
Abstract
Introduction
Nonphagocytic NADPH oxidases provide major sources of ROS in the cardiovascular and renal systems (34). It is a complex that is composed of membrane-associated proteins, gp91phox (Nox2) and p22phox, which require cytosolic components, p47phox and p67phox, and the regulatory protein Rac (34). The discovery of Nox2 homolog, Nox1, was followed by other family members Nox3, Nox4, and Nox5 (Fig. 1). All cells in the cardiovascular system, including cardiomyocytes, endothelial cells, vascular smooth muscle cells, fibroblasts, and kidney tissue, express various catalytic subunits of NADPH oxidase (NOX) components. AngII strongly stimulates NOX activity and expression.
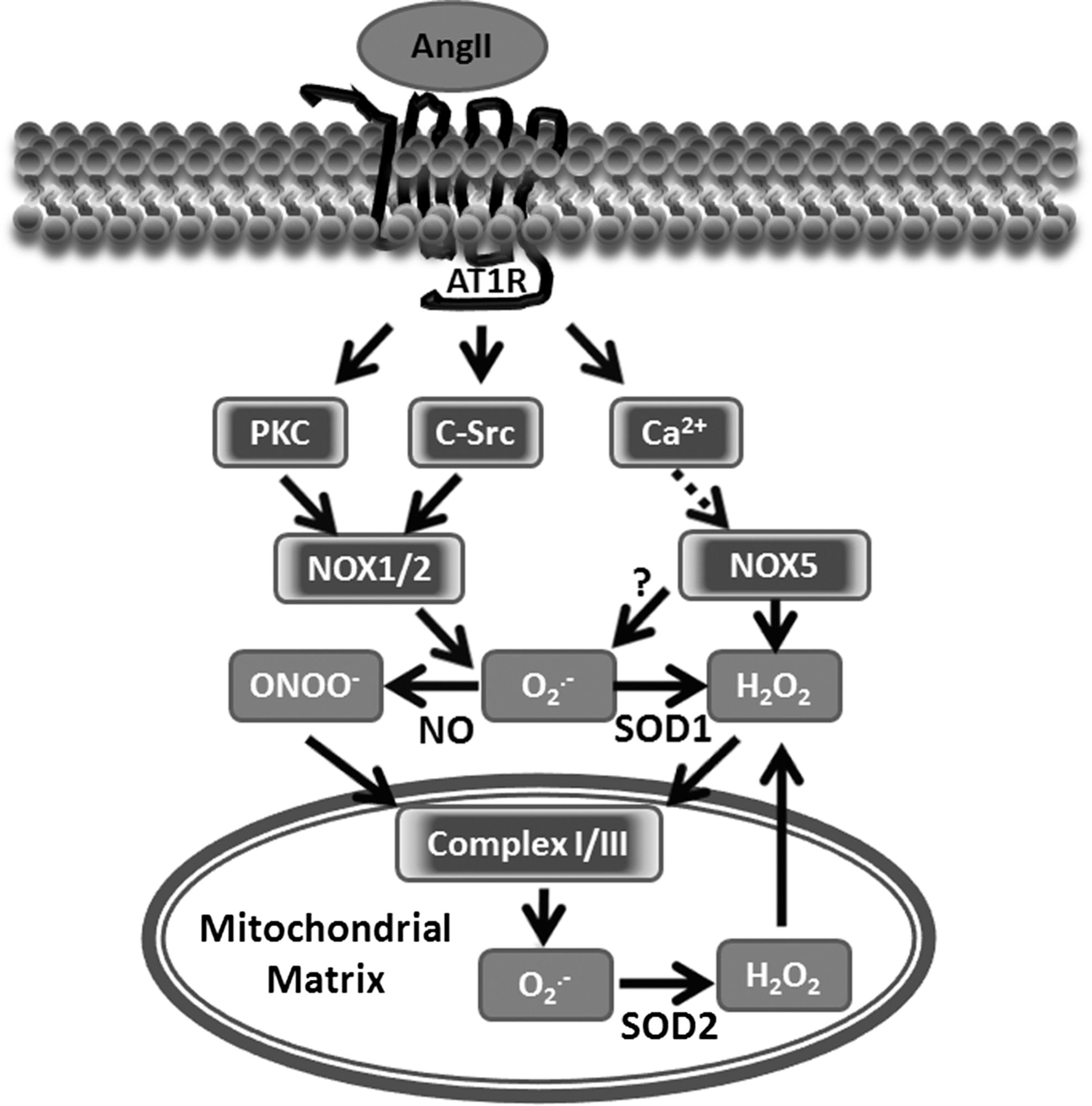
AngII activates NADPH oxidases by protein kinase C (PKC) and c-Src-dependent pathways (Fig. 1) (36). The initial activation of the AT1R leads to PKC-mediated phosphorylation of p47
phox
. This leads to c-Src activation and stimulation of the epidermal growth factor receptor, which evokes phosphatidylinositol 3-kinase-dependent production of phosphatidylinositol (3,4,5)-trisphosphate and, in turn, activates the Rac1 subunit of NADPH oxidase (55). Nox4 and Nox5 do not require p47
phox
or Rac1 subunits (43). Thus, in vascular cells, AngII primarily increases the activity of Nox1 or Nox2 (Fig. 1) (35). The activation of c-Src is redox sensitive and stimulated by H2O2 (60), which appears to represent a feed-forward mechanism whereby the H2O2-mediated activation of c-Src amplifies the NADPH oxidase activity of Nox1 and Nox2. It is important that Nox isoforms not only have different regulations and specific subcellular localization but also generate distinct ROS. For example, Nox4 is responsible for the basal production of H2O2, (19, 59), while Nox1 and Nox2 generates
Stimulation of Mitochondrial ROS by NADPH Oxidases
We have previously reported that AngII increases the production of mitochondrial ROS and decreases mitochondrial membrane potential, respiratory control ratio, and low-molecular-weight thiol content. The depletion of p22phox, an essential component for NADPH oxidase function, led to a significant decrease in ROS production in mitochondria isolated from AngII-treated cells. The inhibition of NADPH oxidases by apocynin or selective PKC inhibitor chelerythrine completely prevented AngII-induced mitochondrial dysfunction and attenuated the production of mitochondrial ROS (Fig. 1) (21). Interestingly, treatment with the mitochondrial ATP-sensitive potassium channels (mitoKATP) blocker 5-hydroxydecanoic acid or glibenclamide prevented the increase in mitochondrial H2O2, attenuated the decrease in mitochondrial membrane potential, and preserved respiratory control ratio and low-molecular-weight thiol content induced by AngII (21). This can be explained by the recently reported redox sensitivity of mitoKATP (51). Taken together, these results suggest that the stimulation of mitochondrial ROS by AngII requires the full enzymatic activity of NADPH oxidases and may depend on the activation of mitoKATP.
