
Abstract
Community participation is vital for the recovery and empowerment of men who have sex with men (MSM) living with HIV. Intersectionality also provides an important lens that inequalities operate in an intersectional manner and pose compound challenges to the lives of minority individuals. However, the association between intersecting stigma toward HIV-positive MSM and their community participation is underexplored. The study drew on a sample of young Chinese MSM living with HIV from a community-based online survey that recruited respondents using nonprobability purposive sampling (n = 1004). Structural equation modeling was performed to investigate the associations among perceived stigma against sexual minorities and people living with HIV, HIV-related self-stigma, and HIV/AIDS community participation. The indirect effect of self-stigma and the statistical interaction between perceived homosexual stigma and perceived HIV-related stigma were further examined. Results show that total direct effect was significant [B (SE) = 0.859 (0.233); confidence interval (95% CI) = 0.402–1.316]. Perceived HIV-related stigma was positively correlated with HIV/AIDS community participation, while HIV-related self-stigma was negatively correlated. The mediating role of HIV-related self-stigma was significant in both types of perceived stigma [total indirect effect: B (SE) = −0.935 (0.175); 95% CI = −1.277 to −0.593]. The interaction effect was also significant and negative [B (SE) = −0.117 (0.056), p < 0.001], showing that perceived homosexual stigma could offset the effect of perceived HIV-related stigma on HIV-related self-stigma. The findings illustrate how intersecting stigma is involved in HIV-related self-stigma and community participation and highlight the importance of applying an intersectionality perspective to investigate stigma toward MSM living with HIV and their community participation.
Introduction
HIV/AIDS has become a pressing concern among the younger generation in China. The Chinese Center for Disease Control and Prevention recorded a 30–50% annual growth rate of new HIV/AIDS diagnoses among college students in recent past years. 1 In particular, men who have sex with men (MSM) experienced a surge of HIV/AIDS, accounting for 28% of the 96,000 new diagnoses in the first three-quarters of 2016. 2 This disproportionate level of HIV/AIDS among MSM has created a problem—the intersecting stigma against HIV/AIDS and MSM. Previous studies have called for research and actions into the intersection of these two forms of stigma to ameliorate their adverse impact. 3,4
Intersectionality theory seeks to illuminate the “mutually enforcing effects of various social locations and experiences of domination and oppression” (p. 272). 5 Most intersectionality researchers disagree with the premise that patterns of inequality are either unitary or equal; instead, they consider the systems of oppression to be fluid and mutually reinforcing. 6 –8 Scholars have applied intersectionality to examine the experiences of intersecting stigma among people living with HIV (PLHIV). For example, Rice et al. suggest that women living with HIV tend to perceive interrelated forms of stigma coming from various sources of interpersonal relationships, communities, and social structures. 9 In addition, several studies have investigated the negative consequences of intersectional stigma, such as how it exerts compound negative impacts on psychosocial well-being of MSM living with HIV, 10 and how the intersecting internalized stigmas can influence HIV self-care among HIV-positive MSM who use substances. 11 Nevertheless, less is known about how intersecting perceived stigma heightens self-stigma.
The analytic approaches to disentangling intersectionality are still developing. 12 The statistical technique of moderation analysis appears useful and appropriate as it addresses how a combination of multiple factors uniquely shapes an individual's experience. 13 Previous studies have applied a moderation analysis to investigate the outcomes of intersecting stigma. 14,15 The present study addressed these research gaps by investigating the intersection through an interaction analysis, hypothesizing perceived homosexual stigma as a moderator in the association of perceived HIV-related stigma with HIV-related self-stigma.
Promoting PLHIV's community participation is crucial to enhancing their personal health and collective well-being. 16,17 PLHIV's community participation has been found to improve their adherence to HIV/AIDS treatment and social services 18,19 and eliminate their self-stigma. 20 Moreover, community participation can empower PLHIV to gain momentum and resources to confront social stigma and structural barriers and fulfil community members' diverse needs. 21 Meanwhile, discrimination against sexual minorities persists in Chinese societies. 22 The HIV epidemic has also drawn the attention of various parties to sexual minority people's health issues. 23,24 In China, collaboration between publicly funded HIV programs and community-based organizations has become a primary model of prevention and support. 25 In addition, the development of patient-centered and LGBT-friendly services to promote the Chinese sexual minorities' participation in health services is increasingly advocated. 26,27 Therefore, promoting participation in the HIV/AIDS community has become a pressing area of service for Chinese MSM living with HIV.
