
Abstract
For persons at risk of HIV infection who practice receptive anal intercourse (RAI), topical rectal microbicides represent a promising option for coitally dependent protection. The study compared colorectal distribution and user sensory experiences of two different volumes of rectal gel for suitability as rectal microbicide. Eight HIV-negative men with a history of recent RAI were enrolled into a two-period, sequence-randomized dosing study comparing 3.5 and 10 ml of radiolabeled (1 mCi 99mTc-DTPA) universal placebo, hydroxyethyl cellulose gel. Each participant received two doses in the research unit, one of each volume, separated by a washout period of at least 2 weeks. Each research unit dose was followed by a self-administered take-home dose in the context of preparing for RAI. Safety and gastrointestinal distribution were assessed after the research unit doses, safety, perceptibility, and acceptability, were assessed after take-home doses. There were no adverse effects of Grade 2 or higher and all resolved spontaneously. Both volumes were well tolerated and received high acceptability scores. Perceptibility scores showed meaningful effect size differences ranging from Cohen's d = 0.5 to d = 1.2. The 3.5 and 10 ml gel volumes distributed similarly (p > .2) within the rectosigmoid, ranging from 0.69 to 18.84 cm and 1.21 to 19.01 cm from the anorectal junction, respectively. Both volumes covered the typical gastrointestinal distribution of ejaculate following simulated intercourse based on other studies. Either of these gel volumes could reasonably be pursued for the next phase of development of rectal microbicides.
Introduction
T
Topical microbicides are products formulated for rectal or vaginal application to protect against sexually transmitted infections, including HIV. Several trials have shown that vaginal antiretroviral-containing gels and rings have modest efficacy in preventing the acquisition of HIV in women when adherence is good. 4 –8 Efficacy of rectal microbicides has not been evaluated in clinical trials, but they represent a promising option for the prevention of HIV acquired through receptive anal intercourse (RAI).
FDA guidance from 2014 on the development of microbicides for the prevention of HIV underlines the importance of testing not only the active pharmaceutical ingredient (API) in microbicides but also the optimal formulation for its delivery. 9 This is especially important given the finding that hyperosmolar lubricants and enemas may damage the colonic epithelium and potentially increase the risk of HIV acquisition. 10 –12
Many formulation factors might influence vehicle distribution within the distal gastrointestinal tract, including rheology, viscosity, osmolality, pH, and excipient content of the gel vehicle. These same factors impact sensations experienced by users and their sexual partners (i.e., perceptibility) and, as such, may impact acceptability and use. The effect of product volume on distribution has previously been assessed in gel and enema studies using larger volumes of gel with widely varying viscosities. 13 –20 One study found no difference in retrograde colonic distribution of 20 and 80 ml of rectally administered, radiolabeled ropivacaine gel. 13 Another study that examined a hypoosmolar product (FemGlide, 32 mOsm/kg) in men who practice RAI assessed the acceptability of four escalating volumes of a placebo gel from 5 to 50 ml and established that the maximum acceptable volume for use during RAI was 35 ml. 21
Efficacy is critical, but not sufficient, for real-world use. To effectively prevent disease, rectal microbicides must be acceptable to the user and used consistently in the context of sexual risk. Previous work has shown that users can discriminate between, and form preferences for, formulations with different physicochemical properties as a function of the sensory experiences elicited by specific formulation properties (e.g., viscosity and rheological performance). 22,23 User sensory perceptions and experiences (USPEs) of applying and using products during rectal sex will likely impact willingness to use rectal products among those at risk for HIV.
The intent of the present study was to evaluate the distribution and user experience of smaller volumes, less than or equal to 10 ml, because these volumes are more easily portable than larger volumes and consistent in size with commercial sexual lubricants. Furthermore, in our prior experience, 10 ml volumes have been shown to distribute within the rectosigmoid to distances consistent with HIV surrogate distribution (cell-free and cell-associated HIV surrogates) within autologous semen following simulated intercourse. They also demonstrate near complete overlap in distribution with microbicide gels in clinical mixing studies where a candidate microbicide is dosed before simulated rectal sex with ejaculation. 24 –28
In contrast, many other rectal HIV microbicide development studies have used a 3.5–4 ml gel volume commonly used in vaginal HIV microbicide studies and often with the same vaginal applicator. 29 –31 The 3.5 ml volume approximates that of vaginal dosage forms used in other clinical settings, is also a well-tolerated volume, and is sufficiently smaller than 10 ml so that we anticipated an ability to show a difference in distribution.
