
Abstract
Background:
Autism research has relatively neglected restricted repetitive behaviors (RRB) and autistic adults compared with the social domain of autism and autistic children. With this review, we aimed to synthesize what is currently known about autistic adult’s self-reported RRB, researcher’s use of methods, and consideration of masking and gender, and to highlight gaps in our knowledge to inform future research.
Methods:
We conducted a systematic search of five databases that we last ran in February 2023. We included studies where autistic adults self-reported on one or more subtypes of their repetitive behaviors. We conducted a narrative synthesis to summarize results. We used the Mixed Methods Appraisal Tool to assess the quality of included studies.
Results:
Our database search identified 35 studies to include for review. The majority of included studies focused on the sensory domain of RRB with other subtypes comparatively neglected. The narrative synthesis identified subject areas of stimuli characteristics, internal reactions, moderators, recovery, self-regulation, and social pressure. We uncovered a narrative where most autistic adults experience hypersensitivity to some sensory stimuli, the unpleasantness of which they then try to avoid, but in doing so may also avoid social situations, contributing to loneliness and increased anxiety surrounding social situations. We identified a cycle of stress where existing stress increased sensory sensitivities leading to more stress and less ability to deal with additional stressors. While the self-regulatory benefits on emotion, cognition, and self-fulfillment of RRB should help with stress, this was prevented by autistic people’s awareness of stigma surrounding these behaviors, leading to masking, which is also stressful.
Conclusion:
The review highlighted the need for a less categorical and more interrelated approach in researching this domain of autism and a need for more awareness surrounding sensory issues and the benefits of RRB. Future research should also strive to improve study sample representation, particularly regarding gender, race, and IQ.
Community Brief
Why is this an important topic?
Historically, research has focused on autistic children and social differences rather than on autistic adults and their repetitive behaviors such as repetitive movements, insisting on sameness, sensory sensitivities, and special or preferred interests. Research has often asked parents and carers about these behaviors rather than asking autistic adults. As such autistic adults’ own experiences of their repetitive behaviors are not well known in research.
What was the purpose of this review?
The purpose of this review was to find out:
Which repetitive behaviors have already been studied in self-reporting autistic adults. How self-reporting autistic adults’ repetitive behaviors have been studied. What the findings of those studies were and to summarize them. If masking (the “hiding” of autistic behaviors) and gender differences have been considered in these studies.
What did the researchers do?
We conducted a systematic review looking at papers where autistic adults self-reported/participated in studies exploring one or more repetitive behaviors. A systematic review searches and summarizes all existing research on a topic to answer specific questions and make clear what we already know about a topic and what still needs to be researched. Our search ran until February 2023 and found 35 papers.
What were the results of the review?
We found that sensory sensitivities are researched more than other repetitive behaviors, followed by special interests. We also found that autistic adults’ repetitive behaviors are self-fulfilling and help them manage their emotions and attention. This helps them to cope with things that might cause stress, such as sensory sensitivities. Autistic people said that they had strong internal reactions to sensory stimuli, especially those such as loud or high-pitched noises, bright lights, scratchy textures, and strong smells. This was made worse where multiple of these things were present; multiple stimuli overlapped, they couldn’t control the sensory stimuli, were already stressed, and because of past or present negative reactions of others. Repetitive behaviors are often viewed negatively or stigmatized by others, and so many autistic adults mask or hide these behaviors. This may cause problems for autistic people—although very little research has looked into this. Gender differences were also not considered often. There was no gender difference in the amount or intensity of repetitive behaviors; females seemed to have increased sensitivity to taste and smell and had different special interests to males.
What are the next steps?
Future research should consider repetitive behaviors as a whole and how they relate to one another. Researchers should recruit participants to better represent autistic adults of all backgrounds, particularly regarding gender, race, and IQ, as current findings are fairly limited to white autistic adults of average or above average intelligence within the gender binary.
What are the potential weaknesses of the review?
The review looks at self-reporting autistic people; this means that the review does not look at autistic people who cannot self-report, and so the findings may not apply to them. It is also possible that we missed potentially relevant studies in our search, although every effort was made to avoid doing so. Some studies had to be excluded because results were reported in a way that did not separate the experiences of autistic adults from other groups such as children or adults with attention-deficit hyperactivity disorder (ADHD) who were not autistic. This increases the review’s relevancy to autistic adults but means that some potentially relevant findings were not reported.
How will these findings help autistic adults now or in the future?
The findings in this review help to highlight the areas of restricted repetitive behavior (RRB) research that are lacking, particularly regarding insistence on sameness behaviors and repetitive movements. This will hopefully prompt more research in these areas and increase understanding of these misunderstood behaviors. The findings also highlighted the experience of sensory sensitivities and the benefits of other forms of RRB, which challenges the stigma surrounding these behaviors and increases awareness.
Keywords
Background
Autism is a neurodivergence characterized by differences in social communication and interaction, and a pattern of restricted repetitive behaviors (RRBs), activities, and interests across the life span.1,2 Research into autism has historically focused on biomedical etiology and perceived issues in the social domain,3–5 relatively neglecting RRB. The broad range of behavioral phenomena that RRBs, activities, and interests encompasses (repetitive movements [aka stimming], insistence on sameness, circumscribed or preferred interests, and sensory sensitivities [APA, 2013]) further compounds this issue. Diagnostic criteria stipulate that two or more of these behavioral phenomena must be present 1 and so individual presentations of RRB may differ greatly. This is pertinent as existing research has proposed two categories of RRB, low-order (repetitive movements and sensory) behaviors and high-order (insistence on sameness, preferred interest) behaviors.6,7 While low-order behaviors occur in typical early development and persist in other neurodevelopmental and genetic conditions, high-order behaviors are potentially autism specific.8,9 However, this low-high order psychometric RRB distinction may not reflect the lived experience where RRB subtypes appear interrelated, share self-regulatory functions, co-occur, and impact the occurrence of other RRB subtypes. 10
Most autism research has focused on autistic children, 11 with autistic adults being relatively understudied. Indeed, previous reviews conducted on RRB have focused on children and measures of RRB for children.8,12 Findings in the relatively few studies that have explored RRB in adulthood have been inconsistent. While some studies have suggested that there is no evidence for changes in RRB across the life span, 13 other studies have found that RRB decreases with age, with low-order behaviors decreasing to a greater degree than high-order behaviors. 7 Thus, the relative prevalence of high- and low-order RRB may vary between adulthood and childhood.
