
Abstract
Transcription factor 7 like 2 (TCF7L2) rs7903146 polymorphism has been associated with metabolic disturbance and cardiovascular disease. The aim of this study was to analyze the association between TCF7L2 rs7903146 polymorphism and potential disturbances on the lipid profile in human immunodeficiency virus (HIV)/hepatitis C virus (HCV)-coinfected patients. We performed a cross-sectional study on 263 HIV/HVC-coinfected patients. TCF7L2 polymorphism was genotyped by GoldenGate assay. The analysis was performed by linear and logistic regression under a dominant model of inheritance. The variables analyzed were total cholesterol (TC), high-density lipoprotein (HDL-C), low-density lipoprotein (LDL-C), non-HDL-C, and triglycerides. Patients harboring the rs7903146 TT/TC genotype showed a diminished concentration of TC (p=0.003), LDL-C (p=0.004), HDL-C (p=0.012), and non-HDL-C (p=0.013), a lower percentage of TC≥200 mg/dl (p=0.038), and a higher percentage of HDL≤40 mg/dl (p=0.023). In addition, we observed that rs7903146 was differently related to fasting serum lipid levels according to the HCV-genotype (HCV-GT). With regard to HCV-GT1 patients, the rs7903146 TT/TC genotype was associated with lower levels of HDL-C [adjusted arithmetic mean ratio (aAMR)=0.91; p=0.049] and an elevated percentage of patients with HDL-C≤40 mg/dl [adjusted odds ratio (aOR)=3.26; p=0.003]. For HCV-GT3 patients, the rs7903146 TT/TC genotype was associated with lower serum values of TC (aAMR=0.81; p=0.037), LDL-C (aAMR=0.67; p=0.001), and non-HDL-C (aAMR=0.75; p=0.002) and a reduced percentage of TC≥200 mg/dl (aOR=0.089; p=0.037). In conclusion, the TCF7L2 rs7903146 TT/TC genotype was associated with lower levels of TC, LDL, and HDL in HCV-GT3 patients, and lower levels of HDL-C in HCV-GT1 patients, suggesting a role in cardiovascular disease and a potential use as a biomarker in HIV/HCV-coinfected patients.
Introduction
C
Dyslipidemia is a main risk factor for cardiovascular disease in patients with HIV infection, which is related to cART. 15,16 Thus, the risk of myocardial infarction is proportional to the time of cART 17 and it has also been demonstrated that it could be partly explained by the dyslipidemia caused by these drugs. 18 In this way, the increased cardiovascular risk is associated particularly with prolonged use of protease inhibitors, which are usually associated with a less favorable lipid profile, in particular elevated TG and TC. 15 Moreover, nonnucleoside reverse transcriptase inhibitors show, in general, the best lipid profile of all antiretrovirals because they are associated with an increase in HDL-C and a significant reduction in the TC/HDL-C ratio. 15 Finally, the effects of nucleoside reverse transcriptase inhibitors on lipids are generally mild and there is a high degree of heterogeneity. 11
The mechanisms leading to lipid disturbances are not completely understood, but there is growing evidence that genetic background may contribute to individual differences in this pathology. 19 –21 The transcription factor 7 like 2 (TCF7L2) is located on chromosome 10q25.3. This gene is integrated by 18 exons that suffer alternative splicing regulation. TCF7L2 is part of the Wnt/β-catenin signaling pathway, which is involved in glucose homeostasis and lipid metabolism. 22 Recently, the rs7903146 (C>T) single nucleotide polymorphism (SNP) located at the TCF7L2 intron 5 region has been strongly associated with metabolic syndrome, 23 type 2 diabetes mellitus, 24 dyslipidemia, 25 and cardiovascular disease 26,27 in the general population. However, to the best of our knowledge, the effect of TCF7L2 polymorphism has not been studied in HIV/HCV-coinfected patients.
The aim of this study was to analyze the association between TCF7L2 rs7903146 polymorphism and potential disturbances in the lipid profile in HIV/HCV-coinfected patients.
Materials and Methods
Study design and patients
We carried out a cross-sectional study on 263 nondiabetic HIV/HCV-coinfected patients from Hospital Gregorio Marañón (Madrid, Spain) between September 2000 and July 2009. All subjects included in our study were HCV treatment-naive patients who were potential candidates for HCV therapy.