It has been recently reported that Nox4 is expressed in the mitochondria of rat kidney cortex (5) and in the mitochondria of cardiac myocytes (33). Ago et al. reported a higher expression of Nox4 in the mitochondrial fraction of cardiac myocytes compared with the microsomal fraction (1). Confocal microscopy showed significant co-localization of Nox4 with mitochondrial F1F0-ATP synthase, as well as the p22phox subunit of NADPH oxidases. These studies, however, remain highly controversial, as they were not able to directly demonstrate Nox4 activity in mitochondrial preparations. Our studies did not show the presence of Nox1, Nox2, Nox4, and p22phox subunits in the mitochondria of endothelial cells and vascular tissue, arguing against the mitochondrial localization of NADPH oxidases in these tissues (21). It has been previously shown that Nox4 is specifically localized in focal adhesions, along stress fibers, and in the nucleus (26, 41). It is possible that the mitochondrial localization of Nox4 reported by Block et al. (5) and Ago et al. (1) differs from previous publications (26, 41) due to the distinct Nox4 antibodies used for immunostaining, as many authors have raised concerns regarding the specificity of some Nox4 antibodies. The difference in Nox4 localization could be also due to the fact that these groups have investigated different cell types, and Nox4 localization in mitochondria may be cell-type specific. Although it may be intriguing to suggest the role of Nox4 in mitochondrial oxidative stress, the lack of data on mitochondrial p22phox and the absence of specific measurements of mitochondrial Nox4 activity have challenged this hypothesis. It is also important that mitochondria do not require any Nox isoform to produce ROS as just described, and ROS production by mitochondria can significantly surpass the amount of ROS produced by Nox4, particularly in the heart. It is conceivable that cytoplasmic Nox4 may contribute to the redox-sensitive upregulation of mitochondrial ROS production. Considering the controversy and inconsistent observations, the mitochondrial expression of Nox4 and its functional significance should be taken with caution and requires additional studies.
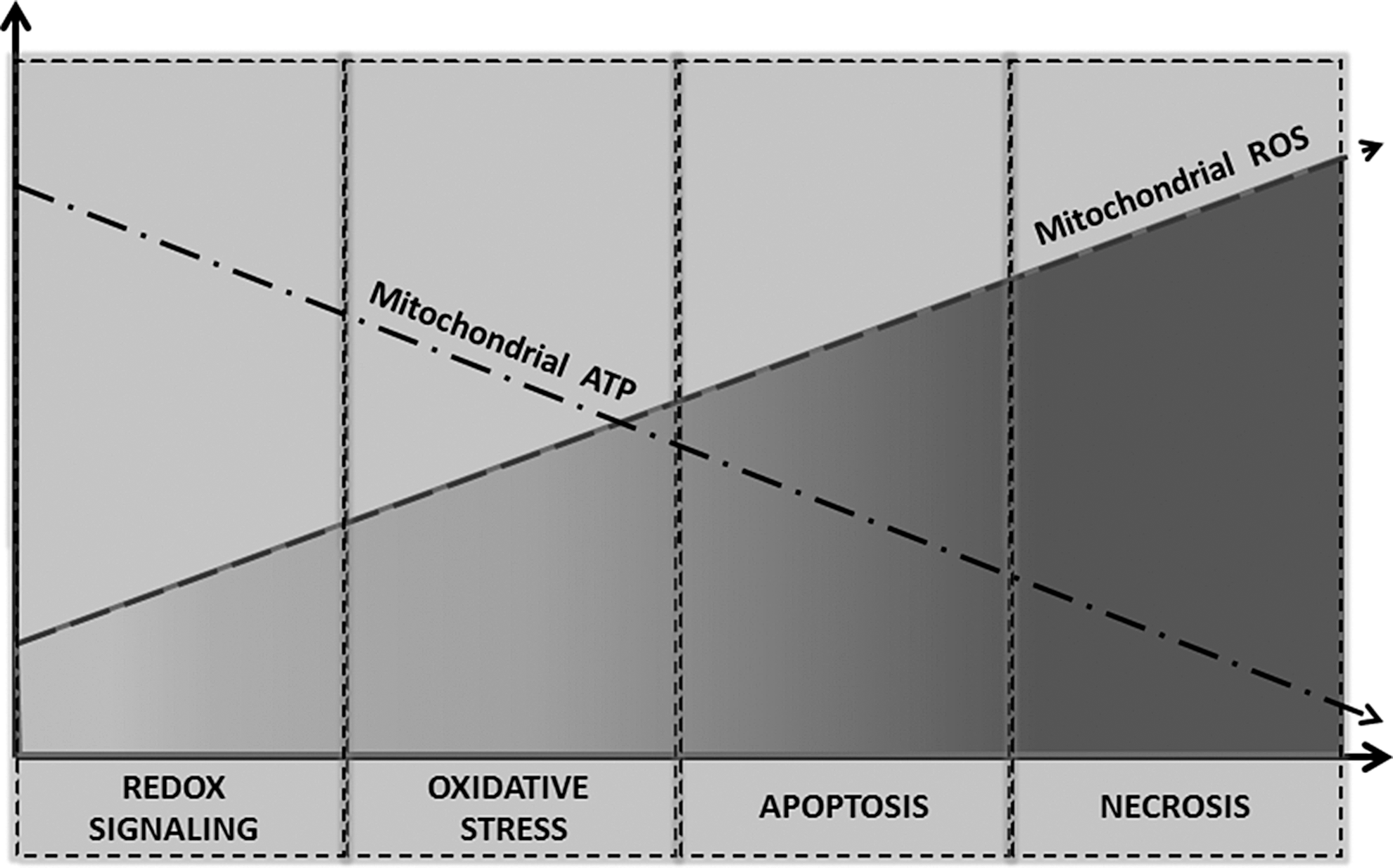
Mitochondria are a major source of ROS and play an important role in cellular redox signaling under normal physiological conditions. The stimulation of mitochondrial ROS by AngII is accompanied by mild uncoupling and decreases in ATP synthesis (21). The overproduction of mitochondrial ROS, however, leads to oxidative stress and a further decline in mitochondrial ATP. This may cause mitochondrial dysfunction and apoptosis or necrosis (Fig. 2). AngII-induced production of mitochondrial ROS in various pathophysiological conditions and different tissues is discussed next.
