
Abstract
We analyzed the impact of HIV viral load on the performance of a limiting antigen avidity enzyme immunoassay (LAg-Avidity assay) and determined if this assay could be used to identify viral breakthrough. Three groups of samples were tested: (1) 18 individuals (30 samples) previously identified as elite suppressors; (2) 18 individuals (72 samples) who were continually suppressed on antiretroviral treatment (ART) with 1 sample before and 2–6 samples (one/year) after ART initiation; and (3) 20 individuals (179 samples) on ART who had evidence of viral breakthrough (>400 copies/ml) with subsequent viral suppression. Elite suppressors had the lowest LAg-Avidity assay values. Among those who were continually suppressed on ART, 83% (15/18) had LAg-Avidity assay values that decreased over time. Although the LAg-Avidity assay on a single sample cannot identify when a viral breakthrough occurs, paired longitudinal samples could identify viral breakthrough (sensitivity: 65%, specificity: 84%).
C
Cross-sectional incidence assays, specifically the LAg-Avidity, have been shown to misclassify individuals infected >2 years who are virally suppressed as recently infected. 5,6 The antibody response to HIV (both titer and avidity) in individuals who start antiretroviral treatment (ART) early in HIV infection (<12 months) is often reduced. 8 In contrast, individuals who start ART later in the course of infection have varied antibody responses, where titer decreases but avidity remains high. 9 We previously demonstrated that these variations in antibody response resulting from changes in viral load can be detected using serologic assays developed for HIV incidence estimation. 10 For example, the BED-CEIA measures the proportion of IgG that is HIV specific; results obtained with this assay vary in response to fluctuations in viral load. 10 In contrast, antibody avidity does not appear to be influenced by fluctuations in viral load. 10 We now present the LAg-Avidity results on this highly curated sample set and determine if viral breakthrough can be identified using this commercially available serologic assay.
Viral breakthrough occurs when a previously virally suppressed individual has detectable virus resulting from the appearance of a drug-resistant variant or ineffective treatment. Current available methodology to determine viral suppression is viral load testing. However, viral load testing requires expensive equipment and laboratory expertise, making it difficult to perform in many resource-limited settings. Less expensive simple laboratory tests are needed for monitoring in these areas. In this study, we evaluated the performance of a LAg-Avidity assay in individuals with natural and drug-induced viral suppression and viral breakthrough. In addition, we evaluated whether this assay could be used to detect viral breakthrough in individuals on ART.
Study participants were enrolled in the Johns Hopkins HIV Clinical Practice Cohort
11
or Elite Suppressor Cohort at Johns Hopkins University in Baltimore, Maryland.
12
These individuals were infected for >2 years and were likely infected with HIV-1 subtype B.
13
Three groups of individuals were assessed: (1) 18 individuals (30 samples) previously identified as elite suppressors; (2) 18 individuals (72 samples) on ART with 1 sample before and 2–6 samples (one/year) after ART initiation; and (3) 20 individuals who were virally suppressed on ART [179 samples, spaced an average of 189 days between visits [interquartile range (IQR): 177–335 days)] who had evidence of viral breakthrough (>400 copies/ml) with subsequent viral suppression. Twelve of the elite suppressors had paired samples (mean time between collection: 41 months, range: 8–51 months). All individuals provided written informed consent, and the study was approved by the Institutional Review Board of the Johns Hopkins University. The LAg-Avidity assay was performed according to the manufacturer's instructions (Sedia Biosciences Corporation, Portland, OR;
LAg-Avidity assay values were highly correlated within a given individual. The median OD-n difference between paired samples was 0.20 [IQR: 0.10–0.32 OD-n]. In contrast, the median OD-n value for all samples from the 18 elite suppressors was 2.77 (IQR: 1.11–4.35). Among elite suppressors, 7/18 individuals (13/30 samples) had LAg-Avidity assay values ≤1.5 OD-n. Of these seven individuals, six had paired samples, where both samples had values <1.5 OD-n.
Among the 18 individuals who were on ART, LAg-Avidity assay results decreased in 15 individuals after 1 year of treatment. For these 15 individuals, the median rate of decrease in assay values was 0.28 OD-n (range: 0.03–0.56) per year on ART. The net decrease averaged 0.48 OD-n (range: 0.15–1.4) for these individuals for the duration of observation.
Among individuals with viral breakthrough, the majority (15/20) had an increase in LAg-Avidity assay results at the time of viral breakthrough; the LAg-Avidity assay result returned to the prebreakthrough value when viral suppression was re-established. The 15 individuals with this pattern of test results had a median increase of 0.45 OD-n (range: 0.12–1.40) at the time of viral breakthrough. The other five individuals had two different patterns of test results. Three individuals with viral breakthrough had a LAg-Avidity assay value increase at the visit after viral breakthrough with a median increase of 0.44 OD-n (range: 0.1–1.15). The other two individuals had no change in LAg-Avidity assay results.
The difference between the OD-n values for individuals who were and were not virally suppressed was analyzed and evaluated. We analyzed the change in OD-n values in longitudinally paired samples, where individuals were suppressed at both time points (n = 120) or at only one time point (n = 22) (Fig. 1). There was a significant difference in the change in OD-n value comparing those suppressed at both time points with those suppressed at time point 1 but not suppressed at time point 2, and between those who had discordant suppression at time point 1 and 2 (p < .001, Fisher's exact test). Using an increase of 0.2 OD-n between paired time points as a cutoff, the sensitivity and specificity of detecting viral breakthrough using the LAg-Avidity assay were 65% (95% CI: 41–83) and 86% (95% CI: 78–92).