The relationship between perceived stigma and community participation is intricate. The rejection-identification model suggests that people's perceived prejudice can promote their group identification and community engagement. 28 Molero et al. 29 found that perceived HIV-related stigma could increase PLHIV's in-group identification and further motivate collective action. However, researchers have also observed the “why try” phenomenon that self-stigma resulting from applying stereotypes to oneself may generate a sense of futility, undermining a person's confidence to achieve personal goals and maintain interpersonal relationships. 30,31 Empirical research has consistently found the adverse effects of self-stigma on community connectedness, 32 group identification, 33 and engagement in health care 34 among PLHIV. These studies highlight the pivotal role of self-stigma in hindering minority individuals' engagement in the broader community.
The psychological mediation framework 35 further explains how perceived distal stigma-related stressors “get under the skin,” affecting psychological and behavioral outcomes through various psychosocial mediators (e.g., self-stigma). 36,37 In addition to exploring psychopathological outcomes, one study also used the framework and showed that perceived HIV-related stigma could affect social relationships among HIV-positive MSM by strengthening their negative self-concept. 38 Viewing this theoretical and empirical literature together, this study proposed a mediation model to examine how perceived stigma affects Chinese HIV-positive MSM's community participation and hypothesized self-stigma as a mediator.
The Present Study
As reviewed above, this study aimed to investigate (1) the direct relationships between stigma associated with homosexuality and HIV/AIDS and HIV/AIDS community participation, (2) the mediating role of HIV self-stigma in the indirect associations between perceived stigma and HIV/AIDS community participation, and (3) whether perceived homosexual stigma and HIV stigma intersect to elevate self-stigma among Chinese MSM living with HIV. In addition, defining community participation as a multidimensional construct, 39 we investigated their distinct correlations with both HIV-related and homosexual stigma among young MSM living with HIV. We proposed the following conceptual framework (Fig. 1).
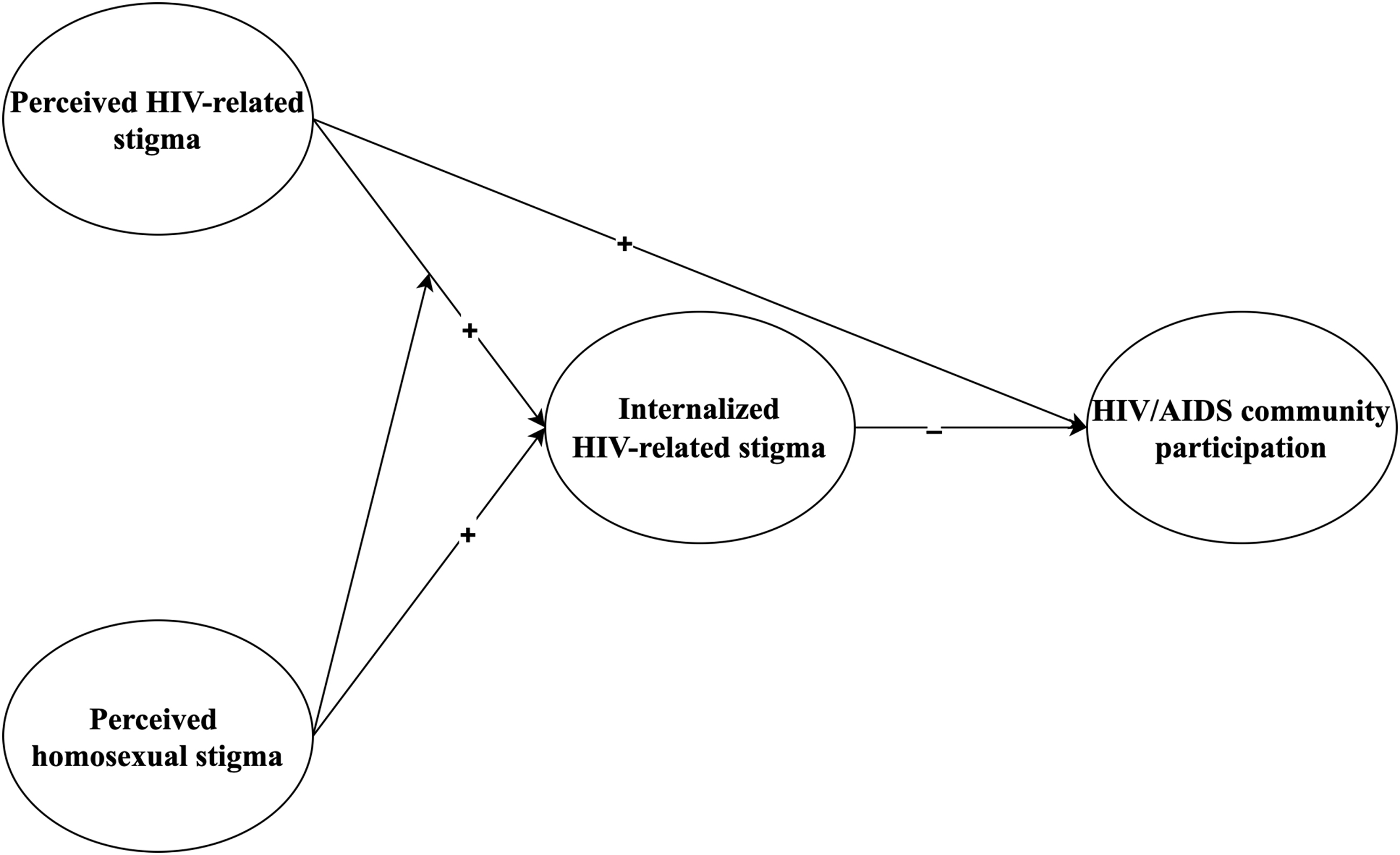
Conceptual framework.
Methods
Respondent recruitment
