
Abstract
The study was designed to investigate the median duration of second antiretroviral regimens and factors associated with early discontinuation in HIV patients who switched with an undetectable viral load. We conducted a retrospective analysis of the Italian Cohort Naive Antiretrovirals Foundation Study (ICONA), which collects data throughout the country. Patients who started first antiretroviral therapy (ART) after January 1, 2008 in any center involved in this cohort and then switched to a second regimen were included in the study. Second ART failure was described as two HIV-RNA >200 copies/mL or the discontinuation of any drug. Statistical analysis was performed utilizing Kaplan–Meier curves and Cox regression model. The study population included 835 patients and the median duration of first ART regimens was 16 months with HIV-RNA undetectable for 13 months. The main causes of switch to second ART regimens were toxicity (42.5%) and simplification (37.5%). The switch mostly involved the third drug (63.5%) and almost one third of the population received a single-tablet regimen (STR) as second treatment (30.6%). The median duration of second ART regimens was 9.2 months and the probabilities of treatment discontinuation at 12, 24, and 36 months were 21%, 35%, and 48.2%, respectively. STR formulations had a protective effect against second ART discontinuation. Almost half of our population needed a third regimen within 3 years, but STR could improve second ART durability.
Introduction
C
The worldwide estimated percentage of patients on second ART regimens is about 4%, with the notable exception of Caribbean and South America, where it strikes at 21%. 10 Few studies have evaluated the effectiveness and durability of second ART regimens in settings other than low- and middle-income countries, where HIV-RNA load monitoring is usually not available and treatment failure is underdiagnosed. Obviously, these data cannot be applied to the European and North American contexts, whereas a precise estimation of these patients' prognosis is still lacking and first ART regimens are changed upon the necessity to achieve maximal efficacy while minimizing toxicity, taking into account previous ART classes and historical genotypic resistance test, drug toxicities, and patient's adherence and preferences.
The aim of this study was to estimate durability of second ART regimens in virologically suppressed patients and to assess factors associated with early discontinuation.
Materials and Methods
The Italian Cohort Naive Antiretrovirals Foundation Study (ICONA) is a multicenter, prospective, and observational study recruiting PLWHIV, which was founded in 1997 and collects patients' data starting from infection diagnosis. Eligible patients have to be at least 18 years of age and have to sign consent forms in accordance with the ethical standards of the committee on human experimentation and the Helsinki Declaration (1983 revision). Demographics, clinical, laboratory data, and information on therapies are collected and recorded online (
We performed a retrospective analysis of this prospectively collected database, including all patients who started first-line ART in Italy after January 1, 2008 and switched, subsequently, to second regimen with HIV-RNA load <50 copies/mL. Patient's follow-up was frozen on December 31, 2015. The study period was chosen to have homogeneous data in the context of modern drugs. The main endpoint of the analysis was second ART regimens' failure, which was defined as two consecutive HIV-RNA >200 copies/mL (virological failure) or discontinuation of any drug (treatment discontinuation), whichever occurred first. We have ignored all changes in formulations that did not imply a modification in the drugs used [e.g., changing from tenofovir/emtricitabine (TDF/FTC) plus efavirenz (EFV) to a single-tablet regimen (STR) containing TDF/FTC/EFV].
All causes of treatment discontinuations were coded in the ICONA database, including simplification, defined as the reduction of drugs in the regimen or the decrease in daily doses or pills, intolerance, defined as patient's rejection in the absence of any clinical and laboratory signs of drug harmfulness, and toxicity defined as an adverse effect related to exposure to that drug at usual doses. Other possible recorded reasons for treatment discontinuation were clinical failure, drug–drug interactions, lack of adherence, patient's decision, and medical decision, as reported by the treating physician.
