
Abstract
Existing research on HIV stigma has not thoroughly studied the healthcare providers' (HCP) judgment toward people living with HIV (PLHIV). The goal of this article is to conceptualize formation of stigma within attitudes of HCP through their judgmental process by using the Fairness Theory. The study is also aimed to develop a model for cognitive patterns of HCPs' stigmatizing judgments toward PLHIV by applying fuzzy logic. We applied a mixed method in two phases, including qualitative method and fuzzy analytical modeling. A sample of 17 physicians and 9 nurses from 6 hospitals in Tehran were recruited and saturation was achieved after 21 in-depth interviews. Then, the answers of six HCPs were selected for defining the fuzzy sets and membership functions' curve. Six patterns of HCPs' judgments emerged that were used for the fuzzy analysis. These patterns are outcomes of assessment on various aspects of fairness of stigmatization that is impacted by HCPs' counterfactual prototypes. Moral codes, hospital and medical rules, and also constraints imposed from the workplace environment are the references of counterfactual prototypes that affected the HCPs' judgment. Health policy makers can design more effective HIV stigma reduction interventions based on the six patterns of HCPs' judgment.
Introduction
HIV
Bias is created by individuals' perception of deviation from social norms, resulting in cognitive affirmations of unworthiness.
5
Because HIV is associated with “deviant” behavior that is perceived as an individual's responsibility and viewed as contagious and a threat to the community, people with HIV are stigmatized.
6
The discriminatory intention of an HCP toward PLHIV can be associated with behavioral memories involved in his/her judgment process to elicit the judgment categories/prototypes used in judgment formulation.
7
Discrimination is affected by the justice perception, related in turn to the biases of those interacting with PLHIV. HCPs do not make the same judgment about the stigma toward the PLHIV when they experience a similar situation regarding PLHIV. Based on a counterfactual thinking theory, when an HCP visits an HIV-positive patient, she or he has behavioral expectations or standards about interacting with PLHIV (Alipour unpublished observations). In this situation, there are several factors that impose limitations such that the HCP's expectations are not actually accrued. Thus, HCPs experience a judgmental process about the fairness of their behavior toward PLHIV, affected by their cognitive maps that alter the real condition to expected condition by using the counterfactual scenarios/prototypes.
8,9
Applications of Fairness Theory to these counterfactual prototypes include the following
10
: Would prototype: This prototype addresses some negative state of affairs that would have been better in a different situation. Could prototype: Under powerful constraints on behavior, people or organizations sometimes do unpleasant things because they have no other choices. When extenuating circumstances exist, a person or a firm can be forgiven for inflicting harm. Should prototype: Individuals and organizations are expected to behave ethically. We are interested in what they should do when faced with a possibly hurtful decision.
The judgmental process leading to development of discriminatory intentions is a complex phenomenon, understanding of which requires novel research methods and diverse measures of stigma. 11 Thus, we intend to shed new light on the HCPs' judgment process by using Fairness Theory and by modeling HCPs' discrimination-enacting processes via applying fuzzy logic—never previously used in HIV stigma research—to determine how to translate this underlying cognitive mechanism into fuzzy membership functions to model and measure stigma more accurately and identify diverse patterns of stigmatizing judgments toward PLHIV.
Methods
In this article, we used a two-phase mixed method: (1) qualitative data collection and (2) fuzzy analytical modeling.
Phase 1—qualitative method: in-depth interview with concerned subjects
Stigma is a complicated, socially defined, and contextual phenomenon. 12
To study HCPs' attitudes and bias toward PLHIV, we took Grounded Theory as the basis of our analysis and used field notes and in-depth interviews for the data collection process. Coding and data categorization processes were developed based on a generic analytic cycle. 13 Themes were identified using reference framework theory, 14,15 which was complemented by categorization and conceptualization based on Fairness Theory (Table 1).
HCP, healthcare provider; PLHIV, people living with HIV.
