
Abstract
Significance:
Several aging-related pathophysiological mechanisms have been described to contribute to increased thrombotic risk in the elderly, including oxidative stress, endothelial dysfunction, and platelet and coagulation cascade activation. Antithrombotic treatment in the elderly should be individualized.
Recent Advances:
Recent studies have clarified some pathophysiological mechanisms of enhanced oxidative stress and thrombotic alterations in older adults. In the last decade, randomized trials have evaluated different antithrombotic strategies to reduce the risk of cardiovascular events in these patients.
Critical Issues:
The proportion of elderly patients included in clinical trials is generally low, thus not reflecting the daily clinical practice. There is no consensus on the most appropriate antithrombotic treatment in the elderly, also considering that bleeding risk management may be challenging in this high-risk subgroup of patients. Routine antiplatelet treatment is not a valid strategy for the primary prevention of cardiovascular events given the associated high risk of bleeding. In elderly patients with acute coronary syndrome, low-dose prasugrel or clopidogrel, shorter dual antiplatelet therapy, and no pretreatment before stent placement should be considered. Advanced age should not be the only reason for the underuse of oral anticoagulation in patients with atrial fibrillation, with direct oral anticoagulants preferred over warfarin for stroke prevention. Instead, a case-by-case clinical evaluation is warranted based on patient's bleeding risk also.
Future Directions:
There is a need for a structured tailored approach to manage thrombotic risk in elderly patients. The choice of the most appropriate antithrombotic treatment should balance efficacy and safety to reduce the risk of bleeding.
Introduction
Globally, the population is aging and the World Health Organization predicts that by 2050, the population of individuals aged ≥60 years will double and those aged ≥80 years will be around 400 million (Singh and Bajorek, 2014). Despite aging being commonly measured by chronological age and, as a convention, a person aged ≥65 years is usually defined as ‘elderly,’ differences in genetics, lifestyle, and overall health have to be taken into account, mainly regarding the response to a specific treatment (Singh and Bajorek, 2014).
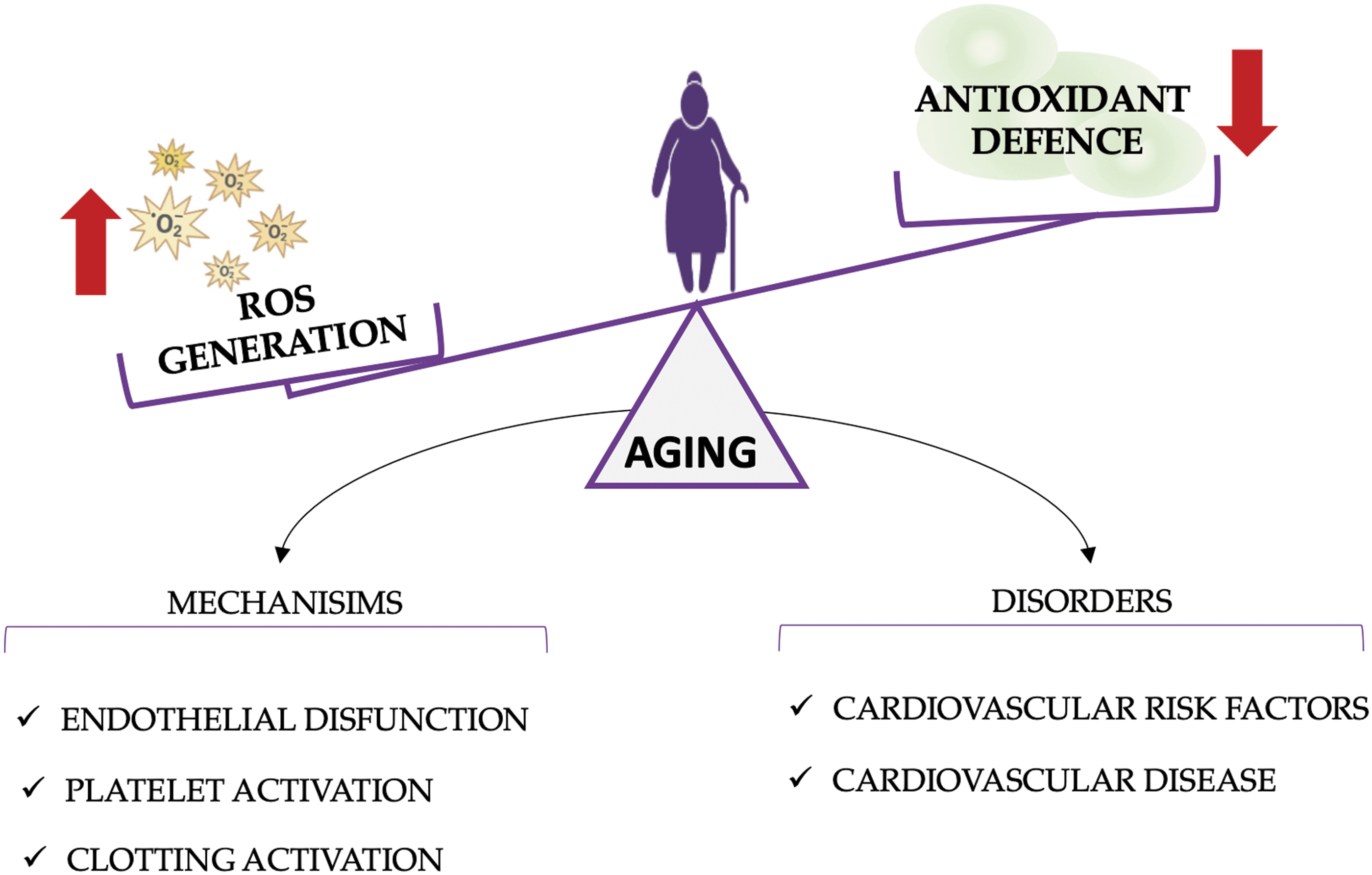
Several physiological mechanisms of vascular biology as well as thrombotic and hemostatic balance change during aging and are responsible for an increased risk of both thrombotic and hemorrhagic complications (Violi et al., 2017). The overproduction of reactive oxygen species (ROS) and downregulation of antioxidant enzymes during aging result in a pathologic imbalance that may affect clotting and platelet activation and impair endothelial function, further predisposing elderly patients to thrombosis (Violi et al., 2017).