Universal placebo (hydroxyethyl cellulose [HEC]) was chosen as the test vehicle as it is readily available, isoosmolar (298 mOsm/kg), previously demonstrated to be safe and acceptable to both vaginal and rectal mucosa, and allows direct comparison of the effects of volume on distribution of the same product within the same study. The isoosmolar HEC was selected to avoid toxicity to the rectal mucosa as seen for hyperosmolar formulations as well as possible negative effects on mucus production induced by hypoosmolar products as seen in some experimental models. 12,32 Furthermore, relevant to the choice to study an isoosmolar gel is the desire to minimize reduction in intraluminal gel volume anticipated with hypoosmolar formulations or increase in gel volume with a hyperosmolar formulation, either of which might affect the colonic distribution of the product.
The study explored the potential differences in rectal distribution due to these relatively small gel volumes to guide subsequent rectal microbicide development studies.
Materials and Methods
Study design
A two-period, randomized, sequential, rectal dosing study was performed, comparing two volumes (3.5 ml vs. 10 ml) of universal placebo gel. Subjects received one dose of each volume mixed with 99mTc-radiolabeled diethylene triamine pentaacetic acid in the research unit and one nonradiolabeled take-home dose for dosing at home in the context of RAI. Participants were provided with and told to self-administer an isoosmolar preparatory enema (normal saline at a volume of 125 ml) at least 8 h before the start of dosing. For ease of initial insertion of the tip of the applicator, a 0.1 oz. packet of lubricant was provided to participants for home use and was also used for the Research Unit doses. However, no additional lubricant was provided to the participants for home use to minimize confounding variables.
Participants were instructed to do what they normally would do in preparation for RAI, including using lubricant if that was part of their routine practice. For Research Unit doses, study staff administered the study product to participants using a 10-cm syringe attached through Luer lock to a rectal applicator (Northern Pharmacy and Medical Equipment, #001-921-6670); doses at home were self-administered by participants using the same applicator, Figure 1.
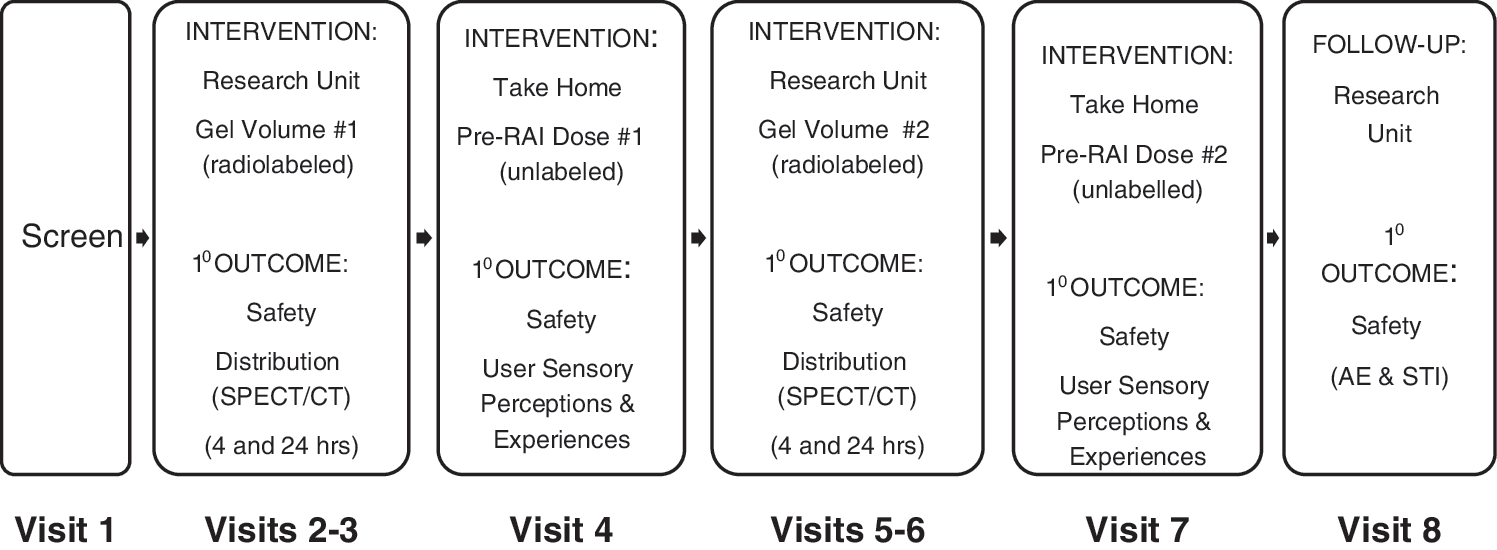
Study schema.
