
Abstract
Retaining HIV patients in clinical care is a critical component of the HIV care continuum, impacting not only patients' virologic suppression, but their overall health and wellbeing. Understanding reasons for patient drop-out is therefore important to improve HIV outcomes and reduce transmission. This study used qualitative in-depth interviews with patients who dropped out of HIV care (n = 16) from the Atlanta Veterans Affairs Medical Center, to explore their reasons for drop-out and how they negotiate barriers to return to care. Results show three interlinked “pathways” leading to patient drop-out —wellness, illness, and medication pathways. These pathways encompass both barriers to retention and triggers to resume clinic visits, with patients following different pathways at different times in their lives. Perhaps the strongest deterrent to continuing clinic visits was participants' self-perception of wellness, which often outweighed clinical indicators of wellness. These pathways suggest that multiple approaches are needed to improve treatment retention, including reducing clinic-based barriers, addressing basic needs that are barriers to clinic visits, and empowering patients to view clinic visits as a facilitator to maintaining their overall health rather than only a reaction to illness.
Introduction
S
Retention in care (i.e., regular clinic visits) and virologic suppression remain the most critical aspects of the HIV care continuum, as breaks in these links of the chain result in significant morbidity, mortality, and spread of HIV. 9 Although virologic suppression can still occur in the absence of regular clinic visits, 10 with mounting medical comorbidities and potential medication interactions or side effects, these appointments become increasingly important to assist with overall health and wellness management of patients. Therefore, it remains imperative that the medical community have a better understanding of how patients negotiate healthy behaviors and clinic visits within a morass of other competing needs. With a better understanding of this process, more effective strategies can be developed to assist patients.
Currently, healthcare officials, clinical program directors, and clinicians are struggling to improve retention in care for the most vulnerable patients in the healthcare system. Patients who “churn” in and out of care account for only 4.9% of the population in one study, 11 but constitute 16.6% of the community viral load, despite substantial efforts by the patients themselves and the healthcare institutions who have pledged to care for them. These patients face daunting structural barriers such as poverty, inconsistent housing, food insecurity, inadequate transportation, and insufficient education. 12 Additionally, migration, child/family care, employment, frequent hospitalization, intermittent incarceration, and periodic lapses in healthcare access create obstacles to keeping appointments. 13 Finally, psychosocial stressors (e.g., stigma, substance abuse, mental health disorders, distrust, and fear of death) can be paralyzing even in the absence of these barriers. 14,15
Despite these seemingly insurmountable hurdles, many patients reliably adhere to often complicated regimens and make the most of their clinic appointments. 10 Important facilitators of retention include demographic, socioeconomic, and psychological factors, as well as perceived needs of the individual. 16,17 Social capital (relationships and networks) and the impact of the surrounding community are likewise important facilitators. Finally, the healthcare system in particular can promote or hinder retention for a variety of reasons, including the degree of distrust of the healthcare system, 18 satisfaction with the clinic experience, 19,20 and cultural competency of the providers. 21
Despite the wide range of studies describing barriers and facilitators to retention in care, there is less understanding as to how individuals negotiate structural barriers, life circumstances, and perceived needs while making decisions to engage with the healthcare system and prioritize their health. Depending upon how an individual values various aspects of their health in relation to other needs, decisions are made in the context of these “preferences.” To improve retention in care, it therefore becomes critical to understand how individuals view these priorities and what motivates positive behavior.
In this study, we conducted qualitative in-depth interviews with individuals who were no longer retained in HIV care to understand reasons for clinic drop-out and to identify ways to improve retention. This was done in the context of a Veterans Affairs Medical Center (VAMC) HIV clinic, where many of the administrative barriers associated with Ryan White clinics (e.g., reenrollment) do not exist, thereby more closely approximating an open-access model of healthcare within the United States. The Atlanta VA ID Clinic provides both HIV specialty and primary care for over 90% of enrolled patients.
Materials and Methods
This study was conducted at the Infectious Disease Clinic (IDC) within the Atlanta Veterans Affairs Medical Center (AVAMC) in Atlanta, Georgia. The IDC is the largest Veterans Affairs (VA) clinic for patients with HIV in the United States, serving ∼1,400 HIV+ patients. This study was part of a larger project at the AVAMC, which included HIV-positive patients who were currently in-care and those who had dropped out of care. This article focuses on the out-of-care group to understand their reasons for treatment drop-out. Patients at the IDC were eligible for the study if they were 18 years or older, first attended the IDC before January 2011, and were diagnosed as HIV positive. Being “out of care” was classified for this study as patients who received at least 6 months of HIV care at the IDC, but had not attended a clinic visit for at least 8 months. Eligible participants were identified through clinic records. Out-of-care patients due for a clinic appointment during the study period were divided into quartiles by their time out of care, and then purposively selected from each quartile. Using clinic records enabled purposive diversity sampling by demographic and treatment retention characteristics; thereafter, iterative recruitment was used to achieve diversity in other characteristics like employment status. Sixteen participants were purposively selected, contacted by telephone, and invited to participate in an interview.
