
Abstract
Maintaining optimal adherence to antiretroviral therapy (ART) is essential for optimizing the management of HIV infection. The aim of this study is to explore ART adherence rates in Turkey. Included in this study were a total of 263 HIV-infected patients followed up by the ACTHIV-IST (ACTion against HIV in Istanbul) Study Group affiliated with four tertiary hospitals. The study population included patients 18 years of age or older who were on ART for over 12 months. Adherence was assessed by the medication possession ratio (MPR) calculated for each patient using data (a list of all drugs dispensed within the previous year for that patient) obtained from pharmacy medication records. In addition, patients completed a self-report questionnaire addressing missed doses and the AIDS Clinical Trials Group (ACTG) adherence questionnaire. The study was reviewed and approved by the Ethics Committee of Cerrahpasa Medical Faculty. Patient ages ranged from 19 to 71 years. Two hundred and thirty-one patients were male (88%). Two hundred and twenty-four patients (85%) had optimal adherence (MPR ≥95%). During the course of ART, 236 patients (90%) reported no missed doses in the past 4 days of their treatment, whereas 206 patients (78%) reported no missed doses in the past month. Simply forgetting was the most common reason for nonadherence. MPR was associated with virologic rebound. Major factors affecting adherence were being female, taking antituberculosis drugs, having an opportunistic infection, being able to take all or most of the medication as directed, and being aware of the need to take medication exactly as instructed to prevent the development of drug resistance. Adherence to ART measured by MPR and self-report surveys is relatively high in Turkey when compared with other countries, which probably led to high ART success rates.
Introduction
S
Currently, there is no consensus on the optimal method to estimate adherence to ART. 8
Several self-report methods, pharmacy adherence measures (PAMs), and electronic drug monitoring methods are widely used to evaluate adherence in clinical trials and observational studies. 9 Electronic monitoring is the most objective method, but its use is limited by relatively high cost and inconvenience. 9 –11 Unlike patient self-report methods, PAMs are objective and convenient for routine use and may be calculated from information available in medical and pharmacy records. PAMs are classified into three categories: medication possession ratio (MPR), pill count, and pill pick-up. 12 The self-reported feedback questionnaire is still the most commonly used method due to its low cost and simplicity. 13
Various factors affecting ART adherence have been identified, including primarily substance use, depression, lack of family and social support, side effects of medication, and stigmatization and discrimination. 14 –16
Turkey has one of the lowest HIV/AIDS seroprevalence rates in the world. According to data from the Turkish Ministry of Health in November 2015, about 11,109 people were living with HIV/AIDS in Turkey. 17 HIV/AIDS was first diagnosed in three patients in Turkey in 1985, with a progressive increase in the annual number of cases during the following years. 18,19
A meta-analysis of studies on ART adherence found that 77% of patients in Africa achieved adequate adherence of 95% compared with 55% of patients in North America. 14 Countries in Eastern Europe and in Asia were reported to achieve higher rates of adherence. 14 In the present study, our aim was to investigate the level of ART adherence and causes of nonadherence in Turkey, a country with low HIV seroprevalence.
Methods
The study was conducted cross-sectionally by the ACTHIV-IST (ACTion against HIV in Istanbul) Study Group. A total of 263patients who had received ART for at least 12 months from March 2014 to March 2015 were enrolled. Adherence was measured by a self-report questionnaire, by the AIDS Clinical Trials Group (ACTG) adherence questionnaire and by MPR.
Ethics statement
The study was reviewed and approved by the Ethics Committee of Cerrahpasa Medical Faculty in Istanbul, Turkey. Written consent was obtained from all subjects before initiation of the study.
Study population
The study was conducted at four tertiary hospitals affiliated with the ACTHIV-IST Study Group in Istanbul, Turkey. Patients 18 years of age or older with a diagnosis of HIV/AIDS were enrolled if they were competent and willing to complete study questionnaires, if they were able to speak and understand Turkish, and if they had received treatment for at least 1 year. Pregnant women and patients with concomitant illnesses (dementia, or severe psychiatric or neurological conditions) that could potentially affect the study results were excluded from the study.
