
Abstract
Previous research suggests that incarceration can have a negative effect on health. These health effects have an especially profound impact on HIV-positive individuals. As such, the current study investigates how incarceration affects the health of 12 African American HIV-positive formerly incarcerated males recruited via an AIDS Service Organization. Individuals were enrolled via purposive sampling and engaged in a series of in-depth interviews over a yearlong period (n=46). Participants ranged in age from 33 to 61 years. Most had finished high school, were not employed at time of first and last interview, and most were primarily residing at a homeless shelter. The time incarcerated ranged among participants from 3 months to 3 years. Findings suggest that health is impacted via limited and delayed access to medication, stigma, and poor quality of medical care while incarcerated. Health continues to worsen after release, largely due to incarceration's impact on individuals' social context. Macro-level policy limits opportunity to fulfill basic needs such as housing and hinders one's ability to be gainfully employed. Moreover, stigma, loss of social support, and a delay in accessing HIV-related services deleteriously impacts individuals' mental and physical health status. Implications for practice, policy and future research are also discussed.
Introduction
The populations most at risk of becoming incarcerated, including African Americans, are similarly at increased risk of becoming HIV positive. The rate of HIV among those who are incarcerated is estimated to be 4 to 6 times higher than that of the general population of the U.S. 5 In 2010, 1.5% of inmates were HIV positive, and 20% also had AIDS, representing an AIDS rate over two times that found in the U.S. general population. 6 Additionally, incarcerated individuals often experience concurrent disorders that negatively affect their health. Research has shown that mental illness, substance use, and socially marginalizing conditions such as poverty are prevalent in incarcerated populations. 7 –10 Therefore, those who are most likely to experience incarceration are also at increased risk of experiencing HIV and other co-occurring conditions that have been demonstrated to be proximal predictors of health.
Possibly exacerbating the effect of HIV on incarcerated individuals' health is the medical infrastructure within the prison or jail setting. 11 Whereas some research has demonstrated that incarceration healthcare can be stabilizing or provide care that would have not otherwise been attained, 12 there is still a need to investigate the ways in which the healthcare system within correctional facilities impacts HIV positive individuals. Hatton, Kleffel, and Fisher 13 investigated the specific issues related to healthcare access for incarcerated individuals and found that administrative errors, hygiene issues, mandatory requirement of co-payment, delay in obtaining needed medications, side effects from medicine, administration of wrong medications, and allergic reactions to medications were common and often negatively affected the health of inmates.
Research has also demonstrated that incarceration affects individuals' post-release social conditions. During this transition period, a history of incarceration can affect one's ability to find employment or job training, access to medications, ability to find housing and shelter, and secure the provision of social or medical services. 14 –18 These worsened social conditions also have a negative impact on self-rated health and health-care service utilization. 19,20 Adherence and maintenance of routine engagement in medical services is often a struggle for HIV-positive individuals after release from incarceration, due in large part to the fact that a history of incarceration itself can be a barrier to adhering to HIV anti-retroviral medications. 21 For instance, among injection drug users, Milloy and colleagues 21 found that HIV-positive individuals with a history of incarceration had nearly double the odds of anti-retroviral adherence lapse.
It is important to note that the impact of incarceration during after release may be differentially affected by the type and location of the facility in which a person is incarcerated (e.g., prison versus jail)—meaning it is impossible to draw conclusions about all incarcerated populations as a whole. A total of over 9 million people cycle in and out of jails each year. 22 Jails typically hold individuals who are awaiting sentencing, trial, or transfer to prison, or those who have a sentence of 1 year or less. Federal prisons house those sentenced to more than 1 year. 22 Making the effect even more complex to isolate is the fact that certain types of facilities (regardless of designation) may have entirely different social environments, behavioral norms, variability in access to resources, and are likely to house a variety of individuals incarcerated for differing types of offenses.
Finally, stigma, regardless of the type of facility that an individual is housed in, has been found to have a particularly salient impact on both HIV-positive individuals and those who are incarcerated. 23 Derlega, Winstead, and Brockington 24 found that both inmates and correctional staff rated people who had HIV more negatively than someone with other diseases such as diabetes, cancer, heart disease, and high blood pressure. HIV-positive, formerly incarcerated individuals may also experience multiple forms of stigma that may act as a barrier HIV medical care and social service linkage after release (L. Brinkley-Rubinstein, unpublished observations). For example, HIV-positive, formerly incarcerated individuals may have trouble finding employment due to policies that restrict certain types of jobs for formerly incarcerated individuals, which can lead to several deleterious outcomes potentially affecting health (e.g. lack of health insurance).
