
Abstract
Background:
Better identification of autistic people and increased life expectancy for people with intellectual and developmental disabilities have given rise to an urgent need to better understand end-of-life care in autistic people. We compared hospice utilization of autistic older adults with non-autistic older adults and examined if known inequities in hospice utilization among the general population are exacerbated among autistic older adults.
Methods:
We analyzed hospice claims from Medicare, which insures Americans older than 65 years and covers hospice costs. Our sample included 5468 autistic older adults and 10,934 matched population comparison older adults who died during 2013–2021. We used multivariable logistic regression to compare these groups on the odds of any, early, intermediate, and late hospice utilization. We defined early hospice utilization as at least 28 days before death, intermediate as 4–27 days before death, and late as within 3 days of death. Interaction terms were used to assess whether effects were modified by beneficiary’s sex, race, or rurality. In a sensitivity analysis, we repeated our analyses in unmatched samples.
Results:
The autistic older adult and matched population comparison groups had similar odds of any hospice utilization (odds ratio [OR]: 1.05; 95% confidence interval [CI]: 0.98–1.13), early (OR: 1.01; 95% CI: 0.91–1.11), intermediate (OR: 1.03; 95% CI: 0.95–1.13), and late hospice (OR: 1.07; 95% CI: 0.96–1.19). In our models evaluating the impact of other known inequities, we did not find significant interactions between autism diagnostic status and sex, race, or rurality. Results were similar in the unmatched samples.
Conclusion:
Given the body of literature documenting health disparities in autistic people, our findings are heartening, suggesting that Medicare-enrolled autistic older adults experience similar receipt and timing of hospice as their non-autistic peers. Our findings highlight the potential power of health policies that provide zero-cost, universal benefits to Americans in reducing health care utilization disparities among autistic people.
Community Brief
Why is this an important issue?
Autistic people may use health care services less than non-autistic peers. It is important to understand differences in health care use and end-of-life care in older adulthood. This information will be useful to autistic people and their families for future planning as well as to the health care system for preparing to meet the needs of aging autistic adults.
What was the purpose of this study?
Hospice care focuses on comfort and quality of life before death when a person is diagnosed with a progressive condition from which they are not expected to recover. The purpose of this study was to compare the hospice use of Medicare-enrolled autistic older adults with that of non-autistic older adults.
What did the researchers do?
We analyzed hospice claims from Medicare, a government-funded insurance program that provides coverage for Americans older than 65 and fully covers hospice costs. We identified 5468 autistic older adults who died and matched them to 10,934 non-autistic older adults who died. Matching involves creating a comparison group of non-autistic individuals who have similar characteristics to the autistic sample, including sex, race, and rurality. We compared groups on the odds of any, early, intermediate, and late hospice use. We defined early hospice use as at least 28 days before death, intermediate as 4–27 days before death, and late as within 3 days of death. We looked at whether differences between groups differed based on sex, race, or rurality. We also repeated our analyses in unmatched samples of autistic and non-autistic older adults.
What were the results of this study?
Autistic older adults and non-autistic older adults had similar odds of any, early, intermediate, and late hospice use. Sex, race, and rurality had similar effects on the odds of hospice use among autistic and non-autistic older adults. Results were similar in the matched and unmatched samples.
What do these findings add to what was already known?
While multiple other studies have identified disparities in health care utilization in autistic people, this study suggests that these disparities may decrease as autistic people age and have access to comprehensive insurance with universal, no-cost benefits such as Medicare. Hospice care is an area in which autistic people may not experience disparities.
What are the potential weaknesses of this study?
Findings may not predict hospice use among future generations of autistic older adults because the older adults in this study were born and raised before access to modern diagnoses and supports. Some autistic older adults may have been miscategorized as non-autistic.
How will these findings help autistic adults now or in the future?
Our findings may provide some comfort about the unknowns of aging for Medicare-enrolled autistic older adults, as they have similar use of hospice compared with their non-autistic peers. Disparities that may exist for other health care services earlier in life may not persist into end-of-life care. Our findings may also be used to advocate for more health policies that provide zero-cost, universal benefits to reduce health care use disparities among autistic people.
