
Abstract
Stigma is a barrier to HIV health seeking, but little is known about institutional and structural expressions of stigma in HIV testing. This study examines evidence of institutional and structural stigma in the HIV testing process. A qualitative, grounded theory study was conducted using secondary data from a 2011 HIV test site evaluation data in a Midwestern, moderate HIV incidence state. Expressions of structural and institutional stigma were found with over half of the testing sites and at three stages of the HIV testing visit. Examples of structural stigma included social geography, organization, and staff behavior at first encounter and reception, and staff behavior when experiencing the actual HIV test. Institutional stigma was socially expressed through staff behavior at entry/reception and when experiencing the HIV test. The emerging elements demonstrate the potential compounding of stigma experiences with deleterious effect. Study findings may inform future development of a theoretical framework. In practice, findings can guide organizations seeking to reduce HIV testing barriers, as they provide a window into how test seekers experience HIV test sites at first encounter, entry/reception, and at testing stages; and can identify how stigma might be intensified by structural and institutional expressions.
Introduction
S
Concepts of structural and institutional forms of discrimination help frame issues for greater clarity. For example, policies restricting access for a particular population are classified as structural stigma and discrimination, because they are rules for communities or organizations that hold positions of power in relation to another population. 7 –10 For HIV testing, such rules are likely acutely felt. Institutional discrimination is similar to structural, but is defined by intentionality: disparity is intended for particular populations, whereas structural discrimination creates disparity unintentionally. 8,9 To understand how stigma impacts HIV testing, we must identify and examine interactions between ‘macro’ level variables of structural discrimination and ‘micro’ level variables such as self-stigmatization. 4,10 –13 This is important because in the United States, 20% of the population with HIV does not yet know it, 10 and 40% who test positive do so late in the disease process. 11,12
Several studies document the relationship between individual and social expressions of stigma and HIV testing. 3,13 –15 What remains unclear is how testing sites reproduce stigma through means other than social; or perhaps through means in addition or in concert with social expressions. Examples might be social geography, organizational, and staff behaviors in the context of the power relationship. Social geography refers to social phenomena in space, 13 or how spaces create “the effects of being in place and out of place.” 14 This study identifies and examines structural and institutional expressions of stigma in HIV testing to help inform the development of frameworks to understand the phenomena.
Methods
This study is a grounded theory study using secondary data with the goal of identifying and understanding structural and institutional forms of stigma. 15 Data included 81 transcribed reports by ethnographer-informants who sought an HIV test at state funded testing sites in a Midwestern, moderate HIV incident state as part of a 2011 evaluation. 16,17 Twenty-two (22) HIV-negative men and women (“test visitors”), reflecting the demographic and experiential diversity of those at risk for HIV in this state, sought an HIV test at 33 testing sites between January and April 2011. This state had three publicly funded HIV testing venues: local health departments (42.4% of the test sites), community based organizations (39.4%), and community health centers (18.2%). Evaluation findings suggested, but did not explore, organizationally generated problems with HIV testing access: (1) confidentiality issues were reported by test visitors at 42% of the sites; (2) one in five (20%) test visitors were not able to receive an HIV test despite attempts to get one; and (3) 48.5% of test sites received a ‘no return’ rating, meaning that test visitors indicated that they would not return to those particular testing sites if they personally needed an HIV test in the future.
Test visitors reported their experiences via digital recorder within 30 min of the site visit in response to 5 open-ended questions. Transcripts included verbatim statements made by the ethnographer informants, and were de-identified for this study. QSR NVivo was used to manage data sortings and classifications. This study was reviewed and deemed exempt by the Indiana University Institutional Review Board.
Initial analysis procedures included independent, open coding by three researchers to characterize stigma from transcripts. Evidence included direct statements made by ethnographers themselves, as well as observation notes from researchers as they experienced the transcripts. These codes, their categories and differences were managed in conference, and differences were managed in conference. Repeated sortings were followed by axial coding using the central categories of stigma, otherness, structures, and power relationships. These categories were compared with a conceptual framework of stigma adapted from Deacon, 18 Corrigan and Watson, 19 and Herek (Fig. 1) for verification.
