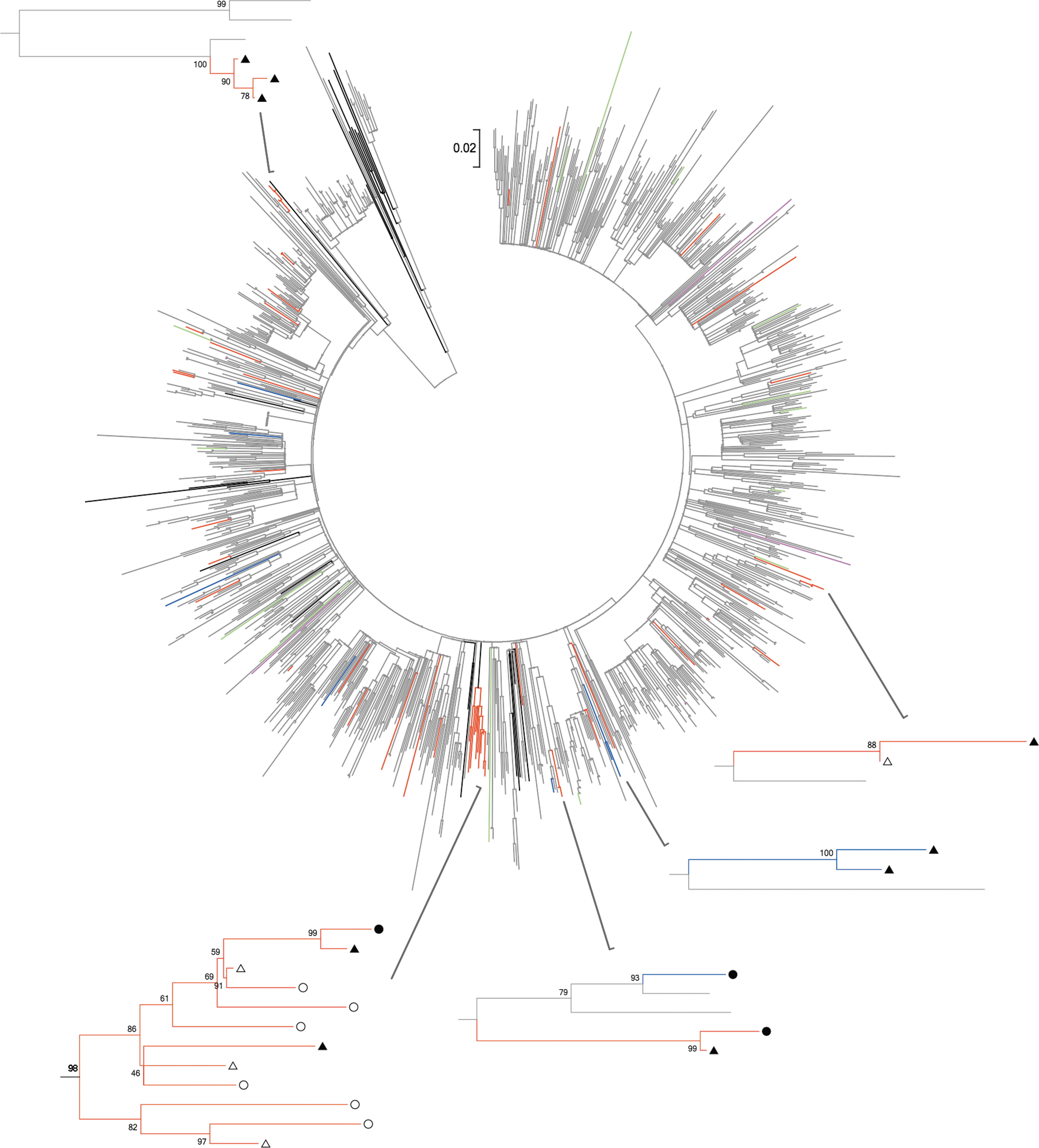
Phylogenetic analysis of 1,084 HIV pol sequences from antiretroviral treatment-naive Guatemalan individuals. The tree was inferred by the maximum likelihood method, using the general time reversible+Γ +I model with MEGA v6.0 software. 23 Significance was tested with 1,000 bootstrap replicates. Evolutionary distances are drawn to scale in base substitutions per site. Reference sequences obtained from the Los Alamos HIV Sequence Database are shown in black. 21 Sequences with NNRTI PDR are shown in red, sequences with NRTI PDR in green, and sequences with PI PDR in purple. Sequences with PDR to two drug families are shown in blue. Details of clusters of sequences with NNRTI PDR are shown: circles, females; triangles, males; open, Guatemala City; full, departments other than Guatemala City.
No associations were observed between PDR and demographic variables including age, genre, geographic location, risk factor for HIV infection, literacy, employment, marital status, or previous pregnancies. No association between PDR and HIV subtype was evident either. After multivariate adjustment, a significant association between NRTI PDR and residence in Guatemala City became evident (OR 4.2, 95% CI 1.2–14.9, p=0.027).
Discussion
We present results of the largest study to date aiming to characterize HIV PDR in Guatemala. The cohort in this study included 55.3% of individuals from Guatemala City. This represents a possible enrollment bias considering that about 30% of the officially reported HIV cases correspond to Guatemala City. 24 According to official statistics, underrepresentation for some departments, such as San Marcos, Izabal, Quetzaltenango, Retalhuleu, and Petén, could exist in our study. The fact that all participants were recruited at only one clinic also limits the extrapolation of our results to the national level. Nevertheless, even though this study does not fulfill the sampling requirements of a nationally representative WHO PDR surveillance study, the size of the cohort and the fact that 70% of the participants came from the three departments representing over 50% of all the reported HIV cases in Guatemala—Guatemala City, San Marcos, and Escuintla—make our results relevant for the country and the field.