Hypertension
Hypertension promotes mitochondrial dysfunction in the brain, heart, vasculature, and kidney (16). These organs are involved in the development of hypertension, and mitochondrial dysfunction may contribute toward retaining hypertension as well as tissue damage observed in hypertension. It has been previously reported that AngII blockade improves mitochondrial function in the kidney of spontaneously hypertensive rats (SHRs). Elevated systolic blood pressure in SHR was accompanied by a reduced kidney mitochondrial membrane potential and an increased production of mitochondrial H2O2 compared with control animals. The treatment of SHR animals with AT1R antagonist candesartan normalized the mitochondrial membrane potential and inhibited the production of mitochondrial H2O2 (16). Interestingly, the treatment of SHR with Ca2+-channel blocker amlodipine reduced the blood pressure but did not affect the mitochondrial dysfunction, while the AT1R antagonist losartan improved both mitochondrial function and reduced mitochondrial H2O2 (17). This difference between amlodipine and losartan was likely due to the inability of Ca2+-channel blocker to inhibit ROS production, because the amount of oxidized glutathione in SHR+amlodipine animals was higher than in control or SHR+losartan rats (17). These data indicate an important role of AT1R signaling in the regulation of mitochondrial ROS.
We have previously reported that the stimulation of endothelial cells with AngII significantly oxidized mitochondrial reduced glutathione (GSH), and the inhibition of NADPH oxidase with apocynin attenuated the loss of GSH, and prevented the stimulation of mitochondrial ROS (21). Furthermore, depletion of the NADPH subunit p22phox abolished the AngII-mediated increase in mitochondrial ROS (Fig. 3). It should be noted that the NADPH subunit p22phox and NADPH oxidase complex were not localized in mitochondria but in the endoplasmic membrane fraction. These data indicate a key role of NADPH oxidases in the AngII-mediated modulation of the mitochondrial redox status, which may be important in the stimulation of mitochondrial ROS. Indeed, Widder et al. have recently shown that the overexpression of a key regulator of mitochondrial redox status thioredoxin 2 blocks the AngII-induced production of mitochondrial ROS. Interestingly, the overexpression of thioredoxin 2 in mice significantly attenuated vascular
The role of mitochondrial
Diabetes and Metabolic Syndrome
AngII is involved in the development and pathological changes in diabetes and metabolic syndrome. Under these conditions, the involvement of mitochondria seems to be critical. It has been recently shown that the AT1R blockade protected kidney mitochondria in streptozotocin-induced type 1 diabetes (13). In streptozotocin-treated rats, mitochondrial H2O2 production rate was higher and uncoupling protein-2 content, cytochrome c oxidase activity, and renal glutathione level were lower than in streptozotocin+Losartan and control groups, indicating an important role of AT1R signaling in the diabetes-induced deterioration of mitochondria (13). The AT1R blockade protects kidney mitochondria and kidney structure in diabetes, independently of blood pressure and glycemia (Fig. 4).