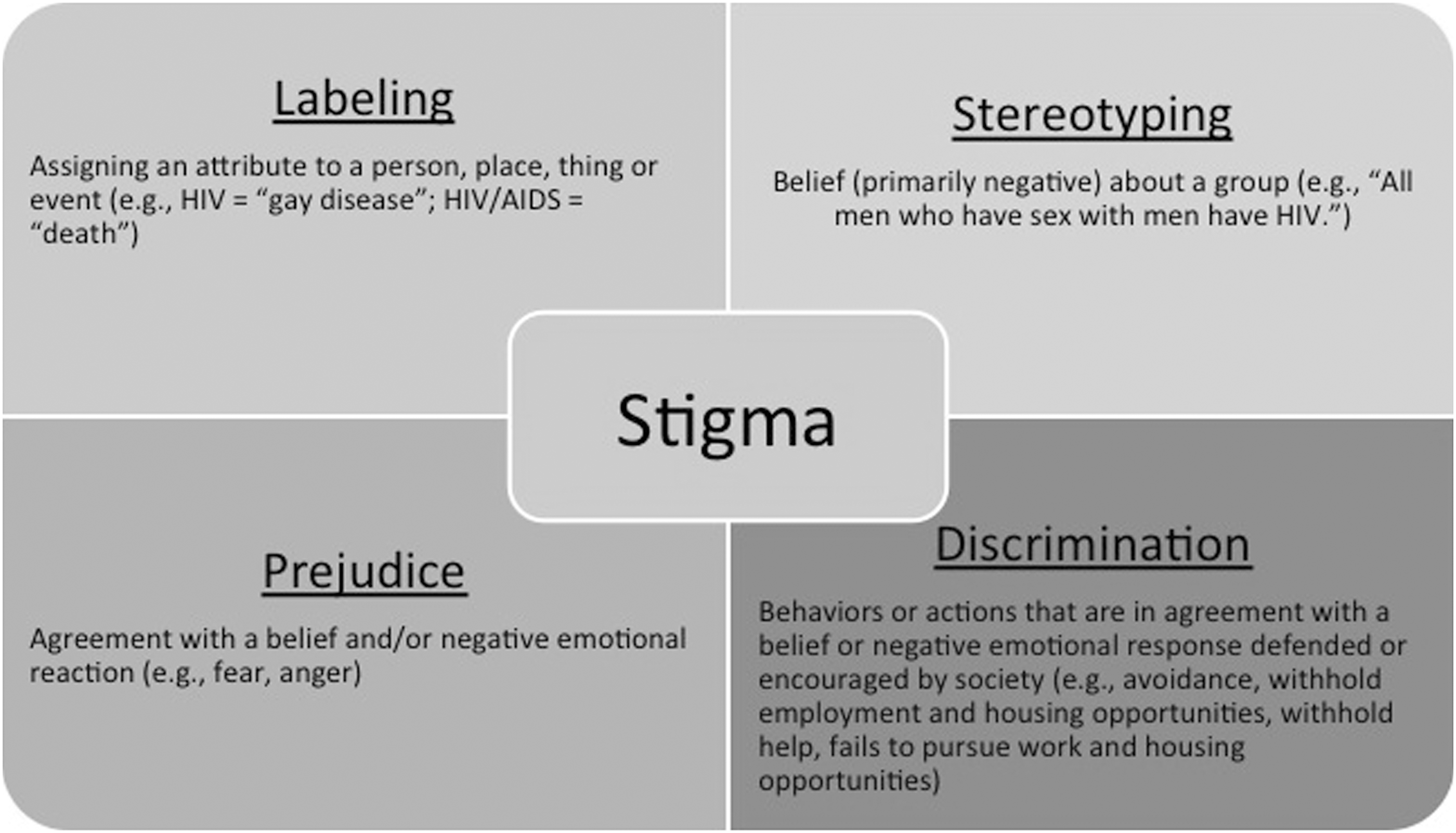
Conceptual framework elements of stigma.
Finally, researchers returned again to the data for selective coding. At this stage of the process, we asked questions of the data such as what evidence is there that stigma was not simply expressed socially? If not socially expressed, or if more than socially expressed, what was the precise nature and characteristics of the phenomena? What were the sources of the expression? What emerged included elements that contribute to a framework of institutional and structural stigma. Stigma experiences appeared to occur at three stages of the testing process: (1) initial phone or physical encounter of the testing site to inquire about or schedule testing (‘First encounter experiences’), (2) spatial and social encounters at entrance or reception (‘Entrance experiences’), and (3) encounters with the testing staff who provided testing services (‘Testing experiences’). Layering onto these experiences were elements of intentionality that then could be classified as structural or institutional expressions of stigma.
