
Abstract
Neuroimaging studies have focused mainly on human immunodeficiency virus (HIV)-infected adults or younger children, showing abnormal brain structures. In this study, we used voxel-based morphometry to investigate the brain integrity of HIV vertically infected adolescents. Twenty-five HIV vertically infected (HIV+) adolescents and 33 HIV-exposed, but uninfected (HIV−) and demographically matched controls participated in this study. T1 high-resolution anatomical magnetic resonance imaging images were obtained and segmented into gray matter (GM) and white matter (WM) segments. Then, population templates were derived from the entire imaging dataset using the diffeomorphic anatomical registration through exponentiated lie algebra (DARTEL) technique. Between-group GM and WM maps were contrasted using independent two-sample t-tests, with age and sex as nuisance regressors of no interest. Significant effects were identified using voxel-wise p < .001 and cluster-level p < .05 with a family-wise error correction. Whole brain volume between the groups did not demonstrate a significant difference. Relative to HIV− controls, the HIV+ adolescents demonstrated less GM in the bilateral cerebellum, right pallidum, right calcarine, left anterior cingulate cortex (ACC), and right superior occipital lobe. HIV+ adolescents also demonstrated less WM volume in the bilateral cerebellum, right brainstem, and left occipital lobe. Furthermore, the volume of the ACC was positively correlated with the Mini-Mental State Examination (MMSE) and the CD4 cell counts in the HIV+ adolescents. The age of highly active antiretroviral therapy (HAART) onset was positively correlated with GM volume in the right temporal lobe, left occipital lobe, and left precentral gyrus. In HIV+ adolescents, a pattern of less WM density and altered GM and WM volume suggests that early HIV infection combined with neurotoxicity effect of early HAART, a lack of viral control may have a significant effect on the brain structural integrity. The process of corpus callosum formation in the corpus callosum and the frontal WM is more susceptible to HIV infection. Altered ACC integrity may represent a promising biomarker of cognitive dysfunction following HIV infection.
Introduction
Perinatal human immunodeficiency virus (HIV) infection remains a major public health problem worldwide, and it disproportionately affects children in developing countries around the world. Although early highly active anti-retroviral therapy (HAART) can reduce the incidence of HIV-associated encephalopathy in children with vertical HIV infection, 1 many children survive to adulthood and are likely to experience continuous and progressive brain damage. How vertical HIV infection affects the brains of infants and children has been documented, 2 but the effects of long-term infection on the brain structure of HIV+ children and adolescents have received relatively little attention.
Recent studies have found neurobehavioral changes in perinatal HIV+ adolescents, and thus, noninvasive brain imaging methods are needed to assess the brain integrity of these patients. 3,4 Precise and early detection of the brain damage are beneficial for medical protocols and cognitive protection of HIV-infected individuals, especially among children and adolescents.
In vivo and in vitro studies have shown regional brain tissue changes in HIV+ patients, including less brain volume. 5 –8 Autopsy evidence suggests extensive neuronal loss across the entire cerebral cortex, basal ganglia, and brainstem. 9 Volumetric magnetic resonance imaging (MRI) studies in HIV+ patients indicates that HIV+ individuals have less volumes in the cerebral cortex, basal ganglia, and white matter (WM). 10,11 Tensor-based morphometry and cortical gray matter (GM) thickness measurements can show less volume in the cerebral cortex, and the volumes of the frontal and parietal lobe are related to the HIV-related neurocognitive dyskinesia and the number of CD4 cells. 6,12 Voxel-based morphometry (VBM) studies have reported that the degree of cortical and subcortical volume loss in asymptomatic HIV+ patients is associated with fewer CD4 cells, and the degree of basal ganglia volume loss is closely related to disease severity. 13 In addition, a recent deformation-based morphometry study 14 has found that despite the use of HAART, HIV+ group has less volumes in the cortical and subcortical regions.
VBM has been proven to be effective for detecting abnormalities in brain volume or density. It achieves an unbiased discovery of abnormalities in the whole brain volume, 15 and it finds the differential brain regions that are difficult to distinguish by region of interest (ROI) analysis. VBM is primarily used to detect brain structural abnormalities that are difficult to observe with conventional imaging methods. 16,17 This method is widely used for detecting the differences in brain tissue in other neurological conditions, such as Alzheimer's, schizophrenia, and amyotrophic lateral sclerosis. 18 –20
Recent MRI studies have reported changes in brain volume in HIV+ patients, mainly in the basal ganglia. 6,11,21 Similarly, neuroimaging studies have demonstrated brain structural abnormalities in adolescents with vertically transmitted HIV infection. For example, a VBM study reported less WM volume in the posterior part of the corpus callosum, external capsule, and ventral temporal lobe in vertically infected youths. 22 Some other studies have identified a smaller GM volume in HIV-infected adolescents, 23 –26 and major neurocognitive disorders or worse cognitive performance were observed in pediatric HIV patients. 24,25,26 An inverse relationship between age and GM volume was found in typically developing youth, but was not observed in youth with perinatally acquired HIV. 27 The trajectory of the left pallidum volume was positively associated with the baseline CD4 count in Thai children with HIV. 28 One study found that the HIV+ patients displayed less GM, mainly located in the bilateral frontal cortices, bilateral anterior cingulate cortices (ACC), and left supplementary motor area. 29
From these observational neuroimaging findings, we hypothesized that there might be less GM in HIV vertically infected adolescents. In this study, we used high-resolution T1-weighted MRI images and VBM analysis to investigate the differences in WM and GM structure between perinatal HIV+ and sex- and age-matched HIV− adolescents.