The inclusion criteria for the study were HIV/HCV-coinfected patients who were over 18 years and HCV treatment-naive, detectable HCV-RNA by polymerase chain reaction, negative hepatitis B surface antigen, availability of a DNA sample, no clinical evidence of hepatic decompensation, no diabetes mellitus, and stable cART for at least 6 months before study entry or no need for cART according to treatment guidelines used in the study period. 28,29 Patients with active opportunistic infections, pregnant women, active drug and/or alcohol addiction, and other concomitant diseases or conditions were excluded. Thus, 495 HIV/HCV-coinfected patients met the criteria described above; 293 of them had a DNA sample available for genotyping, but only 263 patients were included in our study (12 patients were excluded due to DNA genotyping errors and 18 due to the absence of relevant clinical data). All patients were of European descent.
The study was conducted in accordance with the Declaration of Helsinki and patients gave their written consent for the study. The Institutional Review Board and the Research Ethics Committee of the Instituto de Salud Carlos III (ISCIII) approved the study.
Epidemiological and clinical data
The main clinical and epidemiological data of 263 patients analyzed were obtained from medical records. Body mass index (BMI) was calculated as the weight in kilograms divided by the square of the height in meters. The duration of HCV infection for patients with a history of intravenous drug use (IDU) was estimated starting from the first year they shared needles and other injection paraphernalia, which are the most relevant risk practices for HCV transmission. 30
Biochemical data
The biochemistry panel was measured by using an autoanalyzer Hitachi 912 (Boehringer Mannheim, Germany) in fasting patients. We collected data on TC, HDL-C, and TG. LDL-C was calculated by Friedewald estimation [LDL-C=TC – HDL-C – (TG/5)]. 31 Non-HDL-C was calculated as TC minus HDL-C. 32 The degree of insulin resistance was estimated for each patient by using the homeostatic model assessment (HOMA), according to the following formula 33 : fasting plasma glucose (mmol/liter)×fasting serum insulin (mU/liter)/22.5.
Liver biopsy
Liver biopsies were performed on 211 out of 263 patients following the recommendations of the Patient Care Committee of the American Gastroenterological Association 34 as previously described. 35 Liver fibrosis and necroinflammatory activity were estimated according to the Metavir score as follows: F0, nonfibrosis; F1, mild fibrosis; F2, significant fibrosis; F3, advanced fibrosis; and F4, definite cirrhosis. Activity grade was scored as follows: A0, nonactivity; A1, mild activity; A2, moderate activity; A3, severe activity. 36
Genotyping of the TCF7L2 polymorphism
Genomic DNA was extracted from peripheral blood with Qiagen columns (QIAamp DNA Blood Midi/Maxi; Qiagen, Hilden, Germany). DNA samples were genotyped at the Spanish National Genotyping Center (CeGen;
Statistical analysis
All statistical tests were performed with the Statistical Package for the Social Sciences (SPSS) 19.0 software (IBM Corp., Chicago, IL). All p-values were two-tailed and statistical significance was defined as p<0.05.
For the description of the study population, p-values were estimated with nonparametric tests: the Mann–Whitney U test was used for continuous variables and the Chi-square test for categorical variables.
Hardy–Weinberg equilibrium (HWE) for the TCF7L2 rs7903146 polymorphism was assessed by a Chi-square test, considering equilibrium when p>0.05. The genetic association study was carried out under a dominant genetic model for the T allele (CT/TT vs. CC), which was the model that best fit our data. On the one hand, lineal regression analyses were used to investigate the association between rs7903146 and continuous outcome variables, which were log10 transformed. This test provides the differences between groups and the arithmetic mean ratio (AMR), which provides the increase of the value with the presence of the T allele.
On the other hand, logistic regression analyses were used to investigate the association of rs7903146 with categorical outcome variables. This test provides the association between groups through the odds ratio (OR), which indicates the likelihood of having the outcome in the CT/TT genotypes versus the CC genotype. Each regression analysis was always adjusted by the most significant covariables associated with each one of the outcome variables, avoiding overfitting of the regression. The covariables were selected by the “Stepwise” algorithm (at each step, factors are considered for removal or entry: a p-value for entry and exit of 0.15 and 0.20, respectively), including gender, age, BMI, nadir CD4+ T cells, undetectable HIV viral load (<50 copies/ml), time with cART, specific antiretroviral drugs used by each patient (zidovudine, stavudine, didanosine, tenofovir, abacavir, efavirenz, ritonavir, lopinavir, saquinavir, and fosamprenavir), HCV viral load≥500,000 IU/ml, and significant fibrosis (F≥2).