Results
Findings revealed elements of a framework showing that HIV testing organizations produced or reproduced stigma, discrimination, or marginalization at several points in the HIV testing process. Evidence of stigma was found with over half of the testing sites. The central phenomenon was stigma as expressed structurally and institutionally. Causal conditions appeared to be race/ethnicity, disclosure of unprotected sex or injection drug use, and gay male sexual orientation. Strategies to cope with the phenomena were limited, but did appear to be a decision not to test at a particular location in the future (which is also a consequence). While this was a consequence for these ethnographer-informants, a few expressed that an outcome might be more severe for someone who was testing “for real.” Such a person might likely never return for a test anywhere at anytime:
If I were in a real life situation I would have been so frustrated I would have said ‘Well to heck with it!’….They don't care and I don't have the nerve anymore.
Context involved spatial and physical aspects as well as virtual components, as will be discussed. Table 1 displays the elements and their classification as a ‘visual picture’ of the emerging framework. 20 Elements will be discussed by stage of testing experience.
First encounter experiences
First encounter experiences included phone contact mediated by organizational policy or functioning, as well as experiences of the test site's social geography. Experiences classified as organizational policy and functioning were produced by organizational decisions to function in ways that served organization ends. For example, some organizations depended upon volunteers. Others used phone automation.
Most organizations depended upon phone automation as the first contact option with the organization. Outgoing messages conveyed information about service availability and were accessed primarily through phone menus. Many test visitors reported being lost in a maze of phone menus as they tried to identify how to get an HIV test.
I called the number and was given a list of options….birth and death records, immunizations, the next listing was health education STD and car seats and that was all one option. Another one was division director and the next option was office manager, the next option was public health nurse, the next option was community clinic for medical care which was a totally separate phone number, and another option was volunteer coordinator. I called the community clinic for medical care and said that I was looking for an appointment for HIV testing. They said that I called the wrong place and I would need to call the (main health department). I asked for that phone number, but the woman on the line said she had no idea what that number was and did not offer to look it up for me or anything at all.
In many cases, callers were required to leave a voicemail message requesting an HIV test. In a few cases, calls were not returned. The following feelings resulting from these initial contact experiences included: (1) discomfort disclosing personal information with an HIV test request on an unknown voicemail, and (2) disappointment when such personalized calls were not returned. In cases where organizations did not return calls or were not available, test visitors assumed culpability: “Am I doing something wrong?”
The time is 1:30 p.m. I made my fifth call to (community agency). Again, no answer. I left my number on the answering machine.
At three sites, ethnographers experienced a barrier erected by staff for the purpose of the organization. One organization required the test visitor to commit to bring her own Spanish translator to the testing appointment order to get an appointment.
When I called, I asked if somebody speaks Spanish and they told me no…I told him that I was making an appointment for a friend who speaks a little English. He told me that she needed an interpreter in order to go there. I told him okay, just I wanted to make an appointment for her; but he told me “No, just first make sure that she can come with an interpreter.”
Staff at two other organizations engaged the test visitor in a needs assessment conversation to assure that they were eligible for testing based on clinic policy. One test visitor, put off by the personal questions over the phone about sexual practices, expressed desire not to talk on the phone about such personal matters. The staff response was to classify the test visitor as ‘low risk’ and therefore ineligible for HIV testing. This particular experience is one example of the 20% failed HIV test attempts from the 2011 test site evaluation.
Finally, “first encounter” experiences included socio-physical aspects of the testing site, which included the hidden nature of the HIV testing program in a large building complex, and social constructions of the space itself (governmental, church, judicial). Ethnographer informants responded in a way that was similar to the absence of HIV information in automated systems.
It took me forever to find the building because it's like a weird government complex…I was supposed to ask for this guy (name) and his office was naturally in the boonies of the building, so I couldn't find it. I went into like the child's health clinic place and they were like, “You're in the wrong place.” But it was just weird, because it took forever to find his office and when I did find his office, it looked like - - I don't know what this building used to be like a dorm room or something…. (the tester) looked like the health inspector or something, but the sign for the clinic, which is just his office, is not conspicuously displayed.
Entry/reception experiences
Entry experiences included physical and social experiences reported as sites were encountered. Some sites were reported as overly “government,” while others were notable because they were courtrooms, gay, or WIC (Women Infants and Children, food and nutrition program) identified spaces. These socio-physical experiences were closely related to first encounter experiences of social geography, though notably separate for test visitors, as they experienced them separately or in seriatim.