Data were collected from February to July 2013, through qualitative in-depth interviews to identify detailed individual narratives on the context of patients' experiences at the IDC. A semistructured interview guide was developed, piloted, and refined. The following topics were included: influence of military service on healthcare; HIV diagnosis; knowledge of HIV; HIV treatment, care, and support; and barriers and facilitators for receiving HIV care at the AVAMC. Interviews were conducted by researchers trained in qualitative research and experienced with HIV care within the AVAMC system. Interviewers practiced reflexivity to minimize potential influence on data collection. Interviews lasted between 60 and 90 min, were digitally recorded, and conducted in a private room at the IDC. The study was approved by the Emory University Institutional Review Board (IRB00060643).
All interviews were transcribed verbatim, deidentified, and entered into MaxQDA11 software for qualitative data analysis. Narrative analysis 22 and Grounded Theory 23 were used to develop an explanatory framework of the context and influences on patient drop-out of HIV care (Fig. 1). This involved extensive reading and memoing of data to identify issues raised by participants. Each issue was validated by two analysts, given a codename, and listed in a codebook. The codebook included both deductive codes from topics in the interview guide and inductive content-driven codes. Intercoder agreement was conducted to assess the reliability of coding between analysts, and coding discrepancies were resolved before coding the entire data set. Narrative analysis was used to conduct within-case review of each participant's individual narrative to understand issues raised in context and discern any sequence of influences that led to HIV treatment drop-out. These narratives were then compared across the data set to identify core components and sequences influencing missed HIV clinic visits. Grounded theory was then used to search codes across the data to build up a more detailed understanding of each issue and the relationships between issues. Related issues were grouped into categories, and links between categories were explored and verified. A conceptual framework was developed from these analyses to depict various interlinked pathways that lead to HIV treatment drop-out. The framework was validated by continually returning to data, repeating data searches, and reviewing participant narratives to check their fit with the pathways developed. Outliers were examined and incorporated. Additionally, the concept–indicator model 24 was used to confirm that all components of the conceptual framework were well grounded in data. During narrative analysis, we identified a subgroup of participants who had been out of care at the IDC, but received HIV care elsewhere (shown in Table 1), due to periods of incarceration, interstate migration, or a preference for another provider such as at a private clinic. We included these participants in our analyses about reasons for HIV care drop-out to provide a complete understanding on the context of patient drop-out, but excluded them from further analyses, where relevant, to avoid spurious findings.
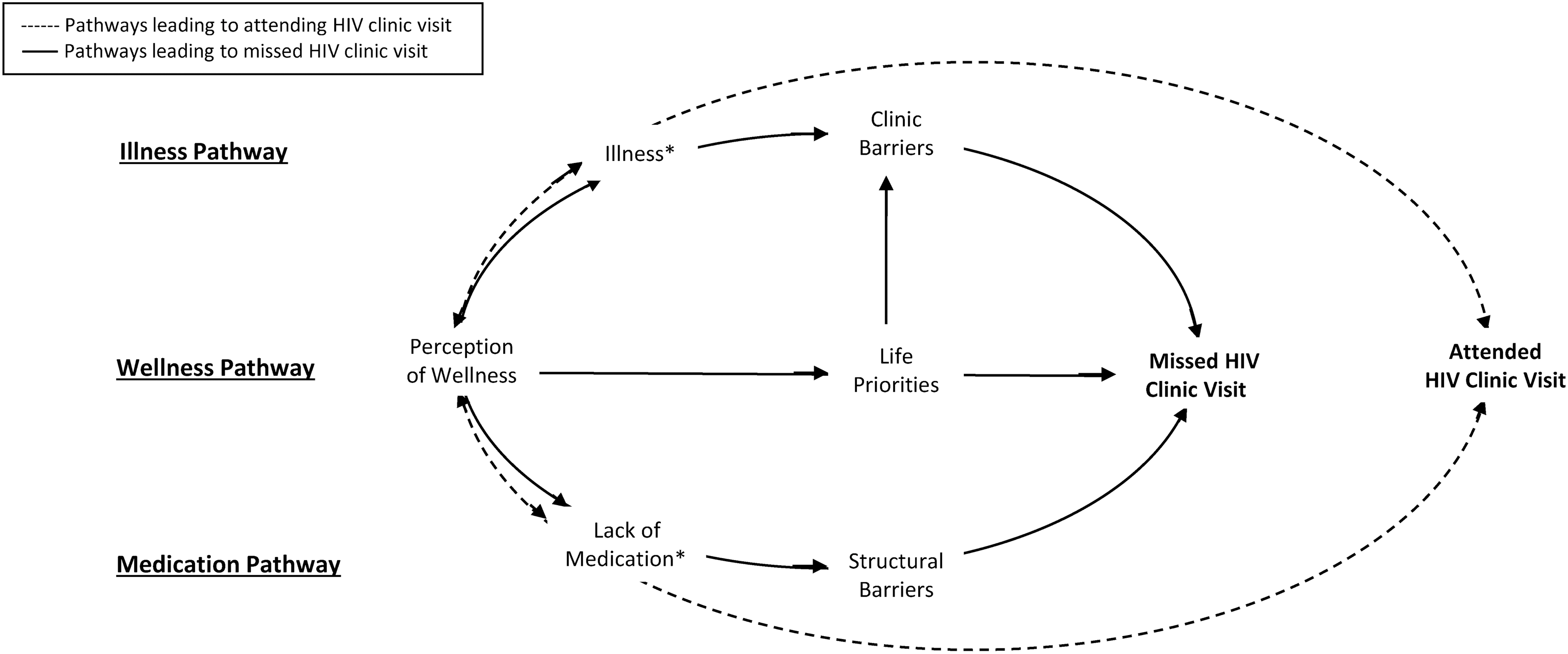
Pathways to missed clinic visits among HIV+ patients at Atlanta Veterans Affairs Medical Center. *‘Illness’ and ‘Lack of Medication’ each acted as both a facilitator and a barrier to attending the HIV clinic for treatment. For example, becoming ill acted as a facilitator to attend the HIV clinic for treatment (dashed line); however, becoming too ill acted as a barrier to being able to attend the clinic (solid line). Similarly, a lack of medication acted as a facilitator to attend the HIV clinic (dashed line) but also became a barrier to accessing the clinic (solid line). See text for further explanation.
Not receiving HIV care at the VAMC or elsewhere.
Out of care at VAMC but in-care elsewhere.
Based on self-report.
GED, General Educational Degree; VAMC, Veterans Affairs Medical Center.
Results
