
Abstract
The effectiveness of self-management programs to improve physical, psychosocial, health knowledge, and behavioral outcomes for adults living with HIV has not been well established. This article reviews the effectiveness of self-management education programs to improve physical, psychosocial, health knowledge, and behavior outcomes for adults living with HIV/AIDS. A systematic review of English articles using CINAHL, MEDLINE, and PsycINFO were used to identify and retrieve relevant studies. Each database was searched from its earliest record to October 2010. Search terms included HIV/AIDS, self-management, self-care, patient education, and education programs. Only studies that (1) reported on a HIV-specific intervention that aimed to increase participants HIV-related knowledge through a self-management component, (2) included a control group, (3) provided skills training or targeted behavior change, and (4) reported clinical outcomes were included. Independent data extraction by one author using the methods described in the Cochrane Handbook for Systematic Reviews. A second reviewer checked the data extraction. Six protocols were reported in eight publications (n=1178), all contained elements of self-management interventions. Effect size calculations were not conducted due to limitations in the available data. The review found randomized controlled trials (RCT) evidence sufficient to infer that self-management programs for people living with HIV/AIDS result in short-term improvements in physical, psychosocial, and health knowledge and behavioral outcomes. Statistically significant improvements were reported for intervention participants compared to control participants across most outcomes. There is insufficient evidence to provide conclusions regarding the long-term outcomes of HIV-specific self-management interventions.
Introduction
The transition of HIV from an acute to a chronic condition means that people living with HIV are now required to take more responsibility for the management of their condition, including making physical, psychological, and social adjustments. Self-management of chronic conditions targets reducing disease progression, managing symptoms and the prevention of disability. 7 Adherence to complex medication regimens often forms a substantial aspect of managing a chronic condition. People living with HIV are required to undertake medication regimens that demand a high degree of adherence and attend 3 to 6 monthly medical appointments. Additionally, they may experience unpleasant side effects resulting from their HIV medications or the virus itself. Research indicates that while optimal adherence rates are 95% or greater, many people report regularly forgetting to take their HIV medications. 6 –8 Consequently, the efficacy of ART can be compromised as nonadherence results in treatment failure and partial adherence may result in the development of resistance to HIV medications.
Physical adjustments are also required from people living with chronic conditions. People living with HIV experience an increased risk for comorbid and coexisting conditions including cardiovascular disease, 9 osteoporosis, 10 dementia, 11 liver, 12 and kidney disease. 13 Additionally HIV medications may produce side effects including nausea, diarrhea, and headaches. It is concerning that people living with HIV have significantly higher smoking rates than the general population in many Western countries with prevalence rates ranging from 40% to 70%. 6,14 –16 Smoking is an obvious risk behavior that may contribute to future comorbid conditions.
People living with chronic conditions are required to adjust to the psychological consequences of their illness. The psychological impact of living with HIV has been well documented. Research indicates that between 10% and 50% of people living with HIV experience depression. 17 –19 Depression among people living with HIV has been linked with impairments in physical and social functioning, general health, overall well-being, and health-related quality of life (QOL). 17 –20
The development of HIV into a chronic condition has increased the importance of addressing personal and social relationships among positive individuals. 21 Research has indicated that QOL among people living with HIV is significantly influenced by social support, coping style, and depression. 22,23 However, health issues, secrecy, issues of disclosure, depression, and most importantly, stigma, present profound barriers to the maintenance of valued relationships and social support. 24 –26 The compounding impact of HIV on the lives of positive individuals often results in social isolation, depression, and withdrawal from previously enjoyed occupations and roles. 25 Stigma poses a prominent threat to numerous domains in the lives of positive individuals, including employment, housing, finances, social support, and professional affiliations. 26 Research has indicated that fear of discrimination hinders disclosure of positive status and reduces access to health services. 26,27 This is concerning considering that disclosure of positive status has been found to be protective against high-risk sexual behaviors. 28,29 People living with HIV clearly struggle with the social and emotional consequences of their diagnosis and would benefit from learning new strategies to assist their management of these issues.