Materials and Methods
Subjects
We recruited 25 HIV-positive adolescents (HIV+; mean age ± standard deviation [SD], 15.0 ± 1.7 years; range, 12–17 years). The presence of HIV was confirmed by enzyme-linked immunosorbent assay (ELISA) and Western blot analysis. We also recruited 33 age- and sex-matched HIV-exposed, but uninfected subjects (HIV−; mean age ± SD, 14.8 ± 1.6 years; range, 12–18 years). All HIV+ adolescents were infected by mother-to-child transmission during pregnancy or childbirth or through breastfeeding, and they were infected with the same clade/strain of the virus that their mother harbored. The HIV− subjects' fathers or mothers also suffered from HIV infections. The socioeconomic status and cultural and ethnic backgrounds of the two groups were comparable. Detailed demographic information and clinical measures are listed in Table 1. All subjects were enrolled from the Center of Acquired Immune Deficiency Syndrome (AIDS) Prevention and Cure of Zhongnan Hospital, Wuhan University. The inclusion criteria for the HIV+ subjects included HIV acquisition during the fetal or neonatal period, currently treated with HAART, and right handed. For the control subjects, the inclusion criteria included confirmation of HIV-negative status by ELISA and right-handedness.
Demographic Information for Subjects in Each Group
NA indicates not applicable or available. Eighteen HIV+ adolescents were with undetectable plasma viral loads.
HIV, human immunodeficiency virus; IQR, interquartile range; MMSE, Mini-Mental State Examination; MoCA, Montreal cognitive assessment.
Exclusion criteria for all subjects included those younger than 12 years of age or older than 18 years of age and with acute medical illnesses, current or past medical or neurological diseases, psychiatric illnesses, mental retardation, current alcohol or drug abuse, opportunistic infections, MRI contraindications, claustrophobia, metabolic disorders, or other brain diseases (not AIDS related). For the control subjects, the exclusion criteria also included serious educational difficulties and chronic medication use. All HIV infection participants underwent laboratory evaluations, such as plasma CD4 T cell counts. In addition, 23 out of 24 HIV infection participants participated in plasma viral load assessments.
This study was approved by the Medical Ethics Committee of Zhongnan Hospital of Wuhan University, and written informed consent was obtained from all participants or their guardians following a complete description of the measurements.
Assessments
The Mini-Mental State Examination (MMSE) and Montreal cognitive assessment (MoCA) were used to assess the cognitive abilities of the subjects.
Image acquisition
High-resolution T1-weighted structural MRI scans were acquired on a 3.0 T scanner (Siemens, Tim-Trio, Erlangen, Germany), which was located at the Department of Radiology, the Zhongnan Hospital of Wuhan University, using a multi-echo magnetization prepared rapid acquisition gradient echo (MPRAGE) pulse sequence (repetition time = 1,900 ms, echo time = 2.1 ms, inversion time = 900 ms, flip angle = 9°, slice thickness = 1.00 mm, and matrix size = 320 × 320) that yielded 160 axial slices with an in-plane resolution of 1.0 × 1.0 mm.
Data processing
VBM analyses were performed using statistical parametric mapping (SPM) software (SPM12; Wellcome Department of Cognitive Neurology, London, United Kingdom) and CAT12 (CAT) based on MATLAB (MathWorks, Natick, MA). All T1 images were manually checked by an operator blind to subject identity. The processing steps were as follows: (1) the raw T1 images were manually reoriented to the center point of the AC-PC plane; (2) the reoriented images were segmented into WM, GM, and cerebrospinal fluid using the standard unified segmented model in CAT12; (3) the GM images were nonlinearly normalized into standard Montreal Neurological Institute space using a pediatric template for 12- to 18-year-old children from the Imaging Research Center at Cincinnati Children's Hospital Medical Center; (4) these normalized segments were then modulated to ensure that the relative volumes of GM were retained after the spatial normalization; (5) the modulated images were resampled to 1.5 × 1.5 × 1.5 mm3 and smoothed with an 8 mm full width at half-maximum Gaussian kernel; (6) to control for deviations, we included an additional quality check based on heterogeneity measurements of the sample as implemented in CAT, using the covariance of voxel-based data to identify the outliers who were two or more SDs outside of the GM volume sample distributions, and one patient and one control were excluded based on this criterion; and (7) finally, exclude voxels with a absolute value <0.15 to eliminate the low probability of tissue segments.