Data were drawn from a large community-based online survey of MSM living with HIV in China aged 18–30 years. Given that the target population is a hard-to-reach, hidden group, 40 we adopted nonprobability purposive sampling to recruit respondents between July 26 and September 30, 2020. A recruitment advertisement was circulated via WeChat, a popular social media app in China. This has been considered a particularly effective and suitable method of recruitment for social investigation in China. 41 The recruitment message was posted on HIV/AIDS-related WeChat Official Accounts, such as “China's CDC” and “UNAIDS2030.”
Potential respondents who showed an initial interest in the survey were directed to an online survey platform, Qualtrics, to read about the purpose and procedure of the survey. Respondents had to click “agree” to indicate their consent before enrolling in the survey, completion of which took around 30 min. Each respondent who completed the entire survey was given an honorarium valued at RMB20. The study was approved by the Human Research Ethics Committee at the University of Hong Kong (EA2005010).
Of 2392 individuals who visited the survey website, 1353 consented to participate and completed the survey. The sample size of this study was 1004 after removing 228 who did not self-identify as homosexual, 96 who were older than the age of 30, 17 who were female, and 8 who were non-HIV-positive.
Measures
Sociodemographics
Respondents' age (18–30 years), educational status, employment status, length of HIV infection diagnosis, and HIV medicine use were collected.
Perceived stigma
Respondents' perceived homosexual stigma and HIV stigma were measured by the Chinese version of the HIV and Homosexuality-Related Stigma Scales that have been validated with Chinese samples. 42 Specifically, the 10-item perceived homosexual stigma subscale (e.g., “many people unwillingly accept gay individuals”) was adapted from a set of scales used to assess perceived racial and homosexual stigma of Latino MSM. 43 The 7-item perceived HIV Stigma subscale (e.g., “HIV-infected people should be ostracized by their spouse and family members”) was adapted from a series of Chinese studies exploring the perception of HIV stigma. 44,45 The two subscales have been widely applied to measure perceived stigma of Chinese MSM and PLHIV. 46,47 Both subscales were rated on a 4-point Likert scale from 1 (strongly disagree) to 4 (strongly agree), and their Cronbach's alphas in this study were 0.870 and 0.881, respectively. Use of the Chinese versions of the two subscales in this study has been authorized by the scale developers.