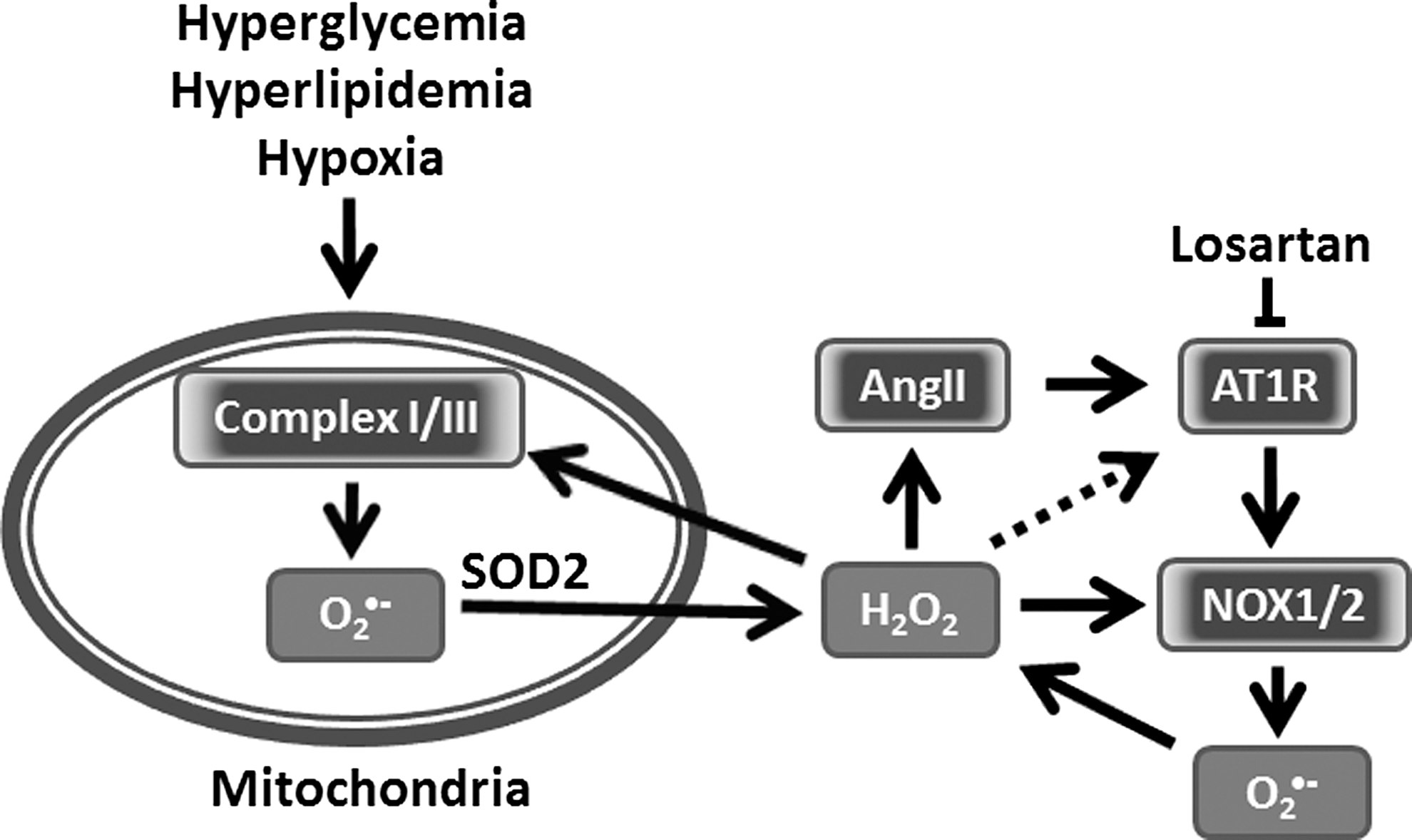
The role of the renin-angiotensin system (RAS) in the diabetes and metabolic syndrome was emphasized in a work by Chan's group (28). They showed that high glucose stimulates angiotensinogen gene expression via ROS generation in rat kidney proximal tubular cells (28). These data, however, do not provide clear mechanisms and primary sources of ROS. We suggest that diabetes and metabolic syndrome may initially cause an increase in mitochondrial ROS production, which stimulates AngII production and the expression of AT1R (Fig. 4). This, in turn, will stimulate ROS production by NADPH oxidases and enhance mitochondrial ROS. Therefore, mitochondrial ROS can be both an initiating factor and a target of ROS under these conditions.
The oxidative stress mediated by the hyperglycemia-induced generation of ROS significantly contributes to the development and progression of diabetes and related vascular complications (22). Many studies emphasized the role of mitochondrial dysfunction and mitochondrial ROS in diabetes (8). Brownlee suggested that the mitochondrial electron transport chain plays a key role in the hyperglycemia-induced overproduction of
Heart
AngII impacts heart functions and remodeling in many ways. As a result of the systematic negative action on vasoconstriction, thrombosis, and inflammation, AngII induces left ventricular hypertrophy, fibrosis, diastolic dysfunction, and heart failure. At the molecular level, AngII directly acts on cardiomyocytes and through signaling events, it modulates hypertrophy, cell survival/apoptosis, mitochondrial dysfunctions, and autophagy. In contrast to other tissues, in the heart, AngII may induce protective responses preventing injury. Both positive and negative actions of AngII in the heart are mediated by AT1R-initiated signaling with ROS as a crucial contributor to these signaling events. AngII induces ROS generation in the cytoplasm and mitochondria of cardiomyocytes. It has been shown that under ischemic conditions, the pharmacological inhibition of AT1R preserves the energy state of mitochondria, indicating the significance of AT1R signaling in the pathology of ischemia-induced heart damage, and links AT1R signaling and mitochondria functions under stress conditions.
