
Abstract
HIV isolates from South Africa are predominantly subtype C. Sporadic isolation of non-C strains has been reported mainly in cosmopolitan cities. HIV isolate j51 was recovered from a rural South African heterosexual female aged 51 years. Near full length amplification of the genome was attempted using PCR with primers targeting overlapping segments of the HIV genome. Analysis of 5593 bp (gag to vpu) at a bootstrap value greater than 70% found that all but the vpu gene was HIV-1 subtype A1. The vpu gene was assigned HIV-1 subtype C. The recombination breaking point was estimated at position 6035+/− 15 bp with reference to the beginning of the HXB2 reference strain. Isolate j51 revealed a unique genome constellation to previously reported recombinant strains with parental A/C backbones from South Africa though a common recombination with subtype C within the vpu gene. Identification of recombinant strains supports continued surveillance of HIV genetic diversity.
H
In Southern Africa, HIV-1 subtype C is the predominant strain in the epidemic, 2,4,5 although sporadic identification of non-subtype C strains has been reported. 6 –8 Although studies have indicated that subtype differences may not have an effect on the response to cART, particularly in HIV-1 group M strains, 9,10 recombinant strains may complicate the course of HIV infection. 11 Studies have implicated globalization and the movement of people from different geographic areas in the increasing rise in recombinant HIV strains. 2,12
In South Africa, HIV-1 subtype C has been reported to be the predominant strain. 4,8,13 First reports of non-subtype C strains in South Africa originated from the highly cosmopolitan global tourist city of Cape Town 14,15 in men who have sex with men (MSM). Since then, there has been continued identification of non-subtype C strains mainly in studies on HIV drug resistance. 8,16 –18 Monitoring the genetic diversity of circulating HIV strains has been encouraged to generate information on patient management and even vaccine strategies. 3 Recently, Palm et al. 11 demonstrated increased risk of AIDS and AIDS-related death in individuals infected with recombinant strain HIV-1 A3/CRF02_AG. The recombinant virus was found to be more virulent causing AIDS and AIDS-related death between 5.0 and 8.0 years from the time of seroconversion. 11 This study describes the first unique near full length HIV-1 recombinant strain isolated from a rural South African heterosexual female who was referred to the Dr. George Mukhari Academic Hospital (DGMAH) in Pretoria.
Ethical approval was granted by the University of Limpopo Research and Ethics Committee (MREC/P/37/2010). The study patient was a rural South African heterosexual female [residing in Lephalale (Ellisras), located some 210 km from Polokwane city in Limpopo Province] who was referred to DGMAH in Pretoria. At the time of sample collection, the patient was 51 years of age and had an HIV viral load of log10 6.0 copies/ml. The revelation of a rare subtype in the region prompted near full-length genome analysis of this HIV strain.
Total nucleic acid was extracted from plasma using the high pure nucleic acid extraction kit following the manufacturer's instructions (Roche Diagnostics, Mannheim, Germany).
Near full length HIV genome analysis was conducted in four overlapping fragments spanning the beginning of the gag gene to the end of the vpu gene. The gag, pol [protease (PR) and reverse transcriptase (RT)], and accessory genes (vif, vpr, tat, rev, and vpu) were amplified as single targets as previously described. 4 For the integrase gene, primers INFORI (5′-GGA ATC ATT CAA GCA CAA CCA GA-3′) and INREV-I (5′-TCT CCT GTA TGC AGA CCC CAA TAT-3′) for the first round polymerase chain reaction (PCR) and primers V1F (5′-GAA AAG GGG ATC CTC TAT CTG GCA TGG GTA CCA-3′) and V2R (5′-AGC CGT CGA TAG TGG GAT GTG TAC TTC TGA-3′) for the second round PCR were used. The amplification cycles were as described for the amplification of the pol (PR-RT) gene fragment after adjusting the annealing temperature to 54°C for both nested PCR cycles. 4
PCR products were sequenced with the ABI 3500XL (Life Technologies, Carlsbad, CA) using gene-specific primers. The HIV pol gene sequences were initially analyzed for genotypic drug resistance-associated mutation and HIV subtype using the online Stanford University HIV drug resistance database interactive tool (
Initial phylogenetic assessment of partial pol (PR-RT) gene sequences isolated from patients at DGMAH indicated the patient sample (isolate j51) as HIV-1 subtype A (Fig. 1a). The sample was assigned 93.6% and 93.5% similarity to HIV-1 subtype A on the PR and RT genes, respectively, by the Stanford HIV drug resistance analysis tool. A phylogenetic tree constructed using PAUP following an HKY85 substitution model with gamma distribution on CRP confirmed the sample as an HIV-1 subtype A1 on the pol gene (data not shown).