The sequence of volumes was randomized to minimize bias stemming from participants' or staff's anticipation of the sequence of volumes, but could not be blinded. Healthy HIV-uninfected men reporting a history of RAI were enrolled; this population was most likely to have opportunities for product use in the time frame prescribed by the protocol and their past experience provided a context for USPE and willingness to use assessments.
Women were not eligible as the focus of this work was on MSM who are the primary, although not only, target group to use rectal microbicide products. Limiting the study to MSM over age 18 also enabled comparisons with our previous enema study results, which were all in adult men, without the potentially confounding sex- and age-related variables (hormonal influence and anatomic differences.) In addition, the very small sample size in this study was felt unlikely to tolerate well the potential for additional variability introduced by anatomic, hormonal, and age-related differences. The Johns Hopkins Medicine Institutional Review Board approved the study and all participants provided their written informed consent to participate in the study before being screened.
Imaging colon distribution of study product
Following each research unit dose of product, one Single Photon Emission Computed Tomography/Computed Tomography (SPECT/CT) imaging study was performed 4 and 24 h after dose administration using a dual-head Millennium VH SPECT/CT system (GE Medical Systems, Waukesha, WI) equipped with a CT unit (Hawkeye). By predetermined plan, it was agreed to stop performing 24-h scans if there was inadequate colonic signal at that time point in the first few participants. All assessments of colonic distribution of gel in this study were made based on the 4-h scans.
As previously detailed, a filtered back projection algorithm was used to reconstruct CT images onto a 256 × 256 matrix size. SPECT images were then attenuation corrected and reconstructed using the ordered subset expectation maximization algorithm and fused with the CT images into a 128 × 128 × 128 matrix size, with each voxel representing 3.45 mm3. This reconstruction was performed using the General Electric Xeleris workstation, software version 3.0 (GE Medical Systems, Waukesha, WI). 25,28,33,34
A flexible principal curve algorithm in R, version 3.2.0 (The R Foundation for Statistical Computing, Vienna, Austria), was used to construct a three-dimensional curve through the colon images, as previously described. 35,36 First, the origin and end of the centerline through the signal were established. Next, a centerline was fit to the signal using a principal curve algorithm, after which a concentration-by-distance curve was constructed based on voxel intensity within a 1 cm radius disc orthogonal to the centerline. Finally, concentration-by-distance curves were generated, with counts per minute in each one-voxel-thick orthogonal disc being the concentration equivalent for this analysis.
To enable a common frame of reference across studies, the axial distance from the anorectal junction (set as distance equal to zero) to the beginning of the centerline was added to the concentration–distance curve. The z-axis location of the anorectal junction was identified as the slice that contained the puborectal sling distal to the most distal air-filled section of rectum.
Pharmacokinetic-distance parameters were calculated using Phoenix WinNonlin software (Certara, LP), as previously described. 36 Briefly, Dmin is the most distal signal in the body, calculated as the distance between the anorectal junction and the origin of the radiolabeled centerline. Dmax is the distance furthest from the anorectal junction (most proximal) at which signal is detected, DCmax is the distance at which maximal signal intensity is found, and Dave is the mean residence distance (area of first moment divided by area of zero moment, similar to mean residence time, but substituting distance for time).