The studies to date have focused predominantly on change in the frequency of those RRB using measures based on child observation and proxy-informant studies adapted for an adult14,15 and cannot assess qualitative changes in the presentation of RRB in adulthood. One way in which RRB may change with age in both frequency and presentation is that of masking. Masking is a phenomenon by which autistic people may try to suppress their autistic traits to appear more neurotypical in response to social pressure.16–18 Research in this area has focused thus far on the social domain, although recent research has shown that autistic adults also report masking their RRB. 10 Masking may impact upon the assessment of RRB, particularly if research uses ratings from proxy-informants rather than self-report. Masking of RRB may appear to proxy-informants as a reduction of RRB. This is pertinent as autistic adults report that resistance to engaging in RRB is highly stressful, and one strategy for managing this stress is for autistic adults to isolate themselves and engage in the RRB alone. 10 Masking research from the social domain suggests that there may be gender differences with autistic females masking to a greater degree than autistic males.16–18 Therefore, it is important to understand the presentation of RRB in autistic adults more fully, and the impact of gender.
Thus, masking of RRB has implications for the appropriateness of proxy-informant report in RRB research, since a proxy-informant can only report on observed behaviors and not on the overall experience. Proxy-informant report has further limitations in the case of independent autistic adults, where proxy-informants may have far less contact. To better understand RRB in autistic adults, investigating RRB via self-report methods is necessary to give a holistic understanding of these behaviors. To the author’s knowledge, there has not been a systematic review specific to self-report of RRB in autistic adults to date.
With this review we aim to (i) synthesize what is known about autistic adult’s self-reported RRB and (ii) highlight gaps in our knowledge to inform future research. To do this, the review shall:
Establish what types of autistic adult’s self-reported RRB research have been investigated (e.g., repetitive movements, insistence on sameness, preferred interests, sensory sensitivities). Outline the methods used to study autistic adult’s self-reported RRB. Synthesize the findings of quantitative and qualitative studies of self-reported RRB with respect to phenomenology and experience of RRB. Establish the extent to which self-reported RRB research has considered masking of RRB. Establish the extent to which self-reported RRB research has considered gender differences.
Methods
Before conducting the review, we registered with PROSPERO (registration number: CRD42021297333). We amended the protocol once after registration to more clearly define and operationalize the inclusion and exclusion criteria.
Search strategy
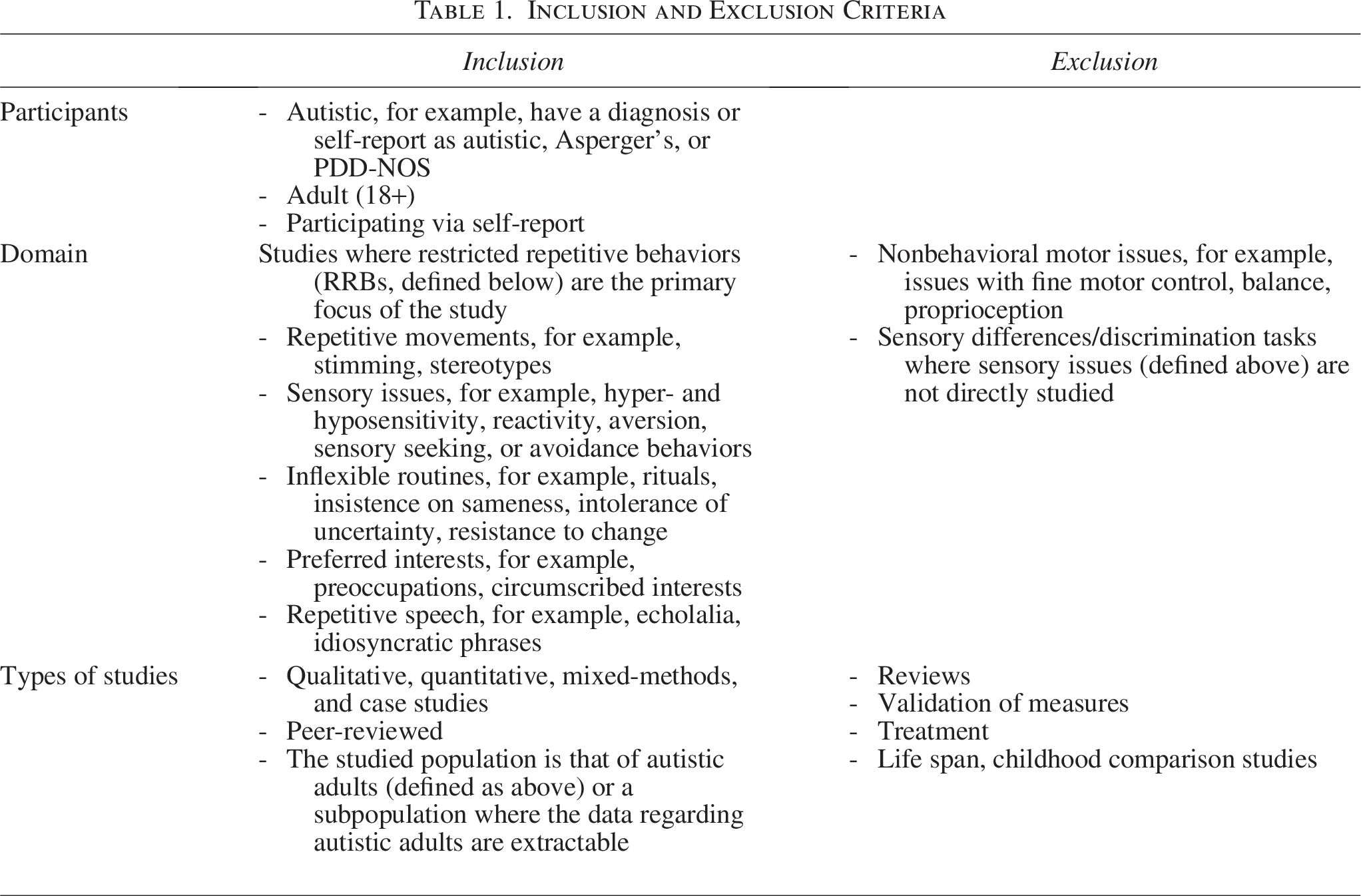
We selected a systematic approach to elucidate a holistic synthesis of our current understanding of RRB and to best address the aims of establishing the ways and extent that studies have investigated RRB to date. In consultation with a subject librarian, we identified the following databases: APA PsychNET, Embase, Web of Science, PubMed, and Scopus. We searched these databases for publications on autistic adults and RRB from inception to current date (last run February 2023) according to our search strategy, with syntax modified for each database (see Appendix A for search strategies), with the search restricted to title and abstract fields to increase relevance. To identify useful studies not captured in the database search, we screened reference lists of included studies for inclusion. We removed duplicates via Endnote and Covidence’s duplication identification strategy, and then manually. The first author initially screened the titles and abstracts of all publications, erring on the side of inclusion where certain criteria were unclear to ensure we retained all potentially relevant publications for review at the full-text level. The first author then screened the remaining publications, by which we retained studies for inclusion in the review if they met all the inclusion criteria and did not meet any of the exclusion criteria (see Table 1 for criteria). The second author screened a random 10% of studies at the title and abstract stage and all studies at the full-text level. Where the first and second authors could not reach agreement through discussion, a third reviewer made the final judgment for inclusion or exclusion.
