
Abstract
HIV-infected individuals receiving regular antiretroviral therapy (ART) can present with a high viral load in cerebrospinal fluid (CSF) at times when it is suppressed in blood. This study presents data of HIV-infected patients who had undetectable or low plasma viral load in blood but presented with neurological signs and symptoms and were diagnosed to have CSF HIV viral escape. Records were reviewed for clinical manifestations, details of opportunistic or coinfection, and HIV viral copies in plasma and CSF at time of diagnosis of CSF escape. A total of 10,200 HIV-infected individuals were registered in HIV care till December 31, 2021. Nineteen individuals (14 virologically confirmed and 5 clinically) were diagnosed with high viral copies in CSF from June 2014 to December 2021. Mean age was 41.5 ± 9.2 (median, 39.5; range, 30–62) years. Average duration of antiretroviral treatment received at the time of diagnosis of CSF escape was 10.1 years. Median plasma HIV-viral copies were 2,469.8 (undetectable to 29,418) and in CSF were 12,773.7 (n = 14, range, 1,340–48,530) copies/mL. HIV viral copies in CSF were significantly higher than in plasma at the time of presentation (p = .003). ART regimen switch was done after identification of HIV CSF escape. Seventeen patients were alive with a regular follow-up of average 35 (range 7–66) months. All had documented clinical improvement with reversal of neurological impairment after ART switch. There was one death and one lost to follow-up. Early identification and timely intervention in CSF viral escape could revert severe neurological impairment and improves treatment outcome.
Introduction
Central nervous system (C
Determining HIV viral load in CSF forms an important parameter to monitor the therapeutic effects of antiretrovial (ARV) treatment, for identifying patients with CNS escape (compartmentalization), and also helps in forming a differential diagnosis in HIV patients with psychiatric disorders. 5 CSF viral escape should be looked up in HIV-infected individuals presenting with neurological symptoms while on combination ART. Canestri et al. initially reported discordance in CSF and plasma HIV viral load in 2010. 9 This study evaluated clinical and laboratory data of patients who presented with neurological symptoms and were diagnosed to have CSF viral escape among a large cohort of HIV-infected patients who are under regular follow-up in a tertiary care center and a research institute in North India.
Methodology
The data files of patients who were on regular ART and presented with neurological signs and symptoms and were eventually diagnosed to have CSF viral escape were retrieved from the archives. CSF viral escape was defined by a detectable level of HIV-RNA copies in CSF, indicative of a viral load of >200 copies/mL, when the viral load in the plasma is <50 copies/mL or by an HIV RNA viral load in the CSF that is ≥1 log higher than that in the plasma. 9 Neurological manifestations, if any, were recorded. Demographic profile, details of opportunistic coinfections, absolute CD4 counts at baseline and at the time of CSF escape were noted. Plasma HIV viral load and HIV-viral copies determined in CSF at the time of suspecting CSF viral escape, were recorded.
ART was given as per prevailing National guidelines. History of exposure to prior ART regimens and ART switch, if done after diagnosis of CSF viral escape, was also noted. Patients were subsequently followed up, and the clinical outcomes were recorded. None of the patients were resampled for CSF viral load after ART switch. Appropriate statistical tests were applied using SPSS version 22. The study was approved by Institutional Ethical Committee (IEC No. INT/IEC/2022/SP2.1201).
Results
A total of 10,200 HIV-infected individuals were registered in HIV care till December 31, 2021. Nineteen HIV-infected individuals were diagnosed with CSF viral escape from June 2014 to December 2021. Fourteen patients were confirmed based on plasma and CSF viral levels, and rest of the five patients were diagnosed on clinical assessment and had not undergone CSF viral load testing; however, they had suppressed plasma virus load.
Table 1 gives the demographic details of patients diagnosed with CSF viral escape. Mean age of patients was 41.5 ± 9.2 (median, 39.5; range, 30–62) years with 15 males and 4 females. Average duration of antiretroviral treatment received in these individuals was 10.1 years at time of diagnosis of CSF viral escape. Neurological manifestations were in the form of acute onset of neurocognitive decline, decreased sleep, decreased motor power, unusual behavior, altered talks, disorientation, increased forgetfulness, headache, and limb weakness. Radio-imaging, available for five patients showed features suggestive of encephalopathy. CSF analysis was suggestive of lymphocytic pleocytosis (n = 4, mean cell count: 44.63 cells/mL; lymphocyte percentage: 94.81%) and showed elevated protein (mean: 125.36 mg/dL).