Background
By 2050, there will be about 5.5 million autistic adults in the United States, and more than 1 million of these autistic adults will be aged 65 or older. 1 The confluence of both the rise in identification of autism in adulthood 2 and the increase in life expectancy in economically advantaged nations for people with intellectual and developmental disabilities 3 has given rise to an urgent need to better understand end-of-life care in autistic people. While autistic older adults with and without co-occurring intellectual disability experience an increased risk for chronic health conditions as they age compared with the general population, very little is being done to further understand how to best meet the service needs of autistic people with these co-occurring conditions at the end of life.4–6 Better understanding end-of-life care for autistic people is particularly urgent given that the National Institutes of Health (NIH) recently identified people with disabilities as a health disparities population 7 and emphasized the importance of understanding how these disparities persist into older adulthood. 8
Hospice care refers to care focused on comfort and quality of life that is provided before death when a person has been diagnosed with a progressive and irreversible condition from which they are not expected to recover. 9 Hospice services are increasingly in demand as the number of older adults with chronic conditions steadily rises and the Baby Boomer population ages into and through older adulthood. 10 In the United States, the vast majority of Americans aged 65 and older qualify for and utilize Medicare, which fully covers the cost of hospice care for individuals who have chosen to pursue comfort care rather than curative care for their terminal illness. 11 Medicare pays over 90% of hospice patient care days in the United States, while Medicaid pays fewer than 5% of hospice patient care days. 12 Medicare beneficiaries who are dually eligible for Medicaid and Medicare receive coverage for hospice care from Medicare and coverage for associated care (e.g., room and board) in nursing facilities from Medicaid.12,13 Before 2020, the percentage of older adults with Medicare who utilize hospice increased every year, with 51.6% of Medicare decedents receiving one or more days of hospice care in 2019. 13 However, since the COVID-19 pandemic, there has been a downward trend, with 47.3% of Medicare decedents receiving one or more days of hospice care in 2021. 13 Earlier admission to hospice is associated with greater levels of patient satisfaction, lower rates of acute care utilization, and decreased costs,14–16 suggesting that early hospice admission is a key metric for end-of-life care quality.
The utilization of end-of-life services, such as hospice, differs substantially across minoritized groups, with race, ethnicity, age, geographical location, and socioeconomic status impacting one’s ability to access services.10,17–19 Rural areas have less availability of hospice services compared with urban areas, and racial and ethnic minority patients who are Medicare beneficiaries are less likely to use hospice services compared with White patients.18,20,21 These disparities may partially explain lower levels of hospice utilization and later timing of hospice utilization among minoritized individuals. 22 These studies display the stark disparities in end-of-life care for individuals in minority populations and provide a path forward so that the U.S. health care system can work toward decreasing the burden of these barriers.
The NIH’s call-to-action as well as the lack of literature about hospice care for autistic older adults reveals a need to explore this area further. Therefore, the primary purpose of this study was to compare hospice care utilization of Medicare-enrolled autistic older adults with that of non-autistic older adults. The secondary purpose was to determine if race, sex assigned at birth, region, and rurality altered rates of utilization in autistic older adults compared with non-autistic older adults. We hypothesized that autistic older adults would be less likely to utilize hospice and would begin hospice closer to their date of death than our population comparison group. We further hypothesized that hospice utilization disparities would be exacerbated for autistic women, autistic people from minoritized racial and ethnic groups, and autistic people from rural areas.
Methods
Data source
Data used in this study are derived from Medicare’s Standard Analytical Files (SAF) for the years 2013 through 2021. Medicare SAF data include limited data set information on 100% of Medicare beneficiaries for these years. We used deidentified beneficiary-level health care claims data for inpatient, outpatient, and hospice records. The outpatient records contain medical billing claims from institutional outpatient providers such as hospital outpatient departments, rural health clinics, renal dialysis facilities, outpatient rehabilitation facilities, federally qualified health centers, and community mental health centers; they do not include professional service claims from noninstitutional professional providers such as physicians, physician-assistants, clinical social workers, or nurse practitioners.
Study population
We included autistic adults in this study if they (1) were aged 65 years or older; (2) were enrolled in Medicare Fee for Service for at least 12 months between 2013 and 2021; (3) had at least one inpatient or outpatient encounter with an assigned diagnostic code for autism spectrum disorder at any time between January 1, 2013, and December 31, 2021; and (4) died during the observation period. Autism spectrum disorder diagnoses were identified using codes 299.0, 299.00, 299.01, 299.9, 299.90, 299.91 from the 9th edition or F84.0, F84.1, F84.5, or F84.9 from the 10th edition of the International Classification of Diseases. We excluded beneficiaries who were enrolled in Medicare advantage plans because of concerns about the availability of accurate, complete data in managed care programs, consistent with standard practices in the existing literature.4,23–25 We included beneficiaries with at least one claim with an autism diagnostic code as previous research suggests that Medicare-enrolled autistic adults with more than one claim with an autism diagnostic code are demographically similar to those with only a single claim. 26 Medicare beneficiary death dates are obtained by the Centers for Medicare and Medicaid Services from the U.S. Social Security Administration nightly. Our population comparison group met the same inclusion criteria as our autistic group, except without an encounter for which the beneficiary was assigned an autism spectrum disorder code within the study period. Variable ratio propensity score matching was used to match at most two beneficiaries in the population comparison sample with one autistic older adult; beneficiaries were matched exactly on sex, race, region, and rurality, while age and year of death were matched with a caliper of 0.2.