Inclusion and Exclusion Criteria
Data extraction
Using a standardized table created for this study, we extracted eligible study data on the following: measures of RRB and/or method of study of RRB, types of RRB studied, participant demographics, difference in RRB by sex/gender (depending upon what studies reported), the consideration of masking (if any) and how, and results. The first author extracted the data, while the second author checked the extraction for accuracy.
Quality assessment
The Mixed Methods Appraisal Tool (MMAT) 19 is a critical appraisal tool designed for use in systematic reviews that include qualitative, quantitative, and mixed-methods studies. It outlines five methodological quality criteria for the appraisal of five different categories of study design: qualitative, quantitative randomized controlled trials, nonrandomized studies, quantitative descriptive studies, and mixed-methods studies. We determined outcomes for each criterion where “yes” means that the study meets the criteria, “no” where it does not, and “can’t tell” where there is insufficient information reported. The MMAT recommends giving detailed summaries of ratings rather than summed quality scores.
Narrative synthesis
We conducted a narrative synthesis
20
to synthesize study findings and their relationships within specific RRBs and between studies across the RRB domain, collating study findings into codes and sorting them into overarching subject areas to translate and categorize the data. The first author, who is autistic, carried this out from an insider’s perspective using an iterative framework consisting of the following four elements:
Developing a theory of how research into RRB has studied autistic adult’s RRB and why. Developing a preliminary synthesis of findings of included studies. Exploring relationships within and between studies. Assessing the robustness of the synthesis.
The second author, who is also autistic, sense-checked the results of this synthesis.
Meta-Analysis
We planned to conduct a meta-analysis where there were at least seven studies quantitatively examining differences in a subgroup on a comparable type of RRB, using mean scores on measures of frequency and standard deviations. Subgroups include gender, presence and absence of intellectual disability, and diagnosis. However, the number of included studies did not reach this threshold and as such we did not conduct the analysis.
Results
Overview
Following the removal of duplicates, we screened 3704 studies, reviewing 90 as full texts, and identifying 357,10,21–52 as eligible for inclusion in this systematic review. We outlined the full process of study selection in Figure 1 and study characteristics for included studies in Table A1.
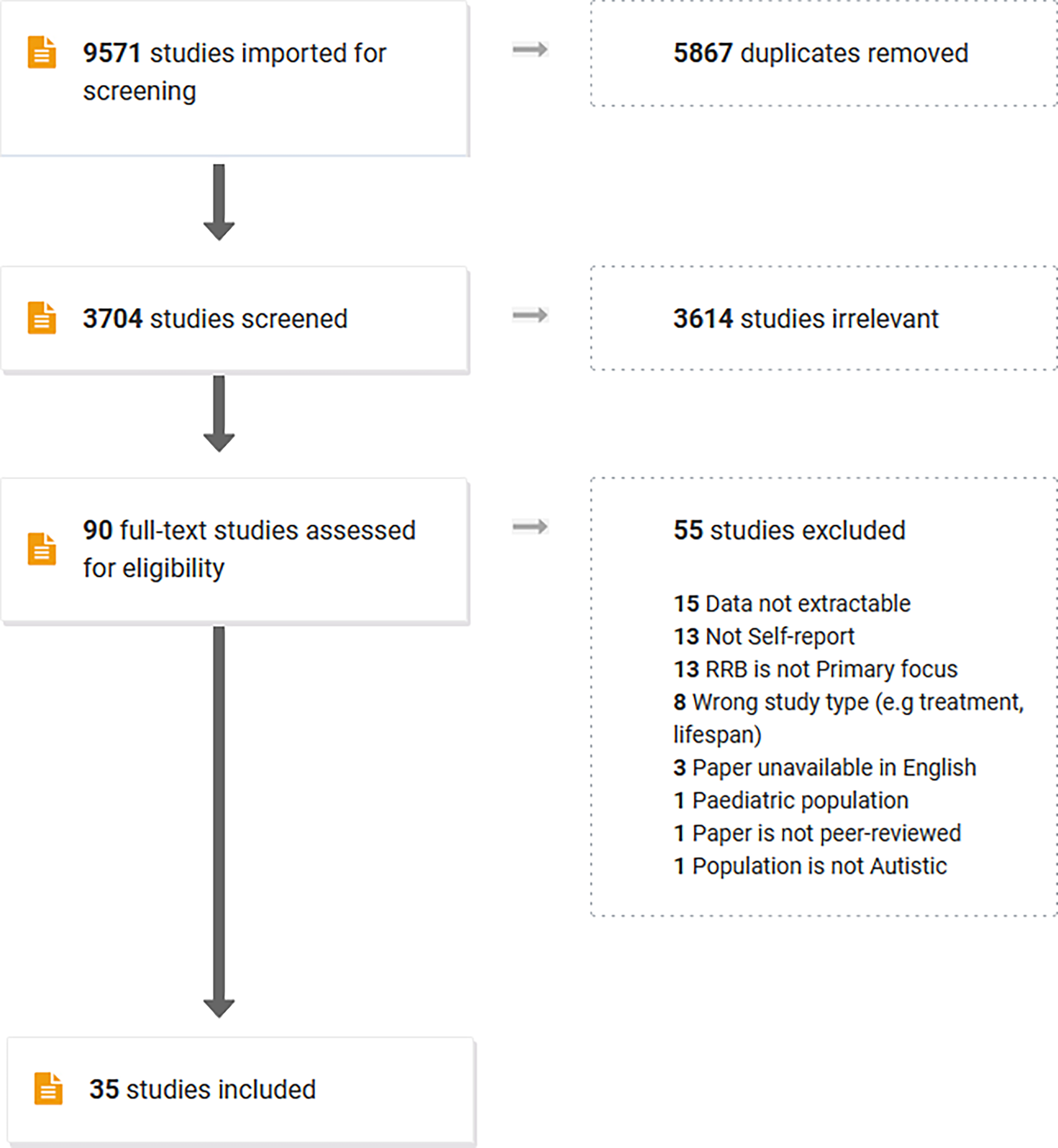
PRISMA flow diagram.
Although the systematic search was not limited by publication date, we found that studies ranged in publication from 2009 to 2022, with the majority of studies published in the last 5 years.
In total, the studies included 3340 autistic participants 3137 (93.9%) clinically diagnosed, and 203 (6.1%) self-identifying, when accounting for duplicated cohorts across studies, with sample sizes ranging from N = 6 to N = 687. All 35 studies included participants formally diagnosed with autism, Asperger’s, or pervasive developmental disorder, not otherwise specified, with only three studies including self-identified, suspected, or participants awaiting a diagnosis. Adults ranged in age from 18 to 77 years. Studies had limited reporting of participant demographics beyond this. Twenty-six of the included studies did not measure race or ethnicity,10,15,24–27,29–34,37,38,40,42–45,47–53 with the majority of participants in those that did being White and/or European. Similarly, only nine studies measured and reported IQ.7,21,25,31,32,38,47,49,50 Within those studies only two reported the range,7,38 with only one reporting the inclusion of participants with an IQ below 70. 47 Seven studies reported the mean IQ score for participants,25,31,32,38,49,50 all of which indicated that participants had average or above average intelligence. Fourteen studies recorded co-occurring diagnoses,26,27,31,32,35–37,39,40,47,49,50 of which 1026,27,31,35–37,39,47,51,52 reported them, and only nine reported specific diagnoses, with depression and anxiety being common among participants.26,27,31,35–37,39,47,52 Studies recruited participants via autism support groups and services, research databases, and social media.