Internalized HIV-related stigma
The Internalized AIDS-Related Stigma Scale 48 was used to assess respondents' internalized beliefs about their HIV-positive status. The scale was translated into Chinese by the first author and reviewed by the second author (both are fluent in both English and Mandarin). Responses of the six items (e.g., “it is difficult to tell people about your HIV-positive status”) are provided on a 4-point Likert scale from 1 (strongly disagree) to 4 (strongly agree). A higher sum score indicates a higher level of internalized HIV-related stigma. In this study, Cronbach's alpha of this subscale was 0.837.
HIV/AIDS community participation
Three separate constructs, participation in organizational activities (e.g., frequency each week of engaging in the organization) (never to often), 49 decision-making (i.e., “what role do you regard yourself playing in the HIV/AIDS community?”—“I take no part at all” to “I am a full partner in planning,” decision-making, and implementation), 50 and as a community representative (e.g., feeling essential in the community) (strongly disagree to strongly agree), 51 measured the extent of respondents' participation in the HIV/AIDS community. 39 Cronbach's alpha for the three-item Participation in Organizational Activities subscale was 0.907 and 0.842 for the 4-item Participation as a Community Representative subscale. These subscales have been used with Chinese samples 32 and were translated into Chinese by the first author and reviewed by the second author.
Data analysis
Respondents' sociodemographic characteristics were computed. Before testing the hypothesized model, we ran confirmatory factor analysis to determine whether the data fit a hypothesized measurement model. Five indices were used to determine the model's goodness-of-fit, that is, chi-square (χ 2 ), comparative fit index (CFI), Tucker Lewis Index (TLI), the root mean square error of approximation (RMSEA), and the standardized root mean square residual (SRMR) metrics. CFI and TLI values above 0.90 and RMSEA and SRMR values below 0.06 suggest acceptable model fits. 52,53
Using Mplus version 8.3, the hypothesized model was tested within a structural equation model, controlling for all sociodemographic variables. Specifically, the XWITH function relying on random effects modeling was used to define the latent variable interaction between perceived homosexual stigma and perceived HIV-related stigma. The Johnson-Neyman (J-N) technique was adopted to interpret the moderating effect and to determine the regions of significance with confidence intervals (95% CI). 54
For illustration, we also tested the simple slope at three points [i.e., M − 1SD (standard deviation), M, and M + 1SD] along with two critical values (i.e., M + 1.25SD and M + 5.25SD). The indirect effects of internalized HIV-related stigma were evaluated using the Model Constraint instead of the Model Indirect command because the latter is unsuitable for random effects modeling. Ninety-five percent CIs were generated to assess the significance of simple slope tests and indirect effects; the effect was significant at the 0.05 level if zero was not included in the 95% CI. 55
Results
Table 1 outlines respondents' sociodemographic characteristics. The mean age of the sample was 25.21 years (SD = 3.18), and nearly 80% had a bachelor or higher degree. Over 65% were in full- or part-time employment. The average length of HIV diagnosis was 2.83 years (SD = 2.45). Most respondents had undergone antiretroviral treatment.
Sociodemographic Characteristics of Respondents (N = 1004)
M, mean; SD, standard deviation.
The measurement model demonstrated acceptable model fit indices [χ 2 (391) = 1661.004, p < 0.001, CFI = 0.916, TLI = 0.906, RMSEA = 0.057, and SRMR = 0.045]. Factor loadings of the five latent constructs (i.e., perceived homosexual stigma, perceived HIV-related stigma, internalized HIV-related stigma, participation in organizational activities, and participation as a community representative) were significant, ranging from 0.578 to 0.763, 0.629 to 0.821, 0.678 to 0.893, 0.833 to 0.932, and 0.597 to 0.897, respectively. The results indicated that the observed variables adequately measure the latent constructs.
In the hypothesized model as shown in Table 2 and Fig. 2, both perceived homosexual stigma (β = 0.168, p < 0.01) and perceived HIV-related stigma (β = 0.4, p < 0.001) were positively associated with internalized HIV-related stigma. Perceived HIV-related stigma was positively related to participation in organizational activities (β = 0.204, p < 0.001) and participation in decision-making (β = 0.161, p < 0.01). However, internalized HIV-related stigma was negatively correlated with all three constructs of HIV/AIDS community participation—participation in organizational activities (β = −0.407, p < 0.001), participation in decision-making (β = −0.306, p < 0.001), and participation as a community representative (β = −0.209, p < 0.001). In addition, Table 3 shows that internalized HIV-related stigma partially mediated the relationships between the two types of perceived stigma and all three variables of HIV/AIDS community participation.