We also included two polymorphisms (ADIPOQ rs2241766 and SLC30A8 rs13266634), which have been related to dyslipidemia in HIV/HCV-coinfected patients, according to two recent studies 20,21 performed by our group in the same cohort.
Results
Characteristics of patients
The study included 263 patients, whose epidemiological and demographic characteristics are shown in Table 1. There were no significant differences between rs7903146 genotypes (TT/TC versus CC).
Categorical variables were expressed in absolute numbers (%). Continuous variables were expressed in median (percentile 25; percentile 75). AIDS, acquired immunodeficiency syndrome; BMI, body mass index; cART, combination antiretroviral therapy; HCV, hepatitis C virus; HCV-RNA, HCV plasma viral load; GT, genotype; HIV, human immunodeficiency virus; HIV-RNA, HIV plasma viral load; HOMA, homeostatic model assessment; IVDU, intravenous drug users; NNRTI, nonnucleoside analog reverse-transcriptase inhibitors; NRTI, nucleoside analog reverse-transcriptase inhibitors; PI, protease inhibitors.
Note that patients infected with HCV-GT3 had lower serum values of TC (p=0.013), LDL-C (p=0.014), and non-HDL-C (p=0.026) than patients infected with HCV-GT1 (Supplementary Fig. S1; Supplementary Data are available online at
Frequencies of the TCF7L2 polymorphism
Allele frequencies for the TCF7L2 rs7903146 polymorphism were 0.64 for the C allele and 0.36 for the T allele. Genotype frequencies for the rs7903146 polymorphism were 0.42 for the CC genotype, 0.43 for the TC genotype, and 0.15 for the TT genotype. These frequencies in our dataset were in accordance with data listed on the NCBI SNP database (
Association of rs7903146 with lipids profile
Patients with the rs7903146 TT/TC genotype showed significantly lower TC serum levels (p=0.003; Fig. 1A), LDL-C (p=0.004; Fig. 1B), HDL-C (p=0.012; Fig. 1C), and non-HDL-C (p=0.013; Fig. 1D) than CC carriers. When we stratified the patients by HCV genotype, rs7903146 TT/TC carriers infected with HCV-GT3 had diminished values of TC (p=0.019; Fig. 1A), LDL-C (p=0.013; Fig. 1B), and non-HDL-C (p=0.020; Fig. 1D).

Summary of the unadjusted association between TCF7L2 rs7903146 and the concentration of serum lipid profile among HIV/HCV coinfection
Patients with the rs7903146 TT/TC genotype had a diminished percentage of TC≥200 mg/dl (p=0.038; Fig. 2A) and non-HDL-C≥130 mg/dl (p=0.041; Fig. 2D) and an elevated percentage of HDL-C≤40 mg/dl (p=0.028; Fig. 2C). When patients were stratified by HCV genotype, rs7903146 TT/TC carriers infected with HCV-GT3 had a lower percentage of TC≥200 mg/dl (p=0.001. Fig. 2A), whereas rs7903146 TT/TC carriers infected with HCV-GT1 had a higher percentage of HDL-C≤40 mg/dl (p=0.018; Fig. 2C).