Intraluminal gel retention
Percent of intraluminal gel retention was estimated as the product of (A) percent of gel removed from the applicator, (B) the percent of that removed gel that was applied to the body, and (C) the fraction of gel applied to the body that remained inside the colon (i.e., was not expelled). Dosimetry determined radiation on gloves, chux, dosing syringe, and other supplies for calculation of A and B. C was determined by SPECT/CT region of interest assessment of intraluminal distinct from extracorporeal signal.
Perceptibility and acceptability
To assess perceptibility, each participant completed a USPE survey—one after RAI with the 3.5 ml volume gel and one after RAI with the 10 ml volume gel. The USPE surveys included questions about sexual behavior (e.g., sexual sequencing, whether the insertive partner used a condom) and items assessing various aspects of the user's sensory experience (USPEs: see table for descriptions of sensations captured by each USPE scale). Likert-type items were rated to assess the level of agreement with each particular item from (1) do not agree at all to (5) agree completely. We conducted both in-depth and cognitive interviews to adapt the items from the vaginal to the rectal compartments and to characterize new concepts (e.g., bloating) that participants noted are relevant to rectal sex. From these items, we calculated averaged scale item scores using scales previously validated for vaginal sex. 22,23,37
To assess acceptability, we asked participants first to rate the likelihood that they would use either product (i.e., the 3.5 and 10 ml products) to prevent against HIV on a five-point Likert scale assessing definitely NOT, probably NOT, unsure, probably, or definitely. We also asked participants to select which of the two volumes they would choose to use if they had to pick a single product.
Statistical analysis
Distribution parameters and retention results for the 3.5 and 10 ml volumes were summarized using descriptive statistics and compared using the Wilcoxon signed-ranks test with a p-value less than .05 considered statistically significant (Stata Intercooled 13.1 for Windows, StataCorp LP, College Station, TX). Results were plotted with SigmaPlot 13.0 (Systat Software, Inc., San Jose, California). Principal component analysis was conducted using IBM SPSS Statistics for Windows, Release 20.0.0 (©IBM Corp., 2011, Armonk, NY,
Results
Subjects
Nine healthy, HIV-seronegative, male research participants were enrolled in the study. One of these subjects discontinued the study early after receiving only one study gel volume due to intercurrent illness deemed by site investigators and the DSMB to be unrelated to the study product; this subject's safety data were included in the analysis, but the SPECT/CT and USPE data were excluded because they were incomplete. Eight male subjects with a median age of 44 years (interquartile range [IQR] 29.2, 49.8) completed all study visits. Research participants self-identified as white (4) and African American (4); none indicated that they were Hispanic.
Safety
A total of 13 unique adverse events (AEs) were reported by a total of six subjects. Five of these AEs were deemed to be related to the product and occurred in a total of two subjects, and all of them were mild (Grade I) and resolved without intervention. The AEs included anorectal pain related to RAI in the absence of lubricant, constipation, tenesmus, mild rectal discomfort associated with constipation, and bloating, Table 1.
Perceptibility and acceptability
Eight participants completed perceptibility (i.e., sensory experiences) and acceptability (i.e., willingness to use) surveys following take-home doses. A final preference survey comparing volumes was completed after the second take-home dose. The USPE sexual activity scales performed well when adapted to the receptive intercourse experience, both on an individual item level and with respect to internal consistency indices for the scales. CCA values for the USPE scales ranged from 0.62 to 0.98 for the 3.5 ml gel and 0.56 to 0.95 for the 10 ml gel, where values <0.60 indicate poor reliability, values .60 to <0.70 are acceptable, above >0.70–<0.80 are considered good, >0.80–<0.90 very good, and >0.90 excellent. 40,41
Several scales showed conceptually consistent findings in volume comparisons. In reviewing the data conservatively (avoiding high interitem correlations and missingness) and only reporting here those scales that have moderate to large preliminary effect sizes (i.e., d > 0.40), we found the following scales had higher averaged scale item scores for the high-volume gel: Application (APP): Leakage, SEX: Spreading Behavior, SEX: Messiness, SEX: Product Awareness, and SEX: Leakage. To the contrary and equally consistent conceptually, SEX: Naturalness and SEX: Perceived Wetness had higher averaged scale item scores for the low-volume gel.