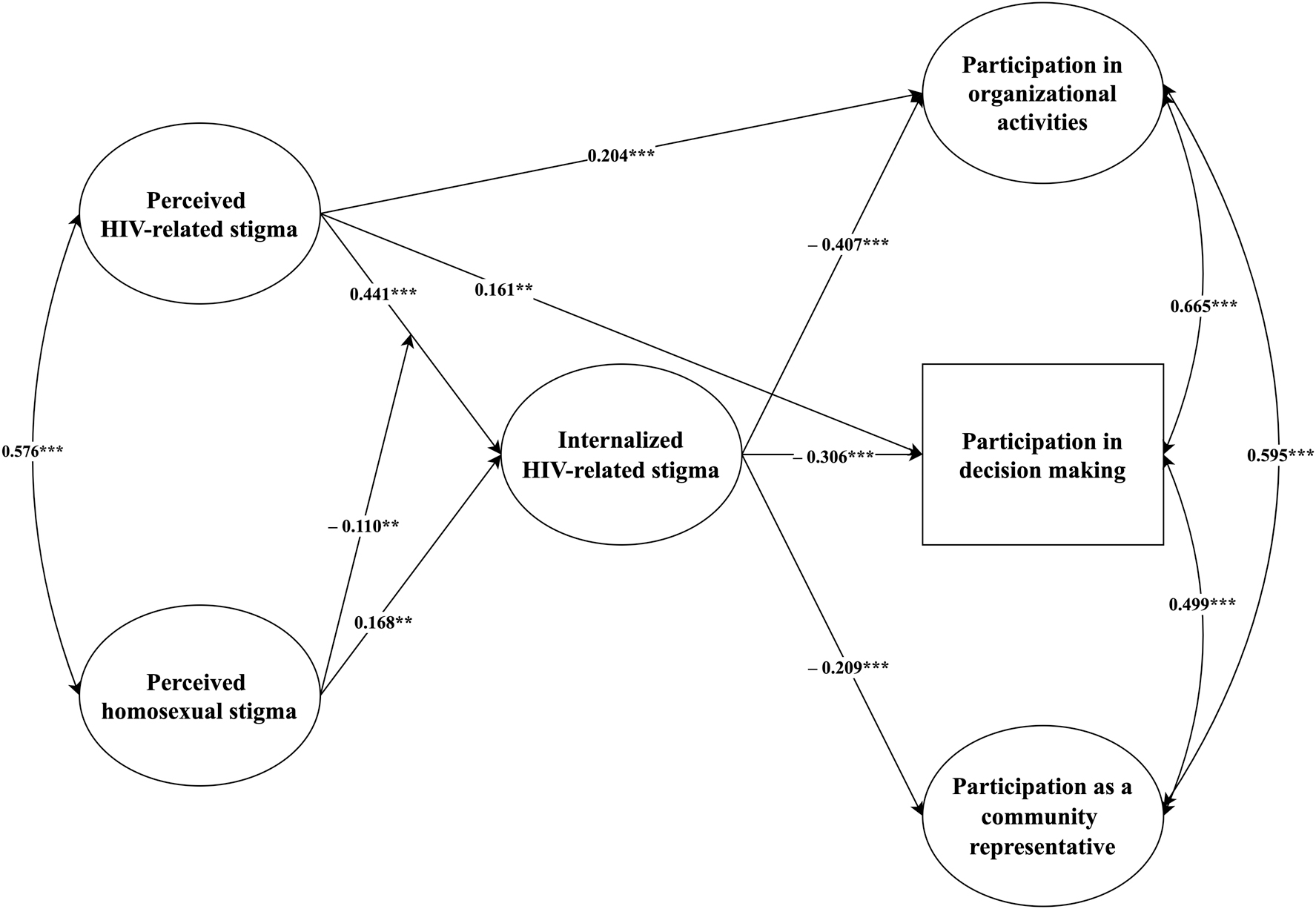
Model for perceived homosexual stigma, perceived HIV-related stigma, internalized HIV-related stigma, and HIV/AIDS community participation among young Chinese MSM living with HIV. MSM, men who have sex with men.
Path Model Parameter Estimates Among Young Chinese Men Who Have Sex With Men (MSM) Living with HIV (N = 1004)
p < 0.001, ** p < 0.01, * p < 0.05.