Many interventions have demonstrated successful outcomes in changing health-related behaviors of people living with HIV, 30 –33 however, the majority of these interventions have been guided by models of cognitive behavioral therapy (CBT). At present, no systematic reviews exist that have examined the effectiveness of self-management interventions aimed at assisting people to live with HIV as opposed to enhancing a singular and specific behavioral aspect of HIV management such as adherence to ART or increasing exercise on improving health-related outcomes for people living with HIV.
Self-management, as described by Lorig and colleagues, 34 involves three tasks: medical management, role management, and emotional management, and encompasses six skills: problem solving, decision making, resource utilization, formation of a patient–provider partnership, action planning and self-tailoring. In order to be a successful self-manager, motivation, healthy behaviors, and effective collaboration with health professionals is required. 35 The World Health Organization includes self-management as best practice to improve clinical care and outcomes for individuals with chronic illnesses. 2
As there is presently no cure for HIV, it is necessary for positive individuals to learn about their condition and the most effective strategies to manage HIV in daily life in order to optimize their health outcomes. Support to improve the physical, psychological, and social outcomes and ultimately improve QOL for people living with HIV is clearly required. The objective of this systematic review was to (1) provide a synthesis of the literature on disease-specific self-management interventions for people living with HIV, (2) summarize the evidence of the effectiveness of health education interventions on physical and psychosocial health outcomes and health-related knowledge and behaviors among people living with HIV, and (3) to provide recommendations for future research and intervention development efforts.
Methods
Electronic searches of three databases (CINAHL, MEDLINE, and PsycINFO) were used to identify and retrieve relevant studies. Each database was searched from its earliest record to October 2010. The main search terms were HIV, AIDS, self-management, self-care, patient education, or education program. All search terms were truncated, adjusted, and exploded to match the specific databases being searched. Manual searches of reference lists of relevant studies were also conducted. We included only published literature and conference proceedings were excluded.
The titles and abstracts of the studies were screened and evaluated against a priori inclusion criteria. Interventions included may have identified as “self-management,” “patient education,” or “self-care” and may have been delivered in individual or group settings. Studies were included if they (1) reported on a HIV specific intervention that aimed to increase participants HIV related knowledge through a self-management component, (2) utilized an experimental design in which individuals were randomly allocated to experimental and control conditions, (3) provided skills training or targeted behavior change, and (4) reported clinical outcomes. No restrictions on the duration, frequency, and mode of delivery of the intervention or the discipline of the health provider were applied. Studies were excluded if they (1) were based solely on CBT, (2) specifically targeted HIV-positive drug users, or (3) exclusively targeted participants from African countries. The authors believe that these populations experience issues that are contextually unique and are therefore less generalizable to others living with HIV. Additionally, interventions for which the primary outcome of interest was medication adherence, progressive and aerobic exercise, or nutrition were excluded as they have been covered in previous systematic reviews. 30 –33,36 Studies targeting adults who were “at risk” of HIV infection but were not currently infected were also excluded.
Assessment of methodological quality
Two reviewers independently assessed the quality of each study using Kmet's assessment tool for quantitative studies. 37 The checklist comprises 14 questions and a scoring system. Reviewers used the Kmet guidelines and instructions to assist in evaluating the quality of the articles. Calculated scores were defined as strong (>80%), good (70–80%), adequate (50–70%), or limited (<50%). Discrepancies in scores between reviewers were resolved by discussion.
Data extraction
The first reviewer independently extracted data from the potential studies using the methods described in the Cochrane Handbook for Systematic Reviews for Interventions. 38 Data extracted included: study objectives; study design; method of participation selection; characteristics of participants; random allocation; blinding of investigators; blinding of participants; outcomes; sample size; analytical methods; estimate of variance; confounding controls; results; and conclusions. A second reviewer checked the data extraction and any data queries were resolved through discussion.
Data synthesis and analysis
Due to variability across studies in outcomes of interest coupled with insufficient data, a meta-analysis was not possible. A narrative analysis of the interventions of the articles was undertaken instead.