Although a large body of literature explores the ways in which incarceration affects health, little research has explored these relationships longitudinally, including both the immediate and lingering effects of incarceration on HIV positive populations. Therefore, the primary aim of the proposed research project is to investigate: (1) how incarceration impacts the health of HIV positive African Americans after release and over time, and (2) how social conditions affected by the process of incarceration impact the health of HIV positive African American males after release and over time.
Theoretical underpinnings
The present study is grounded in a conceptual framework that theorizes that incarceration affects an HIV positive individual's health via: (a) the incarceration experience due to a lack of access to healthcare inside the prison/jail facility; (b) the creation of barriers to HIV medical care and social services after release; and (c) the worsening social conditions (e.g., social support or employment) that are also proximal predictors of health. The framework also takes into account the social environmental risk factors that are both associated with increased risk of incarceration and are proximal predictors of health. The depicted heuristic model (Fig. 1) captures these complex points of intersection. In sum, the current study attempts to understand direct and indirect effect of incarceration on both social conditions and health outcomes, which is an addition to the existing research related to the intersection of HIV and incarceration.
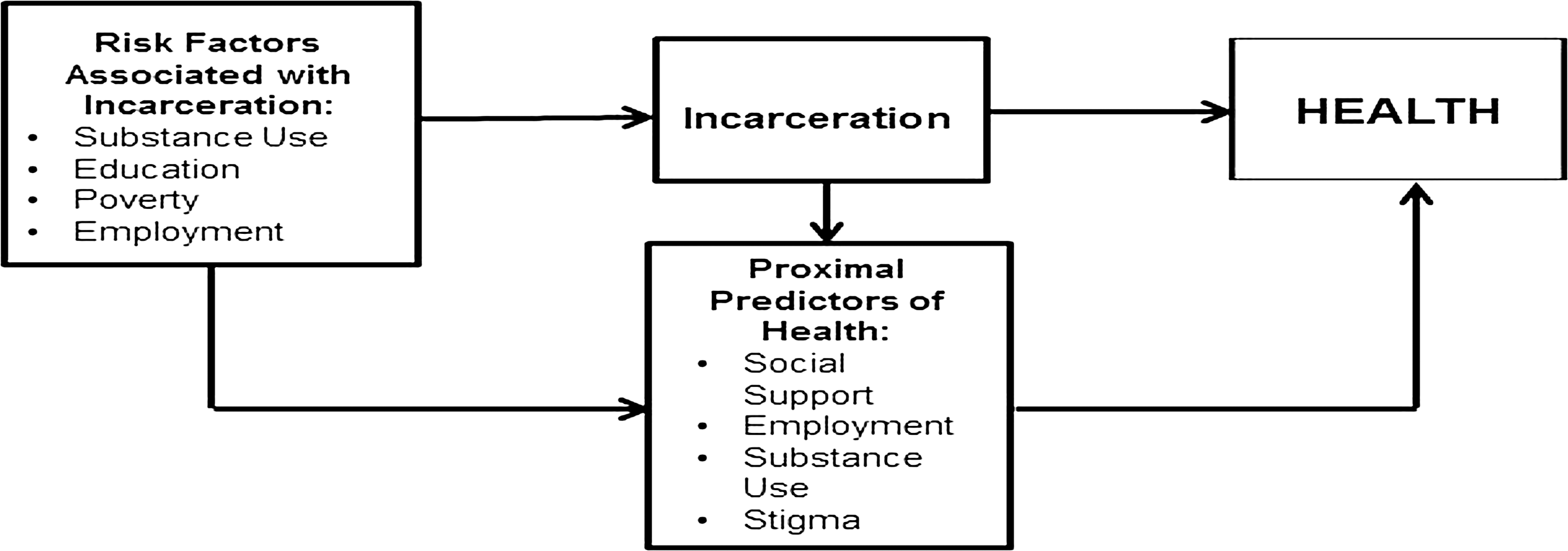
The hypothesized impact of incarceration on health.