Statistical analysis
Statistical analysis for the patient demographics was conducted using IBM SPSS version 20 (IBM SPSS, Inc., Chicago, IL) and included Chi-square and independent two-sample t-tests for the participant characteristics. The significance threshold was set to p < .05.
The between-group GM and WM differences were contrasted using independent two-sample t-tests in the CAT12 and SPM12, and intracranial volume, age, and sex were used as covariates of no interest. The significance threshold was set to voxel-wise p < .001 and cluster-level p < .05 with Family Wise Error correction, and threshold-free cluster enhancement with 10,000 random permutations was used to correct for multiple comparisons.
Brain-behavior associations between GM and WM measures within the significant clusters, with the age of HAART onset and duration of HAART, MoCA, MMSE, and CD4 cell counts were assessed using Pearson's linear correlations, with a significance level of p < .05.
Results
Demographic and clinical data
Table 1 shows the demographic and clinical data for all subjects. There were no significant differences in age or education between the two groups, except for the HIV+ adolescents having significantly lower MMSE scores (p = .006).
The CD4 counts ranged from 144 to 1,025 cells/mm3 (average: 597.5 cells/mm3) for the HIV+ adolescents, and 18 HIV+ adolescents had undetectable plasma viral loads. The MoCA scores were not normally distributed and an additional Wilcoxon rank sum test was performed. After the test, there was no significant difference in MoCA between the two groups (p = .231).
Regional differences in GM volume
Significant GM volume differences were identified in the 24 HIV+ adolescents compared with the HIV− subjects (Fig. 1 and Table 2). The 24 HIV+ adolescents showed significantly less GM in the bilateral cerebellum crus, right cerebellum, right pallidum, right calcarine, left ACC, and right superior occipital lobe compared with the HIV− subjects.
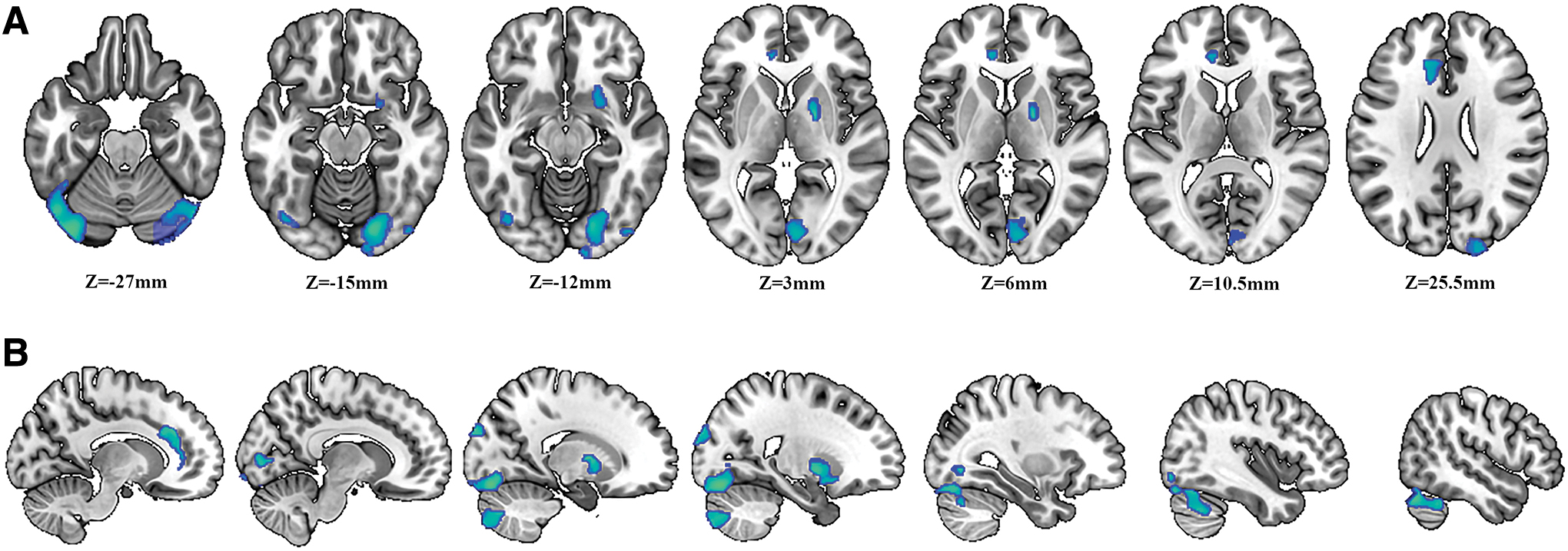
Differences in GM volume. The picture on the left side corresponds to the left hemisphere.