The office itself is strangely situated in the courthouse. It is not exactly the most friendly or comforting place. It is very open because they share the seating arrangement with the courthouse and that was just kind of weird.
Test visitors reported feelings of difference or ‘otherness’ when encountering testing environments that did not clearly speak to HIV. The absence of HIV at entry/reception was at times the third such absence reported in one testing experience by visitors.
The only thing I didn't like about it was that the office was shared with WIC….women and children were there, and I'm coming to get an HIV test so it feels awkward. There were a million (reception) windows labeled for WIC but I didn't know which window to go to for the HIV testing, so I was looking around like um, who do I talk to first?
The act of requesting an HIV test in environments that did not speak to HIV made test visitors feel uncomfortable. Health departments visited tended to orient toward moms and babies with WIC and immunization messages. In this example, the physical and the social aspects of the experience collided for the tester:
When I came to the receptionist at (health department) I told her I had an appointment with (name) who does the HIV testing. And she asked me what the appointment was for, and in front of a group of people I had to say HIV testing. She was prodding me to answer the questions so I had to just say it. It was kind of embarrassing and I didn't feel comfortable with that….I was waiting in the waiting room for probably about 15 to 20 minutes. There was Sesame Street on the TV, it was a crowded room and I think the people who heard what I was there for were kind of giving me strange looks.
Unlike the above example, other stigmatizing social interactions with staff appeared more intentional and occurred primarily at reception. In one case, a tonal change in the interaction occurred once it was known that an HIV test was needed.
As soon as I said who I was there to meet, the tone did change a little bit at the reception desk. It was much more formal and reserved, as if they didn't wish to—I couldn't tell if they didn't wish to invade my space, if they were trying to maintain obvious confidentiality, or if they were afraid or just what it was. But the woman and children that they were interacting with before me, it was much more happy, jovial atmosphere and then when I walked up to the window, it was rather jovial still, but immediately when I said the name of the person that I was there to meet, the atmosphere changed remarkably. It was never rude, but the atmosphere did change.
There were other examples of stigmatization by reception staff in the context of power. Here, in front of a group of people in the waiting room, reception staff breached tester confidentiality. This behavior appeared to be in response to expressed test visitor concerns about access barriers at the first encounter stage. The test visitor believed that the receptionist was trying to get rid of her.
I wanted to inquire about getting an HIV test. At that point I was told I must be a patient. I said, ‘well online you're listed as a free HIV test site for anyone,’ and she said ‘well we don't do it here unless you're a patient or referred from a physician.’ So I said, ‘well okay, I wouldn't have come in but (I was lost in) the phone system.’ And at that point I felt like - - she gave me the impression that I was a bother, that I was wasting her time and her response to the phone issue was that I must have been doing something wrong. She looked at me, rolled her eyes, and said, “Well we don't do HIV testing here for anyone.” At that point when she said that, she said it a little loud, and as I looked around the waiting room, several people looked up which obviously made me feel very uncomfortable.
Reception was also where test visitors encountered mismanagement of appointments and test supplies. Ethnographers experiencing this reported that the mix-ups appeared to be unintentional, though the organizational response was socially expressed, and in two cases perceived as intentional. In one example, the test visitor waited for a scheduled test appointment and when he was called up for the test, he was told that he would have to come back for testing on another day because the site “just ran out of tests.”
I am sitting there (in waiting room) maybe ten minutes and one of the ladies comes out and they tell me, “We are going to have to reschedule an appointment for you because we ran out of test strips and we can't do your test today…. you just call back and we will let you know if we get any test strips in and when you can come back in.” Seeing how they only test on Wednesdays, they don't test any other day, and for them not to have a test today that I have got to wait or come back in like another week and they don't know when they are getting in, I was a little aggravated. I was more than aggravated. I was pissed…. I could only imagine what this would have been like if it was for real. Quite frankly, I don't think I would have come back. They treated it matter-of-factly and there was no “I am sorry.”
Testing experiences
The final stage was ‘testing experiences;’ the point at which the test visitor received counseling and testing. Overall, test visitors reported that positive experiences with the testing staff mitigated any negative effects of initial organizational contact and reception. However, when stigma was experienced at this stage, it appeared to be both institutional as well as structural. Reported experiences of stigma and discrimination involved judgment of behaviors and breaches and confidentiality. Judgment was socially expressed in response to disclosures about sexual practice, condom use, and IV drug use.
I was treated like - - kind of like a junky really. I wasn't treated the nicest. (Tester) was very articulate but he was not the nicest person I've come across. In fact, if I hadn't admitted to using IV drugs then he might have treated me different.