Methods
The current study took place in a midsize city in the Southeastern region of the United States (US). At the end of 2008, there were approximately 586,636 people living in the county in which the city is located, of which 28% were African American. However, African Americans represent nearly 51% of all HIV-positive individuals in the county. In total, at the end of 2008, an estimated 3753 people had received an HIV and/or AIDS diagnosis in the county, accounting for one-quarter of the HIV-positive population in the entire state. From 2004 to 2008, 638 HIV positive individuals with residence in this county were incarcerated in a local jail, and 188 in a state prison. 25
Research design
In order to pursue the relevant research questions, the present study employs an ethnographic approach, including at least two interviews each with a total of 12 participants. The first interview was conducted less than 3 months after the participants' release from incarceration, and a subsequent interview took place at least 6 weeks later. The authors conducted multiple interviews with each participant in order to better understand the ways in which incarceration affects health immediately after release and over time, as an individual reintegrates back into the community. The research design of this study facilitates opportunities for uncovering important nuances in the participants' lives. 26
Respondent selection and recruitment
A local AIDS Service Organization (ASO) helped to recruit participants, and enrollment took place after release from incarceration. More specifically, an early intervention specialist (EIS) who is trained and funded to work with people who are formerly incarcerated evaluated, upon post-release assessment, whether an individual was interested in being involved and met the study criteria. This study utilized purposive sampling and, as such, an individual was eligible to participate if they were: (1) African American; (2) male; (3) HIV positive; (4) had spent at least 3 months in jail or prison, and; (5) were released within 3 months of enrollment in the study. If study criteria were met, the potential participant was given information about the research project and provided their contact information to the EIS. This information was then shared with the research team via the EIS and contact with the possible participant was made. If an individual was still interested in being a part of the study, an information session was scheduled. At this initial meeting, the authors provided details about the study, consent documents were signed, and an initial interview was arranged.
The first 12 participants who were willing to take part in the study and met the eligibility requirements were enrolled. The small sample size was balanced with a longitudinal design and multiple in-depth interviews that enabled the authors to learn about sensitive topics (e.g., HIV, incarceration) and to engage intensely with the participants over time. By generating comprehensive understanding and obtaining rich thick descriptions of incarceration's impact on health, the authors aim to formulate propositions and provide a foundation for research in this important field. 27 To enhance validity and reliability, the authors undertook the following procedures: (1) engaged in peer debriefing in which a colleague familiar with the data reviewed interview tools, transcripts, and analysis throughout the research process; (2) provided transcribed interview summaries to the participants during their second interview. These member checks gave participants the ability to corroborate the interpretation of the interview and to elaborate on or clarify any specific topics; and (3) transcripts were coded by two different coders and 90% inter-related reliability was required. 27 –29
Interviews
Participation in this study included being interviewed by a member of the research team, at least two times for approximately 1–2 h. A semi-structured interview guide was developed and included broad themes related to incarceration and health. The guide was very broad and included questions related to the participants background, history of incarceration, and general health status. Interviews were conducted face-to-face at a location that was convenient and accessible to the participant. Due to the sensitive nature of the subject matter being discussed, the interviews did not take place in public; instead, they were conducted in a private space in a public venue. For example, interviews were often undertaken in a private room in a community center or the public library. The venue of the interview was also determined by the participant's location/neighborhood in an attempt to ease the burden that may have been caused by lack of access to transportation or family obligations (e.g., lack of childcare).
Data analysis
In qualitative research, data collection and data analysis occur simultaneously. All interviews were recorded and subsequently transcribed. Analysis of interview data proceeded inductively through the identification of recurring themes and patterns in transcripts, field notes, and analytic memos. 30,31 Meaningful analytical units were then developed by using a coding scheme that was informed by dominant themes in the data. These topics were then divided into several subtopics based on recurring themes within the larger topics, allowing for more in-depth analysis and complex understanding and interpretation of each particular theme. Each theme and subtheme was then assigned a code, and the codes were compiled in a codebook. The authors then clarified the codes' definitions and ensured that all codes fit into a structure with meaningful and salient inter-relations and distinctions among them. 32 Open and axial coding were then used simultaneously as data were delineated into concepts. Subsequently, the relationship between concepts and categories were analyzed. Quality checks were undertaken to ensure high inter-and intra-coder reliability among coders. After initial coding of the data, the authors summarized and organized the resulting data in Nvivo 9 (QSR International, Burlington, Massachusetts, USA). After attaining inter-rater reliability of 90%, defined as the number of agreements divided by the number of agreements plus disagreements, 29 authors coded all data. The resulting data were utilized to examine the specific research questions guiding the proposed study. Coding of the data coincided with data collection so that the follow-up interviews could build upon the themes that emerged from the first interview with participants.