Regions of Less Gray Matter Volume in HIV-Positive Adolescents Compared with Age- and Gender-Matched Controls
p < .05, with a cluster-level FWE correction and TFCE multiple comparison corrected.
ACC, anterior cingulate cortex; FWE, Family Wise Error; TFCE, threshold-free cluster enhancement; BA, brodmann's area.
Significant GM volume differences were also identified in the 18 virally suppressed HIV+ adolescents compared with the HIV− subjects (Fig. 2 and Table 3). The HIV-positive adolescents showed significant less GM volume in the left middle occipital gyrus, left pallidum, right lingual, right calcarine, and right postcentral compared with control subjects, and more GM volume in the left inferior parietal gyrus, left superior frontal gyrus, left middle frontal gyrus, and left middle temporal gyrus.
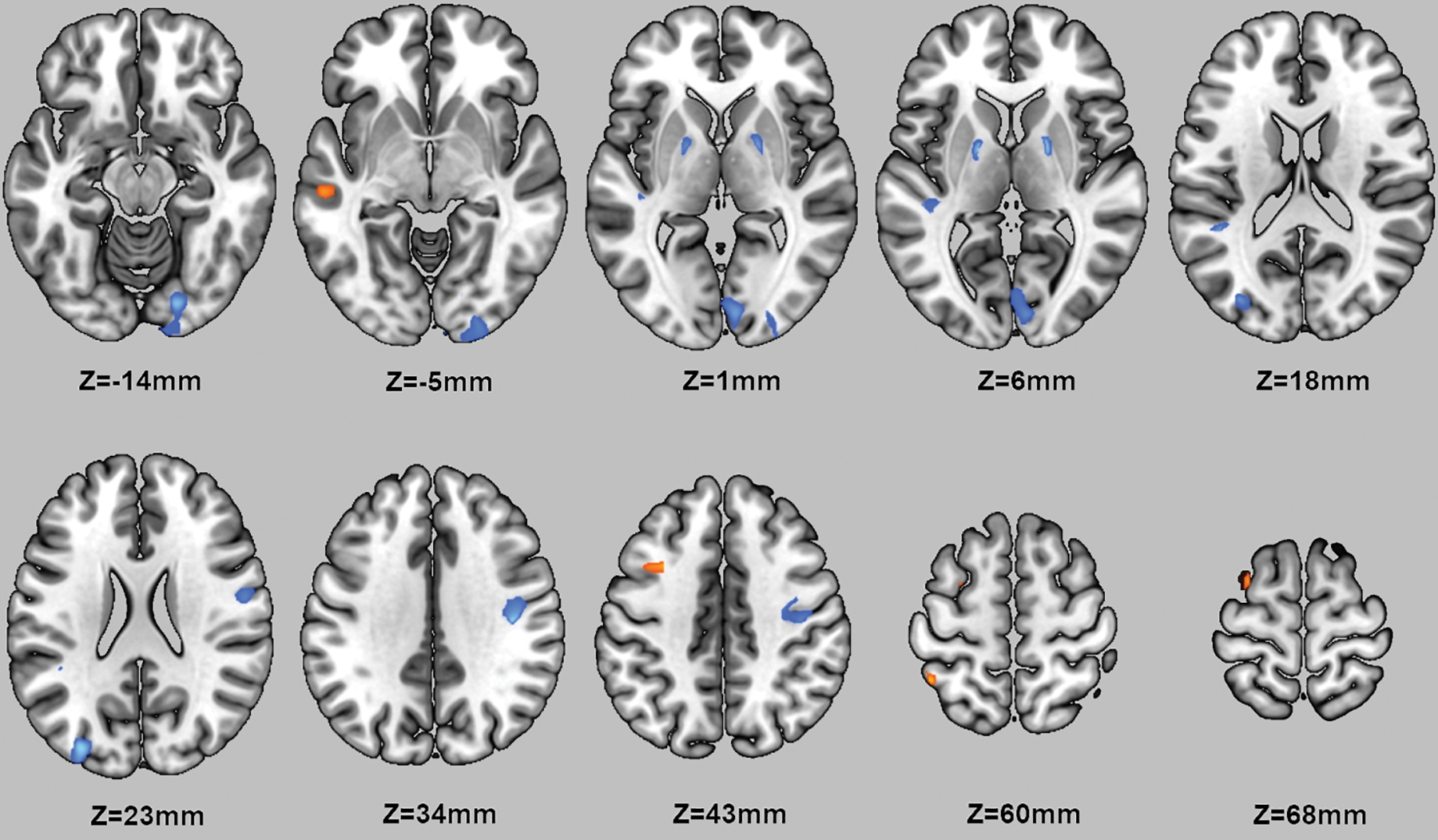
Differences in GM volume in 18 virally suppressed HIV-positive adolescents. The picture on the left side corresponds to the left hemisphere. GM volume changes occur in the region with MNI coordinates in the z direction between z = −14 and 68. The HIV-positive adolescents showed significantly less GM volume (blue) in the left middle occipital gyrus, left pallidum, right lingual, right calcarine, and right postcentral compared with control subjects, and more GM volume (red) in the left inferior parietal gyrus, left superior frontal gyrus, left middle frontal gyrus, and left middle temporal gyrus. Color images are available online.