B, unstandardized coefficient; β, standardized coefficient; SE, standard error.
Regression Coefficients and 95% Confidence Intervals for Direct and Indirect Effects on HIV/AIDS Community Participation and Conditional Effects of Perceived Homosexual Stigma Among Young Chinese Men Who Have Sex With Men (MSM) Living with HIV (N = 1004)
CI, confidence interval; B, unstandardized coefficient; M, mean; SD, standard deviation; SE, standard error.
The simple slope tests showed that the link between perceived HIV-related stigma and internalized HIV-related stigma was significant at the M − 1SD, M, and M + 1SD points (Table 3). The J-N technique (Fig. 3) further indicated the continuous range of both moderator (i.e., perceived homosexual stigma) and the adjusted effect of perceived HIV-related stigma on internalized HIV-related stigma, showing that the effect generally declined with an increase in perceived homosexual stigma. In particular, the J-N graph showed that perceived HIV-related stigma was not significantly associated with internalized HIV-related stigma one way or the other for those between 1.25 SD above and 5.25 SD below the average level of perceived homosexual stigma. The simple slope tests of both these critical values are shown in Table 3.
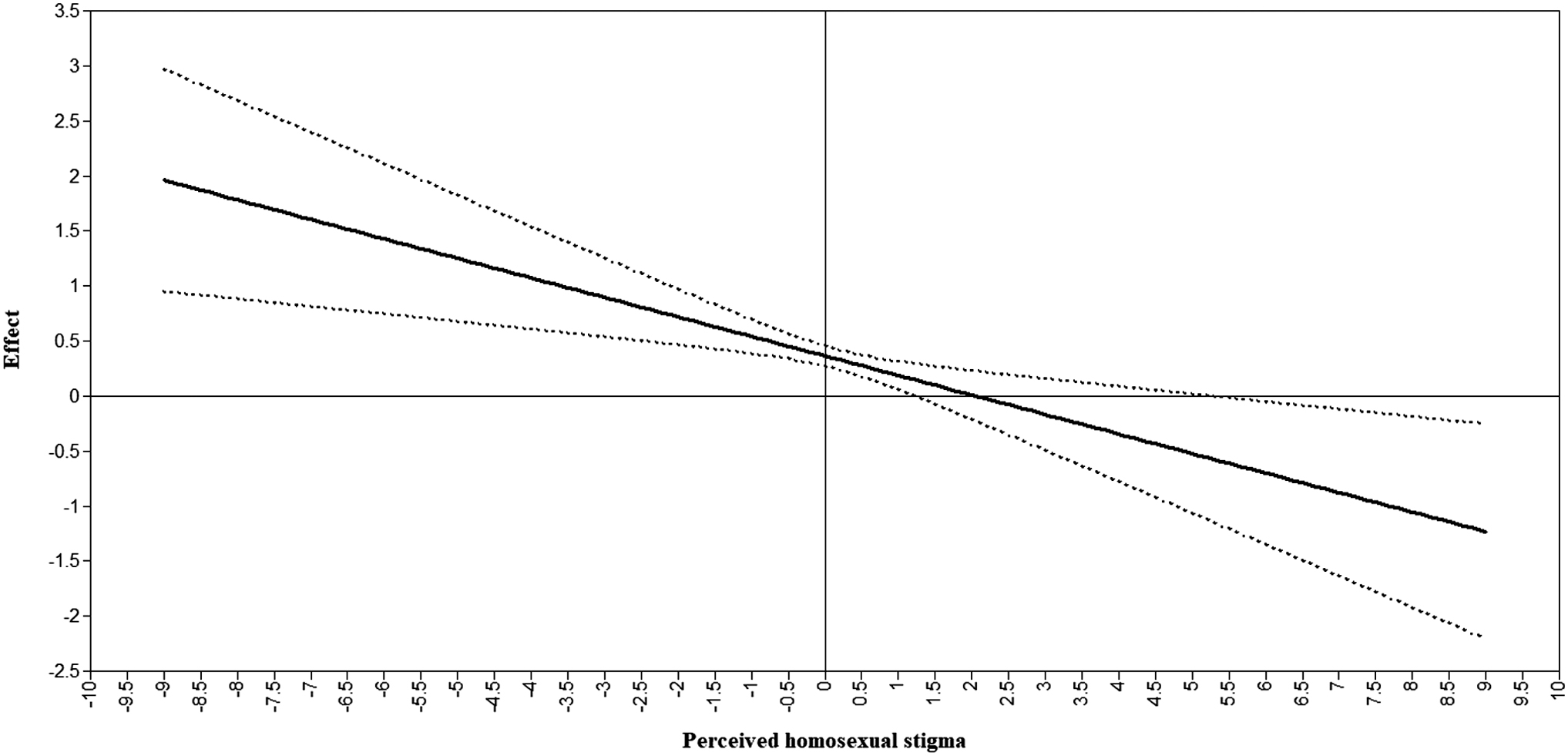
The effect of perceived HIV-related stigma on internalized HIV-related stigma moderated by perceived homosexual stigma with Johnson-Neyman 95% confidence intervals.