Table 1 shows the sociodemographic and clinical characteristics of study participants. Most participants were Black men, aged between 40 and 67 years of age, with over half attaining a high school diploma. A majority of participants were currently employed, with one-third experiencing periods of incarceration. Overall, participants had been out of care at the VAMC for a mean of 22.9 months. The participants had a mean CD4 count of 394 cells/μL and viral load of 3,769 copies/mL. Some participants self-reported having some mental health problems (56%) and drug addiction (31%). Table 1 also shows the characteristics of the four participants who were out of care at the VAMC, but were found to be in care elsewhere (see Materials and Methods).
Study results show three interlinked “pathways” that led participants to drop out of HIV care for extended periods of time—a wellness pathway, an illness pathway, and a lack of medication pathway (Fig. 1). Each pathway has a dominant deterrent as well as secondary influences that cumulatively discourage participants from maintaining regular HIV care at the AVAMC clinic. Participants followed different pathways at various times during their treatment history; therefore, individuals cannot be categorized into any single pathway. For example, a participant may follow the wellness pathway and experience deterrents to clinic attendance typical of this pathway, then become unwell and follow the illness pathway and experience its respective barriers to clinic attendance, and after recovering from illness may again follow the wellness pathway. Participants also moved in and out of HIV care, with extended periods out of care, but also periodically returning to the AVAMC for clinic visits following specific triggers described below. Results are structured around the three pathways depicted in Figure 1.
Wellness pathway
The wellness pathway is characterized by participants having a sufficient supply of medications for HIV, a sense of responsibility to take their medications regularly, and a strong perception of wellness such that they viewed clinic visits as unnecessary and in competition with other life priorities. Participants stressed the importance of always having HIV medication and taking their medication regularly to keep them feeling healthy. This was facilitated by having a sufficient supply of HIV medication at home and the ability to renew their medication in the mail. They also conveyed a sense of independence in managing their HIV and believed that if they continued to take their medications, a clinic visit was unnecessary unless they became ill or needed to renew their medication. All participants followed the wellness pathway at some time during their treatment history.
Perceptions of wellness
A core characteristic of this pathway is a strong perception of wellness among participants, which included their physical wellbeing, an awareness of their viral load, and being comfortable with HIV. Participants typically described that they simply “feel well” and did not see the need to attend HIV clinic visits when they were not sick. For example, “When I'm not hurtin’ and I'm not sick I, I ain't comin’ to no doctor […] It's just not worth it, especially when I'm healthy. If I feel sick, yeah, I'm the first one that's comin’ to knock on the door” (OC3, white male, 55 years of age). Overall, participants conveyed a strong opinion that clinic visits were for illness and were not needed if they felt well.
Being aware of their CD4 count and viral load also contributed to participants' sense of wellness, whereby they often reported that they “know their numbers” or “their numbers are stable”, thus they felt they were effectively managing their HIV without the need to attend the clinic. For example, “I went in and did a test like every three months. And then it became six months, and then it became, uh, every year and then finally I just didn't go back anymore, ‘cause my numbers was never changing […] I probably was here for like a year, but my numbers really never changed. So I never… I just quit coming. To me, it wasn't even reason to until my health started going bad” (OC11, white male, 49 years of age).