Quality assessment
We did not assess studies on the development of scale measures (n = 5) using the MMAT. Overall, the quality of included studies (n = 30) was fair to great (see Table A2) although several issues, particularly around population representation (gender, race, IQ, age range), the use of measures not developed or validated for use with autistic participants, and a lack of reporting surrounding nonresponse bias and noncompletion rates, were common. Although, as part of the MMAT, we did not assess qualitative studies for population representation, and we did not assess quantitative nonrandomized studies for measure validity for autistic populations, these were issues for these studies also. Therefore, findings may not be generalizable, particularly to minorities within the autistic population such as gender-diverse participants, older autistic adults, non-White demographics, and those with below average IQ. The nature of the self-report methods that we used as an inclusion for this review may explain the lack of below average IQ participants—if those with below average IQ are indeed unable to self-report.
What types of self-reported RRB have been studied in autistic adults?
Of the 35 included studies, the vast majority of studies focused on the sensory sensitivity aspect of RRB. Twenty-four (68.6%) studies focused solely on this subtype of RRB,24–28,31,32,34–38,40,42,43,45–53 with an additional five (14.3%) studies examining some aspect of sensory sensitivities within their study’s design either by looking at RRB broadly (n = 4)15,33,39,41 or in combination with another RRB domain (n = 1, sensory and repetitive movements). 23 Within sensory sensitivities, the majority looked at sensory sensitivities generally, with three (10.3% of sensory sensitivity studies) studies looking at a specific aspect (visual, 42 noise, 35 and tactile defensiveness—particularly in relation to clothing 34 ), and five (14%) of the included studies did not look at sensory sensitivities at all.21,22,29,30,44
When considering all RRB examined by scale measures, seven (20%) studies focused on another domain of RRB (five preferred interests,21,22,29,30,44 one repetitive movements, 33 and one insistence on sameness 41 —two of these also included sensory sensitivity33,41).
What methods have been used to study RRB in autistic adults?
Of the included studies, 14 (40%) used primarily quantitative methods, 14 (40%) were primarily qualitative in method, 2 (5.7%) were mixed methods, and 5 (8.6%) studies related to scale development (see Table A1).
Overall, we identified nine distinct RRB scales (accounting for variations e.g., short form). Of those scales, five (55.6%) measured sensory sensitivities (AASP 54 SPQ, 48 SP, 55 SR-AS, 26 SPSI 56 ) one (11.1%) measured preferred interests (SIMS 30 ), one (11.1%) measured insistence on sameness (IUS-12 57 ), and two (22.2%) measured multiple RRB domains (RBQ-2A, 15 RBS-R 58 ) (see Table A1).
In addition to scales, one (2.9%) study used the Inventory for Repetitive Behaviors semistructured interview adapted for self-report 59 , nine (25.7%) studies used semistructured one-on-one interviews, three (8.6%) used focus groups, and one (2.9%) used magazine articles (see Table A1). Multiple studies also used additional questionnaires, including those with free-text response, to measure the experience of one or more RRBs across multiple studies.