Results
Participants ranged in age from 33 to 61 years. Most of the participants had finished high school (n=8), but only one spent some time at an institution of higher education. At the time of the first interview, none of the participants were employed and most were primarily residing at a homeless shelter (n=10). The time incarcerated ranged among participants from 3 months to 3 years across each type of correctional facility, including local jails and state and federal prisons. During the interviews, participants talked about their experiences with incarceration and their perceptions of how incarceration influenced their health. Participants discussed the ways in which incarceration affected their engagement with HIV medical and social service agencies post release and their transition back into the community. Follow-up interviews conducted with each participant facilitated an investigation into whether barriers presented by incarceration eased over time.
Incarceration and the health of HIV-positive individuals
Participants often discussed their perception of how incarceration might have affected their health. Several major themes emerged that included: the quality of care while incarcerated, access to medications and other medical services, and stigma related to their HIV status.
Quality of care
During interviews, several participants discussed the quality of care they received in various settings. The participants spoke about the issues that prevented them from receiving adequate medical care, and frequently hypothesized how this lack of access to quality care might affect their health status. For instance, one participant said:
Yeah, cause you know, like one of the new medicines, it said, “Take two once a day.” And they was giving me one. Being they were given to me at night, I said, “Well, is there any difference between day and night? They say, “Take two once a day.” They didn't say take it at bedtime. But I guess as long as I take it during the day, you know.
This participant knew that he was receiving an incorrect dosage of his HIV medicines and knew that this might deleteriously affect his health, yet did not feel empowered enough to advocate for himself. Another participant stated that he was afraid he was going to die due to the lack of good medical care while incarcerated. He said:
I thought I was gonna die in jail ‘cause I wasn't getting the medical treatment that I needed, and with me being HIV [positive] and 60 years old. And, like I said, I thought that this was it. My worst fear was to die in jail. Two things: die in jail or die high. I don't want neither one of those.
Finally, a participant described the initial medical intake period and how he felt that the staff assumed he had low levels of understanding related to his HIV and treated him accordingly. This same participant indicated that, even though the medical staff acted as if they knew the best course of action for his treatment, he soon became sick due to the antiretroviral medication he was prescribed:
So then they, the nurse came in to interview after he did and I did the same thing with her. So she said, they gonna be calling you for a physical. I'm putting all this in your chart. She told me right there on the spot when she looked at what kind of medicines that I was taking, she told me that we gonna change, but I guess she thought I was stupid, that I don't know what I take, she was like, well we gonna change your medicine because we don't carry this brand and it's gonna be the same pill but two of them pills gonna be in this one pill and, come on man you change my medicine all the way around, when ya'll started giving me this stuff and I started getting sick.
These examples denote that quality medical care was hard to come by in the incarceration facility in which the participants served their time, and that they were very aware of the possible effects of the less than adequate care might have on their health status. Resistance of medical professionals to consider the participants to be active agents of their own health compounded the impact of the lack of quality care.
Access to medical service and medication
In addition to reporting a low quality of care within prison or jail, many participants stated that they had a complete lack of access to healthcare and often lacked access to their HIV-related medications. One participant stated: “I believe that's one of the reasons that my health was bad, I didn't have my medicine right then, but I think about a month later, they started getting my medicine in there.” Another participant indicated that the jail's medical staff refused to give him his HIV-related medication, and he was forced to secure access to the proper medication through his family. He stated: “I had told the nurse and they couldn't get the medicine so I had to call home to get my brother to drop it off, they had to bring it up there and drop it off.” Another participant, who didn't have the option to have a family member or friend drop off their medications, reported that he did not have access to medications while incarcerated, and that not taking his medications affected his health:
They don't have none. They didn't have none at all. I was like, wow! I would die here. ‘Cause I mean, you know I was doin’ so good when I was out, ‘cause I take my medicine like I was supposed to. After I been in there, I kinda dropped a little bit cause I missed them days.