Regions of Less or More GMV in 18 Virally Suppressed HIV-Positive Adolescents Compared with Age- and Gender-Matched Controls
p < .05, with a cluster level FWE correction and TFCE multiple comparison corrected.
GMV, gray matter volume.
There was no significant difference in the intracranial volumes among the groups (including the total GM volume, total WM volume, and the sum of the GM volume and WM volume).
Regional differences in WM measures
Tables 4 and 5 list the coordinates and the areas with less and more WM volume of brain regions, respectively, compared to HIV−. HIV+ had a lower WM volume in the posterior cerebellum, right brain stem, and left occipital lobe compared to the HIV− group, and had a greater WM volume in the bilateral frontal lobe, left temporal lobe, and bilateral parietal lobe.
HIV+ Group WMV Was Significantly Lower than HIV− Group
p < .05, TFCE multiple comparison correction.
WMV, white matter volume.
HIV+ Group Showed Significantly More WMV Relative to the HIV− Group
p < .05, TFCE multiple comparison correction.
WMV, white matter volume.
The spatial distribution of brain regions (Fig. 3 and Table 6) shows the areas of less WM density in the HIV+ adolescents. The HIV+ adolescents had less WM density in the bilateral corpus callosum (including the knees, splenium, and body), bilateral posterior cerebellar lobes, bilateral frontal lobes, left cingulate gyrus, and left temporal lobes.
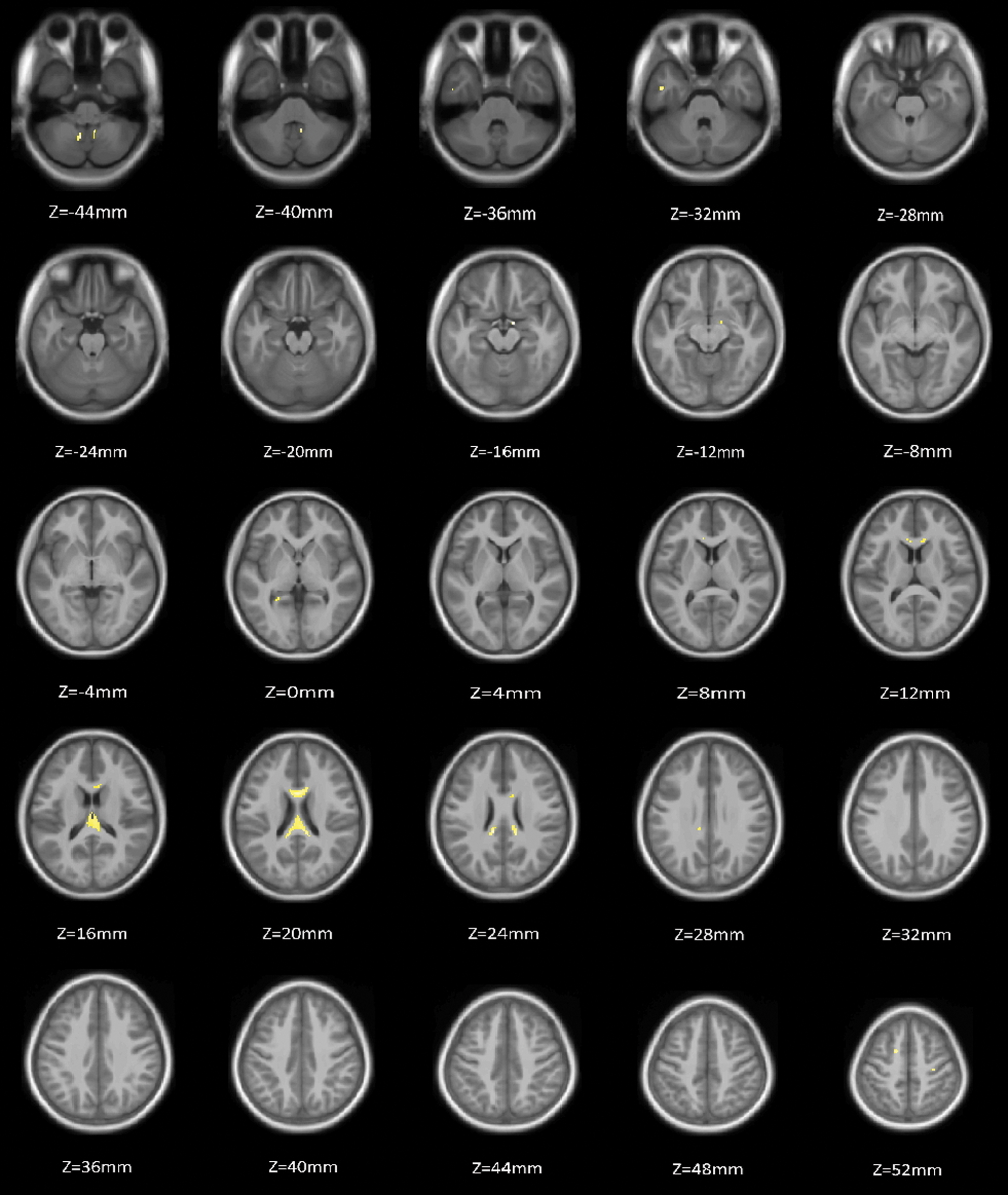
Less WM density in HIV+. Compared with the HIV− group, HIV+ adolescents showed less WM density area in the bilateral corpus callosum (including the knees, splenium, and body), bilateral posterior cerebellar lobes, bilateral frontal lobes, left cingulate gyrus, and left temporal lobes. The HIV+ group did not show a brain area with more WM density. The yellow area in the figure is the area where the WM density of the HIV+ group is lower than the HIV− group. The left side of the picture corresponds to the left cerebral hemisphere. WM, white matter. Color images are available online.
The Less WMD Area in HIV+ Group Relative to HIV− Group
p < .05, TFCE multiple comparison correction.
WMD, white matter density.
Correlation analysis