Statistical analyses
Statistical analyses were carried out using standard survival analysis by Kaplan–Meier (KM) curves and KM estimates with 95% confidence intervals at 1, 2, and 3 years from baseline. Baseline of the analysis was the date of switch to the second ART. Patients' follow-up accrued from the date of the switch up to the date of the first of two HIV-RNA >200 copies/mL or first drug discontinuation or last clinical visit. Cox regression model was employed to identify factors associated with the risk of treatment discontinuation. The factors considered in the univariable analysis were: gender, age, risk factor for HIV infection, nationality, CDC stage at baseline, CD4+ count at ART start and at switch, hepatitis C virus (HCV) antibodies, hepatitis B surface antigen (HBsAg) status, type of first and second ART regimen and type of combination first–second regimen, cause of switch, calendar year, duration of first antiretroviral treatment, length of viral suppression during first ART, STR in second regimens, and change of backbone at switch.
The multivariable model included all factors retained from univariate analysis because of a p value <0.1. Analyses were performed with Stata 10.1 (StataCorp, College Station, TX).
Results
In the study period 7776 naive patients started their first ART regimens and 835 patients were then switched to second ART regimens and represented the study population according to the predefined inclusion criteria. Males were the predominant gender (81.3%), the median age at switch was 41 years [interquartile range (IQR), 34–49] and more than four-fifths were Italian (84.7%). Unprotected homosexual intercourses were the main reported risk factor for HIV infection (49.2%), followed by heterosexual intercourses (38.4%), whereas intravenous drug use was recorded in a minority of patients (6.2%). Coinfections with hepatitis B virus (HBV) and HCV were noticed in 4.5% and 9.5% cases, respectively.
First ART regimens
Almost half of the population showed at nadir a median CD4+ cell count <350 cell/mm3, and 177 patients (21.2%) a very low CD4+ cell count (<200 cell/mm3). Median peak HIV-RNA load was 4.7 log10 (IQR 4.2–5.2). As first regimen, the nucleoside reverse transcriptase inhibitor (NRTI) backbone was prescribed in all PLWHIV, except for 39 cases (4.7%), and was represented by TDF/FTC in 696 patients (83.3%) and by abacavir/lamivudine (ABC/3TC) in 43 patients (5.1%). Overall, the median time from the prescription of first ART to the switch was 16 months (IQR 9–26) and the HIV-RNA at switch was <50 copies/mL for 13 months (IQR 7–24) on average. Other characteristics of study population are described in Table 1.
HBsAg, hepatitis B surface antigen; HCV, hepatitis C virus; INSTI, integrase inhibitors; IQR, interquartile range; NNRTI, non-nucleoside reverse transcriptase inhibitors; NRTI, nucleoside reverse transcriptase inhibitors; PI/r, protease inhibitors/ritonavir.
Second ART regimens
CD4+ cell count at the switch was >500 cell/mm3 in 53.8% patients and only 6.5% demonstrated a poor immunological response (CD4+ cell count <200 cell/mm3). Causes of first to second ART regimens switch were: toxicity (355 patients, 42.5%), simplification (313 patients, 37.5%), enrolment in clinical trials (42 patients, 5%), availability of more effective drugs (16 patients, 1.9%), patient's decision (14 patients, 1.7%), and other causes (49 patients, 5.9%). Reasons were missed for 61 patients (7.3%). According to the per calendar year analysis, 210 PLWHIV (25.1%) changed therapy in the first period of study evaluation (2008–2011), whereas the majority of therapeutic modifications (625 patients, 74.9%) was made in the second phase (2012–2015).
Table 2 summarizes the details of treatment modifications from first to second ART regimens. The NRTI backbone was removed or changed in 200 patients (24%), whereas the switch involved the third drug in 530 cases (63.5%) and 105 patients (12.5%) received a completely new regimen.
This table does not include 138 subjects who changed only backbone while third drug remained the same.
ART, antiretroviral therapy; INSTI, integrase inhibitors; NRTI, nucleoside reverse transcriptase inhibitors; NNRTI, non-nucleoside reverse transcriptase inhibitors; PI/r, protease inhibitors/ritonavir.