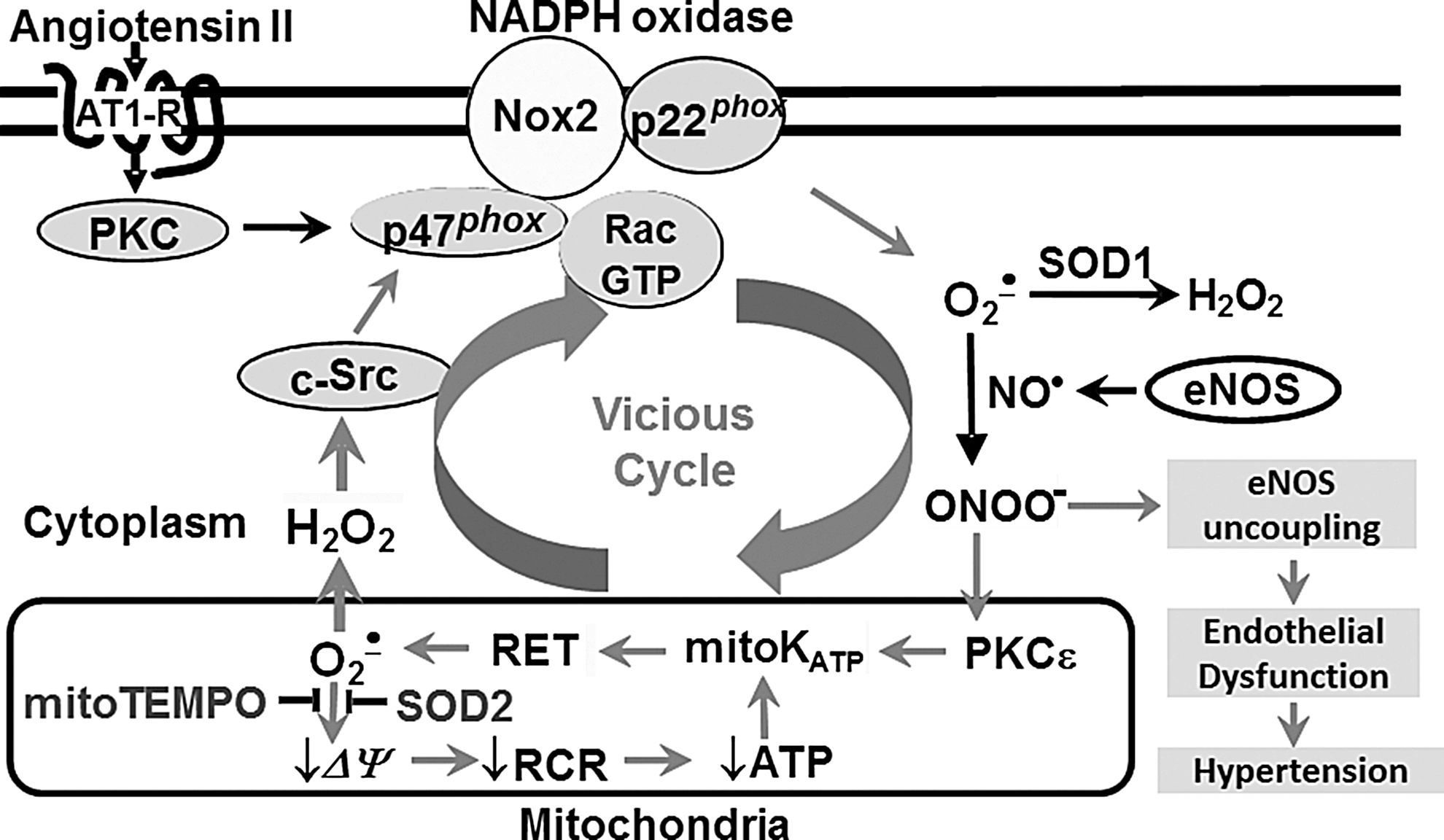
While excessive mitochondrial and/or cytoplasmic H2O2 triggers degenerative changes, moderate and controlled mitochondrial ROS induces an adaptive response which is known as a preconditioning that results in raising the heart's resistance to stress conditions, among others, through an increased expression of antioxidant proteins. In a similar fashion, moderate RAS activation by acute AngII stimulation leads to heart preconditioning through NADPH oxidase and mitochondria-dependent mechanisms (30). Prolonged exposure overwhelms the system and initiates destructive pathological changes. We and others have reported that AngII may utilize the same pathways as those activated on preconditioning (21). The role of the mitoKATP channel has been implicated in this adaptive response to moderate stress and other stress factors. Numerous studies have shown that acute stress leads to the opening of mitoKATP channels, which is prevented by NADPH oxidase inhibition, mitoKATP channel inhibitor 5-HD, or antioxidant treatment. The opening of mitoKATP releases mitochondrial ROS, which stimulates various signaling pathways, including those that are critical for survival and antioxidant protein expression, namely AMPK, p38AMPK, PI3 kinase, and Akt (46). Moreover, Akt activation facilitates NO• production by NOS and NO•-dependent signaling events. AngII is a powerful inducer of ROS and NO•; therefore, protective preconditioning actions of AngII might be, at least in part, mediated by ROS/NO•-dependent signaling events (Fig. 5). We have shown that moderate H2O2 activates an endothelial isoform of nitric oxide synthase (eNOS) that triggers an adaptive response (9). However, excessive H2O2 decreases tetrahydrobiopterin availability and uncouples eNOS and the neuronal isoform of nitric oxide synthase (nNOS) (56). When respiring, mitochondria continuously produce H2O2. The release of H2O2 can be potentially controlled by enzymatic systems such as thioredoxin reductase-2/thioredoxin 2 (57). The H2O2 released from mitochondria may increase the activity of cytoplasmic NADPH oxidases by c-Scr activation that is required for cytoplasmic NOX activity. NOX1, NOX2, and NOX4 have been shown to be expressed in the heart (Fig. 5); however, NOX2 is the most abundant isoforms, and NOX1 is barely detectable (27). It is conceivable that through similar pathways as those just described for heart preconditioning (3), NOX2 initiates a number of pathological conditions, such as AngII-induced hypertrophy (27), and is critical for key processes underlying the development of myocardial infarction, contractile dysfunction, and remodeling (39, 65). The fact that increased NOX2 expression and activity is observed in tissues of the dysfunctional heart indicates the NOX2 contribution to heart disease (32). In line with this evidence, the silencing of Rac, an NOX2 complex component, or NOX2 depletion abolishes both AngII-stimulated ROS generation and cellular hypertrophy in primary neonatal cardiomyocytes (27).