Using a linear correlation analysis, we determined the mean GM volume within the significant clusters (as shown in Fig. 1 and Table 2) were positively correlated with the age of HAART onset, MoCA, MMSE, and CD4 cell counts in the HIV+ adolescents after controlling for multiple comparisons (Fig. 4). There were no significant clusters of WM measures correlated with the MoCA, MMSE, and CD4 cell counts in the HIV+ adolescents after controlling for multiple comparisons. There was also no significant correlation between the GM volume and duration of HAART.
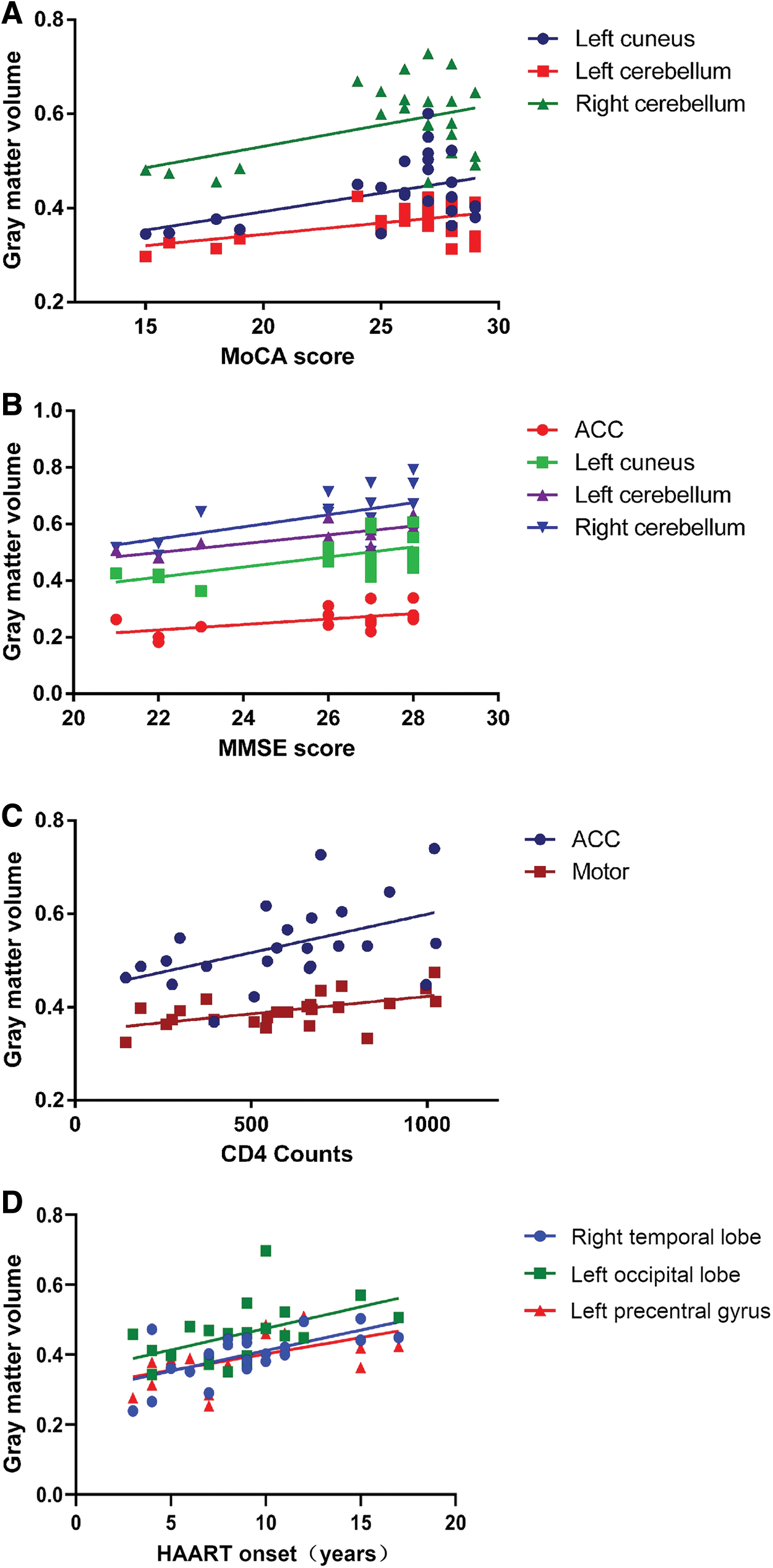
Correlation analysis between the GM volume and MoCA, MMSE scores, and CD4 cell counts after controlling for multiple comparisons in the HIV+ adolescents. The MoCA scores were positively correlated with the GM volume in the left cuneus and bilateral cerebellum
The MoCA scores were positively correlated with the GM volume in the left cuneus and bilateral cerebellum in HIV+ adolescents; the MMSE scores were positively correlated with the GM volume in the left cuneus and bilateral cerebellum; and the CD4 cell counts were also positively correlated with the GM volume in the ACC and the sensorimotor area. The age of HAART onset was positively correlated with the GM volume in the right temporal lobe, left occipital lobe, and left precentral gyrus in HIV+ adolescents.
Discussion
We investigated the differences in GM and WM volume between HIV+ adolescents and an HIV− group using a high-dimension VBM approach. Specifically, we determined that HIV+ adolescents exhibited (1) less GM in the cerebellar regions, the pallidum, and three cortical areas, two of which are mostly linked to visual or visual integration; (2) less WM density in the corpus callosum, bilateral cerebellar lobes, bilateral frontal lobes, left ACC, and left temporal lobes; (3) less WM volume in the posterior cerebellum, right brain stem, and left occipital lobe compared to the HIV− group, and also had more WM volume in the bilateral frontal lobe, left temporal lobe, and bilateral parietal lobe; and (4) significant correlations between the GM volume and the MoCA, MMSE scores, and CD4 cell counts after controlling for multiple comparisons in the HIV+ adolescents. These findings suggest that vertically transmitted HIV infection is associated with altered GM and WM integrity in teenagers.
