
Abstract
African-born immigrants and refugees have HIV infection rates six times higher than any other minority groups in the United States. Despite the increase in the population size and diversity of Somali immigrants and refugees in the United States, Somalis are one of the medically underserved population subgroups in this region. The lack of aggregate HIV infection rates among African-born immigrants, for example, Somali refugees, is a cause for alarm and calls for more research to be conducted in this subgroup. The purpose of this article was to examine contextually relevant HIV prevention strategies that will enhance HIV prevention among Somali immigrant/refugee young adults in the United States. Using the grounded theory approach, a convenience sample of 27 immigrant/refugee young adults was recruited in central Ohio. Recommendations for potential HIV prevention strategies emerged under two main categories: (1) internal community resources and (2) external platforms. Study findings support a collaborative approach involving community leaders (parents, elders, religious leaders) and educational (schools), media, and healthcare settings to tailor HIV prevention strategies that meet the needs of the priority group.
Introduction
G
With regard to HIV transmission rates among immigrants and refugees, those of African descent have HIV transmission rates six times higher than any other minority groups in the United States. 6 –8 However, such immigrants face extensive HIV testing barriers, which can drastically affect efforts for enhancing HIV prevention. 7 In addition, aggregate HIV transmission rates for the various African-born immigrants and refugees in the United States are lacking because they are often included in the larger African American ethnic group. 6 There were 263,662 refugees residing in the United States and 16.7 million refugees globally in 2013, with an estimated 50% under the age of 18 years. 9 The lack of aggregate HIV transmission rates among African-born immigrants is a cause for alarm and calls for more research to be conducted in this subgroup, given that (1) they tend to reside in urban areas that have high prevalence of HIV transmission and (2) are not homogenous, but represent a plethora of other African subgroups in the United States. 6
Somali refugees and immigrants are a growing population in the United States. According to the Office of Refugee Resettlement, 10 in 2014, there were 9011 refugee arrivals from Somalia. Recent estimates for the state of Ohio show that 45,000 Somalis live in the city of Columbus, placing Ohio in the second position among states with largest Somali communities in the country after Minnesota. 10
Despite the increase in the population size and diversity of Somali immigrants and refugees in the United States, Somalis are one of the medically underserved population subgroups in this region. 11 Studies on immigrant health in the United States have primarily focused on larger immigrant populations from Europe, South America, and Asia, which created a gap in knowledge about health of immigrants from Africa. 11 The lack of adequate published evidence concerning health challenges faced by the various subgroups among African immigrants and refugees, for example, Somalis, creates gaps in designing, framing, and implementing targeted interventions. 11
Effective contextually relevant HIV prevention strategies targeting Somali young adult immigrants and refugees should be developed with nuance, given the unique circumstances in the priority population. First, there are challenges associated with reliable HIV/AIDS data in Somalia due to political instability and relocation of their citizens. 12,13 According to UNAIDS, 14 HIV prevalence in Somalia was <1% while the ratio of HIV burden between men and women was 49% and 51%, respectively. With regard to HIV infection, only 4.3% female and 5.4% male youth and young adults (15–24 years) had adequate HIV knowledge. 14 Second, there are almost no studies in the United States that have examined HIV/AIDS in the priority community, despite the fact that African refugees and immigrants tend to reside in high HIV prevalence urban areas. 6
To that end, the design and implementation of HIV prevention strategies and interventions among the Somali youth should involve exploration of their beliefs and attitudes toward HIV prevention, overall sexual health education, and their preferred information delivery modality. Evidence supports that Somali refugees have different unmet healthcare needs largely due to the cultural and socioeconomic barriers that result from resettlement. 15 –17 In addition to cultural norms, Somali women face other healthcare access barriers, including language barriers, stigma from past unpleasant care experiences, or fear for repeated traumatization for those exposed to trauma. 17 Despite the low HIV infection rates in Somalia, given that African refugees tend to reside in high HIV prevalence urban areas in the United States and there are about 50% of youth and young adults in the United States without knowledge of their HIV status, 3,6 there is a need to develop culturally sound HIV prevention interventions in the priority community.