These scores reflect hypothesized relationships between volume and sensory experiences elicited by those gel volumes, with the high-volume gel being rated as spreading more, being more messy, and leaking more, and the low-volume gel feeling more like typical RAI (where lubricants usually are of lesser volume and are applied externally). The SEX: Pleasure and SEX: Stimulating scales also exhibited conceptual consistency, with higher endorsement of pleasure for the participant and partner with the higher volume gel, although both averaged scale item scores were below 2.0 (agreeing a little). See below table for specific details.
When asked to focus on the sensory experience of each product during RAI, four participants responded that they would definitely use either product to reduce their chance of getting HIV. Two responded that they would probably use either product. One participant was unsure of his willingness to use either product. Furthermore, when asked which of the two volumes they would choose to use for HIV prevention if they had to choose one, five of eight chose the 3.5 ml volume, while three of eight chose the 10 ml volume, Table 2.
Rectal USPE scales not included (data not shown): APP: Ease, APP: Discreet-Portable, APP: Product Awareness, SEX: Initial Penetration, SEX: Initial Lubrication, SEX: Lubricity, SEX: Effortful, SEX: Noticeable.
Columns 2 and 3 contain means with standard deviations in parentheses and Cronbach's coefficient alpha in brackets; column 4 contains the adjusted Cohen's d effect size using the correlation between measures with the Cohen's d effect size in parentheses computed with no correlation; column 5 is the p-value for each analysis. Effect sizes of d = 0.2, d = 0.5, and d = 0.8 are considered, respectively, as small, medium, and large.
APP: application experience scale.
Denotes very high correlation (>0.80) that greatly increased analysis effect size and may not be stable.
SEX: sexual activity experience scale.
Denotes negative correlation between measurements that reduced analysis effect size.
One item removed from scale construction because seven of eight participants in high-volume condition had missing data on this item. This resulted in a three-item scale used to compare groups.
CCA, Cronbach's coefficient alpha.
Gel volume retention
After the first four subjects were scanned, it was apparent that no radiolabel remained in the colon 24 h after dosing and therefore as prespecified in the protocol, no further scans were performed at the 24-h time point; 7 of 16 (43.8%) originally planned 24-h scans were performed in four subjects. The applicator delivered a slightly greater but statistically significant percent of the 10 ml dose intracolonically, median 94.8% (range 93.8%–95.6%), when compared with the 3.5 ml dose, 88.6% (range 81.9%–90.2%), using the Wilcoxon matched-pairs ranked-sum test (p = .012).
Luminal distribution
There were no significant differences in the four pharmacokinetic distance parameters between the 10 ml volume and the 3.5 ml volume of gel (Fig. 2; all p-values > .05, paired Wilcoxon rank sum test). Median Dmin was 1.21 cm (range −0.69–4.49 cm) for the 10 ml volume and 0.69 cm (range 3.05–2.76 cm) for the 3.5 ml volume; Dave was 9.18 cm (8.13–12.67 cm) for the 10 ml volume and 9.6 cm (7.95–17.44 cm) for the 3.5 ml volume; DCmax was 10.28 cm (5.67–17.27 cm) for the 10 ml volume and 11.62 cm (5.22–18.21 cm) for the 3.5 ml volume; and Dmax was 19.01 cm (17.36–47.48 cm) for the 10 ml volume and 18.84 cm (16.71–35.56) for the 3.5 ml volume, Figure 2.