Discussion
This study examined the effect of the intersection of perceived homosexual stigma and perceived HIV-related stigma on self-stigma among Chinese MSM living with HIV and the indirect effect of HIV self-stigma on the associations between perceived stigma and HIV/AIDS community participation. While previous studies have illustrated the positive role of HIV/AIDS community engagement in China, 17,56 this study is the first to incorporate intersectionality theory to explore how stigma against HIV-positive MSM is implicated in engagement with the HIV/AIDS community. A novel contribution is the study's focus on community engagement among the younger generation in China, which has experienced a steep increase in HIV diagnosis rates. 1
Consistent with the rejection-identification model elucidating that perceived stigma enhances group identification and community engagement, 28 the results of this study suggest that respondents' perceived HIV-related stigma was positively associated with their HIV/AIDS community participation. However, there was no significant relationship between the three constructs of HIV/AIDS community participation and perceived homosexual stigma. The results suggest that only negative judgment against the HIV-positive status of HIV-positive MSM produces a significant direct effect on their engagement in the HIV/AIDS community.
Unlike previous research, 29 this study conceptualized participation in the HIV/AIDS community as a three-dimensional construct. The SEM results show that perceived HIV-related stigma contributed to respondents' participation in organizational activities and decision-making, but was not linked to their participation as a community representative. As Branscombe et al. note, 28 a common response to discrimination against the group to which one belongs is to elevate identification and investment in the group to feel accepted and achieve a high level of psychological well-being.
Regarding the three constructs of community engagement, the degree of engagement in community activities and perceived role in the community are more related to engagement in and contribution to the community. 39 In contrast, respondents' representativeness in the community depends on their leadership and how they represent their fellow community members. 51 Furthermore, the short average length of HIV infection diagnosis among respondents—more than 85% had a diagnosis <6 years—might also impact their ability to be a representative of the HIV/AIDS community.
Another important finding of this study resonated with the “why try” phenomenon and found a reverse correlation between respondents' internalization of HIV-related stigma and their HIV/AIDS community participation. This result was consistent with previous research showing that self-stigma could compromise one's community engagement. 32 –34 In the model, the negative consequences of internalized HIV-related stigma are in stark contrast to the positive role of perceived HIV-related stigma, indicating that people's engagement in their community varies according to their response to the stigma. Thus, the mere perception of stigma may unite group members, whereas further internalization may disengage members from their community.
The study also highlighted the mediating role of internalized HIV-related stigma in support of the psychological mediation framework. 35 Although the framework has been widely applied to analyze outcomes in addition to psychopathology, 36 such as quality of life 37 and interpersonal relationships, 38 it has never been used to disentangle the interplay between perceived stigma, self-stigma, and community participation. The findings indicate that despite the positive association of perceived HIV-related stigma with community engagement, it could simultaneously lead to people's internalization of stigma, and in turn, undermine their engagement in the community. It is noteworthy that the internalization of HIV-related stigma fully mediates the associations of perceived homosexual stigma with HIV/AIDS community engagement. The result elucidates this complex process through which perceived stigma of HIV-positive MSM disrupts their community participation partly by inducing the internalization of stigma.