Demographic Profile
3TC, lamivudine; ATV/r, atazanavir/ritonavir; CSF, cerebrospinal fluid; d4T, stavudine; , LPV/r, lopinavir/ritonavir; TDF, tenofovir.
Mean CD4 cell-counts at baseline and at the time of diagnosis of CSF viral escape were 120 and 344.5 cells/mL, respectively. Mean HIV-viral copies in blood were 2,469.8 (range, undetectable to 29,418) copies/mL. The concomitant CSF viral load analysis revealed mean viral load of 12,773.7 (n = 14, range, 1,340–48,530) copies/mL. HIV viral copies in CSF were significantly higher than in plasma at the time of presentation (p = .003) (Fig. 1). In addition to these fourteen patients with a paired plasma and CSF viral load confirming the diagnosis of CSF viral escape, five patients did not undergo CSF viral load testing and were diagnosed based on clinical features. These five patients had absent-to-low plasma viral load but had neurological signs and symptoms in the absence of any CNS coinfections and neoplasms, which was indicative of CSF viral escape. A switch in the treatment regimen was also done for these patients. Clinical improvement noticed after ART switch further strengthened the possibility of the diagnosis of CSF viral escape in these individuals.
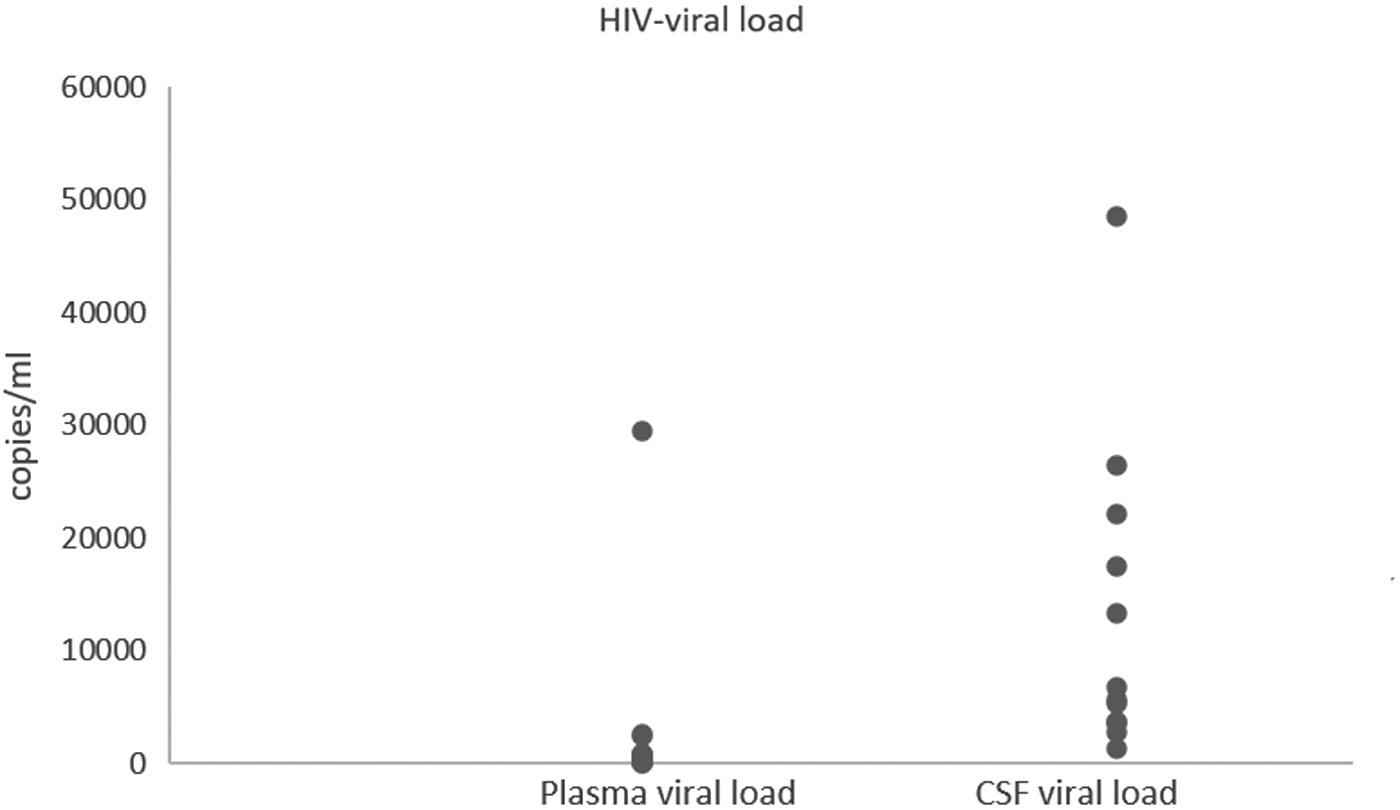
HIV load in plasma and CSF (n = 14). CSF, cerebrospinal fluid.