While research that focuses on HIV prevention strategies for Somali young adults in the United States is scarce, there are a few examples of interventions, which have used different approaches for health promotion. A pilot study 18 that used videos to educate and sensitize Somali refugee women in Minnesota on the importance of prenatal health services was successful because it involved community leaders and aired on a local cable Somali channel. The program addressed gaps associated with the increase in pregnancy complications among Somali women and poor attendance in prenatal care classes, despite availability of interpreters and their own competence with English. 18 The study revealed the need for a contextually appropriate intervention because Somali women participants reported apprehension toward prescribed obstetric procedures, cultural preferences, and the fact that obstetric practitioners were not familiar with Somali customs, including female circumcision. 18
A different health intervention 19 that targeted the Somali Bantu refugee community in Buffalo, NY, found a need for health information that was tailored to refugee women and children in poverty. The Somali Bantu community should not be confused with the general Somali community because they have distinct cultural traits. 19 For cultural sensitivity, this intervention involved home visits using trained community health workers who could speak the Somali Bantu language. Authors aimed to create awareness of the presence of the Somali Bantu community among health professionals as well as health knowledge gaps. Barriers identified included language, female-headed households, food safety, household cleaning, and financial literacy. Such findings support the heterogeneity among refugees and immigrants, even those who hail from the same country.
To that end, potential sustainable interventions need to tailor HIV prevention strategies to meet the contextual needs of Somali immigrant and refugee young adults. Given the gaps in reliable data on HIV transmissions in the priority group and the lack of disaggregated data on subgroups of African immigrants and refugees, the purpose of this article was to examine contextually relevant HIV prevention strategies that could enhance HIV prevention among Somali immigrant/refugee young adults in the United States.
Methods
Study design and recruitment
The grounded theory approach 20 informed the design of this exploratory qualitative study. Ohio University Institutional Review Board approved the study protocol. Using snowball sampling 21 and fliers posted at community centers, a convenience sample of 27 immigrant/refugee young adults was recruited in central Ohio. Eligible participants were 18–25 years old, spoke English or Somali, were residing in central Ohio at the time of the study, and were of Somali origin.
Before collecting data, a semistructured interview was developed and contained open-ended questions and probes. It was translated from English to Somali and translated back for accuracy purposes. Interview items examined sexual health and HIV knowledge (e.g., what do you know about HIV or AIDS, what societal or contextual factors are putting people at risk of HIV in your community); preventive utility of condoms [e.g., do you think condoms: prevent all sexually transmitted infections (STIs), are effective depending on how you use them, don't prevent anything]; preference for receiving sexual health knowledge (e.g., do you think there is a way you can receive this information in a manner that is not stressful or culturally inappropriate for your parents); barriers in accessing sexual health knowledge (e.g., describe barriers to getting knowledge regarding sexual health that you have personally experienced, how can these barriers be overcome); advice to other young adults (e.g., if you were going to warn youth in your community about not contracting HIV/AIDS and other STIs, what would you tell them?); and suggestions on individuals who would be involved in HIV prevention and pregnancy concerns (e.g., who would you consider to be the most important actors in the effective prevention of HIV/AIDS, STIs, and pregnancy).
Data collection
Two 24- to 25-year-old graduate students of Somali origin, gender matched and bilingual/bicultural, served as research assistants. Eligible participants were interviewed using English or Somali language at a private location of their choice after signing informed consent forms. Majority of the participants consented to being audio-recorded. For those who declined, their responses were recorded on paper.