I was valued in some way, but I was also treated with some stigma because I haven't use protected sex. I haven't used protection in sex and I think I was kind of looked down upon for that.
Test visitors reported violations of confidentiality that appeared to be grounded in some form of organizational functioning. Much like the requirement to leave personal information and a test request on a voicemail, clinical practice appeared to allow for service interruptions by other staff members or the presence of others without introduction.
(T)hen a woman just came in. (Tester) didn't really shut the door or anything, which is kind of unnerving…and then they started having a conversation about this piece of paper that she had….but that was just weird because they were having a conversation in front of me.
I was a little put offish because it wasn't just him in the office. There was another person in there with him, and she was kind of helping him writing stuff down and everything that I didn't quite understand. If this was supposed to be something that's actually private, even if he was training her, he could have said that and asked whether or not it was okay for her to stay. But he didn't, she was just there.
In three situations, confidentiality appeared to be compromised to “save time” for the staff member or the organization. In two cases, samples were taken from more than one patient simultaneously. The counseling was separate, but the sampling was not; therefore compromising patient confidentiality for everyone testing. To complicate matters, in all cases, test visitors believed that staff presumed they were there with another patient, “because we were both Black, in the waiting room and wanting an HIV test.”
The front office people didn't really know what to do. They brought a paper out for this other person and they just assumed that we both were together, I guess. But we didn't say we were together or anything…. We weren't sitting together but they still assumed that we were together. (The tester) came back out and called the guy to go back there and I sat there and he said ‘you come too.’ Okay, so I got up and went on back there and while we were walking back he said “We'll do both the tests at just about at the same time - - and I can get back (to) the office.” He said “I'll ask the questions separately. You'll sit - - one of you - - then I'll ask him the questions first while you sit out in front, in the outside. And then I'll call you in and we'll - - I'll ask you questions.”
Discussion
This study provides evidence and additional clarity about institutional and structural expressions of discrimination in HIV testing. The emerging framework elements exist at the nexus of spatial and social encounters with a single HIV testing site. Power relationships that favored the testing organization and staff imbued social expressions and therefore extend beyond the mere social. Experiences of stigma were compounded by their potential multiplicity across stages in the same test visit. Several test visiting experiences held more than one form of stigma expressed at more than one stage.
The mix of social and spatial expressions of structural discrimination (unintentional) included organizational policy mandating phone automation as the first contact with the organization, as well as the visible absence of HIV in a sea of WIC reception windows. Notably, institutional discrimination (intentional) was primarily socially produced through staff behavior. The combination of power relationships and intentionality calls forth what Paul Farmer termed the “materiality of the social;” depicting the relationships of power and violence. 21 The neglect of phone messages, apathy about access issues, use of power to stigmatize at reception, or breach of confidentiality comprised the many and nuanced forms of this expression.
Whether intentional or unintentional, structural and institutional expressions of discrimination had a deleterious effect on the experience of HIV testing. Here is where the interaction between structural expressions or ‘macro’ level discrimination and individual or ‘micro’ level anticipated or experienced stigma meet. Reported outcomes had personal and health implications. On the personal level, ethnographers expressed feelings of otherness, shame, or culpability for the problems of access. On the health level, ethnographers reported future intent to preserve themselves by refusing to return for future HIV testing at particular testing sites. This diminishment of access, though self-preserving, has important health implications. The measured outcome of 20% test failure rate from this 2011 evaluation is certainly sufficient to warrant system review with attention to the potential contribution of institutional and structural expressions of stigma.
These issues are not reserved for publicly funded HIV testing sites, because they are likely experienced in other clinical settings. The implementation of routine HIV testing in clinical settings is not fully realized across the country, and as such, patients continue to carry the burden of requesting a test or waiting for symptoms. Clinical organizations will likely struggle with the aspects of structural discrimination produced and reproduced in organizational operations, particularly given that such expressions serve organizational ends and are not intentional, despite potential impact on patients. These challenges notwithstanding, communities and organizations seeking to reduce the impact of stigma on HIV testing should examine experiences of test seeking with focus on individual, social, structural, and institutional aspects. Further research is needed to deepen the emerging framework of structural and institutional stigma.
Footnotes
Acknowledgments
This study was funded by the Indiana Minority Health Initiative. The authors would like to thank the Indiana Minority Health Coalition for guidance and partnership.
Author Disclosure Statement
No competing financial interests exist.