Data collection
Selection of the HCPs was based on (1) experience in providing medical care to PLHIV at least once during the past 2 years, and (2) willingness to participate in interview sessions. A total of 26 participants—17 physicians and 9 nurses from 2 private and 4 public hospitals in Tehran—participated in the study. In-depth interviews were conducted in Persian in HCPs' offices. Interviews were not audio recorded, since no consent for recording was obtained, but field notes were taken during each interview by the principal investigator and an assistant. Each interview consisted of a 45- to 60-min semistructured interview using open-ended and discovery-oriented questions and a structured interview of ≤45 min using appropriate inquiries regarding personal perceptions and lived experiences of HIV-related stigma. Participants were asked to identify their positions in reference to fuzzy membership function diagrams. Responses and identities of respondents were coded for confidentiality.
Basic meaning units were identified and coded; similar codes were categorized under Judgment, Expectations, Comparative Thinking, Expectation Sources, and Victimization.
Mode of transmission and HCPs' judgments and decision-making
Participants were asked about their thought processes while visiting PLHIV to learn about bias elements that could affect HCPs' medical decisions. Many respondents explained that they tried to accept PLHIV without judgment, but admitted bias. Two respondents described PLHIV as “licentious” and stated that they would either treat such patients as low priority or pass them to other providers. Four other respondents clearly mentioned that their biases affected their medical decisions, especially about drug addicts and sex workers. Several respondents also expressed being unconsciously or indirectly influenced by their biases (Table 2).
HCPs' judgments about fairness of the conditions, their expectations, and comparative thinking
A specific question was posed as to whether it was acceptable to house PLHIV with other patients. Responses show how HCPs' expectations, which form their perception about the fairness with respect to PLHIV, derive from sources justifying their evaluation of enacted stigma toward PLHIV and their perceptions about fairness, including (but not limited to) ethical codes and hospital rules. The HCPs' disparate experience and knowledge about HIV transmission gave them different interpretations about the risk of transmission. While 20 respondents felt PLHIV should be kept isolated from others, 6 respondents had conditional disagreement with isolation (Table 3).
Victimization
HCPs' sense of victimization due to interactions with PLHIV, particularly related to needle stick risk, was expressed by 22 respondents; 18 respondents would decline to inform their family if a needle stick occurred. Both can be sources of justification for avoiding PLHIV (Table 4).
Phase 2—fuzzy analytical study
The concept of fuzzy membership function enables us to model the complex world of the cognitional judgments. 9,16 For modeling the biases of HCPs, we extrapolated cognitive patterns corresponding to judgments about behaviors encountered in relation to PLHIV in the hospital. These behaviors are “real” conditions (x) that given HCPs compare with a “standard or expected” condition (y). Questions were posed in relation to both the degree of real conditions (x or RC) in how they actually behave with their patient and to the expectation (y or EC) of behavior or thinking toward their patient. Given the geometrical distance d(x,y) between the rating (x) and the rating (y), the reference point or prototype plays a main role in formulating the judgment transform d(x,y) to the perceived distance. If a given HCP responds in a five-point Likert scale, we have three main alternative conditions, as shown in Table 5.
Given two HCPs at the same hospital with equal d(x,y), their biases and behavioral intentions toward a given PLHIV can still be unequal. Perceived distance between the RC and the EC is represented by the membership grade μEC (RC) of RC in the fuzzy set EC, which can be interpreted as the grade to which the RC is similar to the EC. 9,17 Thus, in our case, the three fuzzy sets of EC discrimination perception and their membership functions are conceptualized based on the counterfactual prototypes of Would, Could, and Should (Table 6). Several methods for constructing membership functions are described in the literature, which can be calculated based on the experts' judgment or on data. 17 Considering this article's methodological approach, we collected data from 6 physicians from 26 first-phase participants based on (1) those who scored the same for both real and expected conditions, (2) diverse counterfactual prototypes, and (3) willingness to stay in the study's next phase.
Results
Results are shown in Table 4 where two patterns of behavior for each of the three prototypes were identified.
The universal set of Should
Use of the prototype Should assumes a reference point based on the moral codes and ethical norms that is a concept of absolute extreme.