Of the included studies, 18 (51.4%) were conducted online,15,22–24,29,30,36–38,46,49–51,53 with 14 (40%) conducted in person,10,21,25,27,31,32,34,35,42,43,48 4 via mail (11.4%),26,27,39,47 1 (2.9%) on magazine articles, 44 and 1 via internet search (2.9%). 28 Only one (2.9%) study asked about masking as part of its design, which was in relation to substituting stims (i.e., repetitive movements). 23
Self-reported RRB and gender
Nine (25.7%) of the 35 included studies considered gender differences in their analysis7,22,27,29–31,39,50,52 (note: four of these studies were unclear as to whether they were examining sex or gender differences).27,29,30,52 These studies found no significant difference in RRB scores and subscale scores using the RBQ-2A7,39 and that gender was not related to preferred interests and well-being. 22 Additional studies found no difference regarding cluster membership, 27 or in the frequency or intensity of preferred interests and the positive or negative impacts of those interests. 29 The latter also found that autistic males were more likely to report a preferred interest than autistic females, and that males were more likely to be interested in a wide range of activities. Autism, nature and gardening, and art and culture were the most popular preferred interests among autistic females, and computers, gaming, music, and bands were the most popular in autistic males. 29 One study found that autistic females’ special interests were significantly more likely to be motivated by engagement and flow than autistic males. 30 Three studies found significant differences in sensory sensitivity, with females having increased sensitivity particularly in taste and smell and low registration.31,50,52
Narrative synthesis
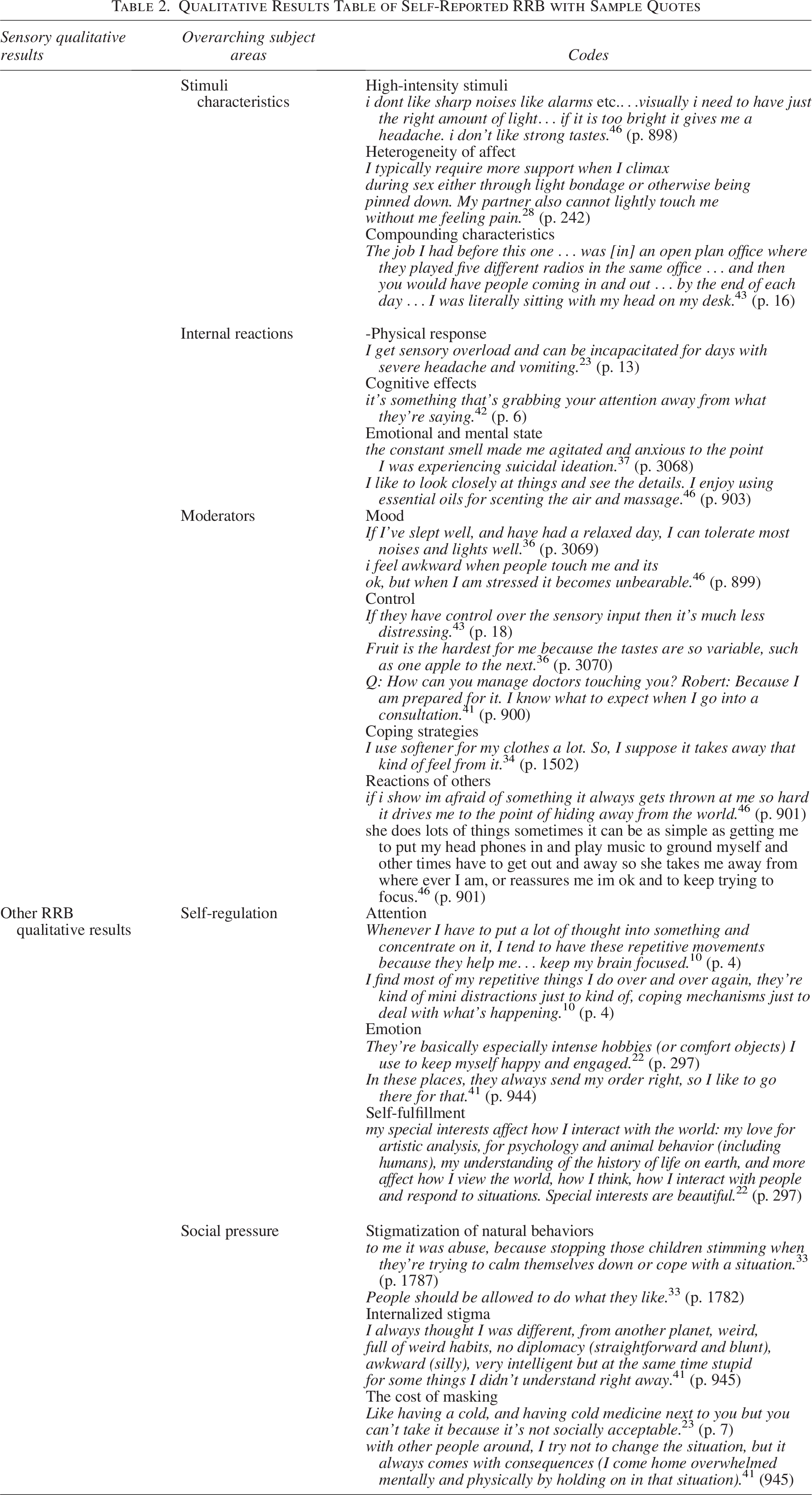
We used a narrative synthesis to examine qualitative and quantitative evidence of self-reported RRB, both in the sensory domain and regarding other aspects of RRB, both separately and in relation to one another. We present the qualitative subject areas and codes in brief in Table 2, in the form of a visual map in Figure 2, and in greater detail in the text.
Qualitative Results Table of Self-Reported RRB with Sample Quotes
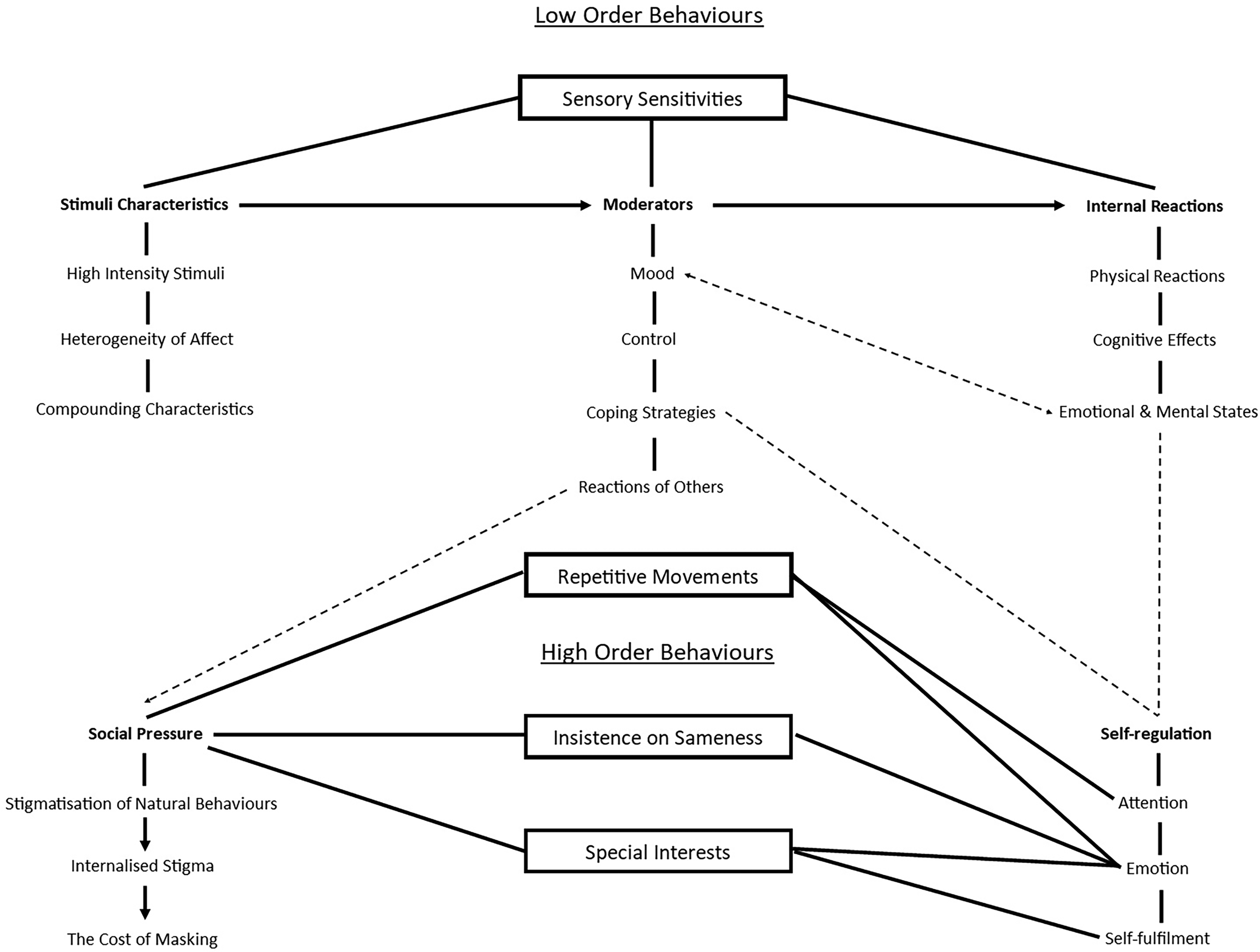
Visual map of qualitative evidence.
Sensory quantitative evidence
A total of 14 studies examined sensory sensitivities quantitatively (see Table A1). Overall, the studies found that the vast majority of autistic adults experienced sensory sensitivities in at least one sensory domain. Autistic trait scores correlated positively with sensory sensitivities, particularly regarding hypersensitivity and sensory avoiding behaviors.38,50,51 Autistic participants showed significantly higher levels of sensory sensitivities compared with nonautistic participants.24,31,38,50,51 Six studies examined hyposensitivity,24,26,27,36,51,53 finding that hyposensitivity was less common (28.6%) in autistic adults than hypersensitivity (93.9%)27,36,51 but co-occurred in high frequency in the sensory sensitivity group 27 while levels of hyposensitivity were not significantly different in autistic than ADHD adults. 24
Sensory sensitivities were highly correlated with all other RRBs,38,39 especially repetitive motor behaviors, 39 as well as being correlated with anxiety,39,47,48,53 aggression, 52 and dysfunctional eating behaviors. 40 Sensory avoiding behaviors were related to loneliness, which in turn contributed to stress and anxiety. 48
Sensory qualitative evidence
Ten studies examined sensory sensitivities qualitatively (see Table A1), from which we identified the following three main areas as part of the narrative synthesis: stimuli characteristics, internal reactions, and moderators.