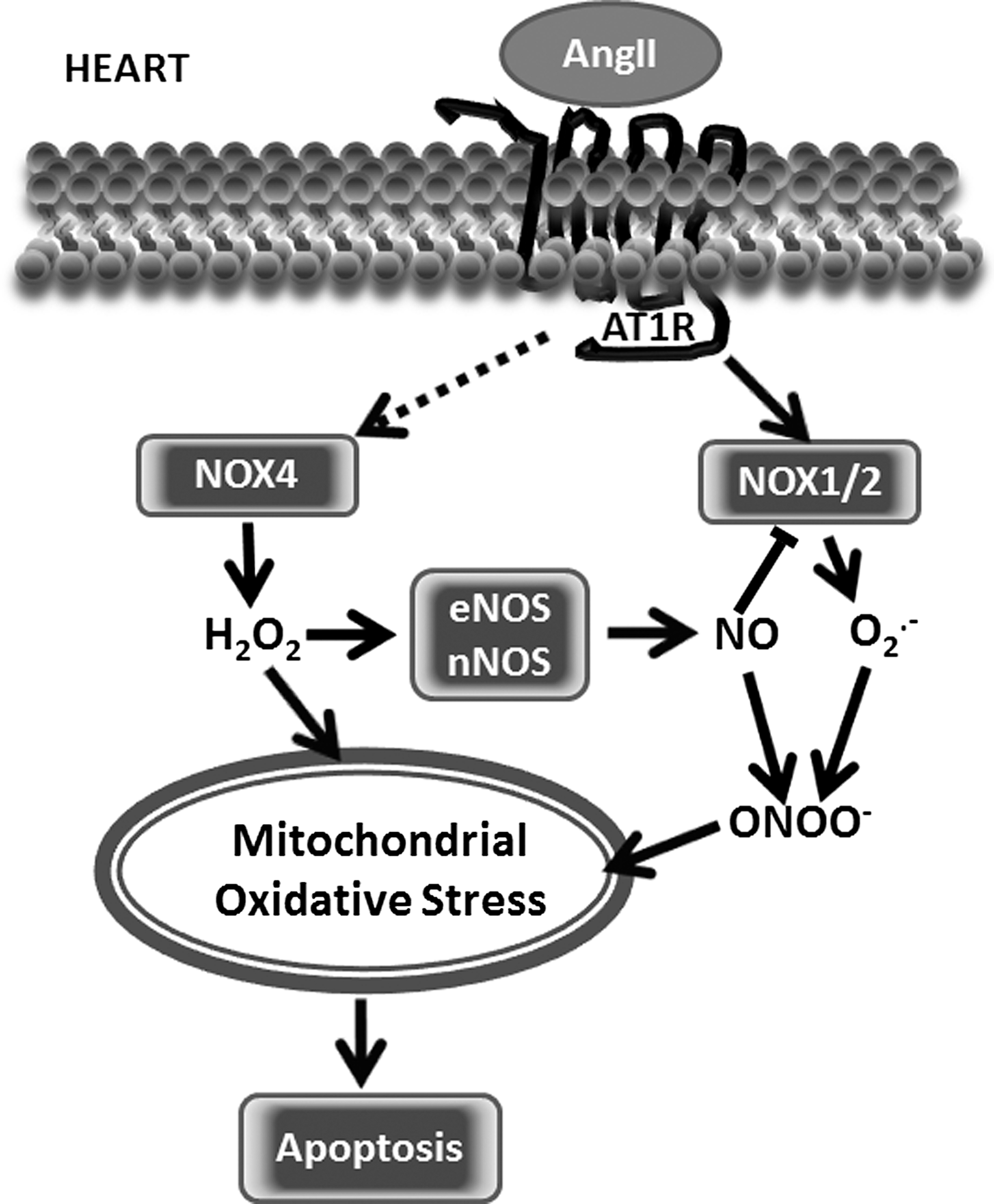
While the role of NOX2 seems to better described, NOX4 contribution to the heart functions, and its pathology is more complex and, in some cases, controversial. It has been previously reported that NOX4 generates H2O2, while NOX2 produces
In contrast to results showing the protective role of NOX4, Sadoshima group reported that NOX4 depletion improved the mitochondrial functions measured by reduced mitochondrial swelling, cytochrome c release, and decreases in both mitochondrial DNA and aconitase activity in response to pressure overload (1). It has been shown that cardiac-specific Nox4 knockout can attenuate cardiac hypertrophy, interstitial fibrosis, and apoptosis, and show better cardiac function when compared with wild-type mice (33). Due to contradicting results shown in literature and unanswered questions, the pathophysiological role of NOX4 in the heart remains unclear.
We suggest that an initial adaptive response mediated by NOX4 can be transformed to maladaptive response due to ROS overproduction. It is conceivable that the physiological role of NOX4 may include the redox regulation of eNOS activity, GSH synthesis, and mitochondria biogenesis. However, NOX4 overexpression and mislocalization may contribute to pathological processes.
Various approaches providing antioxidant defenses to mitochondria resulted in improved mitochondrial functions. Interestingly, mitochondria-targeted antioxidant prevents not only AngII-induced mitochondrial oxidative stress, cardiac hypertrophy, diastolic dysfunction, and fibrosis but also attenuated AngII-induced NOX4 up-regulation (11). AngII induces the pathological hypertrophic growth of cardiac tissue, leading to a significant increase in heart weight that is prevented by the administration of a mitochondria-targeted antioxidant (11). Similar protective effects were observed when mitochondria-targeted catalase was overexpressed in mice chronically infused with AngII (11). Constitutive autophagy in the heart is a homeostatic mechanism that contributes to the mechanisms maintaining cardiomyocytes size and cardiac tissue structure and functions. Significantly, autophagy alterations have been observed in a variety of heart diseases, including cardiac hypertrophy and heart failure. The upregulation of autophagy in pathological heart conditions is an adaptive response that protects cells from stress (45). Autophagy is regulated by ROS-sensitive mechanisms; therefore, mitochondrial ROS may regulate autophagy. Mice overexpressing catalase targeted to mitochondria challenged by AngII infusion are resistant to cardiac hypertrophy, fibrosis and mitochondrial damage, biogenesis, and autophagy induced by AngII (12).