From a clinical point of view, older individuals show higher odds of developing cardiovascular disease, and the prevalence of cardiovascular risk factors (i.e., arterial hypertension, diabetes mellitus, and dyslipidemia) was higher in individuals of advanced age, contributing to the aging-related cardiovascular burden (Violi et al., 2017) (Fig. 1). On the other hand, aging is often associated with inappropriate or reduced dosage and duration of antithrombotic therapy as elderly individuals may be considered at higher risk of drug toxicity or side effects and bleeding events than younger ones.
Inappropriate low dosage of anticoagulants is indeed frequent in elderly patients and shorter treatment duration has been suggested in specific situations, mainly focusing on the safety profile (Lee et al., 2018; Moudallel et al., 2018). Finally, elderly patients may also be downrepresented in clinical trials and clinical decisions on this population are hampered by the lack of data.
The aims of this comprehensive review are to assess the pathogenetic mechanisms of aging-related atherothrombosis and to report available data on antithrombotic therapy during aging.
Pathogenetic Mechanisms Linking Aging with Atherothrombosis
Oxidative stress theory
Oxidative stress is the result of an imbalance between production and removal of ROS (Salisbury and Bronas, 2015; Violi et al., 2017). Even if the underlying mechanisms remain only partly understood, overproduction of ROS plays an important role in the aging-related cardiovascular burden, interacting with endothelial vascular cell homeostasis and functionality, platelet activation, and coagulation factor dysregulation (Liguori et al., 2018; Salisbury and Bronas, 2015; Violi et al., 2017).
The radical superoxide anion (O2 •), hydrogen peroxide (H2O2), hydroxyl ion (OH•), and hypochlorous acid are major endogenous ROS and their production is mainly mediated by the nicotinamide adenine dinucleotide phosphate oxidase (Nox), myeloperoxidase (MPO), lipoxygenase, and angiotensin II activity (Genestra, 2007; Violi et al., 2017).
Results of several experimental models have shown that the activity of some Nox isoforms (e.g., Nox4) as well as serum levels of myeloperoxidase (MPO) increased with age and that their inhibition through specific molecules may limit endothelial structural and functional dysfunction in vascular inflammation, reduce atherosclerotic mechanisms (e.g., endothelial activation, platelet adhesion and macrophage recruitment, and angiogenic mediator production), and promote atherosclerotic plaque stabilization (Fig. 1) (Azumi et al., 1999; Chen et al., 2022; Cheng et al., 2019; Douglas et al., 2012; Guzik et al., 2006; Hoy et al., 2001; Liu et al., 2013; Lozhkin et al., 2017; Ndrepepa, 2019; Quesada et al., 2015; Roth Flach et al., 2019; Scharnagl et al., 2014; Turgeon et al., 2012; Vendrov et al., 2015).