Results
Electronic searches located 240 articles after exclusion of duplicates. Titles and abstracts were reviewed and a priori criteria applied, resulting in the elimination of 204 articles. Full text review of the remaining 36 articles was then conducted. After eliminating articles not meeting the selection criteria, 6 applicable articles were identified. Two additional articles were identified and included from manual searches of reference lists of articles. A total of 8 articles were identified as meeting the inclusion criteria reporting on 6 different intervention protocols with a total of 1178 participants. All 6 interventions were RCTs. See Fig. 1 and Table 1.
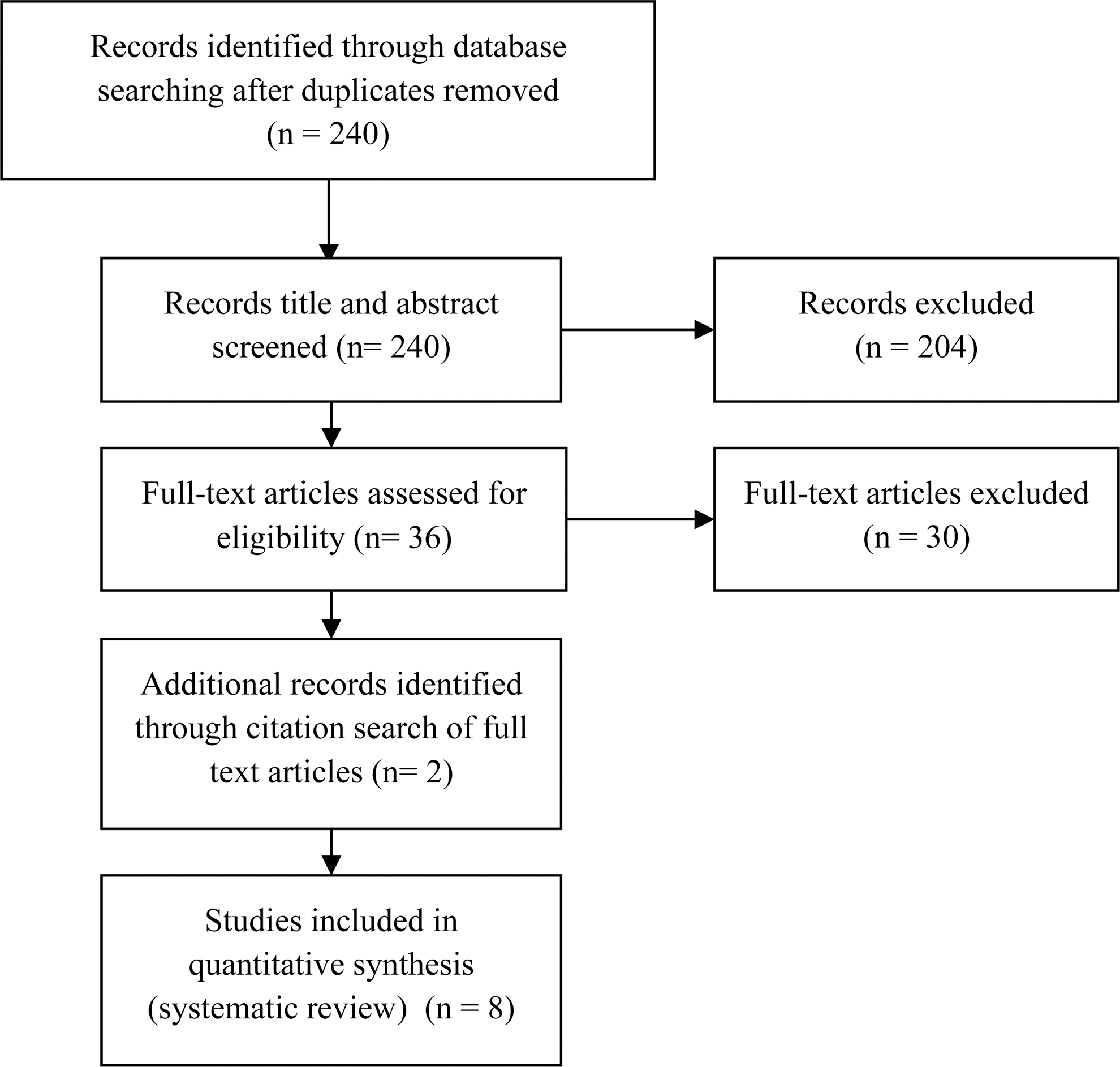
Flow diagram of study selection.