Despite controversy around NADPH oxidase localization in the heart tissue, an analysis of literature indicates a close interrelationship between cytoplasmic and mitochondrial ROS and its role in heart pathological conditions and remodeling. Further studies are required to reveal the precise mechanisms and mediators of NADPH oxidases-mitochondria signaling.
Kidney
The pathophysiological actions of AngII on the kidney have a broad spectrum on different types of cells, including fibroblasts, endothelial cells, vascular smooth muscle cells, mesangial cells, tubular cells, and podocytes. AngII induced pathological changes of kidney morphology, and its functions are primarily associated with the loss of redox homeostasis. The NOX1, NOX2, NOX4, and NOX regulatory subunits are widely expressed in kidney tissue and have been considered key contributors to kidney fibrosis, loss of podocytes, or inflammation. The infusion of AngII to animals increases ROS production in kidneys and the overexpression of NOX isoforms (62). Increased NOX4 expression has been associated with proteinuria and hypertension in rats (47). Consistently with findings showing the critical role of ROS in the development of kidney disease, knockout NOX components prevents AngII-induced kidney damage (4). Significantly, a link between AT1R and kidney mitochondrial functions and mitochondrial ROS has been established. Several reports show that AngII induces the mitochondrial dysfunctions of kidney cells and/or mitochondria-dependent cell dysfunctions/cell death (58). The mitochondria of SHRs generate significantly higher levels of H2O2. The inhibition of AT1R prevents mitochondria dysfunction and morphological changes (16). Combination of a high salt diet and AngII infusion increases NOX2 expression and lowers SOD1 and SOD2 expression (31). It remains unclear whether mitochondria-targeted antioxidants are able to prevent AngII-induced kidney dysfunctions. However, studies with other cells and tissue showing AngII-induced mitochondrial dysfunction suggest a similar mechanism where NOX and mitochondria signal to each other to generate ROS (Figs. 1 and 5). Additional studies focusing on kidney dysfunction are required to test this hypothesis and show the potential physiological effects of mitochondria-targeted treatments.
Brain
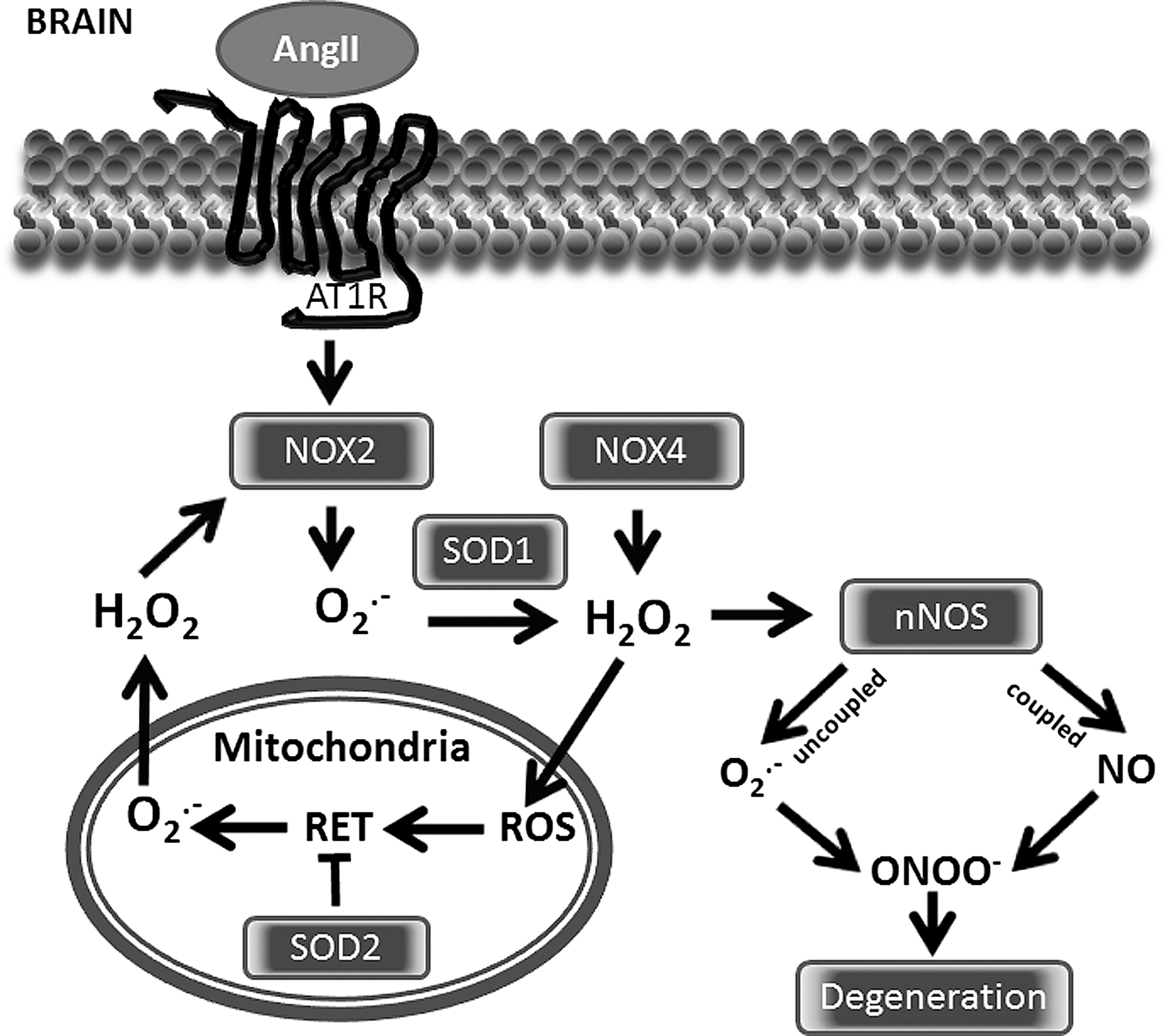
In the central nervous system, AngII triggers intra-neuronal signaling events that lead to neuronal activation (66). Signals of AngII detected by AT1R in neurons are communicated to brain regions, such as the subfornical organ (SFO) or paraventricular nucleus (PVN), in order to initiate sympathetic nervous system responses and restore body fluid and cardiovascular system homeostasis. In pathological conditions, this neuronal response becomes critical for the development of cardiovascular pathology, including hypertension or heart failure. ROS is a critical mediator of neuronal activation that not only facilitates physiological signaling events but also importantly orchestrates the development of disease.