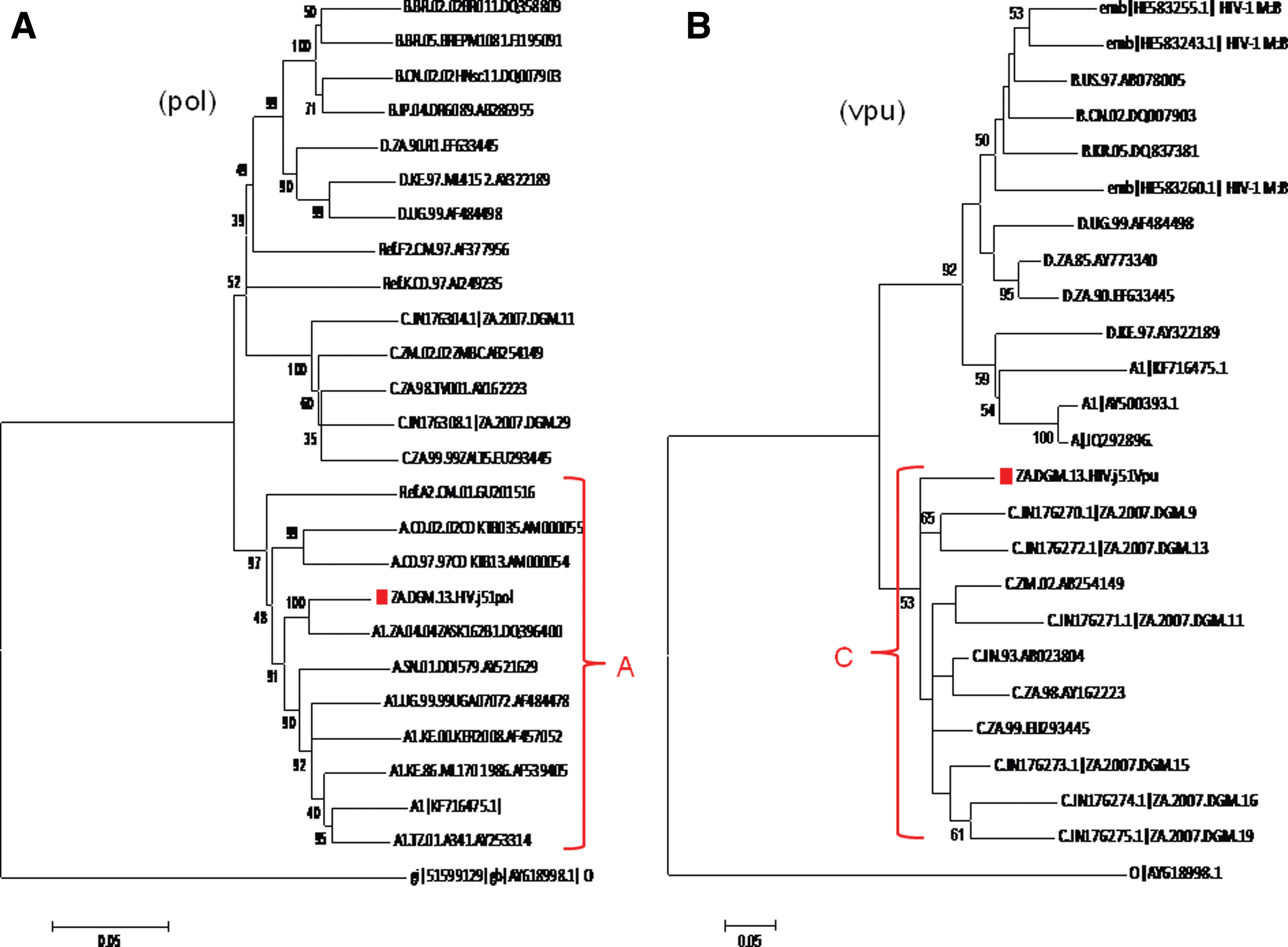
Phylogenetic analysis of the pol and vpu gene sequences.