SSI, Symptom Severity Index; MOS, Medical Outcomes Study; CES-D, Center for Epidemiologic Studies Depression Scale; PSS, Perceived Stress Scale; SSES, Symptom Self Efficacy Scale; RSES, Rosenberg's Self Esteem Scale; MSSKQ, Medication Side Effects Self-Care Knowledge Questionnaire; QLI, Quality of Life Index; KPS, Karnofsky Performance Status; MEMS, Medication Event Monitoring System; SSC-HIVrev, Revised Sign and Symptom Checklist for Persons with HIV Disease; HAT-QoL, HIV/AIDS Targeted Quality of Life Instrument; ACTG, Revised AIDS Clinical Trials Group Reasons for Non-Adherence to Medications; REALM, The Rapid Estimate of Adult Literacy in Medicine (REALM); STAI, State Form of the State-Trait Anxiety Inventory; ABS, Affect Balance Scale; SRS, Social Relationships Scale; LOT-R, 12-Item Life Orientation Test-Revised; RCT, randomized controlled study.
Quality assessment of studies
Overall, the methodological quality of the included articles ranged from adequate to very strong (Table 2). Shortcomings included small sample sizes and lack of blinding, which are common in studies requiring active participation. Additionally, several studies used measurement tools for which the psychometric properties had not been established as they were developed specifically for the study. 39 –44 Summed scores were not always provided, making it difficult to calculate effect sizes.
Interventions strategies
Interventions varied between the protocols, however, all contained elements of self-management education programs. Two programs specifically identified as self-management interventions, 39,41,42 while others identified as a peer-based symptom management intervention, 45 a symptom management program, 40,46 a symptom management manual, 43 and coping effectiveness training. 44
Comparison groups also varied between the protocols. The self-management intervention described by Gifford 39 was compared to a usual care control group; Inouye's 41,42 self-management training intervention was compared to a wait list control group who received only standard care from their primary care providers; Webel's 45 peer-based symptom management intervention was compared to an HIV symptom management strategy manual; Chiou's 40,46 symptom management program was delivered in both one-on-one teaching and group teaching and compared to the control group who received telephone counseling only; Wantland's 43 symptom management manual was compared with a general nutrition booklet; and finally, Chesney's 44 coping effectiveness training was compared to HIV-information and wait list control groups.
Intervention outcomes
Three broad outcomes—physical health, psychosocial outcomes, and health knowledge and behavior outcomes—were evaluated. Physical health outcomes included CD4 cell count, symptom severity, and side effects; Psychosocial health outcomes included self-efficacy, quality of life, coping, depression, and self-esteem; Health knowledge and behavior outcomes included health-seeking behaviors, risk behaviors, knowledge, drug adherence, and service access/utilization.