Low-density lipoprotein (LDL) retention and accumulation within the vessel wall (through neuraminidase-related desialylation) and oxidation (through lipoxygenase and MPO) are further critical steps in the oxidative stress-related atherogenic process of aging (Aureli et al., 2011; Demina et al., 2021; Dobrian et al., 2011; Funk et al., 2002; Iuliano et al., 2000; Mezentsev et al., 2021; Poznyak et al., 2020; Violi et al., 2017).
Damage in the vessel wall due to chronic accumulation and oxidation of LDL causes the migration of inflammatory cells (e.g., monocytes and macrophages) and formation of oxidative stress-related products (e.g., isoprostane and thromboxane production, expression of adhesion molecules) that exacerbate atherosclerotic lesions up to their erosion and rupture (Fogelstrand and Boren, 2012; Tabas, 2017; Violi et al., 2017). Dysregulation in tissue repair, clearance of inflammatory cells and necrotic materials, and vascular regeneration of aging further contribute to atherogenesis (Goldschmidt-Clermont et al., 2005; Karra et al., 2005; Tesauro et al., 2017) (Fig. 2).
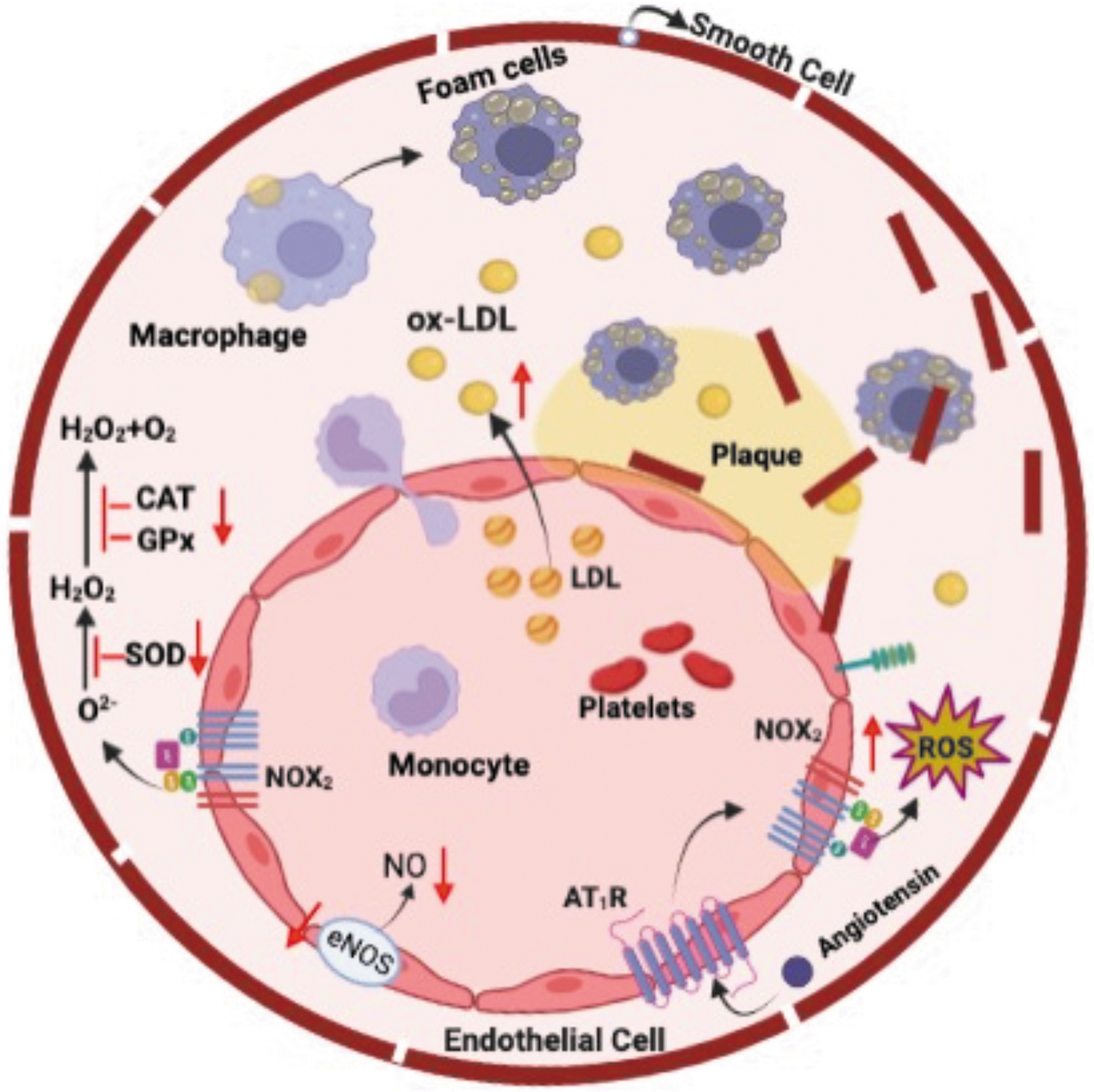
Along with increased systemic oxidative damage, aging seems to modulate the effects of both enzymatic (e.g., nitric oxide synthase [NOS], superoxide dismutase [SOD], glutathione peroxidase [GP]) and nonenzymatic (e.g., glutathione, α-tocopherol, ascorbic acid, and β-carotene) antioxidant pathways (Liguori et al., 2018; Violi et al., 2017).