As evidenced by the clear sense of stress conveyed by each participant when referencing medication lapses, lack of access to medications can be devastating to HIV-positive individuals. Research has shown that antiretroviral adherence lapse can deleteriously affect an HIV-positive individual's health status by causing them to become resistant to certain types of medications. 33 Once a regimen becomes ineffective, an individual's CD4 count can decrease and the viral load can increase, which can cause sickness. Throughout the interviews conducted with the participants, most realized how important it was to consistently take their prescribed medications but discussed the difficulties with doing so while incarcerated.
HIV stigma
Whereas participants discussed the direct effect of quality of care and access to medical services on their health, they also talked about the indirect impact of stigma within the jail or prison setting. One participant stated: “And they thought that I got, I had problem here [in jail], told the people, the guys in the jail that I had HIV, they didn't wanna be around me.” This quote demonstrates the awareness of the participant of the possible impact of stigma on his incarceration experience. Another participant described the intake process and the steps he took to conceal his HIV status from correctional employees:
When you first go in they interview you. Individually they had us in some rooms and I kinda like, they was asking questions and I kinda like grabbed the ink pen and wrote it down on a piece of paper and slid it to ‘em because other people be trying to listen and see what's, you know and he looked at it and he was like, okay.
In this example, the participant took proactive steps to hide his diagnosis from his inmate peers; however, his willingness to share with the jail staff suggests that he knew that he had to reveal his status in order to secure necessary medications and care while incarcerated. Similarly, another participant described the intake process and described “being branded.” He stated: “When they asked me what it [the medications he reported being currently on] was for I said, I said HIV, I said it's for me to live, I got stamped. I'm embarrassed, and he asked me what I want to do, I tell him I want to deal with it.”
Finally, a participant stated that due to stigmatizing attitudes by the nursing staff after they found out that he was HIV positive, he was refused medical services for a non-HIV related injury. He stated:
Like the counselor, you know like, like I said, I had to write ‘em up to get up, I had to write the medical staff up because of my broke finger. I always be crooked like that now cause I couldn't get medical help. I think the counselor she was all right at first and then after you know she really found out that you know [I was HIV positive] and then she start trying to like treat me a little different.
This quotation reveals that stigma attached to the HIV positive diagnosis had compounding impacts on general health due to experiences of denial of services. As previously discussed, stigma impacts both the physical and mental health well-being of individuals, while also potentially mediating individuals' access to necessary resources.
Other participants stated that they had to obtain their medications via the “med-line”. The “med-line” occurred one to two times per day, and during “med-line” individuals who needed medications would line up and wait for their turn to talk with medical staff and be given their prescriptions. This caused a lack of privacy because individuals in line could often see the type and number of medications another individual would receive. One participant described his experience with “med-line”, saying:
But you know, I wouldn't have been able to stay in the cell if they knew I was HIV. That's how stupid people were, cause when I go up and take my medicine, they stand all up on your back. “How you taking all them medicines,” you know? I said, “Why you in my business?” and stuff. You know, a few of ‘em were saying, “What's the matter with you? You taking all this medicine.” ‘Cause I would have a hand full of medicine I'd have to take and everything. So I think I told one guy. I said, “Well, it's like this. The life I live, I destroyed half my body. I got kidney trouble, liver trouble, hepatitis.” I didn't tell him I had HIV.
This quote demonstrates that the participant felt that due to his participation in “med-line” and the fact that he received so many medications, other inmates would learn of his HIV status. However, because the participant knew how stigmatizing it would be to have other prisoners know of his HIV status, he made up other reasons to describe why he had to take so many medications. This may suggest that HIV-positive individuals are less likely to adhere to anti-retroviral medications by choosing not to participate in med-line if they think their health status confidentiality is at risk.
Post release transition and the effect on health
Participants also reported that the post release transition had a significant impact on their health. This resulted from the cumulative impact of many intersecting experiences, including issues with anti-retroviral medication adherence (specifically related to the most immediate post-release period), enduring stigma related to both their HIV status and their history of incarceration, insecurity of a social support network, including friends and family, and, relatedly, macro-policies that prohibited their ability to obtain housing and employment.