Participants also described that they felt “comfortable with the virus” because they had been living with HIV for a long time and understood HIV better now than when first diagnosed They conveyed a sense of confidence in knowing about HIV, how to manage HIV, and how their body responds to HIV medication. Overall, they reported a passive attitude toward having HIV, for example, “I believe that my virus is ok. it's undetectable…so if I miss this appointment it really won't hurt me because I'll continue to take my medications and then you know, I will go to my next appointment just to make sure that everything is still OK. But I've come to believe that HIV isn't as bad as some people may believe it is. So, I guess I'm kind of passive to my virus…I kind of feel safe with my virus” (OC6, black male, 41 years of age)
Overall, participants said they were no longer afraid of HIV and that taking medication meant that they were in control of their HIV. They stated that HIV was “not a death sentence” anymore but a chronic condition. For example; “C'mon (laughs) I mean, it's no longer a death sentence, but you gotta take your meds just like… diabetes isn't a death sentence, but you gotta take your medications” (OC16, black male, 52 years of age). Therefore, participants felt confident they could remain healthy through continued self-management of HIV without attending the clinic and saw limited risk in missing HIV clinic visits. For example, “as long as my HIV is still in check, I don't see a problem with not seeing the doctor that often” (OC13, black male, 43 years of age). The combination of having enough medications that are taken regularly, a strong perception of wellness, and feeling comfortable with HIV led to participants to decide that attending HIV clinic visits was unnecessary.
Participants' self-perceptions of wellness described above were not always supported by clinical records of their CD4 count. Some participants who described feeling well did have a high * CD4 count and their viral load was undetectable, thus supporting their feeling of wellness; whereas others said they felt well but had a low † CD4 count and sometimes a high viral load, including some with a low-enough CD4 count to be considered as having AIDS. Although participants were aware their CD4 count may be low, they reported that this was insignificant to their wellbeing, stating that if they felt well and were taking their medication, then they were unconcerned about the actual clinical diagnosis. Therefore, participants' own perception of wellness had a greater influence on their decision to miss clinic visits than clinical indicators of wellness.
Life priorities
When participants felt well, their scheduled HIV clinic visits competed with other life activities, which they prioritized over what they perceived as unnecessary clinic visits (Fig. 1). Participants felt they were effectively managing HIV with medication; thus, missing clinic visits was viewed as acceptable, and their focus shifted to other life priorities and responsibilities, such as family, work, or leisure. For example, “I ain't say coming to appointments has taken a back seat, it's just that, with so many other things going on in my mind, I guess it wasn't…I guess I can just admit, I guess it wasn't priority enough in my mind, to remember” (OC16, black male, 52 years of age) and “You look up at the calendar and realize, gee I haven't been to the doctor in a whole year!” (OC8, black male, 67 years of age). As a result, some forgot about scheduled HIV clinic visits or were unaware that they have missed clinic visits, leading to apathy, such as “I just don't realize I have not been in a while” (OC8, black male, 67 years of age). Participants also described procrastinating on clinic visits, for example, “Well, I'll do it next week. You know, that type of thing” (OC11, white male, 49 years of age).
A secondary deterrent to attending HIV clinic visits were clinic-related barriers (Fig. 1). Participants described that the “hassle” of attending the clinic was discouraging and an added burden to what is already seen as an unnecessary visit. Clinic barriers included problems with appointment scheduling, transport, waiting time, and provider issues, which are described in detail on the illness pathway below.
Triggers to resume clinic visits
For participants who felt well, the two main triggers to resume HIV clinic visits were becoming sick or needing to renew their HIV medication (see dashed lines in Fig. 1). Becoming sick was a strong motivator to seek a clinic appointment, and care was typically sought immediately for an illness that was seen as serious or prolonged. For example, “I started feeling bad…I wasn't really sick, just seemed like I was more drained… that's when I decided to come back up here” (OC11, white male, 49 years of age). Participants stated that they were familiar with taking HIV medication and could thus identify atypical side effects or other symptoms of illness that caused concern. In these situations, they often attended the HIV clinic as a nonscheduled “walk-in” patient. Family encouragement was described as a motivator for returning to the HIV clinic when participants became sick or were “feeling low.” For example, “They [family] check on me, they try to check out my doctors' appointments, they ask me if I have been taking my medicine. If I started looking like I am tired or I am not up to par. Then they fuss till they can get me back to the doctor” (OC1, black female, 54 years of age). The other prompt to return to the HIV clinic was a lack of medication, when they had completed their supply. In this situation, participants would prioritize their HIV clinic visit over any potential barriers, with the sole purpose of replenishing their HIV medications. For example, “When I know I'm out of refills, now my appointment becomes priority” (OC16, black male, 52 years of age).