Data analyses
All audio-recorded interviews were translated verbatim and transcribed by the two research assistants. All transcripts recorded on paper were reviewed for coherence and accuracy. Twenty-seven participants were deemed sufficient for the study after reaching data saturation. 20 A modified grounded theory approach was utilized to analyze data using the following steps: first, the four-member research team consisting of two research assistants and two investigators conducted open coding, whereby they read through the transcripts while labeling and tagging themes, impressions, or ideas. The team then reviewed each code from each interview and grouped them into broader themes/categories using axial coding. Finally, further selective coding that involved the review and integration of codes was undertaken and incorporated into a master codebook until sufficiency. 22 To ensure reliability, the team maintained an audit trail. 23
Results
Participant characteristics
A total of 27 immigrant Somali youth participated in this study. The gender ratio of participants was almost equal with 13 male and 14 female participants. Ages ranged between 18 and 25 years. Forty-one percent (n = 11) of the participants relocated to the United States at ages 0–5 years old, while 59% (n = 16) of participants were born in Somalia.
Factors that promote effective interventions
Analyses identified various factors that would be essential in raising awareness about HIV prevention in the priority community. Those factors were then utilized to develop recommendations for potential HIV prevention strategies. Two main categories emerged in this regard: (1) internal community resources and (2) external platforms. Subcategories were then developed for each of the two main broad categories, based on interview data (Fig. 1).
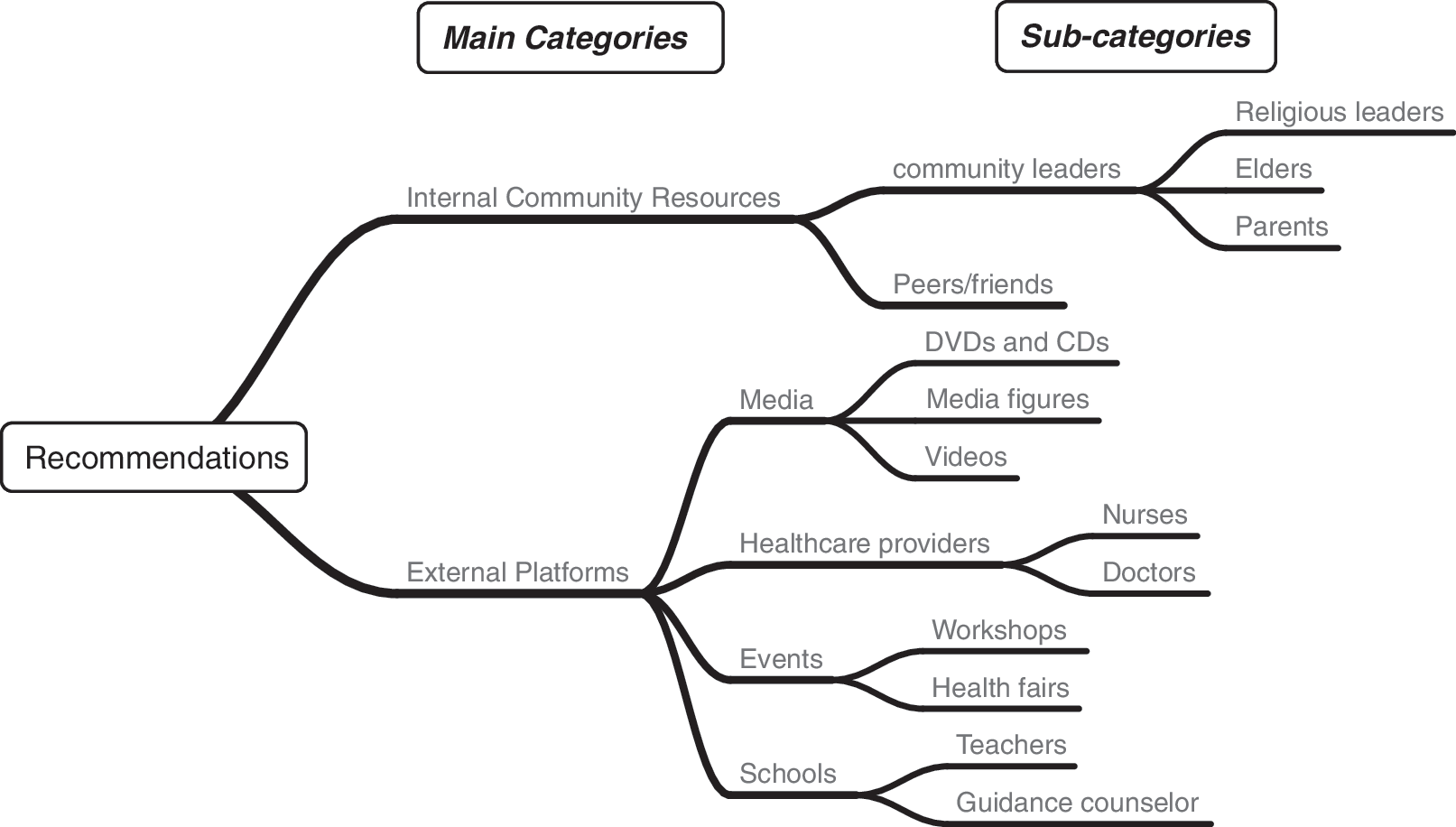
Thematic map.