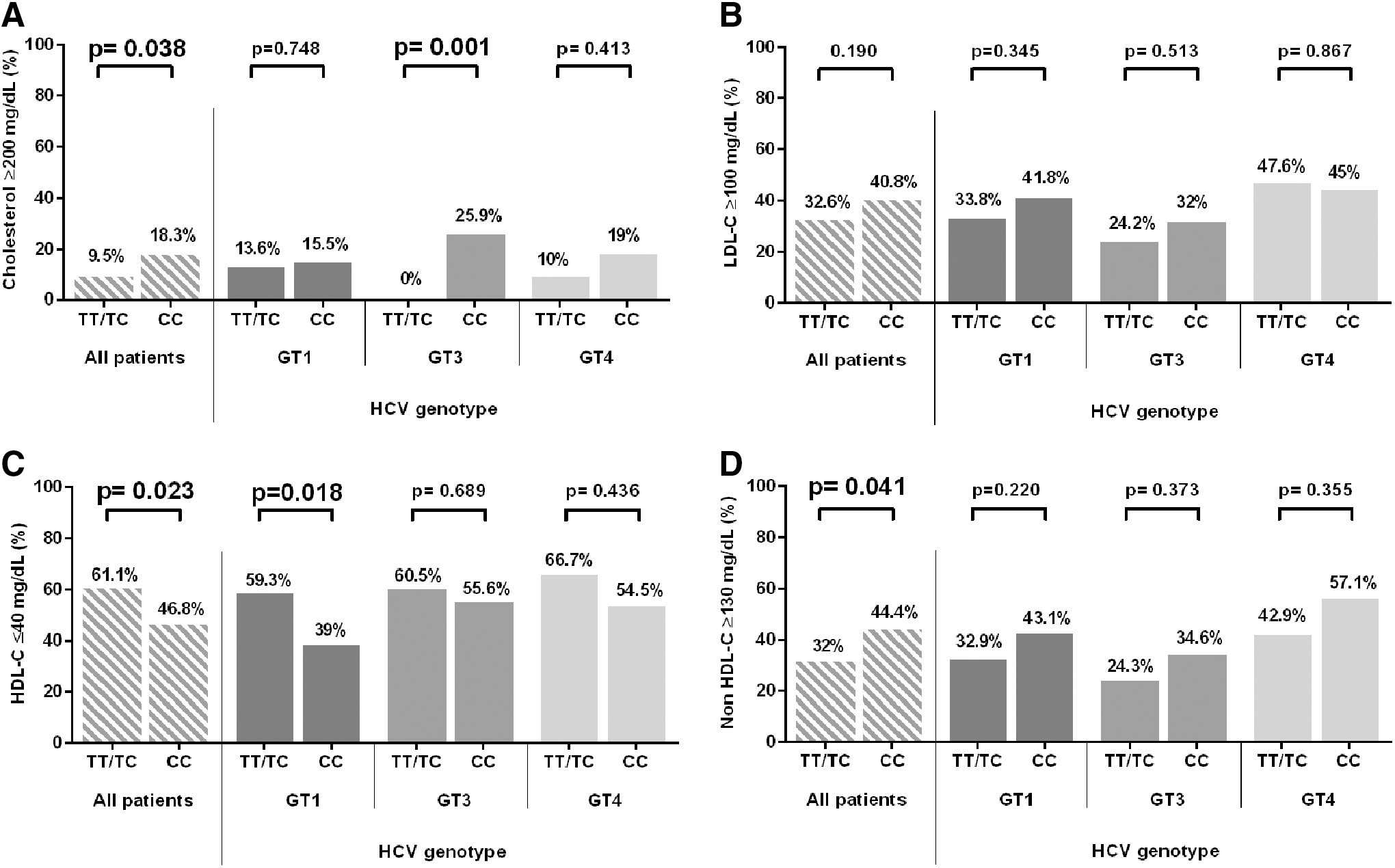
Summary of the unadjusted association between TCF7L2 rs7903146 and the NCEP ATP-III characteristics among HIV/HCV coinfection
When adjusted regression was performed (Table 2), rs7903146 TT/TC carriers infected with HCV-GT3 were associated with lower values of TC [adjusted AMR (aAMR)=0.81; p=0.003], LDL-C (aAMR=0.67; p=0.001), and non-HDL-C (aAMR=0.75; p=0.002), and a percentage of TC≥200 mg/dl [adjusted OR (aOR)=0.89; p=0.037]. An association between rs7903146 TT/TC genotype and diminished levels of HDL-C (aAMR=0.91; p=0.049) and an elevated percentage of HDL-C≤40 mg/dl (aOR)=3.26; p=0.003) was found in HCV-GT1 patents.
Multivariate lineal regression was performed to compare the serum lipid values, which were log10-transformed.
Logistic regression was performed to compare categorical variables. Both tests were adjusted by significant epidemiological and clinical factors (age, gender, BMI, nadir CD4+, CD4+ T cells/μl, HIV plasma viral load, HCV plasma viral load, time on cART, specific antiretroviral drugs, and related SNPs). Statistically significant differences are shown in bold.