The fragmented overlapping amplification yielded a 5593-bp genomic sequence corresponding to position 723 to 6316 with reference to the start of reference sequence HXB2 (Fig. 2A and B). The genomic sequences were defragmented to individual gene sequences with the aid of the sequence locator tool on the online HIV sequence database (Table 1). Analysis by REGA, jpHMM, and neighbor joining phylogenetic inference revealed that the gag, protease, reverse transcriptase and RNase, integrase, vif, vpr, tat, and rev genes were HIV-1 subtype A1 while the vpu gene was assigned to HIV-1 subtype C (Table 1 and Fig.1b). Approximate recombination breaking point analysis estimated that the recombination activity between the parental A1 strain and C strain occurred around position 6035±15 bp with reference to the start of the HXB2 reference sequence (Fig. 3A). The vpu gene was assigned to HIV-1 subtype C with a posterior probability of 1.0 on jpHMM (Fig. 3B). Bootscan analysis confirmed the recombination between parental HIV-1 subtype A1 and C with bootstrap support greater than 70% (Fig. 4).
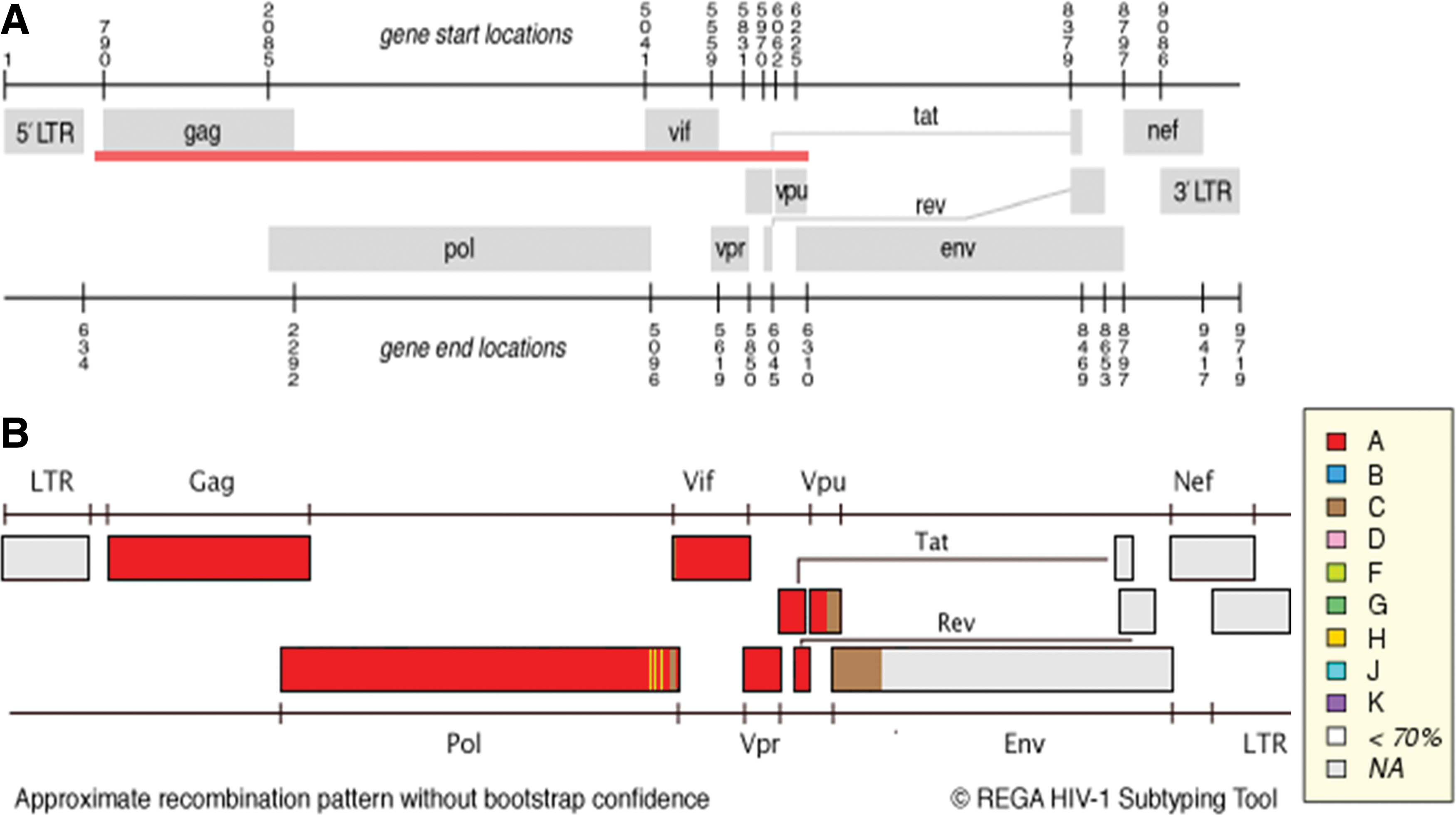
Sequence analysis of combined gene fragments from the suspected recombinant strain by REGA.