In second ART regimens the proportion between non nucleoside reverse transcriptase inhibitors (NNRTIs) and PI/r was inverted, with the first class accounting for the 44.2% of the new anchor drugs, and the latter for the 29.4%. Other combinations rose gradually reaching the 7.8% for NRTIs plus integrase inhibitor (INSTI) and the 14.4% for NRTI-sparing regimen; about 35 patients (4.2%) received drugs belonging to none of the previous classes.
One hundred thirty-eight patients (16.5%) changed only the backbone. STRs were prescribed in 256 second antiretroviral treatments and these patients were previously either on a PI/r-based therapy (47.7%) or on a NNRTI-based regimen (37.1%).
Outcomes
Treatment failure was observed in 267 subjects over a period of 1144 person-year follow-up (PYFU) with an overall incidence of treatment failure of 23.3 × 100 PYFU, and median time between the switch and the second ART regimen cessation was 9.2 months (IQR 3.6–15). Discontinuation of second ART regimens due to virological failure was observed in 37 patients (13.9%), whereas was due to toxicity in 100 patients (37.5%) and simplification in 58 patients (21.7%). Among the other reasons recorded, there were patient's decision (19 patients, 7.1%), enrolment in clinical trial (4 patients, 1.5%), end of clinical trial (4 patients, 1.5%), disposability of more effective drugs (4 patients, 1.5%), medical decision (3 patients, 1.1%), pregnancy (3 patients, 1.1%), drug interactions (2 patients, 0.7%), and modifications according to guidelines (1 patient, 0.4%). Data were missed for 32 patients (12.0%). The probability of treatment failure at 12, 24, and 36 months was 21% [95% confidence interval (CI) 18.1–24.2], 35% (95% CI 31.0–39.3), and 48.2% (95% CI 43.0–53.7), respectively (Fig. 1).
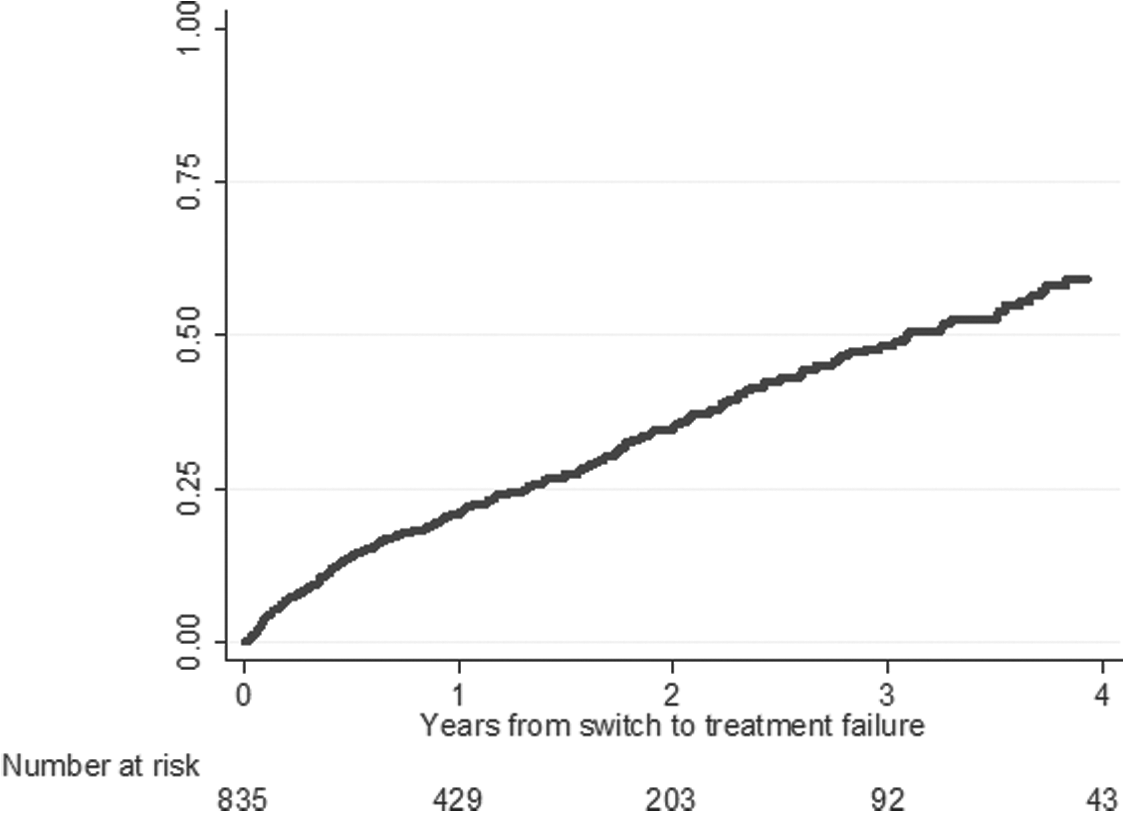
Kaplan–Meier curve estimating the probability of treatment failure.