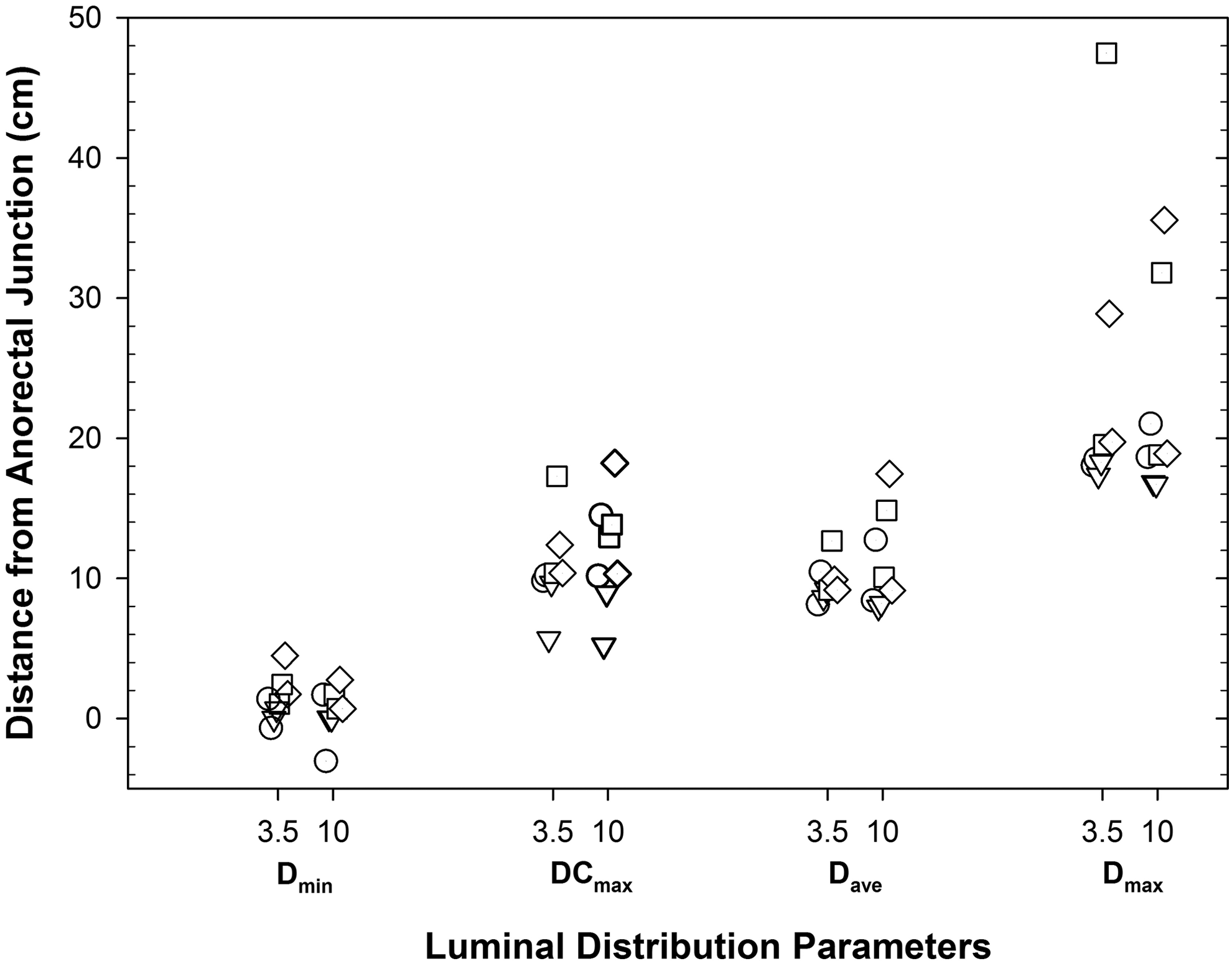
Pharmacokinetic distance parameters (distance from anorectal junction) for two volumes (3.5 and 10 ml) of HEC Gel delivered through applicator. Dmin is the most distal location at which signal is detected, Dmax is the most proximal location of signal detection, DCmax is the distance at which maximal signal intensity is found, and Dave is the mean residence distance. All distances are relative to the anorectal junction (distance equals zero) with progression proximally defined as a positive direction. Each symbol represents one individual subject. HEC, hydroxyethyl cellulose.
Discussion
This study evaluated two rectal gel volumes using luminal distribution of radiolabeled gel at 4 h, safety assessments, perceptibility assessments, and acceptability assessments and found that there were no statistically significant differences in any of these measures. The slight difference in the percent of gel dose retained internally between the two volumes is partly explained by the larger percentage of the dose in dead space for the smaller volume syringe. The distributions seen in this study are consistent with our past work, which has demonstrated that isoosmolar gels tend to distribute proximally to 20 cm by 2 h after dosing and migrate slightly more distally by 4 h after dosing. 42
The present study examines luminal distribution as the initial drug distribution step, which largely determines secondary distribution of drug into adjacent colonic tissue. Adequacy of luminal distribution has been assessed in two ways: luminal centerline distribution of HIV surrogates alone after simulated anal sex and by in vivo mixing experiments in which microbicide candidate dosing is followed by simulated ejaculation of viral surrogates and coincident distribution is assessed.