Illness pathway
The illness pathway (Fig. 1) is characterized by various health issues that interfere with participants' ability to attend regular HIV clinic visits. Participants described prioritizing care for non-HIV illnesses over routine HIV clinic visits, becoming sick from side effects of HIV medication, drug addiction that led to irregular medication adherence, and apathy toward missing scheduled clinic visits. These illnesses and conditions made participants less able to travel to the HIV clinic and less willing to tolerate clinic-based issues such as long wait times. Participants experienced the illness pathway at different times during their treatment.
Illness experiences
In this pathway, participants experienced a range of health conditions that they perceived as unrelated to their HIV that required treatment and medication. Both physical and mental health issues were identified, such as cancer, diabetes, high blood pressure, high cholesterol, depression, post-traumatic stress disorder, and drug addiction. Receiving care for these health issues consumed a great deal of time and energy, which led participants to shift their priorities away from attending routine HIV clinic visits to receive care from subspecialists for these health conditions. For example, “I was going downstairs to the oncologist every week…once a week...then when they get through with you, you be wore out” (OC4, black male, 60 years of age). Participants' shift in priorities was rationalized as they were confident that their HIV was being managed by their medication; thus, attending the clinic was given low priority. At times, managing other health conditions, receiving treatments, or recovering from other illnesses left participants too sick or fatigued to travel to the HIV clinic or endure the long wait times. For example, participants receiving chemotherapy described significant physical weakness, weight loss, and stress, making them unable to focus on HIV clinic visits as well. Participants who experienced depression became indifferent about managing their HIV: either the depression itself or their medications left them in a mental haze, and they forgot their HIV clinic appointments. These conditions in addition to general fatigue from living with HIV led to missing HIV clinic visits. For example, “When I was depressed I didn't want to go and do anything. I didn't care if my numbers was bad, you know, so it didn't matter if I got up [to clinic] or not (laughs) you know, so, I mean it was hard to get out of that” (OC11, white male, 49 years of age).
Participants also described becoming ill when they voluntarily stopped taking their HIV medication due to side effects, substance abuse, or beliefs about gaining resistance to HIV medication. Side effects of HIV drugs such as nausea, insomnia, and irritability caused participants to cease taking their HIV medication for extended periods of time to gain relief before resuming care again. For example, “I've never taken medication more than a year and a half, y'know…to the point where it's just the medication, the side effects, you just can't do it anymore” (OC3, white male 55 years of age). Participants described “going off meds for a while” and therefore felt no need to attend HIV clinic visits unless they became ill. Participants who struggled with substance abuse and drug addiction ceased taking HIV medication or took them irregularly and did not prioritize keeping clinic appointments. Beliefs about developing resistance to HIV medication also led participants to stop taking their medications, sometimes for a year or more, during which time they ceased attending HIV clinic visits. This was described as taking a “drug vacation” and “letting your body cleanse itself” from the HIV drugs, which they believed would mitigate gaining drug resistance. As a result of not taking HIV medication, some participants reported becoming very sick or requiring emergency care, which became a trigger to resume their HIV care. For example, “I realized then if I ain't taking the medicine [for HIV] I was gonna stay sick” (OC14, black male, 57 years of age). These situations then caused missed HIV clinic visits.
Participants who experienced illness, as described above, were further discouraged from attending routine HIV clinic visits due to clinic-based barriers (Fig. 1). Participants described the difficulty of having to endure a long wait time when they were feeling sick, which deterred them from attending the HIV clinic. Long wait times were characteristic of all clinic appointments: even if they arrived on time, were the first patient scheduled, or used a walk-in appointment, they typically waited several hours to see a physician. For example, “I don't want to come here for a 9 o'clock appointment and be seen at 11:30 and then you have to go to lunch and I won't really be seen until 1. What kind of stuff is that? Is my time not valuable? Or are you just not time management savvy?” (OC7, black male, 44 years of age). Despite the long wait times, participants reported that if they arrived a little late, they were refused consultation and required to reschedule. For example, “Why is it OK for them to sit there and be two hours late but yet I get here fifteen minutes or an hour or whatever after my appointment is due and all of a sudden I get ostracized? […] That's one of the reasons why every time I come down here I just go home with more stress than before I came down” (OC3, white male, 55 years of age). In addition, participants reported the time burden of traveling several hours to the clinic, enduring traffic issues, and facing difficulties in parking once at the clinic, all of which discouraged their attendance, particularly when ill. Difficulties with scheduling clinic appointments several months in advance left participants without an appointment, and lack of clinic follow-up meant they then “fell through the cracks” of the scheduling system. Furthermore, the inconsistent travel reimbursement process was an added problem.
Limited physicians on duty, rotating physicians, and provider attitudes caused further frustrations for patients and discouraged clinic attendance. Participants reported that there was only one physician on duty to attend to many walk-in patients, which they felt contributed to the long wait time for care. They also described a constant rotation of physicians, which meant they saw a different doctor at each clinic visit. This required them to describe their medical history anew at each appointment, which left little or no time to discuss other health concerns aside from HIV. As a result, any non-HIV issues were often disregarded. Participants described that providers' attitudes toward patients also created a poor patient–provider relationship. They felt that some physicians did not listen to their concerns and lacked compassion, often focusing more on completing medical forms rather than consulting the patient or they were reluctant to fully explain the patient's health conditions. For example, “I've had some [doctors] that were not as friendly as others, and some that take time with their patients and some don't…I have been with some; they don't even look up at you, they're in that [computer], putting it in there, they ask you a few questions, they never look at you, they never identify with you. You know…I don't like a doctor like that. I want one to at least treat me like I'm human” (OC1, black female, 54 years of age).