Internal community resources
Use of internal community resources such as community leaders and peers/friends was considered critical in enhancing community buy-in for HIV prevention strategies.
With regard to community leaders (e.g., religious leaders, family/parents, and elders), they were deemed important to strategies for HIV prevention because they are key stakeholders in the Somali community. In addition, given that sex and HIV transmission were taboo topics in the community, many participants suggested that community leaders would help reduce stigma and communicate with young people, if educated and engaged in open and informed discussions about HIV transmission.
They can learn about it, teach their kids and their neighbors … education is what makes a difference and we, the community, have to research this for the parents that are afraid to ask those questions. That are afraid to go to the health fairs where they have those information. We need to find a more confidential way for them to get those information if they are embarrassed by it. (Female participant)
With regard to religious leaders, they were considered vital in the community because of their role as advisors, teachers, and religious scholars. Participants acknowledged that parents would be open to their children learning about HIV prevention at the Mosque (place of worship) under the supervision of religious leaders, “through the mosque … everything that my parents learn through religion is vital and so if I learned through Islam and through religious scholars, it would be okay for them” (Female participant). Religious leaders would provide a culturally acceptable setting for young people to learn about HIV prevention without parents being concerned about the appropriateness of information provided.
Parents and family were also identified as important resources for the prevention of HIV transmission, as long as communication was clear and initiated by parents. On the impact of having a sexual health conversation with parents, a participant explained “I would have reacted to it differently if I had heard it from my parents. Because everything in school was you get sexually transmitted diseases but from my parents, I think they would have explained it a bit better” (Female participant). Some participants found the home setting ideal for HIV prevention awareness as opposed to the school setting.
In a related vein, participants supported utilizing the Mosque as a venue for an HIV intervention because it would provide an opportunity for parents and family members to participate alongside their children.
I guess maybe a lot of the big issues can be broached at the mosque where parents might be going to … that's the place where an entire family might congregate. Having discussions that are more open. There have been some but it needs to be more direct and more out there. (Female participant)
Given that Mosques are contextually appropriate in the Somali community, they would be ideal to develop and implement an HIV prevention program in partnership with religious leaders and parents.
Community elders were also considered vital in enhancing HIV prevention among Somali refugee/immigrant young adults. They were deemed influential across all age groups, genders, and generations, given their leadership role in addressing challenges in the Somali community.
When Somali elders are given anything through Islamic lessons, they take it very seriously and it becomes more a lesson, more formal. They respect it more. I remember there was a time when a man was talking going through the same thing with sexual health, with elder women. He was discussing a spiritual bath and mentioned ‘for the elder women that have saggy breasts, they have to make sure they lift their breasts and wash underneath,’ some laughed and some took it very seriously. (Female participant)
Community elders would be ideal to communicate HIV information in a manner and language that resonates with the priority community.
With regard to peers and friends, some participants acknowledged that they preferred discussing HIV prevention and other sexual health issues with them. Such preference was due to the fact that community members were not available or willing to openly discuss such topics due to societal norms, “yes, through friends. You guys can talk about it with each other without it being inappropriate” (Female participant). HIV prevention information among peers was considered contextually appropriate, although the accuracy of information shared among them was not considered.