Changes in physical health status were examined in six of the eight studies. The RCT conducted by Gifford 39 found that the Positive Self-Management Program (PSMP) resulted in statistically significant reductions in symptom severity (mean change PSMP −0.9; Control +0.5; p<0.03) compared with the control group using a symptom severity index. However no significant effects were found for pain (p=0.31) and fatigue (p=0.15) (mean change PSMP pain: −9.8 fatigue: −0.7; control pain: −3.5 fatigue: +1.9). In the RCT conducted by Chiou, 40 the symptom management program resulted in a statistically significant improvement in CD4 cell count for both the individual teaching and the group teaching experimental groups compared to the control group (difference of CD4 between pretesting and posttesting individual teaching: 37.09 mm3 (p<0.05); group teaching: 39.98 mm3 (p<0.05); control: −7.46 mm3 (p=0.636). A significant positive effect on reducing viral load was also reported by the individual teaching group (−14613/mL, p=0.014) and the group teaching (−11779/mL, p=0.005) compared with the control (−575.46/mL, p=0.297). Median differences between pre and post testing of the three groups were compared and a statistically significant difference was found (p<0.05). Mann-Whitney U test revealed median differences of the individual teaching group (z=−2. 234, p=0.025) and the group teaching (z=−2.059, p=0.040) were greater than the control. For participants in Inouye's 41,42 studies of a 7-week self-management training and education program, no significant differences were found for performance status as measured by the Karnofsky Performance Status scale (pretest mean=87.5, posttest mean=88.6, p>0.05), CD4 cell count (pretest mean=474.2, posttest mean=390.4, p>0.05) or mean number of physical symptoms reported (pretest mean=7.2, posttest mean=9.0, p>0.05). Webel's 45 RCT of a peer-based symptom management intervention found a downward trend in symptom intensity among participants in the intervention compared to the control group, however, this difference was not statistically significant. Intervention participants in Wantland's 43 RCT of a HIV symptom management manual demonstrated statistically significant reductions in symptom frequency and intensity compared to control participants at the conclusion of the intervention using a mixed model growth analysis (t=2.36, p=0.018).
Seven studies reported on changes in psychosocial outcomes. Gifford's 39 self-management program resulted in significant improvements in self-efficacy for controlling symptoms among intervention participants compared with control participants (mean change PSMP +4; control −7; p=0.02), however no significant differences were found for depression, anger or stress. Chiou 46 found no significant differences in self-esteem as a result of the symptom management intervention. A statistically significant improvement in pre and post testing of QOL was found in Chiou's 46 RCT among both intervention groups (individual intervention p=0.004; group intervention p=0.031) compared to the control group (p=0.506) with QOL difference between pretesting and posttesting being 1.20, 1.43, and −0.32, respectively. Inouye's 42 RCT of the 7-week individual self-management training and coping skills training intervention found significant improvements in mood (F(1, 29)=5.79, p<0.05) and coping strategies (F(7, 24)=2.62, p<0.05) among participants receiving the self-management intervention compared to participants in the control group. Nonsignificant increases in QOL were demonstrated by intervention participants (p value not provided; improvement of 5.75% for intervention group versus reduction of 0.39% for control group; p value not provided). Effects of the intervention were found to interact significantly with the number of symptoms reported by subjects with participants who had the highest number of symptoms benefited more from participating in the self-management intervention. 41 Webel's 45 study using the PSMP found no significant improvements in QOL as a result of the intervention.
Participants in Chessney's 44 coping effectiveness training (CET) demonstrated statistically significant improvements post intervention compared to HIV information (HIV-Info) only control in levels of perceived stress (CET: pre 18.2, post 14.3; HIV-Info: pre 16.3, post 16.3; p=0.04), burnout (CET: pre 24.9, post 17.4; HIV-Info: pre 20.7, post 22.3; p=0.02) and coping self-efficacy (CET: pre 140, post 168; HIV-Info: pre 148, post 154; p=0.02). Statistical trends were demonstrated for positive morale (CET: pre 11.8, post 14.8; HIV-Info: pre 13.2, post 13.4; p=0.09) and social support (CET: pre 66.1, post 73.6; HIV-Info: pre 66.0, post 71.0; p=0.09). Additionally, CET participants demonstrated statistically significant improvements in levels of anxiety (CET: pre 46.8, post 40.7; HIV-Info: pre 47.1, post 44.9; p=0.04) and positive states of mind (p=0.04) when compared to wait list control. 44
Five of the eight studies evaluated changes in health knowledge and behaviors. No significant changes in stress management, relaxation exercises, or HIV/AIDS knowledge were demonstrated as a result of Gifford's 39 positive self-management program. A trend for increased physical activity was also demonstrated (p=0.06). Chiou 46 reported significant improvements in self-care knowledge for both intervention groups compared to the control group with the individual teaching mean increasing by 8.26 postintervention (p<0.001); group teaching mean increasing by 8.41 (p<0.001) compared to the control mean improvement of 0.73 (p=1.22). Significant reductions in the number of unscheduled hospital visits for the intervention groups (1: −0.48, p=0.017; 2: −0.36 p=0.035) compared with the control group −0.045 (p=0.655) were also demonstrated. Chiou's 40 study found significant improvements in drug adherence among the intervention groups [(1) 5.03% improvement (p=0.004); (2) 6.19% improvement (p=0.004) compared with the control (1.42% improvement (p=0.777)]. Significant improvements in health attribution (p<0.05) were demonstrated by participants in Inouye's 42 self-management and coping skills training program compared to control participants. No significant improvements in drug adherence were reported by Webel 45 using the Revised AIDS Clinical Trials group reasons for nonadherence to medications assessment.