The serum activity of some SOD and GP isoforms, indeed, appeared to be reduced in older people, hampering their role in cell growth, leukocyte adhesion, and platelet aggregation inhibition (Fig. 1) (Pastori et al., 2016a; Rizvi et al., 2021; Sonkar et al., 2023). Similarly, the reduced levels of NOS identified in elderly patients may lead to impaired endothelium-dependent dilation through reduced bioavailability of nitric oxide (NO) (Kilic et al., 2015; Tesauro et al., 2017) (Fig. 2).
Even if studies with animal models have reported a relevant role and a positive effect of antioxidants in atherothrombosis, an interventional trial on antioxidant supplementation (e.g., vitamin C and vitamin E) provided inconclusive results and the heterogeneity of data did not allow any sound conclusions (Morelli et al., 2020; Violi et al., 2022).
The serum and urinary levels of some of the abovementioned molecules involved in aging-related oxidative stress are reported in Table 1.
Levels of Some Molecules Involved in Aging-Related Oxidative Stress from Available Human Studies
MPO, myeloperoxidase; NOS, nitric oxide synthase; Nox, nicotinamide adenine dinucleotide phosphate oxidase; ox-LDL, oxidized low-density lipoprotein; PCI, percutaneous coronary intervention.
Other mechanisms involved in aging-related atherothrombosis
Considering that the integrity of the endothelium and maintenance of its functionality are essential to prevent atherogenesis, mechanisms other than oxidative stress may interfere with the vascular physiology and may enhance atherothrombosis (Bockus and Kim, 2022; Donato et al., 2018; Ungvari et al., 2018b).
Blood flow continuously generates mechanical forces on the vessel wall (radial, circumferential, and longitudinal forces) and on the endothelial surface (shear stress), alteration of which may lead to atherosclerotic plaque development (Kwak et al., 2014; Tesauro et al., 2017). For example, it has been demonstrated that high shear stress maintains the physiological properties of the endothelium and that aging-related reduction in shear stress is an independent predictor of atherogenesis (Carallo et al., 2016; Kwak et al., 2014; Zhang et al., 2017).
Aging is also associated with increase in luminal enlargement and wall stiffness, which are probably dependent on enhanced deposition of collagen fibrils, accelerated degradation of elastin, and calcification (Fig. 1) (Donato et al., 2018; Lakatta and Levy, 2003; Najjar et al., 2005).
In this setting, the intima–media thickness that represents a strong surrogate marker of arterial structural changes appeared to progressively increase with age even in populations at low risk of atherosclerosis and appeared to be strongly associated with future cardiovascular events (Li et al., 2003; Lorenz et al., 2007; Virmani et al., 1991). Similarly, pulse wave velocity that measures the velocity of pulse propagation through the arteries is considered a noninvasive index of vascular stiffness and appeared to increase during aging (Huveneers et al., 2015; Liao et al., 1999).
Several studies have shown that chronic, sterile low-grade inflammation characterizes aging, promoting arterial dysfunction and atherothrombosis (Kong et al., 2022; Ungvari et al., 2018a; Wolf and Ley, 2019). Atherosclerotic lesions are sites of immune inflammation in which several types of inflammatory cells (e.g., macrophage, T, dendritic, natural killer, and innate lymphoid cells) are present (Nilsson and Hansson, 2020).
However, LDL accumulation and oxidation within the vessel wall seemed to represent the main trigger for the proinflammatory response (e.g., cytokine production, in situ macrophage proliferation), while the release of other antigens by apoptotic cells seemed to maintain the atherogenic process (Miller et al., 2011; van der Valk et al., 2016).