Stimuli characteristics
We identified stimuli characteristics across seven of the studies as contributing to hypersensitivity and issues surrounding sensory overload.28,34,36,37,43,45,46 In particular, studies identified that high-intensity stimuli such as loud, high-pitched sounds, bright, flickering, or flashing lights, strong flavors or textures in food, and rough or scratchy fabrics as important factors in how much stimuli affected autistic people.28,34,36,37,43,45,46 “IIt like sharp noises like alarms etc.…visuIlly i need to have just the right amount of light… if it is too bright it gives me a headIche. i don’t like strong tastes” 46 (p. 898). Autistic participants seemed to commonly experience this increased sensitivity to high-intensity stimuli, which they reported contributed greatly to sensory overload, overwhelm, and increased the chance of sensory meltdowns.
One study identified a heterogeneity of affect in relation to stimuli where, depending on the individual, very light touch could be experienced as painful, while a firm touch might not. “I typically require more support when I climax during sex either through light bondage or otherwise being pinned down. My partner also cannot lightly touch me without me feeling pain” 28 (p. 242). At the same time other autistic people might find all touch painful, stating: “A lot the time I just don’t like to be touched at all. Anywhere. Instead of Oooo.someone’s touching me, it’s more like ARGH!! SOMEONE’S TOUCHING ME!” 28 (p. 241) or find touch pleasurable and desirable “I’m very sensitive to touch, which usually heightens my sexual experiences” 28 (p. 242). It is important then to acknowledge that while autistic adults may commonly share held hypersensitivities to high-intensity stimuli, there is heterogeneity in the experience of sensory stimuli by which different autistic individuals may perceive the same stimuli as positive, neutral, or negative.
In addition, five studies described compounding factors through which multiple stimuli and/or factors overlapping or in combination increased sensitivity and the likelihood of overwhelm while attempting to process all of the stimuli.28,36,37,43,46 “The job I had before this one … was [in] an open plan office where they played five different radios in the same office … and then you would have people coming in and out … by the end of each day … I was literally sitting with my head on my desk” 43 (p. 16).
Internal reactions
All 10 studies described internal reactions experienced in response to hypersensitivity to stimuli characteristics.23,28,34–36,38,42,43,45,46 Nine studies described a physical response to sensory stimuli with which they had a hypersensitivity to, through which autistic adults felt physical pain, discomfort, and other physical reactions.23,28,34,35,38,42,43,45,46 “I get sensory overload and can be incapacitated for days with severe headache and vomiting” 23 (p. 13). This shows that autistic people can experience extreme physical responses for enduring sensory stimuli and highlights the need for accommodations to minimize these stimuli in their environments.
Five studies described cognitive effects through which autistic people could not ignore the stimuli, found it absorbed their attention, and distracted or overwhelmed them so they were unable to engage with or pay attention to anything else.23,34–36,42 “It’s something that’s grabbing your attention away from what they’re saying” 42 (p. 6). Sensory issues therefore make the difficulties that autistic people experience because of their social communication differences even more difficult due to the distraction of sensory stimuli in the environment.
Eight studies described the impact sensory stimuli could have on the emotional and mental state, with hypersensitivity contributing to feelings of stress and anxiety, while also relating to self-harm, eating disorders, and difficulties with sex.23,28,34–36,42,45,46 “The constant smell made me agitated and anxious to the point I was experiencing suicidal ideation” 37 (p. 3068). While described in less detail, as the studies primarily focused on sensory sensitivities, participants reported that they experienced other sensory stimuli positively and that they were a point of fascination, relaxation, or enjoyment for them.28,34,37,42,43,46 “I like to look closely at things and see the details. I enjoy using essential oils for scenting the air and massage” 46 (p. 903). That autistic people experience some sensory stimuli as relaxing or enjoyable suggests that these may have an emotional self-regulatory benefit similar to those described later on for other RRBs.
Moderators
Eight studies described moderators, which affected autistic adults’ tolerance of negative sensory stimuli.28,34–37,42,43,46 These moderators included mood, control, coping strategies, and reactions of others.
Three of the studies described how mood affected their ability to tolerate negative stimuli, with a stressed mood making it more difficult to cope with. “I feel awkward when people touch me and its ok, but when I am stressed it becomes unbearable” 46 (p. 899). While a calm mood meant that they could tolerate it for longer or tolerate more stimuli.36,43,46 “If I’ve slept well, and have had a relaxed day, I can tolerate most noises and lights well” 36 (p. 3069). As such, autistic people’s other life stressors can have a direct impact on their sensory sensitivities, and likewise stress reduction in other areas would improve their ability to tolerate sensory sensitivities.
Five studies described control as a moderator, by which the more predictability and control autistic persons had over their environment, the less negatively affected by it they were as they could adapt to the environment accordingly.28,36,37,43,46 “If they have control over the sensory input then it’s much less distressing” 43 (p. 18). While unpredictable environments out of their control further contributed to stress.28,36,37,43,46 “Fruit is the hardest for me because the tastes are so variable, such as one apple to the next” 36 (p. 3070). Foreknowledge of a negative sensory stimuli gave autistic adults time to mentally prepare themselves for the internal reactions it would cause them. Q: ‘‘How can you manage doctors touching you?’’ Robert: ‘‘Because I am prepared for it. I know what to expect when I go into a consultation” 41 (p. 900). Predictability also means that autistic adults could utilize coping strategies preemptively to help moderate their experience of sensory stimuli.
Seven studies described coping strategies through which autistic adults moderated their sensory experience by avoiding the stimuli/environment, adapting the environment to remove or minimize the stimulus, using strategies to dampen or block the inputs (e.g., by using earphones), or using positive stimuli to help counteract the negative effects.28,34–36,42,43,46 “I use softener for my clothes a lot. So, I suppose it takes away that kind of feel from it” 34 (p. 1502).
Four studies found that the reactions of others moderated sensory experiences, by which negative reactions toward their sensory sensitivities led to increased stress, future avoidance, and isolation.36,37,42,46 If I show im afraid of something it always gets thrown at me so hard it drives me to the point of hiding away from the worl” 46 (p. 901). While positive supportive reactions allowed them to use existing coping strategies freely, and provided additional support.36,46 “She does lots of things sometimes it can be as simple as getting me to put my head phones in and play music to ground myself and other times have to get out and away so she takes me away from where ever I am, or reassures me im ok and to keep trying to focus” 46 (p. 901).