The Guatemalan cohort showed characteristics similar to what has been previously described for HIV-infected individuals at the national level. 24,25 The male-to-female ratio observed here (1.5) was similar to the national 2010–2012 value (1.3). The main risk factor reported for HIV acquisition was heterosexual sex, with one in four males identifying themselves as MSM in the enrollment questionnaire, which probably reflects subreporting due to fear of disclosure or stigmatization known to be common in the country. 3,4 Also, most individuals were single (41.0% in this study vs. 46.1% in the 2012 official statistics) and had low literacy levels as has been previously reported. 24 Moreover, a large proportion of the participants (53.6%) presented for clinical care at late stages of HIV disease (<200 CD4+ T cells/μl) as previously observed (56.5% national average 2010–2012). 24
We found an intermediate level of PDR according to WHO categorization, mainly associated with NNRTI PDR. This observation is in accordance with what has been described globally for other low/middle-income countries with recent universal access to ART. 1 Also, it is consistent with the predominant use of NNRTI-containing first-line regimens in Guatemala. 10,26 No trends in PDR levels, both global and to each ARV drug family, were observed analyzing the data by year of collection (2010–2013) or using a moving average approach during the sampling period. This is in accordance to other reports that have been unable to find recent PDR trends in parts of the world different from Africa. 1,27
RI individuals showed a tendency for higher DR than the rest of the individuals in the cohort, although significance was not reached perhaps due to the small number of individuals fulfilling the RI criteria. Interestingly, only NNRTI TDR was observed in RI individuals, consistent with current widespread use of efavirenz-containing first-line regimens in Guatemala and the lower genetic barrier of the NNRTI drug family. On the other hand, considering the fact that individuals with >500 CD4+ T cells/μl and 350–500 cells/μl showed higher NNRTI PDR than individuals with <350 cells/μl, an increasing trend for NNRTI TDR in time could be argued. As CD4+ T cell counts are strongly associated with the time of HIV disease progression in most patients, this categorization would reflect a significant time interval between the mean infection date of individuals from the extreme groups (550 cells/μl difference between the means of the two groups; considering a CD4+ T cell decline between 50 and 70 cells/μl per year, 28 a period of 7.9–11 years).
It is important to mention that this study did not include ART reinitiators, given that a thorough investigation by the multidisciplinary team at the Roosevelt Hospital was made to exclude individuals with previous exposure to ARV drugs from the study. When suspicion was raised concerning the accuracy of the information on previous ARV drug exposure given by the participants in the enrollment questionnaire, individuals were excluded from the study. Also arguing for an increase in NNRTI PDR is the fact that although partial reversion of complex transmitted drug resistance mutation patterns has been reported, 29,30 persistence of TDR mutations for long periods of time in chronic infection has been a common observation in multiple studies. 31 –35
The presence of clusters of sequences with NNRTI PDR and high statistical support suggested possible transmission networks promoting NNRTI PDR. These clusters imply complex transmission networks including males and females from wide geographic areas, not limited to Guatemala City. The role of sexual transmission of ARV drug-resistant virus by patients in care who engage in high-risk activities has been recently demonstrated. 36 However, the importance of ART-naive individuals in the spread of TDR mutations has also been recorded. 32 This is especially relevant in explaining the presence of polymorphisms at RT position 138, associated with resistance to rilpivirine, a drug not included in ARV schemes in the country.
No associations between demographic variables and PDR were observed. This suggests that PDR in Guatemala may not be characteristic of specific social groups, higher risk populations, or geographic locations. Also, no specific PDR trends in time associated with demographic variables were observed in the present study. This contrasts with other studies in which significant PDR increasing and decreasing trends have been associated with demographic variables such as gender, risk for HIV acquisition, viral subtype, and ethnic group. 37 –39 The lack of TDR to NRTI and PI in RI individuals could be related to the recent use of optimal ARV regimens, contrasting with the use of low-potency regimens in the past, as well as the low use of PI-containing regimens as first line.
This study not only suggests slow increasing trends in PDR to NNRTIs that are a concern for HIV management in Guatemala, but also emphasizes the importance of implementing drug resistance testing before starting first-line ARV regimens. 40 Cost–benefit and feasibility studies need to be carried out in order to assess the possibility of implementation of basal HIV drug resistance testing in the country. However, according to results shown here, when lack of resources made HIV pol genotyping an unfeasible option, cheap point mutation assays including at least K103N and K101E would allow detection of the majority of PDR cases, impacting the first-line ARV regimen success rate. Also, PDR would need to be tackled as a generalized phenomenon in the population of HIV-infected individuals, without the need to focus on particular groups, by strengthening clinical follow-up and counseling/education programs for persons under ART and generating data on early warning indicators for HIV drug resistance. 41
Conclusions
In all, we have shown evidence that PDR in Guatemala remains at an intermediate level according to WHO categorization. We did not find associations between PDR and demographic variables. Nevertheless, we have shown evidence suggesting increasing trends in NNRTI PDR, as well as complex transmission networks influencing NNRTI PDR spread, which need to be taken into account in national HIV management policies.
Footnotes
Acknowledgments
This work was supported by grants from the Mexican Government (Comisión de Equidad y Género de la H. Cámara de Diputados), CONACYT (SALUD-2013-01-202475), Instituto de Ciencia y Tecnología del Distrito Federal [PIRIVE09-18], and Fundación Mexico Vivo.
The authors thank all patients for their participation in this study, Zeidy Arenas and Silvia del Arenal for their logistic assistance, Sandra Zamora for her administrative support, Edna Rodriguez and Mario Preciado for CD4+ T cell count assays, and Ramón Hernandez and Carolina Demeneghi for viral load assays.
Author Disclosure Statement
No competing financial interests exist.