External platforms
Schools were identified as an ideal setting to learn about HIV prevention because teachers were available and familiar in a setting that students had a lot in common with each other, “you can receive this information in a classroom because its not stressful and everyone in the classroom is on the same page as you” (Male participant).
Moreover, schools were considered a good resource to obtain sexual health information, given that the topic is taboo and not often discussed in the larger community or family setting.
I prefer in class, in school not from my parents. It's awkward from my parents and they wouldn't want to tell you about it. They would say be safe because they expect you to be safe but you aren't supposed to be doing those things. (Female participant)]
Participants also reported that schools were ideal because young people spent most of their time there. They were, therefore, in a position to engage their teachers by asking questions that would otherwise be frowned upon in their cultural settings.
Most children a lot of time in schools that is where they actually learn and they feel more comfortable in talking to their teachers about it. The teachers ask questions and they engage one on one with the students. That is more convenient for the student to feel comfortable in a classroom. (Male participant)
Within the school setting, participants also noted that a guidance counselor would play an integral role in enhancing HIV prevention strategies in the priority community. This was ideal, particularly for participants who were uncomfortable with receiving sex-related information in a classroom. Such participants preferred the privacy of a guidance counselor's office.
I think guidance counselors could have an affect on that age group. I think there's a lot of laughter. It needs to be something that is continually stressed. Culturally, Somalis shouldn't be treated differently when it comes to sexual health because the information is presented differently and the fact that its kept secret. In different communities at young age there's a lot secret sex going on but no one talks about it. If we are going to cater to the Somali community I think we need to have people informed that they can have sex secretly, but they need to know the dangers of it.
Suggestion to utilize services of a guidance counselor provides perspective for a one-on-one relationship with a given student who would otherwise find it challenging to engage in a sexual health topic, such as HIV transmission, in public. This suggestion highlights the prevailing stigma associated with open discussion of HIV transmission due to societal norms.
In addition to schools, healthcare providers, such as nurses and doctors, were reported to be instrumental in providing information and life skills for HIV prevention. For example, a female participant reported that due to the fact that her mother was a nurse, she was able to discuss with her various things related to sex, HIV transmission, and female circumcision.
My mother is a nurse, like myself, and we had a comfortable conversation about intercourse and circumcision about two years ago. One of her patients had to have a vaginal reconstruction due to a botched circumcision. She explained to me how the patient struggled with intercourse, childbirth and urinating. We discussed various things regarding sex and I even talked to her about my HIV/AIDS class in college. (Female participant)
A Somali parent who is a healthcare provider would help bridge the gap in access to HIV prevention knowledge and life skills.
Other participants underscored the important role that doctors played in the prevention of HIV transmission. In particular, doctors were well respected by Somali parents, which would be vital in creating awareness about HIV prevention among young people.
Yes, through doctors. Most Somali parents they listen more to their doctors so I would say that is something the doctors have to do. They have to talk to the parents, ask for it or not. Hopefully, the kids they can hear about it…I would put the stress on pediatricians. Talk to the kids and talk to the parents with the kids. (Female participant)
Doctors would be able to provide critical information pertaining to sexual health and HIV prevention in their offices during scheduled appointments. However, how much information and ability to answer questions would depend on the doctor's ability to spend more than the regular 5 min allocated to patients.
Other external platforms that were stressed by participants included community events such as workshops and health fairs. With regard to workshops, participants noted that they were ideal for, “raising awareness, holding workshops classes for the community learn more about” (Female participant). Participants recognized that raising HIV prevention awareness should not only be limited to young people but should also include the whole community. Such a perspective creates an ideal opportunity to address taboos associated with HIV transmission and sex.
In addition to workshops, health fairs were considered key in enhancing HIV prevention, “the sexual health information can be dispersed at the annual health fair” (Female participant). Health fairs tend to be larger than workshops and can target more people by utilizing different types of resources, for example, brochures that are translated into the local language, demonstrations, one-on-one with a healthcare provider, interpreters, tokens (e.g., condoms), and much more.
Participants also noted that more community events were needed to provide an opportunity for socialization that would serve as a platform to address misconceptions and taboos, with input from parents, religious leaders, and young people.