At the time of diagnosis of CSF viral escape, seventeen patients were receiving tenofovir (TDF), lamivudine (3TC), and atazanavir (ATV)/ritonavir (r) combination therapy, one was receiving stavudine (d4T), 3TC and ATV/r, and one was receiving lopinavir (LPV)/r. After establishment of CSF viral escape diagnosis, therapy was switched to darunavir (DRV) boosted with r and an integrase inhibitor-based combination in all 19 patients. As per program-policy, patients were followed up at least at 1-month interval. At 6 months of ART switch, 17 patients were alive and had significant clinical improvement. There follow-up plasma viral load was undetectable. However, none of these patients had a follow-up testing for CSF viral load. All 17 patients were alive and on regular follow-up for a mean period of 35 months (with a longest follow up of 66 months). There was 1 death and 1 lost to follow-up among the 14 patients with documented CSF viral escape.
Discussion
National AIDS Control Organization (NACO), India, is supporting free antiretroviral treatment services in our tertiary care hospital since January 2005. Till December 2020, a total of 11,937 HIV-infected individuals were registered in HIV care in program. Previous NACO guidelines recommended first-line ART with a combination of two nucleoside reverse transcriptase inhibitors (NRTIs) Zidovudine (AZT)/d4T/TDF +3TC with non nucleoside reverse transcriptase inhibitor (efavirenz/nevirapine) and the second-line ART as a combination of ritonavir-boosted protease inhibitor (PI) ATV/LPV with two NRTI (NACO guidelines). Individuals failing on second line were given DRV/ritonavir with integrase inhibitor as third-line ART. Recent revisions in NACO guidelines in 2021, recommended rapid initiation of combination ART with Dolutegravir (DTG), an integrase inhibitor-based regimen for all newly diagnosed HIV-infected individuals. 10
There are studies available from western countries reporting a discordance, compartmentalization, and an escape phenomenon. 11 Literature gives an evidence of 5%–10% prevalence of CSF viral escape in HIV-infected patients despite on regular ART. 12 HIV particles in CSF can originate from perivascular spaces or infected cells of the meninges, or in plasma and pass through the choroid plexus during CSF production, particularly in the case of damage to or inflammation of the choroid plexus. 11,12
It is reported that CD4/CD8 count reflects changes in peripheral blood and has limited value in prediction of CSF viral escape. 9 Low baseline CD4 cell count, inadequate penetration of ARV drugs, duration on ART, persistent low-level viremia, and emergence of drug resistance mutation in CSF are some of the predictors of CSF viral escape. 9,13 However, we identified a higher CD4 count with median CD4 count 429 (range, 62–754) at the time of diagnosis of CSF viral escape. Autonomous CNS infection or ongoing infection of glial cells and intrathecal immune activation in HIV infection led to severe CNS manifestations. Numerous previous studies estimated that 30%–60% of HIV-infected individuals harbor viral populations that are compartmentalized between blood and CNS. 14 –18 Antiretrovirals, NRTIs have good penetration in brain. Certain factors such as duration of ART received, treatment interruption, and PI-based ART combination therapy are found to be associated with CSF viral escape. 11,18 –20
Gianella et al., suggested that an independent source of HIV RNA contributes to viral rebound within the CSF after treatment interruption. 21 Also, HIV-1 infection in CNS becomes increasingly compartmentalized during disease progression. There is autonomous infection sustained by longer-lived cells within CNS, not requiring replenishment from blood. 15 There are noted adverse disease events with structured treatment interruption in the form of neuronal injury and increased neurofilaments in CSF, augmenting the risk of CSF viral escape. 5,18 –20
Neurological presentation of symptomatic CSF viral escape varies from focal or nonfocal symptoms and signs. There is characteristic finding of CSF pleocytosis, indicating an ongoing inflammatory disorder. 22,23 However, we identified CSF pleocytosis in only 21% (4/19) patients. CNS imaging plays an important role to document encephalitis. Literature gives the evidence of role of biomarkers in neurodegeneration. 22,23 There is also evidence of chemokine, CXCL10, to mediate brain mononuclear inflammation, and it has been linked with increased HIV RNA replication in CSF. 24 However, we did not study inflammatory biomarkers in our population.