The relationships between both types of perceived stigma and internalized HIV-related stigma support the application of intersectionality theory and shed light on intersecting stigma perceived by HIV-positive MSM. 6,8 First, HIV-related self-stigma stems from both the internalization of HIV-related stigma and some attributes of other types of stigma, such as stigma of sexual minority people. This finding enhances our knowledge about the process of self-stigma formation. We also performed statistical interaction analysis to investigate the outcome of the intersection of perceived HIV-related and perceived homosexual stigma. It is noteworthy that some scholars have noted the limitations of this approach because of the low probability of detecting significant interaction effects. 12,13 However, this study identified the significant main effects of the two types of perceived stigma and the interaction effect between them. The simple slope analysis revealed that the perception of homosexual stigma weakened the association between perceived HIV-related stigma and the internalization of HIV-related stigma.
Attribution theory provides a potential explanation for this interaction. Mak et al. 57 account for self-stigma among PLHIV/AIDS in a sequential attribution model that starts from controllability to responsibility and, in turn, to negative emotional reactions. 58 This result suggests that individuals' internalization of public stigma partly depends on how they explain their own stigmatized identities. Studies with HIV-positive MSM have found that compared with being MSM they thought they had greater control over and responsibility for contracting HIV. 59,60 In contrast, most MSM consider their sexual identity immutable and innate (i.e., that they were “born this way”). 61 Therefore, perceived homosexual stigma might provoke their essentialist beliefs about their sexual orientation and introduce alternative perspectives for HIV-positive MSM to contest public misunderstanding or judgments about PLHIV as immoral, dangerous, or responsible for the infection, thereby mitigating the pathway of applying HIV-related public stigma to themselves. However, this speculation is tentative and deserves further investigation.
This study was subject to several limitations. First, the cross-sectional design did not allow us to draw causal inferences. Future research should adopt a longitudinal design to delineate the causal relationships between stigma toward HIV-positive MSM and their HIV/AIDS community participation. Second, previous research 41 has demonstrated the suitability and usefulness of WeChat recruitment for social investigation in China. However, nonprobability sampling methods limit our ability to generalize the study findings. Third, although previous research has established the validity of the measures used in this study, 32,42,48 self-report data are inherently prone to measurement biases. Future research should use data from multiple sources to address this limitation. Fourth, the study investigated perceived and internalized stigma of young Chinese MSM living with HIV. Future studies should investigate the potential effect and the underlying mechanism of enacted stigma such as violence and prejudicial events on community participation. Finally, the study only focused on the levels of respondents' HIV/AIDS community involvement rather than their engagement in different types of community activities, such as community events and action. Future research can investigate the effects of stigma on specific forms of community participation.
This study makes three theoretical contributions. First, the distinct roles of perceived stigma and self-stigma in HIV-positive MSM's community participation and the mediational pathway suggest that exposure to stigma and stigmatized individuals' response should be accounted for when exploring how stigma affects community participation. Second, the significant mediating role of HIV-related self-stigma supports the psychological mediation framework. The result enriches the model by revealing that perceived stigma could hinder stigmatized individuals' community engagement and cause psychopathological outcomes. Third, the study findings resonate with intersectionality theory insofar as the multiple forms of perceived stigma simultaneously contribute to stigma internalization among MSM living with HIV. The significant moderation effect further illuminates the intersecting function of perceived stigma and the responses of stigmatized individuals with multiple disadvantaged identities. The negative interaction between perceived homosexual stigma and perceived HIV-related stigma reflects a unique attributional pathway of self-stigma.
This study highlights the intersecting perceived stigma among HIV-positive MSM and its respective and interactive contributions to their self-stigma and indicates the distinct effects of perceived stigma and self-stigma on HIV/AIDS community participation. These findings indicate implications for practice to improve community health and well-being among PLHIV. In China, considerable efforts have been made to advance community participation among PLHIV. However, the stigma related to HIV and MSM remain major obstacles. 62,63 This study thus identifies a pressing need to eliminate the intersecting stigma that HIV-positive MSM may perceive and internalize. The contribution of intersecting perceived stigma to self-stigma implies that interventions to reduce self-stigma among PLHIV need to consider the influence of coexisting and mutually reinforcing multiple forms of stigma. Moreover, nongovernment organizations need to strengthen community-building and encourage PLHIV to engage in their services and activities.
Footnotes
Authors' Contributions
Z.L.: conceptualization, data collection, data analysis, and writing; Y.H.: conceptualization and writing.
Acknowledgments
We thank Professor Eric Blyth for editing and proofreading the final draft of this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.