Other RRB quantitative evidence
There was limited quantitative evidence that focused on an RRB other than sensory sensitivity.
Moore 39 found between-factor correlations, with a strong correlation between preferred interests and insistence on sameness, and a strong to moderate relationships between sensory sensitivity and repetitive movements, and insistence on sameness and sensory sensitivities. The latter correlation is especially interesting as it shows the relationship between a high-order and low-order behavior. The above qualitative theme of moderators, particularly in relation to control and coping strategies, may explain this, through which autistic adults require sameness and predictability to moderate their sensory sensitivity.
Three studies examined preferred interests in isolation,21,22,29 finding that the majority of autistic adults had at least one preferred interest, covering a broad range of topics, including creative arts, music, autism, computers, nature, and gardening, with many having multiple preferred interests.22,29 Studies found associations between these interests and positive outcomes, subjective well-being, life satisfaction, and happiness.22,29 At a neurological level, the posterior cingulate cortex may differentially modulate preferred interest in autistic adults, and emotional regulation surrounding preferred interests may be related to self-referential cognition. 21 However, Grove 29 found that high-intensity engagement (spending more days per week and more hours per day on the interest) was related to lower levels of well-being. The study does not examine whether this high-intensity engagement with preferred interest/s may be due to other factors, such as having more free time as a result of a lack of employment, which would also negatively impact well-being. Likewise, this lower well-being with higher intensity engagement may be due to a lack of support in this engagement from others and bullying surrounding preferred interests, which Bross 22 reported as associated with higher levels of depression, anxiety, and stress.
Other RRB qualitative evidence
Qualitative studies on RRB other than sensory sensitivities were lacking, with only three studies looking at repetitive movements, two on preferred interests, and one on insistence on sameness (see Table A1), from which we identified two themes in the narrative synthesis: self-regulation and social pressure.
Self-regulation
All three studies on repetitive movements10,23,33 described them as having a self-regulatory function both in terms of attention and emotion. Participants described how repetitive movements helped to regulate their attention to help them focus on something “Whenever I have to put a lot of thought into something and concentrate on it, I tend to have these repetitive movements because they help me … keep my brain focused” 10 (p. 4). Repetitive movements also distracted them from distressing things, such as negative thoughts or overwhelming environments and sensory sensitivities. “I find most of my repetitive things I do over and over again, they’re kind of mini distractions just to kind of, coping mechanisms just to deal with what’s happening” 10 (p. 4).
Autistic people likewise used repetitive movements alongside special interests to self-regulate emotion, allowing for release of overwhelming emotions (positive and negative), emotional expression, while being soothing. “They’re basically especially intense hobbies (or comfort objects) I use to keep myself happy and engaged” 22 (p. 297). Interestingly, this complements the findings of the sensory sensitivity analysis through which repetitive movements provide relief for the internal reactions triggered by hypersensitivity to sensory stimuli. It also provides a potential explanation for the quantitative evidence, which demonstrates a strong relationship between sensory sensitivities and repetitive movement behaviors, by which an increase in sensory sensitivities would result in an increase in repetitive movements to self-regulate the impact of those sensitivities. Park-Cardoso 41 found that insistence on sameness in food spaces also had a preemptive self-regulatory benefit on emotion by reducing uncertainty and the amount of stressful situations autistic adults encounter. “In these places, they always send my order right, so I like to go there for that” 41 (p. 944). Repetitive movements and preferred interests also held other self-regulatory benefits by providing pleasure and release10,22,28 and in the case of preferred interests, provided motivation and contributed to self-fulfillment and development.22,44
“My special interests affect how I interact with the world: my love for artistic analysis, for psychology and animal behavior (including humans), my understanding of the history of life on earth, and more affect how I view the world, how I think, how I interact with people and respond to situations. Special interests are beautiful 22 (p. 297).
Social pressure
We identified social pressure across studies about repetitive movements, insistence on sameness, and preferred interests,10,22,23,33,41,44 leading to masking of all three types of behaviors.10,22,23,33,41
Self-reported RRB and masking
Three studies considered masking within their introduction or when designing the study methods,10,23,41 although two additional studies reported findings of masking repetitive movement behaviors. Between the five studies,10,22,23,33,41 they reported masking in repetitive movements, insistence on sameness, and preferred interests, but not sensory issues. The masking of these behaviors was a result of social pressure surrounding their RRBs, by which the negative reactions of others led to a perception of stigmatization, an unaccepting social environment, and internalized stigma in autistic adults.10,22,23,33,41 “I always thought I was different, “from another planet,” weird, full of weird habits, no diplomacy (straightforward and blunt), awkward (silly), very intelligent but at the same time stupid for some things I didn’t understand right away” 41 (p. 945).
This internalized stigma led to autistic adults masking their RRB to try to avoid judgment from others,10,41 but came at a cost, with masking contributing to negative effects on emotions and cognition, provoking stress, anxiety, and meltdowns due to masking itself being stressful. “With other people around, I try not to change the situation, but it always comes with consequences (I come home overwhelmed mentally and physically by holding on in that situation)” 41 (945). In addition, negative effects of masking resulted from the loss of the benefits that performing RRB provides as described above.10,23,33,41 “Like having a cold, and having cold medicine next to you but you can’t take it because it’s not socially acceptable” 23 (p. 7).
Autistic adults described RRB as natural autistic behaviors and ways of coping, which could occur both purposefully and without thought, 10 objecting to teachings that they should stop them. “To me it was abuse, because stopping those children stimming when they’re trying to calm themselves down or cope with a situation” 33 (p. 1787). Participants expressed a desire for RRB to become socially acceptable so that they could benefit from them, freely be themselves, and no longer feel the need to mask.10,33,41 “People should be allowed to do what they like” 33 (p. 1782).
Discussion
This is the first systematic review of RRB in self-reporting autistic adults, identifying 35 studies that met the inclusion criteria.
The majority of included studies focused on the sensory domain of RRB, finding that sensory sensitivities were higher in autistic adults and those with higher autistic trait scores than non-autistic participants and those with lower trait scores. Studies found that hypersensitivity was more common in autistic adults than hyposensitivity, and sensory issues were related to mental health issues such as anxiety, stress, aggression, and disordered eating. Sensory sensitivities were related to all other types of RRB, and our narrative synthesis identified subject areas including stimuli characteristics, internal reactions, and moderators, self-regulation, and social pressure. This suggests a narrative where most autistic adults experience hypersensitivity to some sensory stimuli, the unpleasantness of which they then try to avoid, but in doing so may also avoid social situations, contributing to loneliness and increased anxiety surrounding social situations. These sensory hypersensitivities caused discomfort and stress that could not be easily ignored. This decreased autistic adults’ ability to function and cope with everyday life and other everyday stressors, which in turn reduced their capacity to cope with sensory sensitivities. In response to these stressors, autistic adults self-regulate via RRB in other domains. Insistence on sameness behaviors allows moderation of the impact of sensory sensitivities through predictability, giving them the opportunity to adapt their environment or avoid it. Autistic adults used repetitive movement behaviors to self-soothe, allow them to redirect their attention, and allow for the expression and release of emotions. However, social pressure and stigma from others disrupted these methods of self-regulation, leading to autistic adults masking their RRB to appear more socially acceptable or neurotypical, thus not only reducing their ability to self-regulate in this manner but also adding additional stressors. This would further contribute to what appears to be a cycle of stress given that autistic adults describe how sensory sensitivities can too contribute toward stress; it follows that prior stress would lower their threshold to cope with further stress (from the sensory stimuli or otherwise) before becoming overwhelmed. As such, reducing stressors in other areas of their life would help autistic people tolerate sensory stimuli, and likewise, reducing sensory stimuli stressors would help autistic people to cope with other stressors in their life.