Although we anticipated that clinic barriers would pose a barrier across all pathways, results show that clinic issues were isolated to the illness pathway and indirectly in the wellness pathway. Therefore, our figure reflects this focused influence of clinic barriers across the different pathways.
Lack of medication pathway
The lack of medication pathway (Fig. 1) is characterized by participants seeking a clinic appointment to replenish their depleted medication supply, but they faced a range of structural barriers that led to missed or delayed clinic visits. Work commitments, time release from work, incarceration, and moving between states presented barriers to attending HIV clinic visits. These barriers often left participants without an adequate supply of HIV medication for extended periods of time.
Structural barriers
In this pathway, participants described taking HIV medications regularly until their supply ended. Although they sought to attend the clinic, they faced structural barriers that led them to miss, delay, or not renew their clinic appointments. Participants described prioritizing work commitments over clinic visits, even if they needed to replenish their HIV medication. They also stated that attending a single clinic visit often required taking a whole day out of work, which was problematic due to the nature of their employment. Working long hours, shift work, inflexible schedules, and lack of sick leave all restricted their ability to take time from work. As a result, participants used vacation days to attend clinic appointments, but when these expired, they were unable to attend further clinic visits. For example, “I'm very religious [with appointments] up until I run out of vacation. The second I run out of vacation, I can't come back up [to clinic] until I get my vacation back again” (OC11, white male, 49 years of age).
Participants were also concerned that taking so much leave for health reasons would raise suspicion among their employers and work colleagues. Those whose HIV status was concealed feared stigma and job loss if the reason for their time off became known. For example:
“I'm still taking four, five hours of leave from work, and so it's kind of a hassle […] and it seems like, are they wondering what's going on? “Why's he have to take this… go to the doctor often?” And then, “He's gone for half a day […] It just makes me feel uncomfortable, you know, they might not… come out and ask me, “Are you sick?,” you know, but […] I can tell that they're wondering ‘cause, so…I feel uncomfortable having to be put in that situation” (OC13, black male, 43 years of age).
To alleviate suspicion at their workplace, participants would regularly miss clinic appointments, thus reducing the amount of leave time needed. For example, “Sometimes just to keep the heat down, so you're not having problems at work, you know, sometimes you have to reschedule” (OC11, white male, 49 years of age).
Incarceration and interstate migration also caused participants to miss HIV clinic visits. Although clinic records will indicate that these participants fell out of care, they were actually still receiving HIV medication while incarcerated or from another VA facility if they had moved residences. Participants also sought HIV care from non-VA providers, thus dropping out of care at the VA clinic periodically while receiving care elsewhere. For example, “My charts in the computer will show some extensive lengths where I wasn't [attending clinic] and that was due to incarceration for some periods as well as me just not living in Georgia” (OC6, black male, 41 years of age).
Discussion
Reducing barriers and promoting facilitators
This qualitative study described three pathways whereby patients fall out of HIV care at a VA facility: a wellness pathway, an illness pathway, and a medication pathway. Perhaps the strongest reported deterrent for participants in this study to remain in HIV care was their self-perception of wellness (wellness pathway). However, their perception of wellness was not necessarily correlated with clinical indicators of wellness, emphasizing the discrepancy between patients' current lack of symptoms and their underlying disease. Participants equated adherence to antiretrovirals (and virologic suppression at times) with wellness and clinic visits with illness, whereby the clinic represented a place to go when feeling ill, presenting with atypical symptoms or having pain. Participants perceived that the function of clinic visits was to “know their numbers” and receive medication refills. If these requirements are already fulfilled, a clinic visit was not valued by patients. Under these circumstances of perceived wellness, any obstruction to keeping an appointment with the clinic providers—namely, life priorities and clinic barriers—became a significant deterrent, only overcome by a stronger trigger to return to care—namely, becoming sick or needing to renew their medication.