AMR, arithmetic mean ratio (how many times greater is the value in the presence of the TT/TC genotype versus CC genotype); OR, odds ratio (likelihood of having the outcome in the CT/TT genotype versus CC genotype); CI, confidence interval; GT, genotype; HCV, hepatitis C virus; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; TG, triglycerides.
Discussion
In the present study, we evaluated for the first time the impact of the TCF7L2 rs7903146 polymorphism on the serum lipid profile in HIV/HCV-coinfected patients. The major findings were (1) the rs7903146 TT/TC genotype (T allele) was related to lower fasting serum levels of TC, LDL-C, and non-HDL-C in HIV patients coinfected with HCV-GT3 and (2) the rs7903146 TT/TC genotype was linked to diminished levels of HDL-C and an elevated percentage of patients with HDL-C≤40 mg/dl among HIV patients coinfected with HCV-GT1.
Several reports have analyzed the association of the TCF7L2 polymorphism with serum lipid disturbances in the non-HIV/HCV-coinfected population, providing discordant results. Thus, the presence of the rs7903146 T allele disrupted the lipid metabolism, inducing low levels of HDL-C and apolipoprotein (Apo)-A1 in healthy young men, 25 high levels of TG in familial combined hyperlipidemia patients, 37 and an atherogenic lipoprotein profile in nonalcoholic fatty liver disease. 38 Moreover, the rs7903146 T allele has been linked to a greater severity of coronary artery disease, a higher death ratio by cardiovascular event, and increased cardiovascular risk in nondiabetic individuals. 39 In contrast, it has been described that rs7903146 T carriers show a favorable lipid profile with lower TG and higher HDL-C concentration. 40 However, other studies did not find a significant association between rs7903146 and lipid metabolism. 41,42 These inconsistencies could be due to different study designs (transversal, retrospective, cohorts, etc.), patient characteristics (age, race, etc.), environmental exposure (mainly diet), or underlying comorbidities (polycystic ovary syndrome, metabolic syndrome, type 2 diabetes mellitus, etc.).
The cardiovascular risk and atherosclerosis associated with CHC infection have been previously reported. For instance, HCV infection has been related to carotid atherosclerosis, coronary artery stenosis, and increased carotid intima-media thickness. 43 According to the National Cholesterol Education Program Adult Treatment Plan Guideline III (NCEP ATP-III), the evaluation of total cholesterol, triglycerides, lipoproteins, and several risk factors is useful to assess the person's risk status for CHD. 44 Elevated LDL-C is considered as a major risk factor. For this reason, cholesterol-lowering therapy is a primary goal. Treatment of patients with CHD or equivalent risks should aim at reaching an LDL<100 mg/dl. 44 Nevertheless, the adequate interpretation of our data in the context of cardiovascular risk in coinfected patients is complicated, due to interactions between HIV, HCV, and cART. For instance, (1) HIV infection is strongly related to lipid disturbances in cART-naive patients, including reduced levels of TC, HDL-C, and LDL-C, and elevated levels of TG 45 ; (2) cART induces increased levels of TC, LDL-C, and TG 13 ; and (3) HCV replication depends on the lipid metabolism of the host cells, which generates an increased lipid cellular content, generates alterations in membrane structures, and induces dyslipidemia, mainly represented by low circulating levels of TC, LDL-C, 2,46 and HDL-C. 46 For these reasons, we consider that the multivariate regression with continuous values of TC and lipoproteins could be a better indicator than thresholds to evaluate the impact of TCF7L2 polymorphism on relative cardiovascular risk in HIV/HCV-coinfected patients.