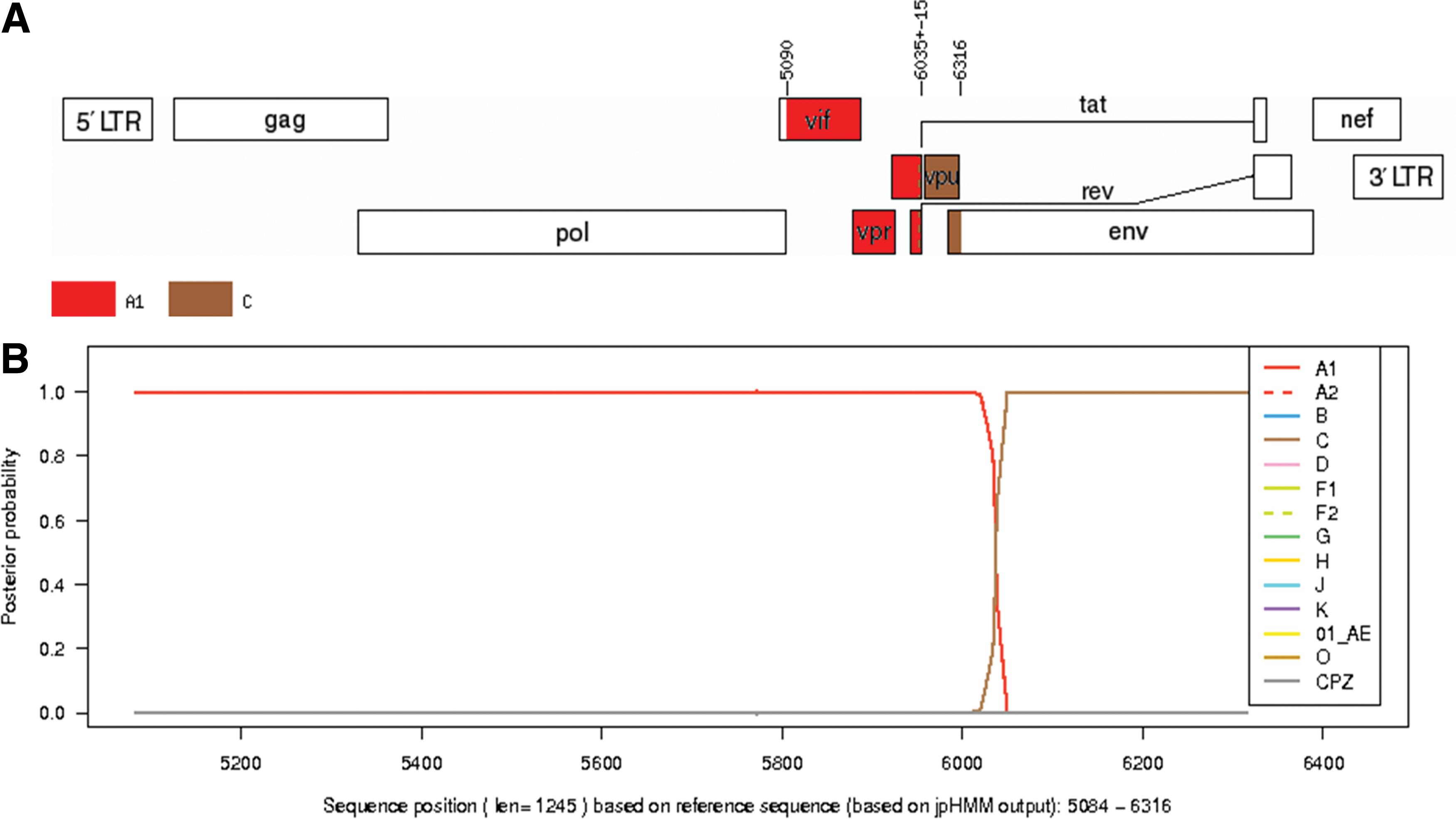
Analysis of the accessory genes genome fragment by jpHMM.