To address the perceived wellness barrier, one priority would be to determine whether certain patients actually could “self-manage” their HIV care. Most HIV clinic visits involve comprehensive health evaluations consisting of three areas: (1) HIV management (i.e., CD4/VL monitoring, adherence, side effects/toxicity, drug interactions), (2) preventive care/health maintenance, and (3) primary comorbidity management. For individuals who are knowledgeable about their HIV disease, are virologically suppressed with high CD4 counts, and do not have medical comorbidities, these visits could be less frequent and focus on holistic prevention strategies and health maintenance. For all other patients, annual visits at least twice are necessary. With this in mind, providers should clarify these expectations and discuss the frequency and length of the visits when first meeting with the patient and at periodic intervals thereafter. Providers should also adhere to these expectations by structuring visits around wellness education, rather than just updating the patient on their laboratory results. Additionally, it is important to recognize that patients' understanding of wellness as being independent of CD4 count might be in part a reflection of prior common clinical practice; previously, providers would reassure virologically suppressed patients who had low CD4 counts but felt well and were adherent to medications. However, it is now recognized that a low CD4 count is associated with morbidity and mortality and should therefore remain a clinical concern. 25 Although to date therapeutic options to improve low CD4 counts for these patients do not exist, clinic visits can be an opportunity to ensure that lifestyle modifications are being adopted and appropriate cancer and cardiovascular screening takes place regardless of perceived wellness.
Additionally, to make these clinic visits easier and more comfortable experiences for patients, clinic managers need to continue to find ways to improve administrative and logistical barriers. Attention should be paid to enrollment procedures, scheduling, parking, waiting times, staff culture, and clinic environment. 20 Task shifting some of the parts of the visit to other providers (e.g., pharmacy members, social workers, psychologists, and other members of the care team) and telehealth visits can streamline the visit and provide more convenient options for patients. Indeed, some study participants suggested shifting certain care tasks, such as blood draws, to VA satellite sites closer to their homes. Multiple VA sites have been implementing telehealth collaborative HIV care programs for precisely this reason. 26 Finally, it will be important to engage family members, as they are shown in our study to be facilitators for staying in care.
When participants became acutely ill or dealt with multiple comorbidities (illness pathway), they faced several obstacles to keeping routine HIV clinic visits. Sometimes the illness prevented travel to the clinic or visits would be missed due to hospitalization. For those with multiple comorbidities, participants focused more on subspecialty clinic visits (cardiology, oncology, etc.), and their HIV visits would be deferred. On the other hand, illness also served as a motivator to return to the clinic. For example, when participants described taking a “drug vacation” due to treatment fatigue, significant side effects, or concerns about drug resistance, they would develop symptoms they perceived as being related to HIV. This would prompt them to return to the HIV clinic to resume care. Various strategies could address barriers experienced on this pathway. Special accommodation could be made for hospitalized patients where the routine clinic visit goals are accomplished within the inpatient setting and “counted” as an outpatient visit. Similarly, during acute walk-in visits, providers could attempt to “catch-up” patients on routine care goals at that time. For individuals with multiple comorbidities, clerks could schedule visits on the same day as specialty appointments when feasible (if colocated) to consolidate trips. To decrease treatment interruptions, providers need to increase education around the harms of this practice and have this literature widely available in waiting areas. Finally, a reduction in the aforementioned clinic barriers would assist patients in this pathway, since these are significant obstructions when unwell or managing multiple conditions.
Finally, for those participants who felt well but ran out of medication refills (medication pathway), they came to the clinic only to renew their medications as long as other structural barriers were manageable. For these patients, every effort should be made to reduce structural barriers such as employment release time and psychosocial stressors such as workplace stigma. Organizations such as the Center for HIV Law and Policy and Legal Action Center offer education, legal assistance, and policy advocacy to counter such structural barriers and stigma, through advocating workplace protections, housing rights, and anti-HIV discrimination. Again, the clinic should make every effort to reduce clinic barriers, such as offering more flexible hours, home visits, a patient portal that allows patients to interact with providers, and medication renewal through secure messaging, telephonically, or through telehealth visits.
It is clear that a single strategy is unlikely to be effective for all patients or even any given patient at all times, as evidenced by the fact that participants in this study were influenced by different pathways at different times in their treatment history. Improving issues related to one pathway may have little impact on participants in another, since there are different deterrents in each pathway. For example, improving clinic issues may assist those on the illness pathway, but not on the wellness pathway. Thus, a range of interventions spanning issues in various pathways may be most effective to facilitate regular clinic visits.