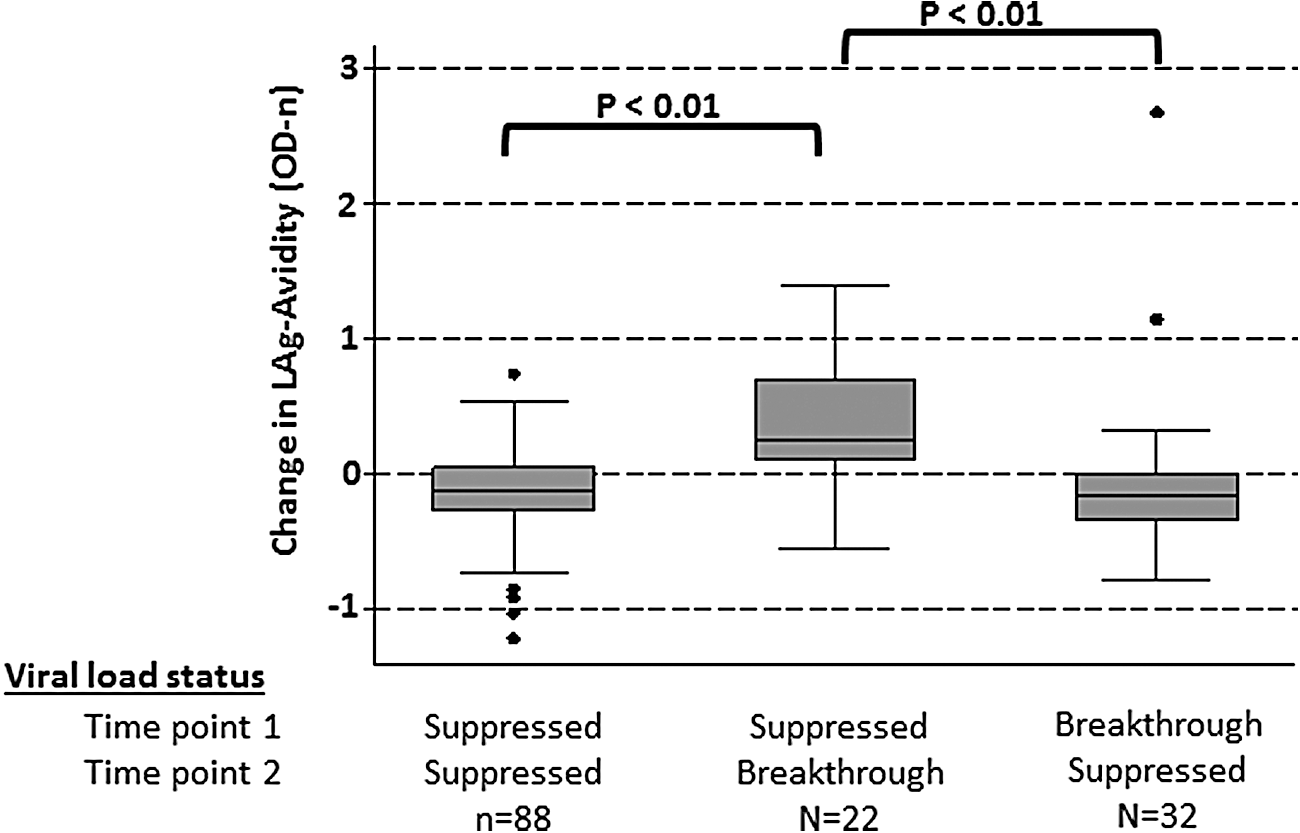
Change in LAg-Avidity assay values in paired samples by viral load status. Box plots show the change in normalized optical density (OD-n) values obtained with the LAg-Avidity assay OD-n values. Test results were compared for paired samples from individuals who were virally suppressed at both time points, at the first time point only, or at the second time point only. p values compare viral load results obtained for the different participant groups.
This study demonstrates that viral breakthrough is associated with a reduction in LAg-Avidity assay results within this observed population. In addition, elite suppressors have a high rate of misclassification with the LAg-Avidity assay. Longer duration of ART was also associated with decreased OD-n values. These observations are consistent with previous studies evaluating the impact of viral suppression on the BED-CEIA. 10 This may reflect the fact that the LAg-Avidity assay and BED-CEIA use nearly identical target peptides. 3,5 Although the LAg-Avidity assay has a lower rate of misclassification than the BED-CEIA among elite suppressors and has a lower median decrease in OD-n values in virally suppressed individuals, the Lag-Avidity assay and BED-CEIA have similar patterns of misclassification in individuals with viral suppression and viral breakthrough. These results are supporting previously published data that suggested LAg Avidity fluctuated with viral load. 15 While LAg-Avidity assay does not accurately identify individuals with viral breakthrough using a single sample, it can be used to identify viral breakthrough using longitudinal samples in most cases.
Footnotes
Acknowledgments
This work was supported by the Division of Intramural Research, National Institute of Allergy and Infectious Diseases (NIAID), and National Institutes of Health, (NIH). Additional support was provided by the HIV Prevention Trials Network (HPTN) sponsored by the National Institute of Allergy and Infectious Diseases (NIAID), National Institutes of Child Health and Human Development (NICH/HD), National Institute on Drug Abuse (NIDA), National Institute of Mental Health, and Office of AIDS Research, of the NIH, Department of Health and Human Services (UM1-AI068613), and by 2R01-AI095068-05. The Johns Hopkins HIV Clinical Practice Cohort was supported by NIDA (R01-DA-11602), National Institute on Alcohol Abuse and Alcoholism (R01-AA16893), NIAID (R01-AI-80328), and NIAID (R24-AI-067039).
Author Disclosure Statement
No competing financial interests exist.