Pattern 1: Physician #1 rated RC = 2 and EC = 4, so d(x,y) = −2, x < y (Table 7 and right side of Fig. 1). Here, −2 means that she or he perceives some discrimination toward PLHIV in her or his hospital. She or he identified a 0.3 nondiscrimination (fairness) and so 0.7 discrimination toward PLHIV in the hospital. Framed under the prototype “Should,” her or his expectation is defined by moral principles. In addition, she or he perceives a high level of discrimination toward PLHIV at the hospital (0.7). Therefore, the probability of her or his contribution to nondiscrimination programs toward PLHIV is high because she or he believed in moral codes and perceived that the hospital broke with ethical frameworks.
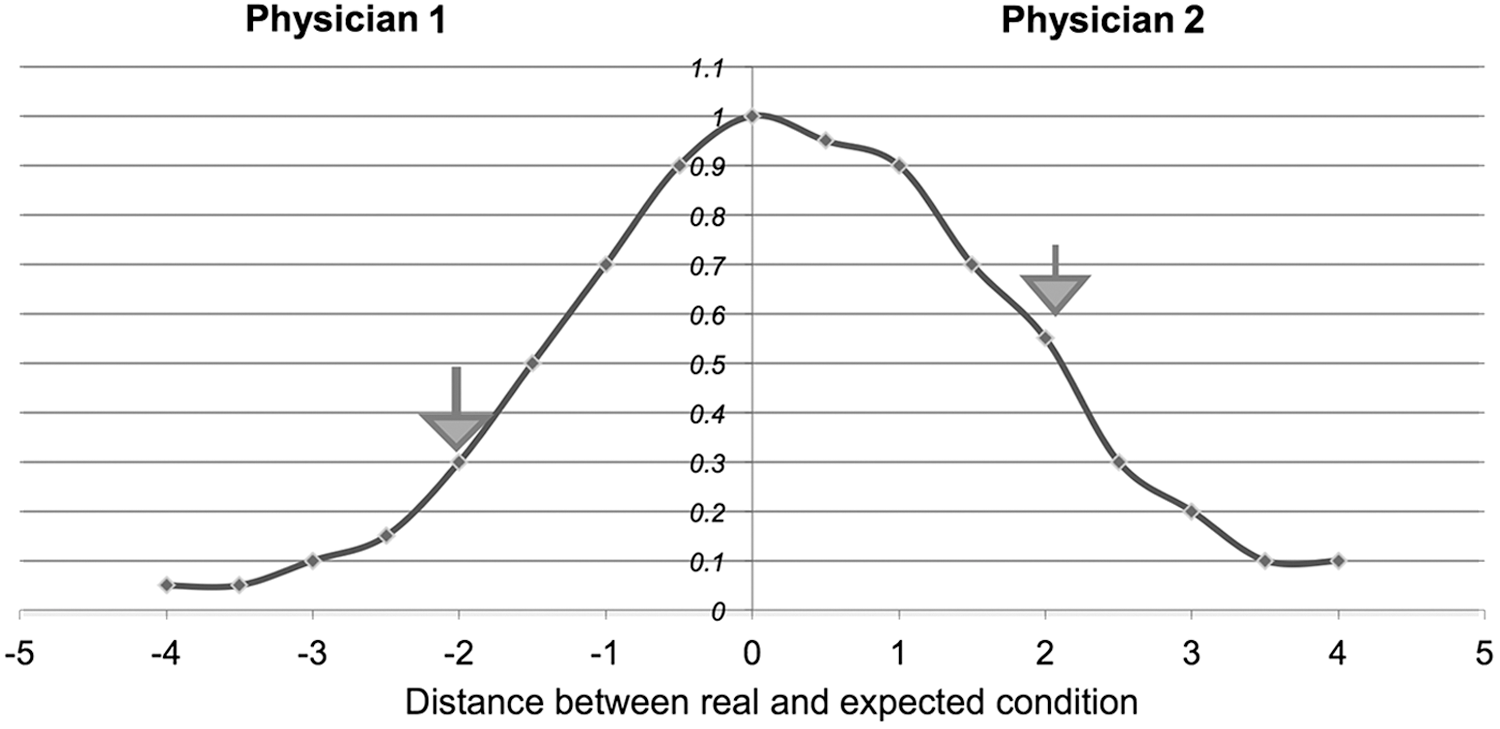
Patterns 1 and 2 for Should membership function.