At the univariate analysis, men who have sex with men (MSM) presented a major risk of second ART discontinuation [hazard ratio (HR) 0.73; 95% CI 0.57–0.95 vs. heterosexual; p = 0.02], as well as PLWHIV who switched ART regimens at their own request (HR 3.11 95% CI 1.45–6.68 vs. toxicity; p = 0.004). Other demographic and clinical characteristics, including age, gender, nationality, CD4+ cells count, and HCV coinfections were not associated with treatment failure.
STR prescription in second ART regimens had a protective effect on discontinuation (HR 0.59; 95% CI 0.43–0.80; p = 0.001), whereas longer duration of first ART regimens (HR 0.91 per 1 year increase; 95% CI 0.80–1.04; p = 0.16) and the length of virological suppression had minor influence (HR 0.89 per 1 year increase; 95% CI 0.78–1.00 p = 0.058).
Compared with the switch from one NNRTI to another NNRTI-based regimen, all the following types of switch showed an increased risk of discontinuation: from PI/r to PI/r (HR 2.47; 95% CI 1.45–4.23; p = 0.001), from PI/r to NRTI-sparing regimen (HR 2.01; 95% CI 1.13–3.59; p = 0.018), and from regimens containing third drugs belonging to two different classes to PI/r (HR 3.72; 95% CI 1.71–8.07; p < 0.001). No single drug demonstrated to specifically enhance the risk of treatment failure.
The multivariate analysis confirmed the increased risk of second ART failure switching from one PI/r to another PI/r (HR 1.95; 95% CI 1.10–3.48; p = 0.023), from a PI/r to a NRTIs-sparing regimen (HR 2.15; 95% CI 1.13–4.07; p = 0.02) and from complex ART regimens, containing more than one third drug (mega ART), to a PI/r (HR 3.04; 95% CI 1.21–7.60; p = 0.018) (Table 3). The risk of regimen failure increased consistently with all changes of first ART to unconventional regimens (HR 2.12, 95% CI 1.18–3.81; p = 0.012). The decreased risk of failure for patients taking STR in a second ART regimen did not reach statistical significance (HR 0.75, 95% CI 0.51–1.10; p = 0.142).
The model was adjusted also for HCV Ab positivity, CD4 cell count at switch, duration of viral suppression and STR second line.
AHR, adjusted hazard ratio; CI, confidence interval; HCV, hepatitis C virus; HR, hazard ratio; INSTI, integrase inhibitors; NRTI, nucleoside reverse transcriptase inhibitors; NNRTI, non-nucleoside reverse transcriptase inhibitors; PI/r, protease inhibitors/ritonavir; STR, single-tablet regimen.
Discussion
The maintenance of HIV-RNA <50 copies/mL is the guiding principle in every ART switch and clinicians should avoid the selection of resistances to preserve future treatment options. 11
In this study, the median durability of second ART regimens, among patients who discontinued the treatment, was 9.2 months. To the best of our knowledge this is one of the first attempts to estimate second ART regimens' durability in a high-income country, but the duration appeared to be significantly shorter than previously showed in a cohort from the United States. 12 Indeed, more than 20% of patients interrupted second ART regimens after 1 year, and half of them needed a third ART option within 3 years, leading to increased costs and morbidity. 13 Comparing these percentages with those from the first-line analysis of the same ICONA population, we found that treatment failure rates at 12 and 24 months tended to be lower in second ART regimens (second ART vs. first ART 21% vs. 26% at 12 months; 35% vs. 39.7% at 24 months), but similar after 36 months, 9 suggesting an overall limited durability of ART over years.