Discussion
This systematic review sought to identify and critically appraise the literature regarding the effectiveness of self-management education programs on improving physical, psychosocial, and health knowledge and behavior outcomes for people living with HIV/AIDS. The review found RCT evidence sufficient to infer that self-management programs for people living with HIV/AIDS result in short-term improvements in physical, psychosocial, and health knowledge and behavioral outcomes. Statistically significant improvements were reported for intervention participants compared to control participants across most outcomes. All of the studies examined short-term outcomes with only one study 44 evaluating outcomes beyond 3 months. Consequently, there is insufficient evidence to provide conclusions regarding the long-term outcomes of HIV specific self-management interventions.
The Stanford Program (The Positive Self-Management Program [PSMP)) has been widely accepted and used across America and the United Kingdom. Evidence of its efficacy however, is conflicting. The PSMP consists of a 7-week peer-led group intervention targeting symptom and medication management, communication with health care providers, exercise, nutrition, and goal setting for behavior change. Gifford 39 reported reductions in symptom severity and an increase in self-efficacy for symptom control and physical activity as a result of participating in the PSMP, however the more recent study conducted by Webel 45 found no significant improvements in symptom intensity, QOL or medication adherence in women living with HIV who participated in the PSMP. Differences between these studies include the fact that Gifford's participants were more recently diagnosed with HIV and had more symptoms at the beginning of the intervention. Advances in the medical management of HIV and consequently changing needs of people living with HIV may have also contributed to the conflicting results between these two studies, with Giffords' study conducted in 1996 and Webels' in 2008. Although the program was updated between the studies, it was not based on a new needs assessment which would be required to accurately identify the changing needs of people living with HIV.
Chiou's intervention comprised a 3-week individual or group teaching class targeting symptom management. 40,46 Telephone counseling was also available for participants in the intervention groups. The improvements reported in Chiou's studies 40,46 in self-care knowledge, number of unscheduled hospital visits, CD4 count, viral load, drug adherence, and QOL are promising. Similar results were found between the individual and group interventions when compared with the control intervention indicating either mode of delivery is appropriate. The telephone counseling provided in addition to the individual or group teaching may account for this finding as participants in both groups were provided equal opportunity to clarify information and skills content on an individual basis.
The average duration of HIV-positive diagnosis for participants in Chiou's study was 2.5 years and participants had been on HAART for an average of 2.2 years. 40,46 A possible explanation for the positive results obtained through Chiou's intervention, which was conducted in 2003 may be that participants were relatively recently diagnosed and had relatively recently began taking HAART medications. In Webel's study, conducted in 2008, the average duration of HIV positive diagnosis was 12.5 years and participants had on average began taking HAART for 8 years. 45 We may be able to infer that individuals recently diagnosed with HIV would benefit more from self-management interventions targeting symptom intensity than those who have been living with HIV and on HAART for longer periods of time. Chiou's intervention also specifically targeted the management of side effects from HAART and thus, may have recruited participants who were experiencing side effects. 40,46 Wantland's findings of a significant reduction in symptom frequency as a result of using a symptom management manual promoting self-care for 3 months compared to a nutrition manual also highlights the benefits to be obtained from self-management with regard to symptom management for people living with HIV. 43
Chesneys' study of a 10-week group intervention using coping effectiveness training provides encouraging support for the effectiveness of self-management programs to improve psychosocial outcomes for PLWHA including stress and burnout, anxiety and self-efficacy. 44 Additionally, the design utilized by Chesney allowed for comparison between CET and an active informational control condition, with results indicating that provision of information material alone is less effective than CET in reducing psychological distress and enhancing coping in PLHIV. 44
Empirical evidence for the effectiveness of self-management programs improving the specific outcome of adherence to HAART has been provided in a literature review conducted by Ruedea et al. 33 Additionally, data supporting self-management interventions specifically aimed at increasing exercise among PLHIV have been reported. 31,32 A Cochrane review analyzing the effectiveness of lay-led self-management interventions for people with chronic conditions found that in the short term, these programs improve health status, improve cognitive symptoms, and frequency of exercise and also increase self-efficacy to manage symptoms. 47 Considering the findings of this review in light of previous research suggests that HIV specific self-management programs may improve physical, psychological, and behavioral outcomes.