Pattern 2: Physician #2 rated RC = 4, EC = 2 so d(x,y) = 2, x > y (Table 7 and left side of Fig. 1). Here, +2 condition means that she or he perceives a 0.55 nondiscrimination (fairness); thus, 0.45 discrimination is applied. She or he believed mixing PLHIV with other patients may cause harm to others in the hospital and described separating PLHIV as protecting both other patients and hospital personnel from the risk of transmission as well as protecting HIV patients from stigma and discrimination by others, stating, “Actually, we respect PLHIV by isolating them.” Framed under the prototype “Should,” her or his ethical principles and moral codes focus on protecting herself or himself and society. Her or his discriminatory perception toward PLHIV was not high; she or he may not contribute to reducing discrimination toward PLHIV, but rather than viewing this condition as discrimination, she or he interpreted it as means of protecting social interests and healthcare benefits (Fig. 1).
The universal set of Would
Use of the prototype Would assumes a reference point, e.g., hospital rules, medical protocols, and social realities.
Pattern 3: Physician #3 rated RC = 2, EC = 4, so d(x,y) = −2, x < y (Table 7 and right side of Fig. 2). Here, −2 produces a 0.70 nondiscrimination (fairness) and 0.3 discrimination applied toward PLHIV. Under prototype W, she or he believed that patient mixing was not allowed in her or his hospital and interpreted this as a social reality stemming from the decision-making authority of the hospital, stating, “The reality is not always in line with our expectance, and if we allow PLHIV to mix freely with other patients, it will cause some disturbance.” Therefore, her or his discrimination perception is reduced to 0.3. Although she or he has no objection to mixing, she or he may not actively contribute to reduce discrimination because she or he obeys the rule of the hospital.
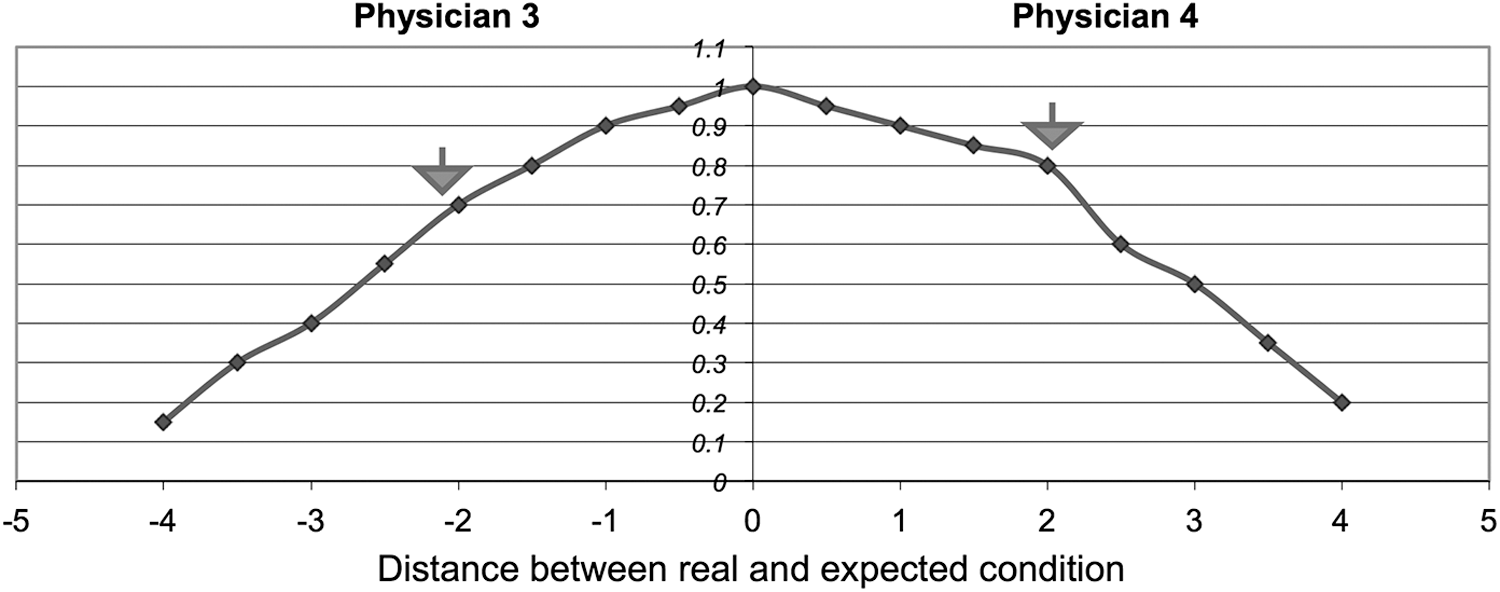
Patterns 3 and 4 for Would membership function.