The brain regions with less WM density in the HIV+ adolescent group were comparable to the brain regions reported in an earlier diffusion tensor imaging (DTI) study, 30 which showed compromised WM integrity in the corpus callosum and frontal lobe. There have been few specific reports of differences in WM density based on T1 images in vertically infected adolescents, although T1 images are not an ideal tool for routinely studying the integrity of the WM. The splenium and genu of the corpus callosum, crucial left–right hemispheric connections, and the inferior longitudinal fasciculus, an important occipital-temporal tract involved in visual processing, show the earliest and most rapid changes of fractional anisotropy (FA) with age. The WM myelin development of these major fiber tracts is near maturity by the age of 11 in typically developing adolescents. 31 By 8–9 months, the development of the corpus callosum is close to that of adults. 32 These results suggest that early HIV infection combined with a lack of viral control, poor immunosuppression, and/or a longer duration of untreated infection may affect the integrity of the WM, especially in the corpus callosum and frontal lobes. Combined with previous DTI findings, we can speculate that the process of corpus callosum formation in the corpus callosum and frontal WM is more susceptible to HIV infection.
Our results showed that the brain regions of the posterior cerebellum, right brain stem, and left occipital lobe had less WM volume in the HIV+ compared with the HIV−. A recent study reported brain structural differences could be observed in HIV+ patients and in vertical transmission HIV+ young people (age range 13–25 years), and less WM volume is present in the corpus callosum, external capsules, and temporal lobe. 22 The possible inadequate penetration of some antiretroviral medications into the central nervous system with resultant poor local control of infection, 33 and our findings of less WM volume may reflect these changes. The etiology of a greater WM volume we observed in perinatally HIV+ youths remains unclear and such findings have not previously been reported. These results may indicate WM injury in perinatally HIV+ adolescents, and another potential explanation could be delayed or altered developmental trajectories depending on the age range studied. In addition, the clinical evaluation of the two groups of patients found that the MoCA and MMSE scores in the HIV+ group were lower than in the HIV−, and the MMSE score showed a significant difference (p < .05), so it can be inferred that the cognitive function of HIV+ patients is impaired.