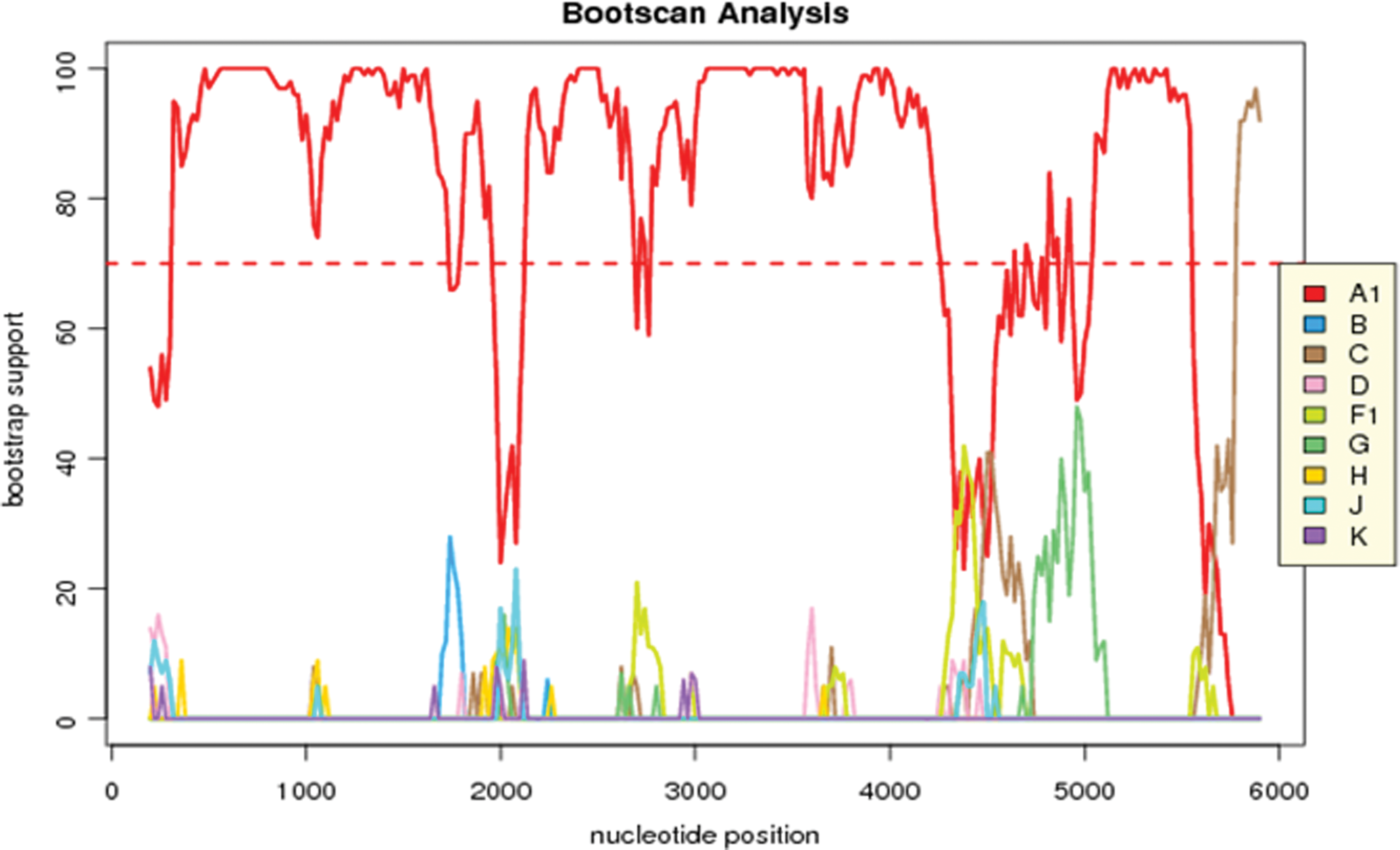
Recombination analysis of the amplified 5593-bp genome fragment. Bootscan analysis at greater than 70% shows recombination between HIV subtype A1 and C. Color images available online at
Nucleotide position relative to HXB2 genome start.