I mean, Somalis don't even discuss menstruation. You know? We need more community events that stress the importance of sexual health … where there is talk, socialization, and a discourse about fears, how to talk to young people, and how parents need to have more a comfortable zone where their children can feel like they can approach them with anything. (Female participant)
Another external platform deemed critical in enhancing HIV prevention was the use of media. One male participant volunteered to create a cartoon video that would have information on HIV transmission ideal for young Somalis, “I will just make a little cartoon video explaining on how HIV transmitted mostly through sex and I will give it to the Somali youth on their birthdays” (Male participant). Cartoon videos would resonate with the young Somalis, which would be ideal for their developmental stage. However, information in such videos would need to be reviewed by a health practitioner to ensure the content is age appropriate and accurate.
In fact, providing information to young Somali youth at a young age was a recommendation from some participants who felt that receiving information while young would prepare them to receive more information later on in life.
I think it would have been easier at a young age if they taught how to, or feel comfortable to talk about it. Not only, the diseases or the outcome you can get but at least if they were to educate us, it would be easy for us to receive more knowledge. It should come from the parents.
Once again, participants allude to the importance of having parents provide HIV education information to their children.
In addition to videos, participants noted that CDs and DVDs would be ideal media outlets for providing HIV prevention information and life skills for both parents and children, “they can create CDs and DVDs to explain sexual health and inform the parents. The youth will benefit from the CD and DVDs” (Male participant). Use of CDs and DVDs is a good idea, and instead of reinventing the wheel, those that are validated from the Centers for Disease Control and Prevention can be adapted to meet the contextual needs of the Somali young adults.
Apart from DVDs and videos, other participants alluded to the use of media figures to create awareness about HIV prevention in the priority community, “… a lot of kids listen to K'Naan. He is one of them … and all the other singers, I have no idea who they are but K'Naan would be one of them; media figures” (Female participant). Participants acknowledged that there were celebrities of Somali origin who had made an impression on young Somalis and could be effective in enhancing HIV prevention.
Discussion
Findings from this exploratory study revealed recommendations for various contextually relevant HIV prevention strategies that can be implemented among Somali immigrant and refugee young adults in the United States. Recommendations revolved around two major categories: (1) internal community resources and (2) external platforms. While HIV/AIDS among immigrants is well documented, this is the first study that has used disaggregated data to examine contextually appropriate HIV prevention strategies among Somali young adults in Ohio. Despite low HIV transmission rates in Somalia, HIV prevention is still relevant due to the fact that the priority community resides in urban areas that have high HIV transmission rates, almost 50% of young people are unaware of their HIV serostatus and there are limited studies examining HIV prevention as well as sexual health in the priority community in the United States.
Furthermore, Somali parents and children born in the United States or immigrated when they were young are likely to undergo acculturation at a varying pace. Often, children are able to adapt to the prevailing culture at a faster pace than their parents. This may present communication problems between the parent and young Somalis, leading them to seek out information elsewhere (e.g., Internet or peers) that may be inaccurate and lead to negative outcomes. 24 To that end, future studies may examine the impact of acculturation on HIV risk among Somali refugee/immigrant young adults, especially because most of them are born in the United States or immigrated at a young age and could have adopted host country's culture that may place them at an increased risk of HIV transmission.
Internal community resources
For potential HIV prevention strategies to be effective, participants emphasized the importance of involving community leaders such as religious leaders, elders, and parents/family members. Given that the priority community's norms are largely driven by culture and tradition, any type of intervention to address HIV transmission vis-à-vis sexual health needs to be a collaborative endeavor with community leaders to ensure buy-in and ownership. Such collaboration will provide an opportunity for community leaders to be educated and trained on the benefits of HIV prevention vis-à-vis sexual health education and life skills to mobilize the community to raise awareness and address prevailing taboos and stigma.