The low rate of virological failure observed in both first and second regimens confirmed the results of similar analyses based on the Europe Cohort. 14,15 This suggests that if viral suppression is achieved and adherence is maintained, the chance of failure is extremely low. Moreover, toxicity and simplification, accounting together for 80% cases, were identified as the main reasons for starting second ART, consistently with previous findings. 5,16,17
Different switch strategies led to different outcomes, and modifications within the PI/r class were related to an increased risk of second ART discontinuation. This is in contrast with studies that proposed ATV/r- and DRV/r-based treatment in PLWHIV previously on LPV/r, demonstrating not only an improvement in serum lipids, but also the maintenance of an undetectable viral load or better immunological parameters. 18,19 Discontinuation of second ART regimens was also more likely to happen when switching from PI/r to NRTI-sparing regimen. This choice aimed to the reduction of mid- and long-term NRTI side effects. 20 –32 Few studies have been published on virologically suppressed patients who switched to dual therapies, and our results underlined the concerns about NRTI-sparing regimens' long-term efficacy. 33 Furthermore, dual therapies' effectiveness has been addressed in a recent meta-analysis, which suggested caution for the potential selection of resistant viral strains. 34
Considering prescription trends over the time, about three-fourths of the changes were made in most recent years (2012–2015). This appears to be justified by the arrival of new and more tolerated drugs [rilpivirine, elvitegravir/cobicistat (EVG/COBI) and DRV/r 800/100 once daily] and new STR formulations (TDF/FTC/RPV and TDF/FTC/EVG/COBI). 35 –38 Overall STRs accounted for the 30.5% of second ART and showed a significant protective effect against treatment discontinuation at the univariate analysis. This result strengthens the importance of a once-daily strategy with a low pill burden, which has been demonstrated to improve the outcome in both naive and experienced PLWHIV, 38 –46 enhancing the adherence and reducing adverse effects. 47 –53
In our cohort, only a minority of patients were taking an INSTI-based therapy, following local guidelines' and drugs' availability, but this percentage doubled over the observation period and the low rate of PI/r to INSTI switch could have been influenced by the results of the SWITCHMRK study. 54
Despite the different settings and the higher rate of virological failure in resource-limited countries, second and third ART regimens are urgently needed in these regions 55 and our study offers some insights on the expected durability, especially when toxicity is a major concern.
Nevertheless, our study has some limitations related to the retrospective nature of the analysis and the lack of adherence assessment, relying only on serum HIV-RNA as a proxy of patient's commitment to ART.
In summary, this study tried to fill a knowledge gap on second ART regimens' durability and factors associated with treatment discontinuation. Our data showed that, in a setting with free access to drugs and diagnostic tools, patients tended to switch earlier and at higher CD4+ cell counts. Any ART change requires an accurate evaluation and the right balance between efficacy and a low pill burden could be offered by new STR formulations, helping clinicians to enhance the durability of second ART regimens.
Footnotes
Acknowledgments
The ICONA Foundation Study is sponsored by unrestricted grants from Abbvie, Italy; Bristol-Myers Squibb, Italy; Gilead, Italy; Janssen, Italy; and ViiV Healthcare Italy. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the article.