Recent experimental studies have suggested that gut dysbiosis, possibly through the proatherogenic molecule lipopolysaccharide, may favor arterial inflammation and atherothrombosis (Violi et al., 2023). A pathogenetic gut microbiota, indeed, is more common in patients with symptomatic atherosclerotic lesions (Violi et al., 2023).
Platelet and coagulation cascade activation
Platelets play a relevant role in aging-related atherothrombosis (Montenont et al., 2019). However, several studies have shown that the platelet count may drop approximately by 10% after 70 years of age probably due to a reduction in the hematopoietic stem cell reserve or a shift in the hematopoietic stem cell population toward a megakaryocytic bias (Biino et al., 2013; Montenont et al., 2019; Rossi et al., 2007; Rundberg Nilsson et al., 2016; Segal and Moliterno, 2006; Troussard et al., 2014; Vazquez-Santiago et al., 2016).
The platelet-related increased thrombotic risk of aging, conversely, appeared to be associated with enhanced platelet activity, in which the response to common agonists (e.g., adenosine diphosphate) is higher than in a younger population (Mohebali et al., 2014; Sverdlov et al., 2014). Furthermore, the serum levels of platelet-mediated cytokines (e.g., β-thromboglobulin and platelet factor 4) and metabolites (e.g., thromboxane products) appeared to be higher in patients at risk or with overt atherosclerosis, as well as in older ones (Bastyr et al., 1990; Eikelboom et al., 2008; Pastori et al., 2016b; Reilly and FitzGerald, 1986; Zahavi et al., 1980).
Shorter bleeding time in older compared with younger patients confirms these data even if it should be acknowledged that this test represents both platelet activation and vascular reactivity in vivo (Franchini, 2006; Jorgensen et al., 1980) (Fig. 3).

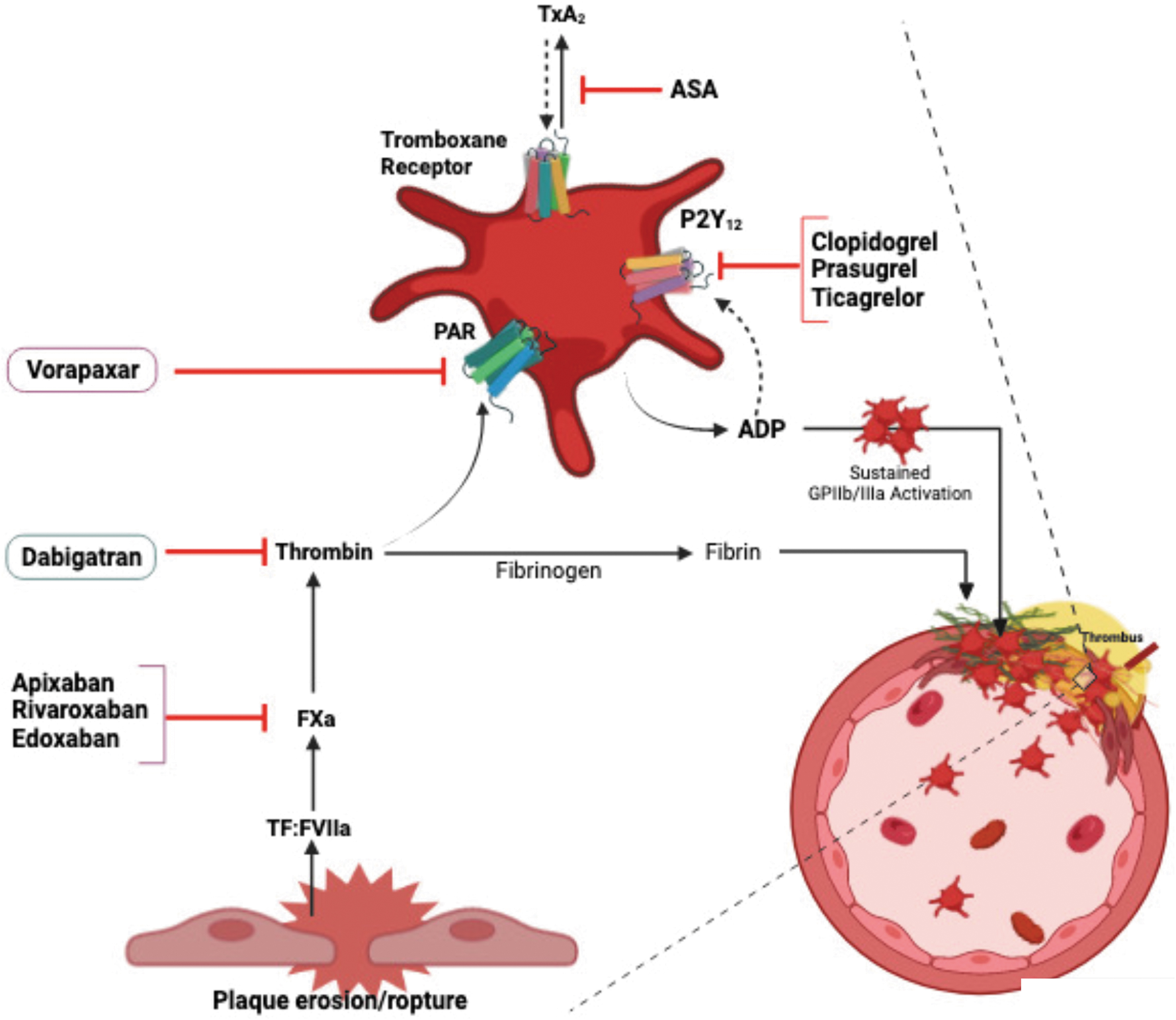
Growing evidence supports the role of the coagulation cascade in the atherothrombotic process. Rupture of atherosclerotic plaque is a major cause of coagulation cascade activation through exposition of tissue factor (TF) (Olie et al., 2018; Palmerini et al., 2013). Furthermore, coagulation activation and generation of thrombin not only promote fibrin production and platelet activation but also seem to be involved in atherogenesis, mainly through protease-activated receptor activation (Olie et al., 2018).
Aging may exacerbate these mechanisms as it is associated with increased concentration of some coagulation factors (e.g., factor V, factor VII, factor VIII, factor IX, and fibrinogen), reduction of natural anticoagulants (e.g., antithrombin III, proteins C and S, TF pathway inhibitor), and alterations in the fibrinolytic system activity (Franchini, 2006; Sakkinen et al., 1999) (Fig. 3).
Cardiovascular Risk Management in Elderly Patients