While the involvement of aforementioned community leaders in HIV prevention strategies is a documented successful strategy, 24 –26 Smerecnik et al. 26 found that some study participants questioned their religious leader's expertise, authority, and interpretation of the Qur'an's teachings on sexuality because his perspective contradicted their own in relation to the conservative nation of Islam. To that end, it is imperative that before implementing any intervention in the priority community that community readiness is assessed.
To assess community readiness for an HIV prevention intervention, Aboud et al. 27 adopted the community readiness stages model to examine the extent to which community leaders in Bangladesh were prepared to facilitate HIV prevention strategies. Aboud et al. 27 reported that most of the community leaders advocated for enhancing HIV prevention awareness and social norms advocating for morality. This model can be adopted in the Somali community to engage community leaders before developing any HIV prevention strategies.
In addition to religious leaders, involvement of parents/family in HIV prevention vis-à-vis sexual health is well documented. 28,29 In the current study, some participants preferred receiving HIV prevention information and life skills from their parents. Relevant to the current study, Prado and Pantin 29 found that the family-based—Familias Unidas—intervention targeting Hispanic youth was effective in improving family function and reducing unsafe sexual behavior. It focuses on enhancing positive parenting, parental involvement, parent–child communication, and adolescent family support, to reduce risk of irresponsible sexual behavior and drug use. Such an intervention can be adopted in the priority community to reach out to Somali parents and young adults to address HIV prevention.
External outlets and platforms
With regard to external outlets and platforms, participants identified the following mediums—healthcare providers, schools, media, and events—as ideal for enhancing HIV prevention among Somali young adults in Ohio.
Majority of respondents identified the school setting as the most adequate place to receive sexual education because it is a familiar setting and teachers were in a position to openly discuss topics that are considered a taboo in most households. Such a strategy would help curtail HIV stigma as well. Given that schools are already offering basic sexual health education, the challenge has been having parents allow their children to participate in such courses, given that there is an option for parents to opt their children out. To that end, a community participatory approach that brings together parents, teachers, and young adults from the priority community would be ideal in meeting contextual [cultural] needs. In a study 24 conducted among Latino youth, a culturally appropriate intervention—Familias:Preparando a la Nueva Generación—was developed using a community-based participatory research approach to reduce alcohol and drug use among Latino youth by enhancing parent education using existing and validated curricula that have previously been used among Latino youth. 24
The Familias:Preparando a la Nueva Generación intervention was developed upon request of teachers and parents for the purpose of improving parenting practices by enhancing parent–child relationship, parent-to-parent support, and infusing cultural norms. It was informed by the ecodevelopment approach and offered at a school attended by youth from the community. 24 The intervention was tested for efficacy and found to be effective in promoting positive behavior because it was tailored to the contextual environment of parents, teachers, and children. 30 It reinforced the importance of developing bicultural interventions that are implemented by bicultural/bilingual practitioners targeting immigrant communities. 24 Future studies can examine the feasibility of adopting and tailoring such an intervention to meet the needs of the priority community from an ecodevelopmental approach.
With regard to healthcare providers, participants highlighted the importance of involving nurses and doctors because of their profession and were highly regarded by Somali parents. While not all doctors would be available to provide HIV prevention information and other sexual health services, a novel intervention called Project Connect Health Systems Intervention (Project Connect) can be implemented in the priority community. 31 Project Connect is lauded for providing referral information on local healthcare providers who provide sexual and reproductive healthcare services; it has been utilized by nurses to link adolescents with relevant services. 31
In addition to the aforementioned outlets/platforms, participants also emphasized the need to hold community events such as workshops and health fairs. Participants acknowledged that such events would be able to provide various resources that would enhance HIV prevention awareness information and behaviors. With regard to workshops, participants deemed them essential in educating their parents so as to reduce stigma and taboo associated with sex-related topics such as HIV/AIDS. Culturally competent health professionals from health departments, universities, and refugee/immigrant community-based organizations can partner with the priority community and conduct workshops in collaboration with the Somali community-based organizations, community leaders, translators, and peer educators. Nevertheless, future studies should interview parents and other community leaders to better understand their salient perspectives regarding HIV transmission and sexual health in general, to determine the best approach to enhance HIV knowledge and preventive behaviors.