Linkage to care and anti-retroviral medication adherence
Most participants reported that they were released from jail or prison with a 30-day supply of anti-retroviral medication. However, most also reported that 30 days of medication was either not enough due to an extended wait for a post-release medical appointment or issues related to addiction often led to missing appointments before they came. For instance, one participant stated:
But when I got out of prison, I hooked up with [a social service agency] and then made an appointment for [a medical provider], and then you know, I got that job and then before the appointment came, I got that first paycheck and stopped taking my medicine, started smoking crack.
In this case, despite the participant's efforts to transition back following his release, his substance abuse issues lead to missed appointments and a secession of his treatment regimen. Participants also often reported missing appointments because of competing social-structural barriers that plagued their post-release experience. For example, the same participant explained how lack of access to transportation made it difficult for him to keep medical appointments, especially when paired with competing commitments: “I had missed a couple of appointments and my transportation was kinda crazy and I had made an appointment and something had come up at this time and I missed it.” Finally, participants seemed to understand the impact of missing medications and not engaging in routine medical care had on their HIV disease. For instance, a participant who stated that he had a prolonged lapse in adherence to his HIV medications said:
So and then after my doctor's appointment, this was on the 10
th
, after my doctor's appointment, I mean, after the court date I went to my doctor's appointment and found out that I thought I was real sick, but my T cells were still a little over 200 and my viral load, he said was like 55.
This quote suggests that the participant understands that not taking his medications had affected his health deleteriously. In light of the previous findings though, it is likely that the participant, despite his clear sense of health literacy, experienced various compounding barriers that limited his access to care until he reached this critical point.
HIV stigma
Several participants also discussed the impact of HIV-related stigma on their ability to seek services in the community. Many mentioned not utilizing services at all or having to go to a doctor or social service agency across town to avoid being seen by people they might know. For instance, one participant stated:
I couldn't seek services anymore over there. I have two friends who live right next to the clinic. They're always peeking out their window trying to see who is walking in and getting services. So I travel across town to get services so nobody sees me.
Having to travel across town to seek services rather than obtaining medical care at the local community clinic may lead to undue stress and may also lead to less engagement in routine care due to the added transportation burden.
Additionally, participants also spoke about the painful nature of HIV-related stigma within the context of a neighborhood and how living on the street provided a more bearable existence. For instance, a participant stated:
I just smoke crack and not take the medicine. Cause on the streets you can live like you want to live. I mean, to be honest with you, don't nobody care what you got, they don't care what the disease you got, they don't care about nothing. It's all about the crack. So and in some kind of sick way it's, you can feel normal.
This quote seems to suggest that the power of stigma is stronger than the urge to engage in medical care after release and has implications for medical service provision for HIV-positive individuals. In lieu of seeking a stable home and supportive community, the threat of stigma tied to their diagnosis led many participants to the streets where they could assume an anonymous role without harassment or judgment from peers.
Loss of social connections
Further compounding the issues that HIV positive individuals face after their release is the fact that being incarcerated can cause a loss of social support. For instance, one participant stated: “[The prison was] too far away. Yeah, but you know, my granny died while I was in prison. You know, my granny died. They wouldn't take me to the funeral, you know, so I didn't get to see her no more.” Another participant expressed a similar sense of isolation while incarcerated: “And the whole time nobody come to see me. I barely got mail. If I got any mail it's from my momma. I think my mom wrote me a couple of times, but I didn't get no visits.” Research has indicated that lack of social support can deleteriously affect health status especially of those with co-occurring issues, such as HIV and substance use issues. 34,35 These quotes seem to suggest that loss of social connections and support or a feeling of social isolation is a common “side-effect” of incarceration, which can be detrimental to both health and successful reintegration into the community after release.
Resilience through faith
Although participants often discussed the negative effects that incarceration had on their post-release experience, many also shared that they found strength and resilience in their faith. Almost all of the participants relied consistently on their faith to bring them through challenging circumstances. For instance, a participant stated: “And I got locked up again and I prayed and I prayed and I prayed, I asked God to take the desire [to use drugs] away from me and he did and I've been clean since.” Participants voiced that their difficult circumstances had helped them to gain faithful perspective: “It allowed me to be where I'm at. And my disadvantages gave me the experience of my advantages today because I have to thank God that I'm alive and I'm healthy.” This finding suggests that, when considering the design of a possible intervention, faith-based communities should be considered as collaborators.