Elderly patients constitute the majority of patients encountered in clinical practice. These patients represent a high-risk subgroup of patients given their high cardiovascular burden and mortality rate. Cardiovascular disease still represents the main cause of death in elderly patients, accounting for ∼40% of all deaths (Fleg et al., 2011).
This increased cardiovascular risk observed in the elderly is likely the result of long-term exposure to some specific risk factors (i.e., raised cholesterol levels, smoking) and the consequence of accumulating comorbidities such as heart failure, hypertension, diabetes, and atrial fibrillation (AF). The latter is particularly important in elderly patients as its incidence rises sharply with age (Roth et al., 2020).
Cardiovascular risk stratification in older people should take into account some specific age-related factors such as life expectancy, quality of life, frailty, comorbidities, polypharmacy (with related drug–drug interactions and side effects), and competing (noncardiovascular) risks (Lettino et al., 2022).
In 2021, the SCORE2-OP tool was proposed to calculate the 5- and 10-year risks of fatal and nonfatal cardiovascular disease events (myocardial infarction and stroke) in adults older than 70 years.
Some previous studies, however, showed some differences in the prognostic role and management of cardiovascular risk factors according to age. As such, the therapeutic target for elderly patients may be different compared with younger ones.
For instance, the systolic blood pressure target for the elderly is set at <140, but not <130 mmHg (Williams et al., 2018). Elderly patients may be at higher risk of drug-induced hypotension with consequent risk of syncope and falls (Rutan et al., 1992), translating into worse quality of life and higher mortality risk (Wiersinga et al., 2022).
Regarding dyslipidemia, administration of statin therapy is recommended to prevent cardiovascular disease, but its benefit seems to be mitigated in elderly patients without evidence of occlusive disease (Cholesterol Treatment Trialists, 2019). A large study on 208,673 Korean participants without cardiovascular disease at baseline and aged ≥60 years found no predictive value for total cholesterol against mortality and cardiovascular events (Yang et al., 2021). However, recent data coming from stroke patients have shown that lack of statin therapy is associated with greater risk of cardiovascular events also in elderly patients (Lefeber et al., 2021).
In addition, for blood glucose control, recommendations from international societies differ between older and younger patients. In elderly patients, glycemic targets and drug regimens need to be adjusted to minimize the risk of hypoglycemic events that are associated with an increased mortality rate. In this context, it may be necessary to simplify complex therapeutic regimens for some patients.