Pattern 4: Physician #4 rated RC = 4, EC = 2, so d(x,y) = +2, x > y (Table 7 and left side of Fig. 2). Here, +2 means a 0.8 nondiscrimination (fairness) factor, and so 0.20 discrimination is applied toward himself or herself. Under prototype W, he or she considered hospital rules allowing patient mixing to have a negative impact on personnel yet viewed them as a reality to be accepted, stating, “In order to observe hospital rules and protocols, we are forced to allow PLHIV to mix freely with other patients. We don't have any authority to change the circumstance” (Fig. 2).
The universal set of Could
Under prototype “Could,” the powerful constraints of social and contextual limitations are imposed such that people sometimes do unpleasant things because they have no other choices. Therefore, the rate of the “expected condition” in perception of the respondent is less than the expected y that she or he expresses in the questionnaire, and the geometric distance decreases; accordingly, we assume Y = y – 1 and d(x, Y) = [−3,3], UC = {x | x [−3,3]}.
Pattern 5: Physician #5 rated real condition = 2, expected condition = 4, so d(x,y) = −2, x < y (Table 7 and right side of Fig. 3). Here, −2 means she or he thinks 0.85 nondiscrimination (fairness) toward PLHIV and so 0.15 discrimination toward PLHIV. She or he described an incident in which an HIV-positive infant was housed with other infants: “[the mothers] protested and made chaos in the hospital … and complained to hospital managers. To avoid disturbance, it is better to isolate [PLHIV], even if I believe they should not be isolated.” For this reason, her or his discrimination perception reduced to 0.15; although she or he agrees with mixing, the probability of her or his contribution to reduce discrimination is very low.
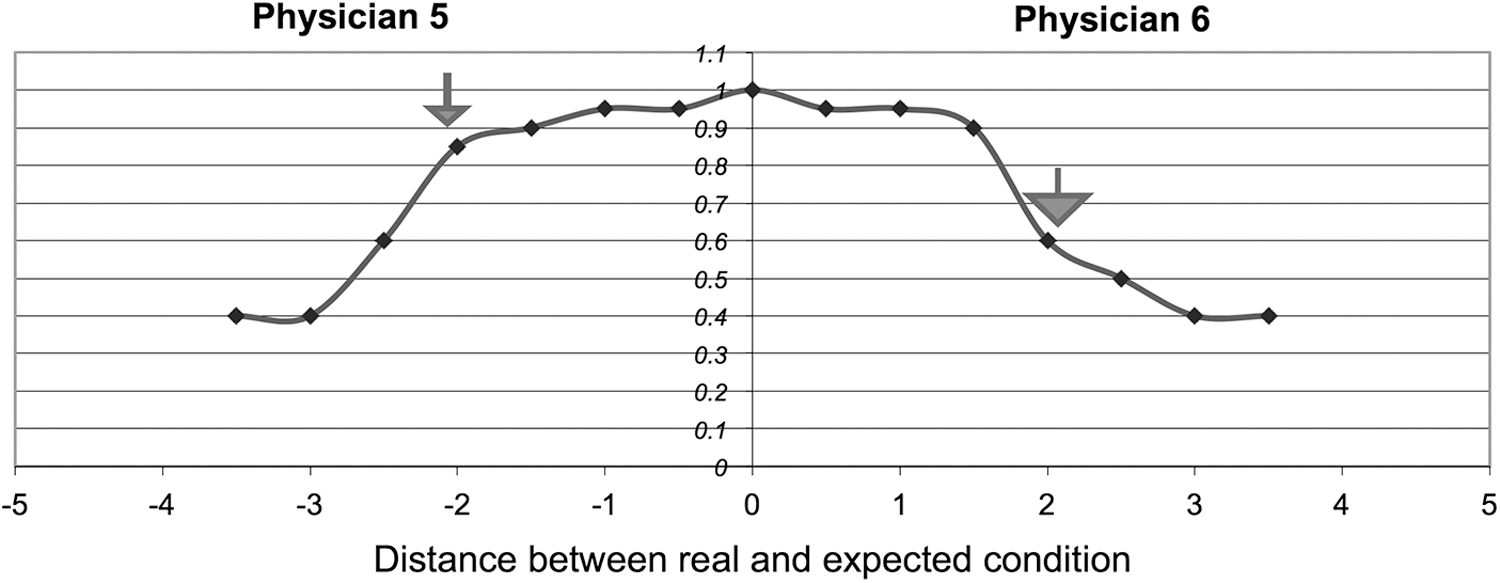
Patterns 5 and 6 for Could membership function.
Pattern 6: Physician #6 rated RC = 4, EC = 2 so d(x,y) = +2, x > y (Table 7 and left side of Fig. 3). Here, +2 means he or she thinks 0.6 nondiscrimination (fairness) toward himself or herself and so 0.40 discrimination toward himself or herself. Under the prototype “Could,” with powerful limitations imposed by public health policies, he or she thinks that people must adapt to their environment and often have no choice but to behave in unpleasant ways. He or she stated, “I am relatively tolerant … because I work in a public hospital that hosts a big segment of HIV population in Iran… [but] if we allow PLHIV to mix freely with other patients, it may make me a victim of hospital decisions that ignore the rights of other patients and hospitals' personnel.” Accordingly, the probability of his or her contribution to HIV stigma reduction programs is not relatively high (Fig. 3).