Macro policy level effects on health
In the past decade, rehabilitation services and policies to help inmates reintegrate to their community have decreased, but the legal and practical barriers have increased. 36 Research has shown that, as a result of the tougher political stance towards crime, a restriction of the rights of ex-prisoners has proliferated. 37 Participants in the current study often discussed how incarceration restricted their access to stable housing (and, subsequently led to homelessness) and gainful employment (which often pushed them into the informal economy).
Lack of access to affordable housing
Formerly incarcerated populations often have trouble securing housing after their release. 36 Further complicating this issue is the fact that federal legislation gives local entities the choice to disqualify individuals who have drug charges from accessing subsidized housing. Several participants indicated that they were affected by this legislation and continued to struggle to find housing long after their release. For instance, one participant stated: “They took that [his right to federally subsidized housing] and that's still in effect right as we speak, will not be eligible to get back on section 8 till 2015.” Other participants stated that before they were incarcerated they were stably housed, but after release they often found themselves homeless: “So when they busted me then, that made me lose my apartment, so my mom came and got my stuff. Didn't have nowhere else to go [other than the homeless shelter].” Another participant who shared that he was living in the woods, under bridges, and sleeping on park benches also stated that he was homeless after release: “So I'm just trying to get my apartment back. I got homeless again after I got locked up.”
Participants often discussed the direct effect that homelessness had on their health, especially around caring for their HIV diagnosis. Specifically, many participants who were homeless mentioned that they often lacked a place to store their HIV medications securely, which led to the pills getting lost, or becoming stolen and, subsequently, resulted in an adherence lapse. For instance, one participant stated:
Yeah, now, when I was homeless, I had, I kept my medicine in a plastic bag where I stick a pill bottle in here, a pill bottle in my pocket, a pill bottle in my sock, you know. I had to keep up my medicine. And then, one of the homeless guys stole my bag with my medicine. So, I've been out of my medicine. Then, I got nothing at least eight months. And then, I couldn't take it [the medicine] no more.
This theme was echoed by multiple participants who had or were currently experiencing homelessness. For example, one said:
I was getting my meds stolen. Everything I had, everybody keeps stealing it what you had in the Mission. They are robbers, they steal food, and I can't get be toting around all that stuff. You know what I mean? And so I kept my meds with me.
In both of these examples, and many others throughout the interviews, participants attributed their housing status with an adherence lapse, due to the lack of a secure location in which to secure his medications. The confluence of social contexts with one's health status resulted in deleterious effects on the impact of his drug regimen and management of the disease, and cannot be overlooked.
Employment
In addition to experiencing homelessness after release, several participants also reported an inability to find gainful employment. One participant stated:
I don't even know cause I've put in so many online [job applications], just that, I had me doing 10 a week. It [incarceration] affect any ex-felon, it affected and affects you real bad cause a lot of ‘em said, it don't matter, but a lot of ‘em still holding it up above your head and it is difficult for someone to come out of prison and get a job.
Another participant added:
I've put in quite a bit [of job applications] since I've been out and I'm still unemployed, so I had to go to the Homeless Paper thing that they got now, where they got you standing on the corner making you legal to sell papers, but that ain't working there's too many of us doing it.
These quotations illustrate participants' motivation to find jobs and their active search for employment; however, both participants emphasize the struggle to find employment opportunities given their criminal record, even following successful completion of a sentencing term. Many participants expressed similar sentiments and reported that their inability to find a job forced them to participate in the informal economy within their neighborhoods. These jobs, while providing participants with some money to take care of their needs, were often irregular and seasonal, did not offer employee benefits (such as health insurance) and were sometimes illegal (e.g., selling drugs), which was both detrimental to their health and well-being and increased the chance of re-incarceration. For example, one participant stated:
And I went back for selling the products that I used to smoke because I felt like it was easy money and just, like now I'd been out 6–7 months and I still hadn't found employment and I knew that selling crack was gonna make money cause I've been helping out every little chance I get ‘cause I can't find a job. Somebody need to move? I try to help ‘em move, you know handy work type stuff, that's about it.
This narrative suggests that inability to find a job forced this participant into the informal employment market and caused him to ponder whether he should begin selling drugs, as it promised to be provide a steady income stream. Other participants also reported cleaning, detailing and repairing cars, landscaping, construction, cleaning their neighbors' houses, and panhandling as viable options to make money after being incarcerated.