AngII-related neuro-cardiovascular diseases are associated with excessive redox sensitive sympathoexcitation, which can be potentially counteracted by angiotensin-1-7 via an NO• pathway (66). Although AngII directly stimulates Nox1 and Nox2, it has been recently reported that Nox4 also contributes to redox signaling in the PVN, leading to sympathetic overactivation and a decline in cardiac function (29). In a number of pathological conditions such as SOD1 mutations, malignant gliomas and cerebral ischemia brain tissue can be overwhelmed with excessive
Aging
Aging is a complex and not fully understood process that leads to the progressive loss of tissues and organs without the capability to regenerate. In normal healthy humans, aging is associated with progressive endothelial dysfunction, remodeling of the small and large arteries, leading to arteriolosclerosis, kidney, and heart dysfunctions. Clinical factors, including hypertension, diabetes mellitus, and local and systemic inflammatory processes or tissue factors such as AngII, oxidative stress and mitochondrial dysfunction have been linked with aging-related deterioration. A clear connection between RAS and aging provides an opportunity for possible interventions that prevent some of the degenerative processes. The pharmacological inhibition of the AngII converting enzyme or AT1R prevents numerous age-related changes in animal studies (14). Furthermore, AT1R deficiency in mice promotes a longevity that is associated with decreased cardiac, vascular, renal, and pancreatic injury; reduced oxidative stress; and upregulation of the prosurvival gene sirtuin 3 (Sirt3) (4). These authors, in line with previous reports, have also shown in vitro that AngII decreases prosurvival and antioxidant enzyme expression. These changes are observed along with a decline of mitochondrial biogenesis, mitochondrial energy production, and its antioxidant defense mechanisms that result in apoptosis and senescence. The deleterious effects of AngII on mitochondrial function and biogenesis leading to degenerative changes in tissue can be prevented by the pretreatment with the AT1R blockers or mitochondria-targeted antioxidants. Mitochondrial ROS and mitochondria dysfunction initiated by AT1R-dependent cytoplasmic NADPH oxidases may represent a vicious cycle that may contribute to progressive cell and tissue degeneration. Since AT1R blockers have much more broad effects and prolonged treatment may not be the most efficient and targeted approach, targeting dysfunctional mitochondria may prove to be more therapeutically beneficial.
Conclusions
Hypertension is a common disease that affects one-third of adults in Western societies (10), and approximately 60% of the population is affected by cardiovascular conditions (54, 61). Oxidative stress is strongly implicated in the pathogenesis of these cardiovascular diseases (23). Mitochondria are one of the most important sources of ROS, and mitochondrial dysfunction is a prominent feature of most cardiovascular diseases (42, 49); however, the role of mitochondrial ROS is not completely understood.
Recently, it has been proposed that mitochondrial dysfunction along with endothelial dysfunction represents an important early step in the chain of events leading to atherosclerotic disease (49), and mitochondrial dysfunction in response to AngII could have direct ramifications for the development of endothelial dysfunction (21). Interestingly, angiotensin-converting enzyme inhibitors and AT1R blockers reduce age-related mitochondrial dysfunction, attenuate hypertension-induced renal mitochondrial dysfunction, and protect against cardiac mitochondrial dysfunction in the setting of acute ischemia (15, 17, 44). These findings suggest that AngII can alter mitochondrial function presumably by NADPH oxidases. Indeed, the inhibition of NADPH oxidases by apocynin and chelerythrine or the depletion of p22phox, an essential NADPH oxidase complex component, completely prevented mitochondrial dysfunction and attenuated mitochondrial ROS in response to AngII (21). On the other hand, consistent with the concept of NADPH oxidase-mitochondrial crosstalk (18), SOD2 overexpression and mitochondria-targeted SOD-mimetic, mitoTEMPO attenuated the AngII stimulation of NADPH oxidase and reduced hypertension (20). Taken together, these studies indicate that the interplay between mitochondrial and NADPH oxidase-derived
During the past decade, it has become apparent that crosstalk between mitochondria and NADPH oxidases plays a critical role in the genesis of many cardiovascular diseases (18). Since mitochondria are both a target and source of ROS, they play an important role in ROS-induced ROS production. Interestingly, the scavenging of mitochondrial ROS-attenuated responses to AngII in the brain, kidney, and endothelial cells. These data indicate that the stimulation of mitochondrial ROS by AngII is an important amplification of redox signaling, which can be important for normal physiological functions. However, diminished SOD2 expression (20), decreased redox mitochondrial status (63), or metabolic syndrome may result in the uncontrolled amplification of AngII signaling, leading to a feed-forward viscous cycle of ROS production by mitochondria and NADPH oxidases that can be pharmacologically targeted by AT1R blockers or mitochondria-targeted antioxidants. The use of antioxidant strategies specifically targeting mitochondria (11, 20) is a new promising approach for the treatment of many pathological conditions, including aging, atherosclerosis, diabetes, hypertension, and degenerative neurological disorders in which mitochondrial oxidative stress seems to play a critical role. Additional studies conducted on the AngII-mediated production of mitochondrial ROS are required to reveal the detailed mechanisms and specific mediators that could serve as novel targets for pharmacological treatments.
Footnotes
Acknowledgment
This work was supported by funding from the National Institute of Health grant HL094469.