Insights from behavioral psychology
According to Maslow's hierarchy, 27 an individual's needs are prioritized such that fundamental needs (i.e., food, sleep, water, and safety) must be satisfied before addressing higher-order needs (i.e., financial security, health, and well-being). 28 To an extent, when an individual is deficient in a basic physiological need (e.g., lack of food), an innate drive (e.g., hunger) will lead to a motivated behavior (e.g., eating). This simplistic model can be useful to explain how social determinants, such as income or food availability, can influence health behaviors. However, the threshold at which a motivated behavior can satisfy a basic need differs among individuals. As an example, certain addictions can override innate drive pathways, giving rise to an individual who can forego eating for several days or longer during an alcohol binge. 29 Additionally, beyond these direct pathway alterations, the value that an individual applies to basic needs can also vary along with the temporal relationship between action and consequence. Essentially, these preferences are interpreted in terms of costs and benefits with a discount applied for future realization of outcomes (theory of delay discounting). 30
Such intertemporal choices are influenced by the environmental context and personal experiences of the individual. This can lead to cognitive biases that can heap psychological barriers on top of existing structural barriers. To illustrate, studies have shown that when individuals are raised in violent neighborhoods or experience significant trauma, safety becomes overvalued when compared with a higher-order need (e.g., education), 31 future benefits are discounted to a greater extent, 32 –34 and impulsive behavior or mental illness can develop. 35,36 This is known as a present-bias preference. 37 Certainly, actual ongoing safety concerns exist for many of these individuals, but even when the context improves, the psychological barrier can persist in the form of post-traumatic stress disorder or symptoms of a foreshortened future. 38 For these individuals, despite thoughtful plans about the future, lifetime benefits (e.g., health, self-actualization) are rapidly discounted to near zero (hyperbolic discounting) to gratify immediate needs. This creates dynamic time-inconsistent behavior, wherein the best laid plans are postponed indefinitely in the face of an onslaught of seemingly more pressing issues. 39
By applying these theoretical constructs to the results of this study, a clearer understanding of health-related decisions becomes possible. When a patient feels well, they will first ensure all other fundamental needs (life priorities) are addressed before considering higher-order needs, such as attending a routine HIV clinic visit focused on primary care and prevention. Since most of the benefits related to primary care and prevention are realized in the distant future, other higher-order needs with an earlier payout such as maintaining employment will take precedence. Those with present-bias preferences will apply an even greater discount on those health behaviors. At the same time—and not hierarchically as Maslow would suggest—feelings of distrust, stigma, and disenfranchisement will increase the cost associated with attending a clinic visit. On the other hand, when a patient feels ill, every effort is made to alleviate these symptoms. If it is determined that a visit to the HIV clinic will accomplish this goal, very little can prevent that visit from occurring. Otherwise, patients will find alternative ways to mitigate their concerns.
With this construct in mind, the need for a strategic approach aimed at addressing both basic needs and enhancing self-actualization becomes apparent. Capitalizing on the lessons learned from Behavioral Economics, simple nudges and incentives (i.e., commitment devices and contingency management) can effectively improve health-related behaviors. 40,41 Incentives have the added benefit of providing financial support for fundamental needs while simultaneously restructuring priorities in favor of delayed gratification. Motivational interviewing, message framing, and empowerment techniques have also been shown to be effective to induce behavioral modification and resilience for individuals with HIV or substance use disorders. 42 –45 Although data are lacking on whether strengthening agency for individuals living with HIV can enhance retention, self-determination and self-efficacy theory have been successfully integrated into strategies to improve physical activity for individuals living with cardiac disease. 46 Our findings suggest that such approaches might likewise be applied effectively to address barriers to retention in HIV care.
This study is limited in its focus on a clinic setting, where patients are veterans and mostly male, therefore, the issues of other types of clinic populations may not be captured in our results. Despite this limitation, many of these patients intermittently obtain care outside of the VA and describe very similar experiences in other clinics. Similarly, the decision-making process of patients from this study are reflective of those reported from HIV clinics throughout the southern U.S. and nationally. Additionally, although interviews were conducted outside of the clinic, they were within the hospital itself. This environment could have restricted what patients were willing to share in response to the clinic-specific questions. However, responses did capture substantial critiques regarding the clinic experience, staff, and providers.
Conclusion
Improving retention in care for individuals living with HIV can have a substantial impact on patient health and the reduction of HIV transmission within the community. This study highlighted three interlinked “pathways” that led participants to fall out of HIV care for an extended period of time: a wellness pathway, an illness pathway, and a lack of medication pathway. These pathways illustrated both barriers to retention and facilitators for returning to care. An individual participant could navigate each of these pathways as their life circumstances and health status changed. This model identified several approaches that could be implemented to improve clinic retention: (1) reduce clinic-based barriers (e.g., clinic wait times, provider continuity, and customer service), (2) address patient foundational needs (e.g., food insecurity, housing, transportation, and child care), and (3) empower patients to become invested in their health even while confronting a lack of basic needs.
Footnotes
Acknowledgments
The authors would like to acknowledge the contributions of the following individuals: Hannah Wichmann, Jed Mangal, MD, Carlos del Rio, MD, James Crowe, Susan Schlueter-Wirtz, MPH, Runa Gokhale, MD, Abeer Moanna, MD, Kelly VanMaldeghem, MPH, Kelcie Landon, MPH, and Matthew Wessinger, MPH. This study was funded by the Emory Center for AIDS Research (Grant P30 AI050409) and the Infectious Disease Society of America Medical Scholars Program. B.N.K. was supported by a postdoctoral fellowship from the Duke Global Health Institute and the Franklin Humanities Institute Health Humanities Laboratory.
Author Disclosure Statement
No competing financial interests exist.
*
A high CD4 count refers to 500 cells/μL or above, whereby risk of death and serious clinical conditions are roughly equivalent to HIV-negative individuals.
†
A low CD4 count refers to 200 cells/μL or below, whereby a patient is considered to have AIDS.