Discussion
Our findings corroborate results from other recent studies that investigate the impact of incarceration on health. Extensive scholarship has reviewed the impact of incarceration on access to services both pre-and-post release, risk behavior, and health outcomes. 38 –41 Those who are HIV positive are disparately represented in the prison and jail population, experience issues related to obtaining medication and linkage to medical services after release. 5,42 Relatedly, research has shown that individual vulnerabilities (e.g., substance abuse) can be exacerbated by structural issues such as lack of access and thus affect the reentry process of formerly incarcerated individuals. 43 The findings of the current study also demonstrate that structural impediments do affect individual behaviors, one's ability to successfully reintegrate after release, and health outcomes.
However, whereas previous research has demonstrated the ways in which incarceration can impact health and the re-entry process, little research has explored the prolonged impact of the incarceration experience on the health of HIV positive populations. In this article, we illustrate how incarceration and the post-release experience interact to affect HIV-positive populations. Our findings show that the effects of incarceration do not end after release. Due to stigma, social conditions that are worsened by incarceration, and the macro-level polices that manifest as lingering “side effects,” the health of HIV positive individuals is detrimentally affected. These findings support the conceptual model presented within this article by demonstrating the impact of incarceration on HIV-positive populations via lack of access to HIV-related medical attention, low quality of healthcare, continued stigma (both pre-and-post release), barriers to reintegration posed by restriction of rights, and worsened social conditions after release.
The results of the current study reveal the need for interventions to aid in post-release medical care linkage and to ease the transition back into the community. These interventions should: (1) begin while incarcerated and continue far after release to ensure full community reintegration and medical service linkage support; and (2) not be solely HIV related and, instead, address other social determinants of health that may compound the effect of incarceration on health. Possible interventions should include specifically providing help with: housing, employment, stigma-related concerns, substance use, and reestablishing social support after release.
A successful intervention designed to simultaneously address the many issues faced by HIV positive incarcerated and formerly incarcerated populations will also need to include cross-sector partnerships between criminal justice entities, public health personnel, and other social service agencies. Additionally, this study demonstrates that HIV-positive African Americans, and perhaps specifically those living in the Southern region of the US, often rely on religious entities and their faith to sustain them through difficult circumstances. For this reason, interventions designed to target these populations should include faith-based community organizations as key stakeholders and collaborators.
Correctional policies also often deleteriously affect incarcerated populations. Modification of policies related to obtaining HIV-related medications is needed. For example, HIV-related medications should always be available to incarcerated individuals and should be accessible immediately upon booking into a correctional facility. In prisons and jails, medication dispersion policies, such as “med-line”, threaten confidentiality for HIV positive inmates, thus making them vulnerable to stigma both on the part of facility staff and their incarcerated peers. Alternatives such as private dissemination of medications would mitigate this risk.
Finally, macro-level policies that prohibit access to certain employment opportunities and housing also disproportionately affect formerly incarcerated populations making them vulnerable to reincarceration and worsened health. As noted by participants in the current study, these policies create excessive stress and can lead to the use of negative coping mechanisms, HIV antiretroviral adherence lapses, a higher incidence of mental health issues, and can affect and exacerbate other social determinants of health.
Future research and limitations of the current study
The current study provides the foundation for future research to investigate the ways in which incarceration affects the health of HIV positive African American men. Quantitative research that is more generalizable and examines the association between incarceration and proximal predictors of health is needed to shed light on which health-related variables are most affected by incarceration and which components of the incarceration experience are most detrimental to an individual's health. Continued research should build on the framework revealed via the current study, as individual outcomes must be considered in relation to the broader social context in order to have a more complete understanding of the intersection of HIV and incarceration. However, some of the results may be informed by the setting in the American South. Further research is needed to understand if the issues are the same regardless of geographic location. For instance, a follow-up study may examine whether HIV-positive, incarcerated individuals in a rural area experience incarceration and post-release reintegration in the same way. Additionally, the current study only includes African American men. This is due to the fact that incarceration most disproportionately this population. However, a similar study conducted with women and other racial groups is needed to highlight the distinct experiences that others who have experienced incarceration may face.
Footnotes
Author Disclosure Statement
No competing financial interests exist.