Distribution of both the 3.5 and 10 ml HEC gel volumes in this study is consistent with the luminal centerline distribution of the cell-free and cell-associated HIV surrogates in autologous semen after simulated anal sex in prior work 25 and in prior studies using 10 ml gel volumes. In those studies, HIV cell-free surrogate was observed to colocate almost completely (86%) with a rectal microbicide vehicle when examined on an SPECT voxel-by-voxel basis indicating substantial intraluminal mixing. 27 It is our suspicion that with 3.5 ml volumes, while overall luminal distribution may be the same, the mixing with as much as a 2.5 ml ejaculate in the lumen is less effective than with a 10 ml volume.
Among other important study limitations, the product examined vehicle only without API. This also prevented our assessment of tissue API concentrations. In particular, tissue drug concentration and homogeneity in the region of expected HIV distribution would be highly influential in rectal microbicide product development and are influenced by more variables than luminal distribution alone.
As mentioned, this study was performed only in adult men. While the ultimate goal of developing an effective HIV microbicide would be to develop a product for women and adolescents too, and for dual compartment use, the goal of this study was to describe the rectal distribution of differing volumes of universal placebo. There is a crucial need to involve women and adolescents in future clinical development where inclusion is more statistically sound, with larger sample sizes, and where planned comparisons between genders and across the age spectrum can be performed.
This is the first study to use perceptibility (USPE) measures for product evaluation in RAI. Differences of half a standardized deviation or greater were noted in a subset of user sensory perception and experience (USPEs) scales between the volumes experienced in this sample, but given the small sample size, statistical power was low, and comparisons in USPE scale scores should be interpreted as preliminary.
In general, effect sizes for behavioral measures are typically in a medium effect size range (i.e., d = 0.50) and require larger samples to be adequately powered to achieve statistical significance. 43 However, averaged USPE scale item scores show little differences in the sensations participants felt when evaluating the two volumes of gel. These perceptibility responses suggest that both volumes of gel elicit similar sensory experiences. When perceptibility responses are aligned with the acceptability (i.e., willingness to use) responses, and with the imaging data, the overall interpretation of the data suggests that either volume could be tolerated and would likely be used in similar participants.
Larger psychometric validation studies would allow for more robust analyses of user sensory experience patterns that could further delineate which product properties, including volume, will most consistently and clearly predict user sensory experiences and practices. Subsequent studies with larger sample sizes could add great value in using USPEs to better understand the relationship between product properties, USPEs, drug delivery, acceptability, and use.
Overall, our study suggests that both volumes of HEC universal placebo gel administered rectally are safe and well tolerated by participants, consistent with numerous prior studies of a variety of gels. Furthermore, both of these volumes distribute in the same manner within the distal colon. Fundamental questions of tissue concentrations of API and their persistence, luminal mixing of microbicide and virus, pharmacodynamic measures such as antiviral effect, and other formulation factors remain for further study and are active areas of investigation in several ongoing projects within the larger Integrated Preclinical/Clinical HIV Topical Microbicide Program. This study addresses an important pharmaceutical variable in optimizing formulation development of a much needed, safe, effective, and highly acceptable rectal microbicide for the prevention of rectally acquired HIV.
Footnotes
Acknowledgments
The authors gratefully acknowledge the time and contributions of the research participants in this clinical study, the staff of the Drug Development Unit, and the kind assistance of Jeff Leal of the Image Response Assessment Team (IRAT) Laboratory at Johns Hopkins University and Jim Turpin of the Integrated Preclinical/Clinical HIV Topical Microbicide Program. Funding: NIH U19AI101961 Development and Evaluation of Dual Compartment Combination Microbicides; NIH T32 GM066691-11; and GM066691-12, NIGMS.
Disclosure Statement
No competing financial interests exist.