The small number of studies, lack of reported effect sizes, and methodological quality of the studies limit the findings of this review. This review only searched for articles located in three databases. These databases are, however, most likely to identify research in this field. Only published peer-reviewed articles were included in the review. Additionally, specific searches of HIV/AIDS journals were not undertaken. There was a lack of consistency in outcome measures and analytical methods across the studies, however, this is typical of complex intervention studies. There was also considerable variability in the method of delivery and frequency of the interventions. Furthermore, two of the included studies 39,44 were conducted prior to HAART and therefore may not accurately represent PLHIV in the current HAART era. Overall, the heterogeneity of outcomes coupled with these limitations mean that reaching conclusions about what aspects of self-management programs work or do not work is difficult.
Interventions that targeted more specific behaviors such as coping or symptom management 40,43,44,46 appeared to be more effective than programs that have a boarder focus and targeted several different behaviors. 39,41,42,45 Chiou's study was the only one to evaluate individual versus group delivery. 39,46 While the individual teaching group demonstrated slightly greater improvements compared with group teaching across the majority of outcomes, making a solid conclusion about the effectiveness of group versus individual interventions for people living with HIV is not possible at this stage. Chiou's study found similar results between the individual and group interventions when compared with the control intervention indicating either mode of delivery is appropriate, however this may have been influenced by the additional telephone counseling offered to participants in both experimental groups. 39,46
People living with HIV are presented with unique and complex issues including stigma, disclosure and managing HIV within intimate relationships. Due to the success of ART, people with HIV are living longer and consequently aging. The increasing population of people who have been living with HIV for long periods of time are now experiencing additional chronic and comorbid conditions such as cardiovascular disease, depression, liver and renal diseases, and cancer. Accordingly, self-management programs targeting people living with HIV should alter their focus to incorporate the prevention and management of such conditions.
While there is limited evidence of the effectiveness of self-management programs improving health status, programs have consistently demonstrated improvements in symptom frequency and intensity, psychosocial, and mental health needs of people living with HIV. More research is needed to evaluate the effectiveness of self-management programs improving social support, the management of HIV within intimate relationships and quality of life.
Programs which are HIV specific provide the opportunity for PLHIV to learn in an environment where they are supported and not at risk of discrimination. Researchers have began to evaluate the effectiveness of self-management interventions delivered online with the aim of reducing barriers to access including stigma, rural and remote locations, and confidentiality issues. 45,46 Due to the sensitive and complex issues faced by people living with HIV, online self-management programs are viable options that should be further explored. Additionally, researchers need to streamline assessments used to evaluate the effectiveness of their interventions in order to provide more uniformed, interpretable, and comparable results. Future research should focus on participant follow-up and intention-to-treat analysis.
This review found RCT evidence sufficient to infer that self-management programs for people living with HIV/AIDS result in short-term improvements in physical, psychosocial, and health knowledge and behavioral outcomes. Statistically significant improvements were reported for intervention participants compared to control participants across most outcomes. Clearly, targeted self-management interventions informed by thorough needs assessments could provide beneficial outcomes for PLHIV.
Footnotes
Author Disclosure Statement
No competing financial interests exist.