Study adherence measures
As an initial method, MPR was calculated for each patient using data (a list of all drugs dispensed within the previous year for that patient) obtained from pharmacy medication records.
MPR = Sum of the number of days'—in which drugs were supplied within the past 12 months (days)/12 months (365 days).
Second, a simple, self-report questionnaire consisting of four questions on medication use was administered to patients. Patients were asked to report whether they had missed a tablet during the past 4 days, within the past 1 week, within the past month, and within the past 3 months. Patients responding “no” to all questions were considered “adherent,” whereas patients responding “yes” to any of the four questions were considered “suboptimally adherent.” As a third method, patients were asked to complete the ACTG Adherence Baseline Questionnaire and the ACTG Adherence Follow-Up Questionnaire provided free of charge by the Center for AIDS Prevention Studies (AIDS Research Institute, University of California, San Francisco, CA). ACTG adherence questionnaires have been used extensively to measure self-reported adherence to ART internationally. In the ACTG questionnaires, patients are asked to apply 1 of 4 options—“never,” “rarely,” “sometimes,” or “often,”—to 14 different reasons for missing a dose (Likert format). This self-report questionnaire included factors relating to missed dosing, substance use and frequency, and sociodemographic characteristics.
The linguistic validation of the Turkish version was done by HIVEND (HIV Enfeksiyonu Derneği). The questionnaires were translated into Turkish and subsequently back translated by a panel of independent experts. After the pretesting and cognitive interviewing process, minor changes were made. The final version was checked and approved by HIVEND's scientific committee.
Patients' epidemiological data, CD4 count, and HIV-RNA levels were obtained from their medical files. The viral loads of the patients were recorded at the time of the questionnaire. A viral load >200 copies per milliliter was considered virologic rebound (VR).
The drugs history of the patients included the nucleoside analogues Tenofovir/Emtricitabine (TDF/FTC), Zidovudine/Lamivudine (ZDV/3TC) or Abacavir/Lamivudine (ABC/3TC), the non-nucleoside analogue agent Efavirenz (EFV), and the protease inhibitors Lopinavir/Ritonavir (LPV/RTV) or DRV/Ritonavir (RTV).
Statistical analyses