Measures
Our dependent variables were as follows: (1) any hospice utilization, (2) early hospice utilization, (3) intermediate hospice utilization, and (4) late hospice utilization. Hospice utilization was identified by the presence of claims in the Hospice Medicare SAF. Any hospice utilization was defined by hospice admission at least a day before death. Early hospice utilization was defined as hospice admission at least 28 days before death. Intermediate hospice was defined as hospice admission between 4 and 27 days before death. Late hospice was defined as hospice admission within 3 days of death. 21 Our primary independent variable was autism diagnostic status. Our secondary independent variables were sex, race, U.S. region, and rurality. The beneficiary’s sex, race, and region were obtained from the Master Beneficiary Summary File. Rurality was obtained by using the beneficiary’s Social Security Administration code for their county of residence to create categories of rurality based on U.S. Department of Agriculture’s rural–urban continuum codes. 27 Covariates included Medicare-recorded year of death, age at death, and medical comorbidities defined by the Charlson Comorbidity Index. 28
Statistical analysis
Descriptive statistics included median and interquartile range for continuous variables and frequencies and percentages for categorical variables. Multivariable logistic regression was used to compare the odds of hospice utilization between autistic adults and the population comparison group, and interaction terms were used to assess whether these effects were modified by beneficiary’s sex, race, or rurality. Significance was evaluated at the 0.05 level, and 95% confidence intervals (CIs) for the odds ratios (ORs) were provided. As a sensitivity analysis, we repeated our analyses on the unmatched samples of autistic older adults and the population comparison group. All analyses were performed using SAS v9.4.