Discussion
In this study, we analyzed HCPs' judgments using fuzzy logic principles after conducting in-depth interviews within the framework of Fairness Theory. In the first, qualitative phase, we categorized different HCPs' biases toward PLHIV based on judgment sources, stereotypes, and feelings, some of which were identified in previous studies. 18 –20 Moral codes, religious attitudes, and social norms identified as contributing to stigma 21 –23 were reviewed and classified under the Should prototype based on Fairness Theory. We used concept of attribution model of stigma that includes “justifications” as a reason for prejudices 22 as well as System Justification 24 in our classification of the Could prototype to identify HCPs' sources of judgments. For the Would prototype, we did not find an appropriate model serving to our case. However, studies find that a lack of specific policies or guidelines about PLHIV care can increase discriminatory attitudes of HCPs. 25 To get to zero discrimination, we need to design effective interventions not only to learn about the prevalence of different cognitive prototypes among HCPs but also to assess the strength of counterfactuals among HCPs 26 to enable cluster analysis of different types of HCP stigma.
Conclusions
As the first users of fuzzy logic as an exploratory methodology in this context, we found it to be a solid framework for unfolding the complex issue of discrimination toward PLHIV through more in-depth understanding of HCPs' judgments. Using this methodology in future surveys can provide more accurate predictions about HCPs' discriminatory behavior toward PLHIV. Although the purpose of this qualitative study was not to seek generalizability of the findings, the self-selected, convenient sampling method limits our ability to generalize these results; nevertheless, we believe our findings can be representative of similar situations.
Footnotes
Acknowledgment
The work is dedicated to the memory of Dr. Mathilde Krim and her tireless scientific and advocacy efforts to halt the HIV/AIDS epidemic.
Author Disclosure Statement
No competing financial interests exist.