Descriptive statistics included the mean, standard deviation, median, lowest and highest frequencies, and ratio values. The Kolmogorov–Smirnov test was used to assess the distribution of the variables. Quantitative data were analyzed using the independent sample t-test, and qualitative data were analyzed using a chi-square test. The SPSS 22.0 software package was used for all statistical analyses. A p-value of <.05 was considered statistically significant.
Results
A total of 263 patients with a mean age of 40 years (ranging from 19 to 71) were enrolled in the study, of whom 231 were males (87.8%). See the flow chart describing participant numbers (Fig. 1).
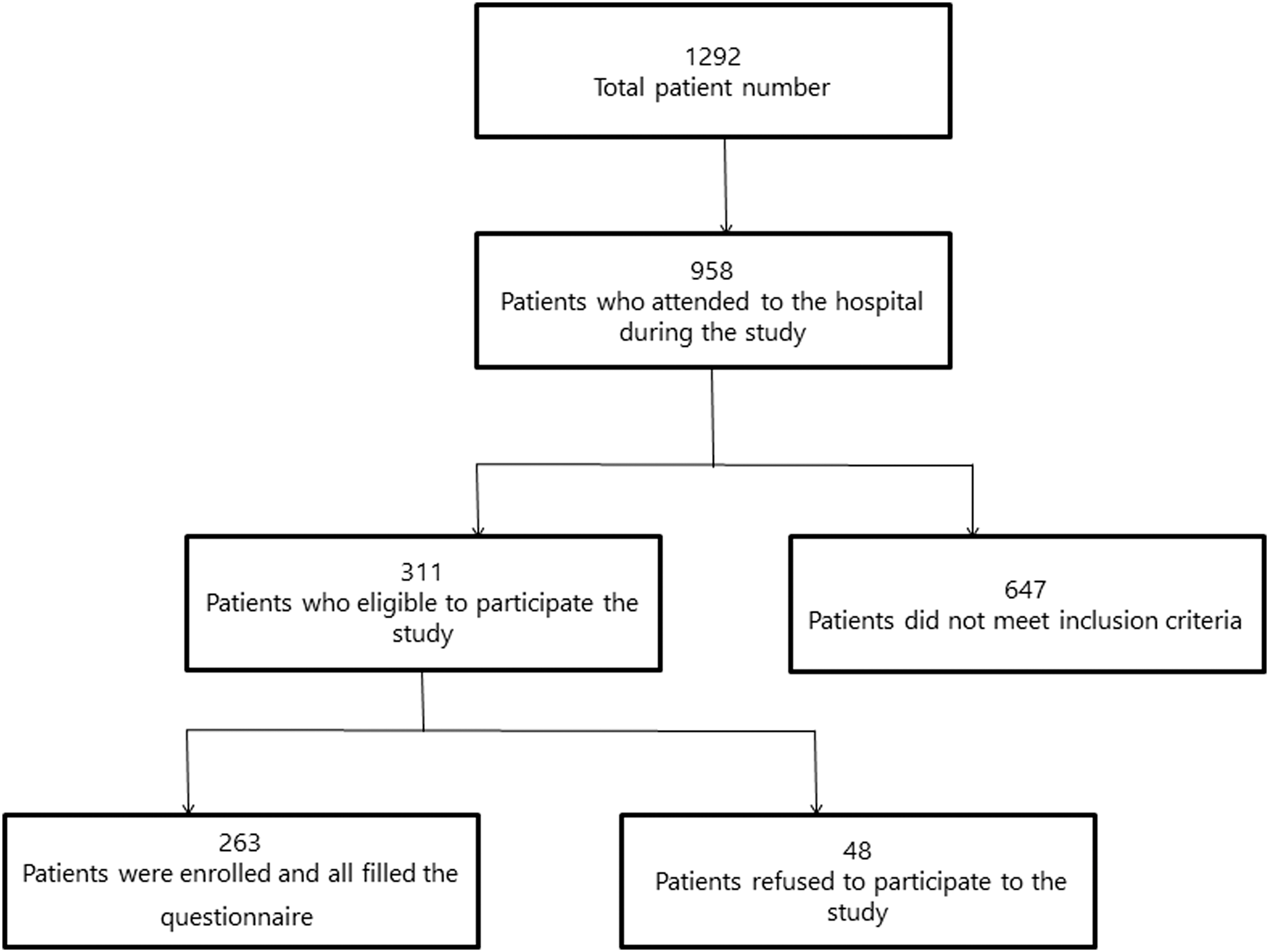
Patient consort flowchart of the study.
Patient sociodemographic characteristics are shown in Table 1. The mean CD4 count of patients was 505 cells/mm3 (range: 2–1,450).
Medical drugs: antihypertensive, antidiabetic, analgesic drugs.
SD, standard deviation.
Table 2 shows adherence as assessed by self-reporting, MPR, and ACTG questionnaires.
ACTG, AIDS Clinical Trials Group; MPR, medication possession ratio.
Table 3 provides the reasons cited for nonadherence as reported by patients through the ACTG questionnaire. Simply forgetting was the most common reason (41%) for nonadherence. Other common reasons included being away from home (29%), experiencing a change in daily routine (23%), and falling asleep or sleeping through dose time (20%).
The nonadherence rate indicated by MPR was significantly greater among patients with VR compared with patients without VR (p < .05). Nonadherence rates estimated by self-reported measures and by the ACTG questionnaire did not differ significantly between patients with or without VR (p > .05) (Table 4).
Bolded values are statistically significant.
Chi-square test.
Distributions of patient age, education level, and employment status were not significantly different between MPR adherent and nonadherent groups and between ACT adherent and nonadherent groups (p > .05). The MPR nonadherent group and the ACT nonadherent group had significantly higher percentages of female patients compared with the MPR adherent group and the ACT adherent group (p < .05) (Table 5).
Bolded values are statistically significant.
The MPR nonadherent group had a significantly lower percentage of patients who reported that they were “sure that if they do not take this medication exactly as instructed, the HIV in their body will become resistant to HIV medications” compared with patients in the MPR adherent group (Table 6).