Another external platform reported by participants as key in enhancing HIV knowledge in the priority community was media (videos, media figures, and DVDs/CDs). In the advent of technological advancement and its utilization among young people, it is necessary to tailor such media strategies to better reach out to the young Somali refugees/immigrants. Media campaigns are well documented as effective strategies for addressing HIV prevention because they provide cues to action, such as HIV testing and condom use. 32 –34 HIV testing and condom use among immigrants and refugees are reportedly hampered by significant barriers 7,35 such as low HIV transmission risk perception, testing in health departments, which are not deemed confidential and anonymous, having already been tested as a requirement to immigrate to the United States, marginalization, and lack of health insurance, among others. To that end, novel strategies, such as use of media, to enhance HIV testing and overall HIV prevention among immigrant and refugee youth are warranted.
Yadav et al. 34 found that young participants in rural India were largely aware of HIV transmission through media. On the contrary, Gakahu 33 found that media containing various sexual graphics in advertisements and TV shows were likely to promote irresponsible sexual behavior in youth in Kenya. To that end, use of media to enhance HIV prevention among African-born immigrants such as Somali young adults should be addressed with nuance to tailor messages that are contextually acceptable. Future studies can pilot potential media campaigns with the involvement of the Somali young adults and community leaders to ensure cohesion and sustainability.
To contextualize media strategies to the Somali young adults, existing videos, CDs, and DVDs from the Centers for Disease Control and Prevention can be adopted and tailored instead of reinventing the wheel. Another option is to utilize mobile phone service platforms such as applications or text messages that can be tailored. Mobile telephony has in the recent past become popular as an HIV prevention strategy in the United States as well as internationally. 36,37 Juzang et al. 36 piloted a 12-week text messaging intervention targeting African American male youth. Each week they received three text messages. Findings revealed that messages helped increase monogamy as well as HIV transmission awareness. Such a strategy can be tailored and utilized in the priority community, particularly Somali young men, given that some male participants in the study anecdotally acknowledged that they were sexually active with young women from the African American and Latino communities. However, with text messaging, consideration for messaging charges has to be taken into consideration and an intervention has to determine how to reduce those rates or provide messages for free.
Limitation
Given that the sample for this study was drawn from one region, findings may not be generalizable to all Somali refugee/immigrant young adults residing in the United States. Also due to the fact that recruitment was predominantly done through referrals, some potential participants were not included in the sampling. There is also a likelihood that even though research assistants were in the same age group as participants, cultural norms could have influenced the responses provided due to fear of sharing private information. Nevertheless, the exploratory study findings provide an opportunity to inform the development of a pilot intervention in the current priority group in Ohio as well as larger studies in other locations where the Somali refugee/immigrant young adults reside.
In conclusion, study findings reveal a need to design culturally appropriate strategies in the priority community. Most importantly, potential strategies should be implemented in collaboration with community leaders to ensure buy in and overall sustainability. Such strategies should provide much needed HIV transmission education and life skills to young adults as well as the community leaders to minimize stigma and socially driven taboos, provide information on where to locate resources for prevention (e.g., condoms and HIV testing), and should be conducted in mosques and community centers where participants are comfortable receiving such information. In addition, media interventions utilizing mobile phone messages and media figures could be adopted in the priority community. Capacity building for such a strategy can be provided through partnerships with telecommunication companies, universities, and Somali community-based organizations that would assist with translating messages into Somali, training participants to retrieve messages, and waiving message retrieval charges or providing a discount. Overall, more research on HIV transmission, sexual health, and STIs in the priority community is needed to increase disaggregated data that minimize generalizing Somalis into “African” or “Black” refugee groups.
Footnotes
Acknowledgments
We would like to extend thanks to study participants, co-authors, and research assistants. Contents of the paper are solely the responsibility of the authors and do not necessarily represent any official view. Special thanks are extended to Hibo Noor, Nasro Jama, Roda Hassan, and Teena Stambaugh.
Author Disclosure Statement
No competing financial interests exist.