Comparison with previously reported recombinant strains with a parental HIV-1 subtype A and C backbone revealed that the genome constellation of the study isolate j51 was unique. Isolate 98ZADU178 had a subtype C constellation within the gag, pol, vif, and vpr genes with the tat and rev genes revealing a subtype A constellation followed by subtype C in the vpu gene. Isolate TV239 showed the HIV-1 subtype C genome only within the vpu gene in comparison to the same amplified genome segments as isolate j51. Isolate 8519 revealed a recombination pattern consisting of HIV-1 subtype A and C with breaking points within the gag, pol, and vpu genes (Fig. 5).
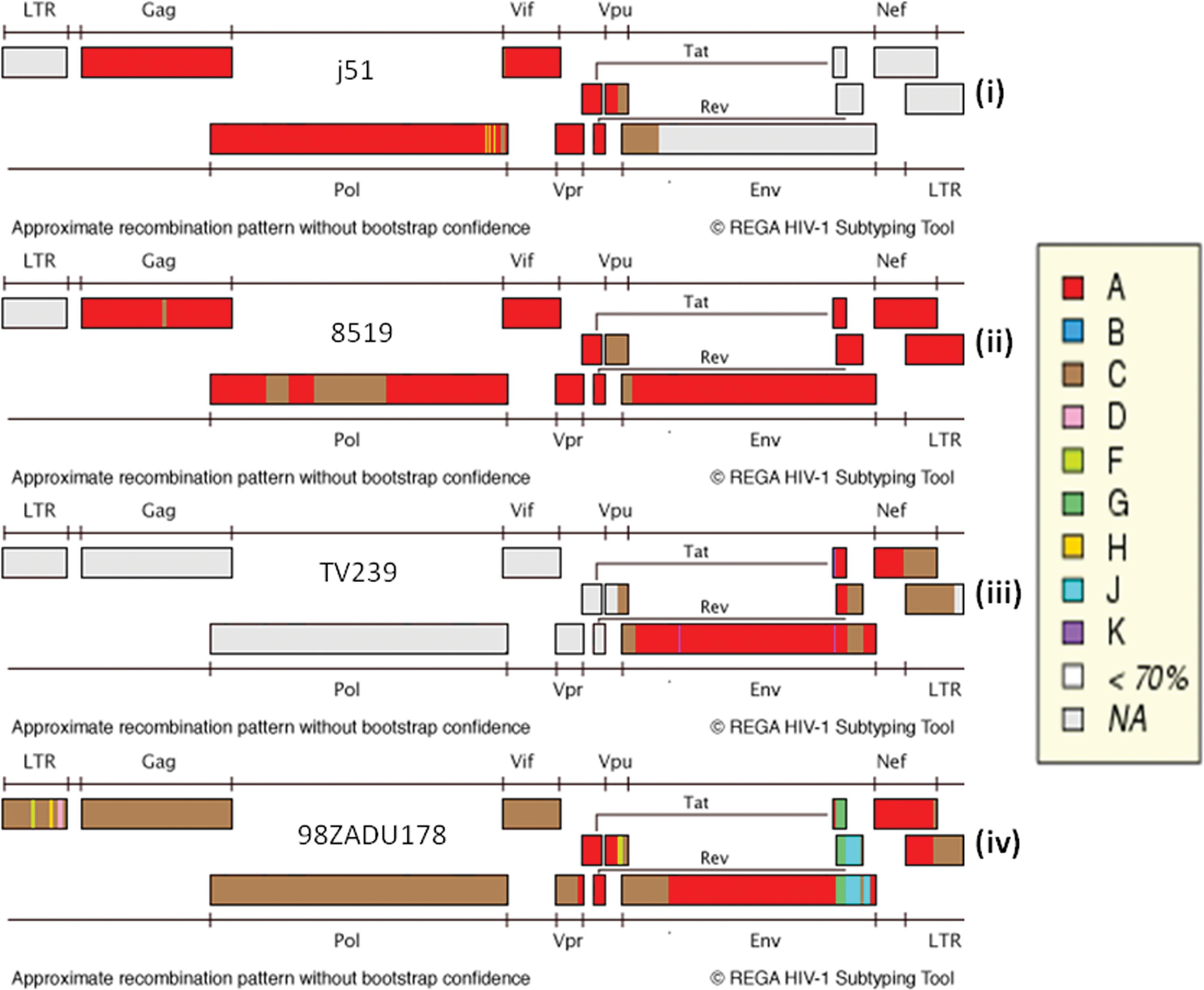
Approximate recombination pattern analysis using the REGA HIV-1 subtyping tool without bootstrap confidence.