We found that HIV vertically transmitted adolescents also had less GM in some areas compared with the HIV− group. This finding is consistent with some previous HIV+ adult studies. 12 –14 However, one study showed more GM volume in the putamen, 34 which is not within the brain region in our findings. It is interesting that there were no significant effects in the cerebellum or the ACC, alongside the areas with larger GM between the whole HIV+ group and the virally suppressed group. The whole group reported more significant effects of less GM relative to the 18 virally suppressed, and there were regions with more GM in the virally suppressed, which was not the case in the whole group. The virally suppressed were presenting a different pattern, and in somewhat different regions, but it is not clear how one could interpret the role of poor viral suppression being more or less negative nor does it clearly implicate toxicity. Therefore, the subset of 18 virally suppressed individuals suggested a different pattern that was not completely clear.
Consistent with the results of the previous structural MRI study, 6,8,35 we used VBM to compare the GM volume of the two groups and found less ACC volume of HIV vertically infected adolescents. In further correlation analysis, it was found that the volume of the ACC was positively correlated with the MMSE score and CD4 cell count, which reflected that the structural integrity of the ACC of the HIV+ group was closely related to their cognitive function and immune status. It is believed that the cingulate is part of the limbic system and injury at this brain site may produce the characteristic state of deficits in memory storage. The involvement of the ACC has been highlighted in relationship to HIV-related pathology. Evidence from neuroimaging studies 36 has linked HIV infection and ACC changes that may affect its structure, cerebral flow, diffusion, and metabolism. These findings suggest that altered ACC integrity may represent a promising biomarker of cognitive dysfunction following HIV infection.
During our research, the age at first HIV treatment was variable, with an average age of 8.5 ± 3.3 at first HIV treatment. Although HAART can effectively suppress the HIV systemic burden, poor penetration into the central nervous system (CNS) provides incomplete protection to the brain. Increasing evidence has also suggested that certain HAARTs may cause mitochondrial toxicity and lead to neuronal loss. 37,38 In further correlation analysis, the age of HAART onset were positively correlated with the GM volume in the right temporal lobe, left occipital lobe, and left precentral gyrus in HIV+ adolescents. From the correlation results, it can be concluded that the earlier the treatment, the more disadvantaged the adolescent's brain structure, and the later the treatment, the better the brain structures that focus on language, social interaction (temporal lobe), 39 sensorimotor (occipital lobe and precentral gyrus). In our previous study, we found that the FA values in the bilateral frontal WM were negatively correlated with the duration of HIV treatment, which suggests that a longer treatment duration may be associated with possible neurotoxicity in the frontal WM in HIV+ adolescents. Therefore, the potential neurotoxicity effect of early anti-retroviral (ARV) treatment should be considered.
Differences in GM volume and WM volume may also be the result of inflammation. We know that the neuropathological pathogenesis of AIDS is that HIV is accompanied by HIV virus proteins that cause brain inflammation. 40 Continuous neuroinflammation persists even after initiating HAART. 41 Activation of inflammation may be a hallmark of neurological progression from the asymptomatic phase of HIV infection to the symptomatic phase. 42 In the early stages of HIV infection, gliosis and neuronal loss are accompanied by the upregulation of inflammatory cytokines leading to immune-mediated neuronal damage.
Limitations
A main limitation of this study was the small sample size and cross-sectional study design. Since all subjects in the trial were receiving HAART at the time of having the examination, and the age at first HIV treatment was quite variable, a longitudinal study of adolescents with perinatal HIV infection is required to confirm our results and compare potential differences between the treated and untreated groups. In addition, a larger sample size should be studied and subjects should be subjected to more detailed assessments of cognitive function to determine the association between HIV infection and neurocognitive function.
Taken together, the pattern of less WM density and altered GM and WM volumes suggests that early HIV infection combined with the neurotoxic effects of early HAART and lack of viral control may have a significant impact on brain structural integrity. The process of corpus callosum formation in the corpus callosum and frontal WM is more susceptible to HIV infection. Altered ACC integrity may represent a promising biomarker of cognitive dysfunction following HIV infection.
Footnotes
Authors' Contributions
Z.Y. and J.L. were involved in the conception of the project. J.L. was involved in the design of the study. J.L. collected the data. L.G. and J.L. analyzed the data. L.G. and J.L. interpreted the data. J.L. prepared the article. Z.Y. and J.L. supervised the project.
Acknowledgments
The authors sincerely thank the reviewers of the article and all of the subjects who participated in this study.
Author Disclosure Statement
The authors declare no competing financial interests.
Funding Information
No funding was received for this work.