The 2022 American Diabetes Association guidelines recommend a therapeutic goal according to the general health status of patients. Indeed, in healthy patients, a target of glycated hemoglobin (HbA1c) may be maintained, while a value <8% for older patients with complex medical issues is indicated (American Diabetes Association Professional Practice, 2022).
In more complex patients with limited life expectancy, HbA1c should not be considered for drug monitoring, but rather a blood glucose level of 100–200 mg/dL may be satisfactory with monitoring to avoid hypoglycemia (American Diabetes Association Professional Practice, 2022).
Elderly Patients in Cardiovascular Clinical Trials
Despite aging being considered a major risk factor for the incidence of different cardiovascular diseases (Violi et al., 2017), the proportion of elderly patients in major cardiovascular clinical trials performed in the last decade (testing antithrombotic strategies) is generally limited (Rodriguez and Harrington, 2021) (Table 2). These trials tested antiplatelet and anticoagulant drugs alone or in combination for reducing cardiovascular events. These drugs act synergistically by impairing platelet function and inhibiting clotting activation (Fig. 4).
Proportion of Elderly Patients and Outcomes in Representative Major Cardiovascular Trials in the Last Decade, 2012–2022
ACS, acute coronary syndrome; AF, atrial fibrillation; CAD, coronary artery disease; DAPT, dual antiplatelet therapy; HR, hazard ratio; MACE, major adverse cardiovascular events; MI, myocardial infarction; STEMI, ST-segment elevation myocardial infarction.
However, the benefit of combination therapy should be balanced against the increased risk of bleeding with this therapeutic approach, which may be particularly challenging in elderly patients. Thus, although antithrombotic therapy has been proven to provide a clear net clinical benefit in elderly patients with established cardiovascular disease, data from studies on primary prevention of cardiovascular events are controversial.
Primary prevention of cardiovascular events
The ASPREE trial randomized healthy elderly subjects to receive either aspirin (9525 subjects) or placebo (9589 subjects). The trial found an increased overall mortality rate in subjects on aspirin than controls, mainly due to cancer-related deaths. This result was evident in the subgroup of elderly subjects (Table 2). An analysis of the same trial showed no difference in the rate of major adverse cardiovascular events, but an increased risk of major bleeding (Table 2).
The ARRIVE trial randomized patients at moderate cardiovascular risk to receive either placebo or aspirin for prevention of a first vascular event. The aspirin treatment was not superior to placebo in the elderly patients (Table 2), but in the safety analysis, the risk of gastrointestinal bleeding was doubled in the group of patients treated with aspirin compared with placebo (HR 2.11, 95% CI: 1.36–3.28; p = 0.0007). No data on the subgroup of elderly patients were provided.
In the ASCEND trial, 15,480 patients with diabetes and no cardiovascular disease at baseline were randomized to receive either placebo or aspirin. In the overall population, aspirin lowered the risk of cardiovascular events, but increased the risk of bleeding (rate ratio 0.88; 95% CI: 0.79–0.97; p = 0.01; and 1.29; 95% CI: 1.09–1.52; p = 0.003). In the subgroup of elderly patients, the effect on cardiovascular events was not statistically significant (Table 2).
Altogether, these data do not indicate a clear benefit of routine antithrombotic treatment in elderly patients for primary prevention of cardiovascular events.
Acute coronary syndrome/coronary artery disease
In clinical trial on patients with acute coronary syndrome (ACS) testing different antiplatelet drugs or different lengths of combination therapy, the proportion of patients aged 75 years or older was generally low (Table 2).
In 2014, the dual antiplatelet therapy (DAPT) trial found no significant reduction in cardiovascular events in the subgroup of elderly patients assigned to prolonged DAPT with thienopyridines. The more recent TICO study (2020) found a reduction in bleeding events with ticagrelor monotherapy compared with ticagrelor plus aspirin after 3 months of DAPT in the subgroup of patients aged 65 years or older (Table 2).
Two studies, ATLANTIC and ACCOAST, evaluated pretreatment with ticagrelor and prasugrel in patients with ACS. No difference in reduction of ischemic endpoints was found in the group of elderly patients, but excess bleeding was found for prasugrel in non-ST-elevation myocardial infarction ACS (Table 2).
In general, studies comparing different antiplatelet drugs did not reveal a clear advantage in using any of them in terms of bleeding prevention or cardiovascular event reduction.