ICONA Foundations Study
BOARD OF DIRECTORS: A. d'Arminio Monforte (Vice President), M. Andreoni, G. Angarano, A. Antinori, F. Castelli, R. Cauda, G. Di Perri, M. Galli, R. Iardino, G. Ippolito, A. Lazzarin, C.F. Perno, F. von Schloesser, and P. Viale. SCIENTIFIC SECRETARY: A. d'Arminio Monforte, A. Antinori, A. Castagna, F. Ceccherini-Silberstein, A. Cozzi-Lepri, E. Girardi, S. Lo Caputo, C. Mussini, and M. Puoti. STEERING COMMITTE: M. Andreoni, A. Ammassari, A. Antinori, C. Balotta, A. Bandera, P. Bonfanti, S. Bonora, M. Borderi, A. Calcagno, L. Calza, M.R. Capobianchi, A. Castagna, F. Ceccherini-Silberstein, A. Cingolani, P. Cinque, A. Cozzi-Lepri, A. d'Arminio Monforte, A. De Luca, A. Di Biagio, E. Girardi, N. Gianotti, A. Gori, G. Guaraldi, G. Lapadula, M. Lichtner, S. Lo Caputo, G. Madeddu, F. Maggiolo, G. Marchetti, S. Marcotullio, L. Monno, C. Mussini, S. Nozza, M. Puoti, E. Quiros Roldan, R. Rossotti, S. Rusconi, M.M. Santoro, A. Saracino, and M. Zaccarelli. STATISTICAL AND MONITORING TEAM: A. Cozzi-Lepri, I. Fanti, L. Galli, P. Lorenzini, A. Rodano, M. Shanyinde, and A. Tavelli. BIOLOGICAL BANK INMI: F. Carletti, S. Carrara, A. Di Caro, S. Graziano, F. Petrone, G. Prota, S. Quartu, and S. Truffa. PARTICIPATING PHYSICIANS AND CENTERS: Italy A. Giacometti, A. Costantini, C. Valeriani (Ancona); G. Angarano, L. Monno, C. Santoro (Bari); F. Maggiolo, C. Suardi (Bergamo); P. Viale, V. Donati, G. Verucchi (Bologna); F. Castelli, E. Quiros Roldan, C. Minardi (Brescia); T. Quirino, C. Abeli (Busto Arsizio); P.E. Manconi, P. Piano (Cagliari); B. Cacopardo, B. Celesia (Catania); J. Vecchiet, K. Falasca (Chieti); L. Sighinolfi, D. Segala (Ferrara); F. Mazzotta, F. Vichi (Firenze); G. Cassola, C. Viscoli, A. Alessandrini, N. Bobbio, G. Mazzarello (Genova); C. Mastroianni, V. Belvisi (Latina); P. Bonfanti, I. Caramma (Lecco); A. Chiodera, A.P. Castelli (Macerata); M. Galli, A. Lazzarin, G. Rizzardini, M. Puoti, A. d'Arminio Monforte, A.L. Ridolfo, R. Piolini, A. Castagna, S. Salpietro, L. Carenzi, M.C. Moioli, C. Tincati, G. Marchetti (Milano); C. Mussini, C. Puzzolante (Modena); A. Gori, G. Lapadula (Monza); N. Abrescia, A. Chirianni, G. Borgia, F. Di Martino, L. Maddaloni, I. Gentile, R. Orlando (Napoli); F. Baldelli, D. Francisci (Perugia); G. Parruti, T. Ursini (Pescara); G. Magnani, M.A. Ursitti (Reggio Emilia); R. Cauda, M. Andreoni, A. Antinori, V. Vullo, A. Cristaudo, A. Cingolani, G. Baldin, S. Cicalini, L. Gallo, E. Nicastri, R. Acinapura, M. Capozzi, R. Libertone, S. Savinelli, A. Latini (Roma); M. Cecchetto, F. Viviani (Rovigo); M.S. Mura, G. Madeddu (Sassari); A. De Luca, B. Rossetti (Siena); P. Caramello, G. Di Perri, G.C. Orofino, S. Bonora, M. Sciandra (Torino); M. Bassetti, A. Londero (Udine); and G. Pellizzer, V. Manfrin (Vicenza).
Authors' Contribution
A.D.B. and G.G. contributed equally. A.D.B., G.G., P.L., and A.D.M. conceived and designed the study; P.L. performed statistical analyses. All authors contributed to the interpretation of data. A.D.B., G.G., and P.L. drafted the article. All authors reviewed the article critically for important intellectual content and approved the final version.
Author Disclosure Statement
No competing financial interests exist.