There were no drug resistance-associated mutations on the protease, reverse transcriptase, or integrase genes. The sequences revealed other mutations that do not influence drug susceptibility (data not shown).
This study describes the genetic constellation of a unique HIV-1 recombinant isolate from a heterosexual female from rural South African who was referred to a tertiary hospital. To date, isolation of HIV-1 recombinant and or non-subtype C strains has mainly been reported in cosmopolitan urban cities. 8,16 In investigating the importance of HIV-1 subtype differences in drug resistance, Lessells et al. 10 concluded that although there is no compelling evidence that the HIV-1 subtype needs to be considered in choosing ART regimens for first-line or second-line therapy, subtype differences may play a role in assessing the response to treatment and surveillance for the transmission of resistance.
In South Africa, HIV subtype reports indicate an almost 100% HIV-1 subtype C dominance. 2,4,5,18 However, there have been rare reports of pure HIV-1 non-C and recombinant strains. 8,16 –18 In drug resistance analysis of the sequences in an HIV genetic diversity study, the isolate from patient j51 was reported to have no drug resistance-associated mutations, but was classified as HIV-1 subtype A1 on both the PR and RT regions. The recombination event was estimated to have occurred around sequence position 6035±15 bp with reference to the beginning of the HIV HBX2 strain (Fig. 3A). The individual genes were then defragmented with the aid of the HIV sequence locator tool on the HIV sequence database. Analysis of the individual gene fragments showed that the vif, vpr, tat, and rev genes were HIV-1 subtype A1 (Table 1). The vpu gene was assigned to HIV-1 subtype C with a posterior probability of 1.0 on jpHMM (Fig. 3B).
Iweriebor et al. 18 described an A1/C strain isolated from a patient from Belabela in Limpopo, about 200 km from Lephalale (Ellisras) where the study patient resides. The isolate had six recombination breaking points while the isolate from the patient in this study had 1 recombination breaking point within the amplified genome region (Fig. 5). Comparison with other isolates reported to have an HIV-1 subtype A/C backbone from South Africa 16,18,19 revealed that the study isolate was a unique virus. Nonetheless, all the South African A/C isolates revealed a common recombination with HIV-1 subtype C within the vpu gene (Fig. 5). The epidemiological implications of this strain isolation in this region is not known.
Movement of people and interaction with foreign nationals coming from regions dominated by different HIV subtypes have been noted in the emergence of uncommon HIV subtypes and recombinant strains. 2,12 The travel history and other possible contributing factors that could expose the patient to non-C strains could not be ascertained from the available patient's records. Furthermore, this study did not establish whether the infection was of a recombinant strain or whether the patient was coinfected with pure HIV subtypes C and A parental strains that recombined in this patient. Nonetheless, since population-based sequencing was used, the recombinant strain appeared to be the dominant isolate.
Although Lessells et al. 10 alluded to the fact that there is insufficient evidence to contraindicate the HIV-1 group M subtype difference in the choice of an ART regimen, it is important to note the complications that may arise due to subtype recombination. Palm et al. 11 revealed an increased risk of AIDS and AIDS-related deaths in patients infected with an HIV recombinant A3/02 strain rather than their parental strains. This emphasizes the need for continual surveillance of HIV genetic diversity to aid in management, diagnosis, and prevention strategies.
In conclusion, the isolation of a unique recombinant HIV strain in a predominantly HIV-1 subtype C region is indicative of the spread of new HIV strains into rural South Africa. The implications of infection with recombinant HIV strains are poorly understood, emphasizing the need for continued surveillance of circulating strains in endemic regions.
Sequence Data
The genomic sequence of the study isolate has been deposited in GenBank and assigned accession number KM272944.
South Africa sequences downloaded for comparison with the study isolate were retrieved from GenBank using accession numbers AF411965.1, FJ647147.1, and GU201611.1.
Footnotes
Acknowledgments
This project was supported by grants from the Poliomyelitis Research Foundation, National Research Foundation, and National Health Laboratory Service Research Trust (all from South Africa). A.M. Musyoki was supported by bursaries from PRF, NRF, and the University of Limpopo. We thank Ms. Edina Amponsah-Dacosta for proofreading the manuscript.
Author Disclosure Statement
No competing financial interests exist.