Bolded values are statistically significant.
Independent sample t-test/chi-square test.
ART, antiretroviral therapy.
The ACT nonadherent group was found to have a significantly higher proportion of patients who were taking antituberculosis drugs, experiencing opportunistic infections, and taking concomitant medication in comparison to the ACTG adherent group (p < .05). Furthermore, the ACT nonadherent group also showed a significantly lower proportion of patients who reported that they were “able to take all or most of the study medication as directed” versus the ACT adherent group. The ACT nonadherent group also had a significantly lower percentage of patients who reported that they were “sure that if they do not take this medication exactly as instructed, the HIV in their body will become resistant to HIV medications” in comparison to the ACT adherent group (Table 6).
Discussion
This is the first study to have investigated adherence to ART in Turkey. In this study, although we found that Turkey had a higher adherence rate compared with rates reported in other Asian countries, it was similar to the adherence rate reported by Wasti et al. in Nepal. 14,15 The high rate of adherence found in Turkey may be explained by the ease of access to ART drugs nationwide, the coverage of these drugs by reimbursement programs for all patients, and the lack of a contribution fee requested from patients for examination and treatment. Other reasons may include the use of self-report measures and MPR as study methods and the inclusion of patients who were provided full care and followed at outpatient clinics.
In the present study, we used three different methods to evaluate adherence to ART and compared the results with VR data. As with similar studies, both MPR and the other PAMs were consistent with virologic failure and VR. 12,20 –24 Thus, MPR may assist in identifying patients currently at risk of VR. MPR is thus predictive in this study, and although it was not shown to be predictive for future outcomes, it can be used to assess adherence as it is a simple and inexpensive method.
Consistent with previous studies, simply forgetting was found to be the most common reason for ART nonadherence (41%). 25,26 Other common reasons included being away from home (29%), experiencing a change in daily routine (23%), and falling asleep or sleeping through dose time (20%). 25,26
Adverse drug effects have been cited as a major reason for nonadherence in some studies. 14,26 However, “wanting to avoid side effects” was cited as a reason for nonadherence only by 7% of patients in the present study. While treatment cost is the key barrier to seeking treatment in other developing countries, it did not emerge as a reason for nonadherence in Turkey because ART is provided through public health insurance to all patients who need it.
Although education level has been reported to be correlated with adherence in several studies, 14,15,27 age, education level, and employment status were not associated with adherence in the current study. Cauldbeck et al. found that education level did not have any effect on adherence, lending support to our findings. 28 This result may be explained by a high level of awareness of ART among the study patients (Table 6).
Adherence rates were lower among females compared with males. This is an important finding that has been shown in only a few previous studies 15 and that may be explained by the poor sociocultural status of women in Turkey. Women have a disadvantaged position in many areas of life compared with men in Turkey, which is a developing country. Acceptance of an HIV diagnosis by women is far more difficult than by men, and women have greater concerns about being stigmatized. Another reason might be women's greater responsibilities for daily household chores.
This study was limited to hospitals located in Istanbul, and study data may not be considered representative of the current situation in other parts of Turkey. However, Istanbul, which comprises more than one-fifth of the general population, is Turkey's most populous city and is home to people of different backgrounds from all geographic regions. Additionally, since a substantial proportion of people infected with HIV live in Istanbul, it is our belief that the study data can be extrapolated to the Turkish population in general.
In the current study, the following factors were found to be significantly associated with ART adherence: female sex, use of antituberculosis drugs, opportunistic infections, sureness that all or most of the study medication can be taken as directed, awareness of that drug resistance could develop if the medication is not taken exactly as instructed, and use of concomitant drugs.
In conclusion, adherence to ART, as measured by MPR and self-report survey questionnaires, is relatively high in Turkey when compared with other countries, which has probably led to Turkey's high ART success rates.
Footnotes
Acknowledgments
This study was supported by the Gilead Sciences Turkey Fellowship Program and HIVEND (Istanbul, Turkey). The authors would like to thank Dr. Berna Ozelgun, MD for her kind efforts and contribution in proofreading of the article.
Author Disclosure Statement
No competing financial interests exist.