We identified CSF viral escape phenomenon in nineteen HIV-infected individuals who had earlier received ART for average 10.1 years at the time of diagnosis. All presented with varied neurological manifestations. Majority (79%, 15/19) of our patients were males. Plasma viral load at the time of such presentation was undetectable to low viral copies. Thereafter, a high clinical suspicion of CSF viral escape was kept, and CSF viral copies were determined, which subsequently showed a higher level than in plasma. CSF viral copies could not be carried out in five patients, although plasma viral load was available for these patients. However, there were subtle neurological clinchers such as neurocognitive decline, decreased sleep, decreased motor power, unusual behavior, altered talks, disorientation, increased forgetfulness, aphasia, in the absence of CNS coinfections and neoplasms, which helped in diagnosis of CSF viral escape. Further, clinical improvement after ART switch in these five patients, strengthened the possibility of diagnosis of CSF viral escape.
Literature gives evidence of 5%–10% prevalence of CSF viral escape in HIV-infected patients, despite on regular ART. 25 A few studies have also previously reported CSF escape from India. 13,25,26 Patel et al. found incidence of CSF viral escape at a rate of 4.4 (95% confidence interval 2.7–7.2) per 10,000 person-months follow-up in patients receiving ATV/r containing ART. 25 Symptomatic or asymptomatic CSF viral escape was also observed in patients receiving PIs monotherapy. 20 These authors also reported neurological signs and symptoms, in the absence of other known etiologies, as the most common presentation.
Eighteen out of 19 of our patients were receiving ATV-based ART. TDF usually achieves a lower CSF level in individuals with concomitant ATV as PI. However, drug levels within brain tissue forms a significant parameter to determine drug efficacy. This combination is largely responsible for escape if there is existing drug resistance and poor adherence. 24 High CSF viral load has been found to be associated with poor penetration of antiretrovirals into CNS compartment which eventually leads to continued replication of HIV in CSF. 27,28 HIV genotype resistance testing was not done in any of our patients diagnosed with CSF viral escape. Research has also proposed CNS penetration effectiveness (CPE) scoring of HIV regimens as a useful tool to compare different drug regimens to improve neurological symptoms in patients with CSF escape. 12,29
The study has several limitations. CSF viral copies were not determined on follow-up. Also, we could not study drug levels in our cohort. Adherence assessment was only done by recall method. We did not analyze association of neuropsychiatric conditions with CSF viral escape. Severity of symptoms was not entered in the records and therefore symptoms could not be correlated with CSF viral load. However, this study highlights future investigation for frequency and consistency of CSF viral escape as a large prospective study in neurologically asymptomatic or stable HIV-infected individuals, receiving standard HIV treatment regimen, is likely to yield useful data. Paired sampling of blood and CSF and determination of biomarkers leading to CNS inflammation and CPE scoring are proposed for future studies. Findings from our study need an extension in the form of longitudinal studies, suggesting utility of measurement of load in CSF compartment, as a strategy to modify treatment regimen and for improved treatment outcome. This might aid in planning long-term treatment strategies in HIV.
Footnotes
Authors' Contributions
R.K.S. and G.S.R.S.N.K.N. conceptualized the study, did the data curation and formal analysis, and did manuscript writing and review. P.C., S.K., and J.K. were involved in data curation. P.J. and S.A. performed the laboratory investigations and validation. A.S. did project administration, reviewed, and edited the manuscript.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding received for this study.
Acknowledgment
Authors wish to acknowledge National AIDS Control Organization (NACO) & Chandigarh State AIDS Control Society for the support.