It has previously been indicated that patients with CHC have a lipid profile similar to that of patients with familiar hypobetalipoprotinemia. These diminished levels on beta-lipoproteins are more commonly present in HCV-GT3 infection than HCV-GT1. 47 These facts are in agreement with our results, which reveal a key role of the rs7903146 polymorphism on beta-lipoprotein metabolism in patients infected with HCV-GT3. We observed that the presence of a minor T allele at the rs7903146 polymorphism was associated with a favorable cardiovascular profile represented by diminished serum levels of TC, non-HDL-C, and LDL-C among HCV-GT3 patients. In contrast, the rs7903146 T allele was correlated with lower levels of HDL-C and an elevated percentage of patients with T allele showed HDL-C≤40 mg/dl among the HCV-GT1 patients, which is considered an independent risk factor by NCEP ATP-III. 44
Considering that the presence of the rs7903146 T allele was related to dislipidemia, the genotyping of the TCF7L2 rs7903146 polymorphism could help to identify individuals with lipid disturbances, opening the possibility of implementing early treatment for these patients. However, the analysis of the rs7903146 T allele for the prediction of dyslipidemia according to NCEP ATP-III thresholds revealed a low diagnostic performance [area under the receiver operating characteristic curves (AUC-ROCs)<0.6 (data not shown)]. Thus, the utility of the rs7903146 polymorphism for the prediction of dyslipidemia is limited according to our data, even though further extensive clinical research studies will be needed to clarify the impact of this SNP on cardiovascular disease in HIV/HCV-coinfected patients.
Many studies have described the interaction of HIV, HCV infection, and antiretroviral therapy to increase the risk of insulin resistance and T2DM, 48,49 although the mechanisms are not completely understood. Moreover, there is growing evidence that genetic background may contribute to differences between individuals in complex diseases. 19,50 A strong association between T2DM risk and TCF7L2 SNPs was reported by Grant et al. 51 Next, genetic variations in TCF7L2 (particularly rs7903146) were related to T2DM 52 and glucose metabolism. 53,54 Later, the association between a minor T allele of rs7903146 and T2DM was replicated in multiple different populations, as shown in an independent meta-analyses by Cauchi et al., 55 Luo et al., 56 Tong et al., 57 and Peng et al. 24 Furthermore, the T allele has been associated with an increased proinsulin/insulin ratio, impaired beta cell function, and hyperglycemia. 54,58 –60 The participants of the present study were nondiabetic HIV/HCV patients, but 34.6% showed insulin resistance (HOMA≥3.0). Nevertheless, an exhaustive analysis showed that the rs7903146 polymorphism was not related to HOMA values in our HIV/HCV-coinfected population (data nor shown). This lack of association with glucose metabolism could be due to the limited number of patients used in the stratified analysis, or also to the possible distortive effect of direct and indirect factors related to both HIV and HCV infections and cART. 48 Moreover, we must not discount the fact that our patients had a relatively low BMI (median: 22.5 kg/m2).
The present study has several limitations that must be taken into account for the correct interpretation of the data: (1) this is a cross-sectional study with a limited number of patients, which could limit achieving statistical significance; (2) lipid disturbances may be caused by several interacting genetic and environmental determinants, making it difficult to find the true individual effects of each disease-associated factor; (3) our study must also be performed in monoinfected and untreated patients in order to evaluate the effect of chronic hepatitis C, HIV infection, and cART separately; (4) our study was carried out entirely in whites; therefore as allele frequency differs among ethnicities, 24 it would be necessary to perform an independent replication of this study in different ethnicities.
Conclusions
The TCF7L2 rs7903146 TT/TC genotype was associated with lower levels of TC, LDL, and HDL in HCV-GT3 patients and lower levels of HDL-C in HCV-GT1 patients, thus suggesting its role in cardiovascular disease and its potential use as a biomarker in HIV/HCV-coinfected patients. Nevertheless, we consider that further analyses on a large population are needed to conclusively corroborate these results.
Footnotes
Acknowledgments
The authors thank the Spanish National Genotyping Center (CeGen) for providing the SNP genotyping services (
D.P.T., M.A.JS., and M.G.A. have received research funding from “Instituto de Salud Carlos III” [grants CM12/00043, CM10/00105, and CD12/00442, respectively]. J.B. is an investigator from the Programa de Intensificación de la Actividad Investigadora en el Sistema Nacional de Salud (I3SNS).
This work has been supported by grants from Fondo de Investigación de Sanidad en España (FIS) [Spanish Health Funds for Research] [grants PI08/0738, PI11/00245; PI08/0928, and PI11/01556], and “Fundación para la Investigación y la Prevención del Sida en España” (FIPSE) [grant 361020/10]. This work has been (partially) funded by the RD12/0017/0024 and RD12/0017/0004 projects as part of the Plan Nacional R+D+I and cofinanced by ISCIII––Subdirección General de Evaluación y el Fondo Europeo de Desarrollo Regional (FEDER).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.