Based on this, the European Society of Cardiology Working Group on Thrombosis recommends that patients (aged ≥75 years) treated with percutaneous coronary intervention (PCI) for ACS should be given reduced doses of prasugrel (i.e., 5 mg daily) or clopidogrel. In addition, DAPT should be limited to 12 months and be reduced depending on the bleeding risk (Andreotti et al., 2023).
Furthermore, pretreatment with P2Y12 inhibitors (unless in cases of ST-elevation myocardial infarction) could be avoided, and the use of single antiplatelet therapy (e.g., aspirin, clopidogrel, ticagrelor) after 1–3 months of DAPT should be considered to reduce bleeding risk (Andreotti et al., 2023).
Stroke prevention in patients without AF
In the last decade, three major trials tested antiplatelet and anticoagulant drugs in patients with stroke (Table 2). The SOCRATES study randomized patients with acute non-severe ischemic stroke or high-risk transient ischemic attack to receive either high-potency ticagrelor or aspirin treatment. In the subgroup of elderly patients, the two antiplatelet regimens were similar regarding the risk of occurrence of stroke, myocardial infarction, or death (Table 2).
Two trials tested the anticoagulant therapy with direct oral anticoagulants (DOACs) for secondary prevention after embolic stroke of undetermined source. In the RE-SPECT ESUS trial, dabigatran was not superior to aspirin in the overall analysis in terms of recurrent stroke risk. However, the subgroup analysis of the elderly showed a favorable effect of dabigatran, with reduction in recurrent stroke and a similar bleeding risk (Table 2).
In the NAVIGATE ESUS trial, rivaroxaban was compared with aspirin in patients with embolic stroke of undetermined source. The study found that rivaroxaban was not superior to aspirin for stroke prevention in the overall analysis and also in the subgroup of elderly patients. The risk of bleeding was increased in the whole cohort, but no data on the subgroup of the elderly were reported (Table 2).
Anticoagulant therapy in elderly patients with AF
Anticoagulant therapy is generally underused in elderly patients with AF, especially in very old ones or in those with previous stroke or major bleeding (Munir et al., 2023). Several studies have consistently demonstrated a net clinical benefit of DOACs compared with vitamin K antagonists (VKAs) in elderly patients (Shah et al., 2019), with apixaban being associated with a lower risk of major bleeding in elderly patients with AF (Rutherford et al., 2022). A more challenging clinical scenario is represented by patients with AF experiencing ACS undergoing PCI, for whom combination therapy with anticoagulant and antiplatelet drugs is needed.
Two studies tested the safety and efficacy of rivaroxaban in patients with AF and coronary artery disease (CAD). In the subgroup of patients aged ≥75 years included in the AFIRE trial, rivaroxaban reduced ischemic events with a similar bleeding risk (Table 2).
In the PIONEER-AF trial, patients with AF undergoing PCI were randomized to receive either VKAs plus DAPT or rivaroxaban (15 mg once daily) plus a P2Y12 inhibitor. The study found a similar risk of ischemic events with lower bleeding risk in the group of elderly patients receiving rivaroxaban (Table 2).
In addition, using dabigatran in the REDUAL-PCI trial and apixaban in the AUGUSTUS trial, a subgroup analysis on elderly patients reported similar bleeding and ischemic risks between DOACs and VKAs (Table 2).
Conclusions
Several pathophysiological mechanisms contribute to the age-related thrombotic risk, including oxidative stress, endothelial dysfunction, low-grade inflammation, and platelet activation. Routine antiplatelet treatment should not be prescribed for primary prevention of cardiovascular events.
In older patients with ACS/CAD and without AF, strategies to reduce bleeding risk may include the use of low-dose prasugrel or clopidogrel, reduction in the length of DAPT, and no pretreatment before PCI. In elderly patients with embolic stroke of undetermined source, dabigatran was associated with lower risk of recurrent stroke.
Advanced age should not be a reason for the underuse of oral anticoagulation in patients with AF, and DOACs are generally preferred over VKAs, also in patients undergoing PCI, in whom dual antithrombotic therapy with rivaroxaban reduced bleeding risk in the subgroup of elderly patients.
In conclusion, older adults are underrepresented in cardiovascular clinical trials, and antithrombotic therapy in elderly patients should be tailored to balance ischemic and bleeding risk.
Footnotes
Authors' Contributions
E.V., P.P., and D.P. were involved in conceptualization (lead), writing—original draft (lead), and writing—review and editing (lead); and S.B. was involved in writing—original draft (supporting), and writing—review and editing (lead).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.