A better understanding of hypersensitivity of sensory stimuli allows for minimizing those stimuli in social environments, reducing overlapping stimuli, and particularly those that are loud, high-pitched, bright, or scratchy, to better include autistic people. This emphasizes the need for more initiatives, similar to those advocated for by the National Autistic Society such as Autism Hour in supermarkets where sensory stimuli are reduced in store for an hour, 62 throughout society to improve accessibility and reduce anxiety. Likewise, increased awareness of the self-regulatory benefits of repetitive movements or “stims,” would reduce the stigma of these behaviors and therefore stress. Stigma motivates autistic people to mask RRB and so the reduction of stigma would allow for a reduction in masking, leading to an increase in the self-regulatory benefits, which would make coping with sensory sensitivities and other stressors easier.
Research’s sudden interest in sensory sensitivities can likely be explained by the APA diagnostic criteria adding sensory sensitivities in 2013. This surge further highlights how underresearched other areas of RRB have been, 3 which a lack of research on adults relative to autistic children has further compounded. 11 Insistence on sameness behavior was the least researched area of RRB, followed by repetitive movements and special interests. Research relatively neglecting high-order behaviors compared with low-order behaviors is at odds with the suggestion that while low-order behaviors (i.e., repetitive movements, sensory sensitivities) occur in typical development and in other neurodevelopmental and genetic conditions, high-order behaviors may be autism specific.8,9 As such, future research should look to examine insistence on sameness behaviors, and preferred interests in particular, as well as repetitive movements to better understand these RRBs.
The inclusion criteria of self-report methods may explain the lack of research included before 2009. Historically, autistic adult studies have used childhood observation, and proxy-informant measures adapted for use in adults, rather than using self-report measures for adults.14,15 This is despite the majority of autistic adults being capable of self-report60,61 and the potential limitations of proxy-informant-only report, particularly in autistic adults, who may live independently and/or mask their RRB around others. 10 Despite the importance of considering masking in RRB research, only three studies considered it within their introduction or when designing the study methods.10,23,41 However, we identified evidence of masking in both those studies and an additional two qualitative studies on RRB.22,33 This suggests that masking RRB is commonplace for autistic adults and is an intrinsic part of the experience of RRB. Such existing measures, which do not consider masking, as well as observation and proxy-informant report, are unlikely to capture this aspect of autistic adult’s experience of RRB and furthermore provide less valid and reliable measurement of RRB in adulthood. Therefore, future research should consider masking RRB in their design, include items related to masking RRB in scale development, and develop a specific measure of RRB masking. This is particularly important given the finding that masking RRB both reduces autistic adults’ ability to self-regulate and causes additional stress. 10 Future research should aim to better understand the impact masking RRB has on functioning and emotional and mental well-being in autistic adults.
Less than half of the included studies considered gender differences. Of the studies that considered gender differences, findings were mixed and limited to one to two studies in each area. Where studies found differences, they did not investigate the reasons behind it, so while some gender differences in sensory sensitivity and preferred interests may exist, whether this is due to biological or societal factors, or some combination thereof, is unknown. As such, future research should consider whether gender differences exist in each domain of RRB and uncover the reason for any such differences. While thus far the limited research on gender difference has concentrated on the difference between male and female autistic adults, future research should also include other gender identities, such as nonbinary autistic adults, as research has shown that autistic people have higher rates of gender variance than controls. 63
Limitations
The review’s focus on autistic people’s self-reported repetitive behaviors highlights the experience of RRB, but those who cannot self-report may experience RRB differently. The studies in the review did not include many autistic people with below average IQ, potentially because of difficulties this group may have in traditional methods of self-report. Although only one study 47 reported including participants with below average IQ, it is important to note that these participants were able to self-report in this context. As such, self-report research should not exclude those with below average IQ from participating simply on the basis of their IQ score and should aim to include them as much as possible and develop new methods to make self-report more accessible. Where self-report is not possible, research should look to address how to examine their experience while accounting for and identifying potential masking of RRB. Another limitation lies in our exclusion criteria for the database search, which may also have excluded potentially relevant studies as a result of data on the target population of self-reporting autistic adults not always being extractable or separatable from, say child and adolescent autistic people included in some studies, or adults from other populations such as those with ADHD. This meant that we did not report some potentially relevant results even in included studies. However, this meant we could ensure the relevancy of results to the review, and to autistic adults.
Conclusion
Overall, the systematic review found that research into RRB in self-reporting autistic adults is a new and emerging area of study in the past 13 years and that research has so far focused predominantly on the sensory domain with repetitive movements, insistence on sameness, and preferred interests comparatively neglected. Existing research used both quantitative and qualitative methods, with the majority using survey and questionnaire measures or semistructured one-on-one interviews. We rated research quality from fair to great for all studies (excluding scale development), which indicates a need for improvement in obtaining representative samples for autistic populations, particularly with regard to gender (including gender-diverse participants), race, and below average IQ, and in the validation of measures for use with autistic people. Initial evidence suggests that, while topographically distinct in form, RRBs have a self-regulatory function of emotion and attention, which helps autistic adults cope with their sensory sensitivities, among other issues, suggesting a need for a less categorical and more interrelated approach in future when researching this domain of autism and a need for better understanding and awareness of these benefits. However, social pressure hampers this strategy, which leads autistic adults to mask their RRB, which causes additional stress and is detrimental to well-being. Despite this, RRB research’s design does not often consider masking, with gender differences also often neglected, both of which should be considered in future research.
Footnotes
Author Disclosure Statement
The authors have no known conflicts of interest to disclose.
Funding Information
This study was funded by the
Authorship Confirmation Statement
E.C.: Conceptualization, data curation, methodology, formal analysis, investigation, project administration, writing—original draft, and writing—review and editing. E.D.: Data curation and investigation. A.R.: Conceptualization, methodology, writing—review and editing, and supervision. M.B.: Conceptualization, methodology, writing—review and editing, and supervision. The manuscript has been submitted solely to this journal and has not been published elsewhere.