Results
In total, 5468 autistic older adults met the inclusion criteria for analyses and were matched to a population comparison sample of 10,934 older adults. Demographic information for autistic older adults and our matched population comparison group is displayed in Table 1. Beneficiaries were mostly male (64.5%) and White (88.5%). Among our sample of autistic older adults, 34.2% had diagnostic codes for a co-occurring intellectual disability, compared with 1.8% of the population comparison group. The majority of beneficiaries were located in metro areas with either a population greater than 1 million people (45.9%) or less than 1 million people (35.4%).
Characteristics of Matched Cohort
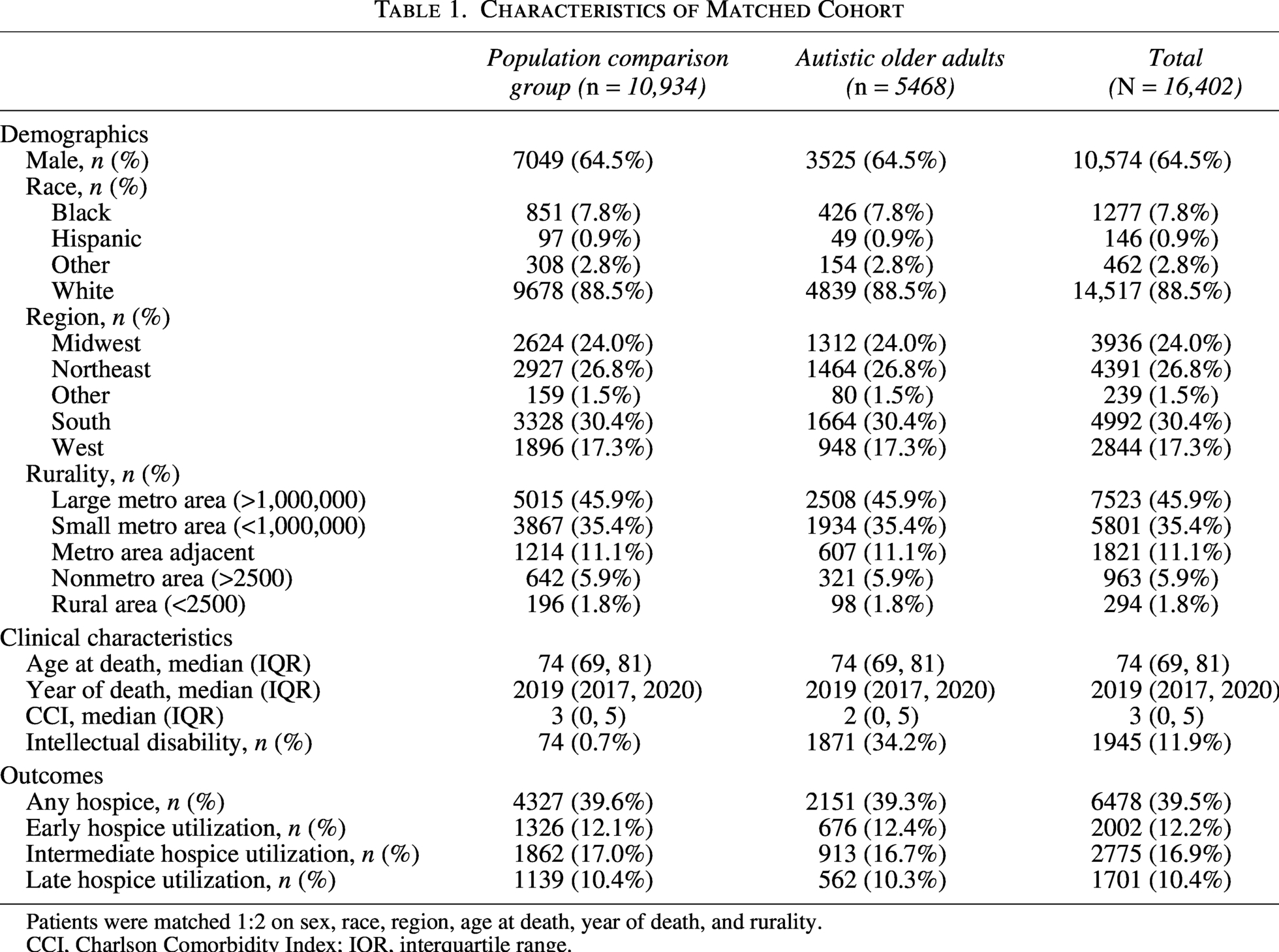
Patients were matched 1:2 on sex, race, region, age at death, year of death, and rurality.
CCI, Charlson Comorbidity Index; IQR, interquartile range.
Overall, our autistic older adult and matched population comparison groups had similar odds of any hospice utilization (OR: 1.05; 95% CI: 0.98–1.13). Also, our autistic older adult and population comparison groups had similar odds of utilizing early hospice (OR: 1.01; 95% CI: 0.91–1.11), intermediate hospice (OR: 1.03; 95% CI: 0.95–1.13), and late hospice (OR: 1.07; 95% CI: 0.96–1.19). In our multivariable models evaluating the impact of other known inequities (Table 2 and Fig. 1), we did not find significant interactions between autism diagnostic status and sex, race, or rurality.
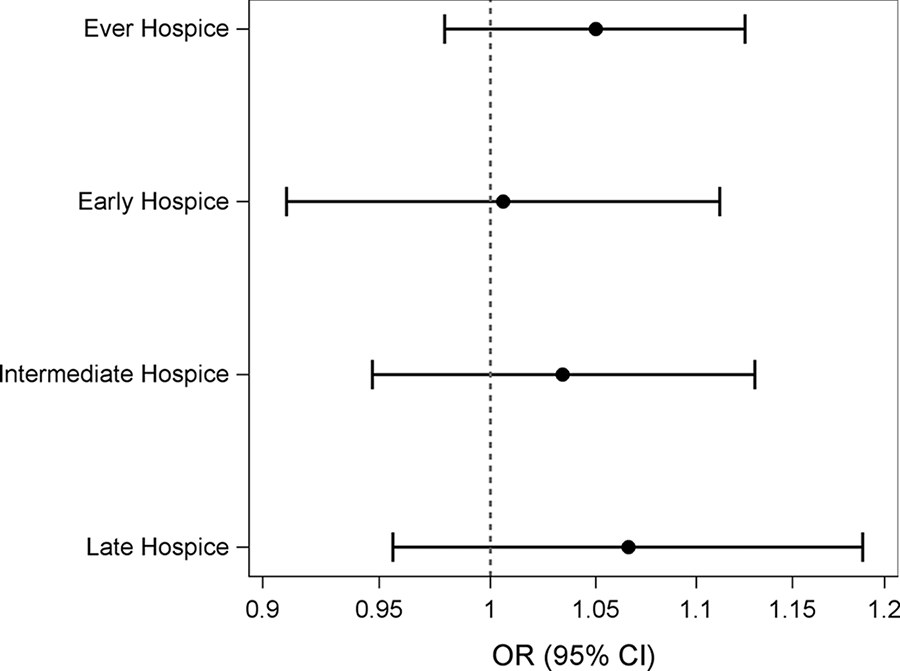
Adjusted odds ratios comparing hospice utilization between Medicare-enrolled autistic and non-autistic older adults.
Odds Ratios and 95% CIs Comparing Hospice Utilization Between Autistic Adults and Non-Autistic Adults Stratified by Sex, Race, and Rurality, Controlling for CCI, Age at Death, Year of Death, and Region
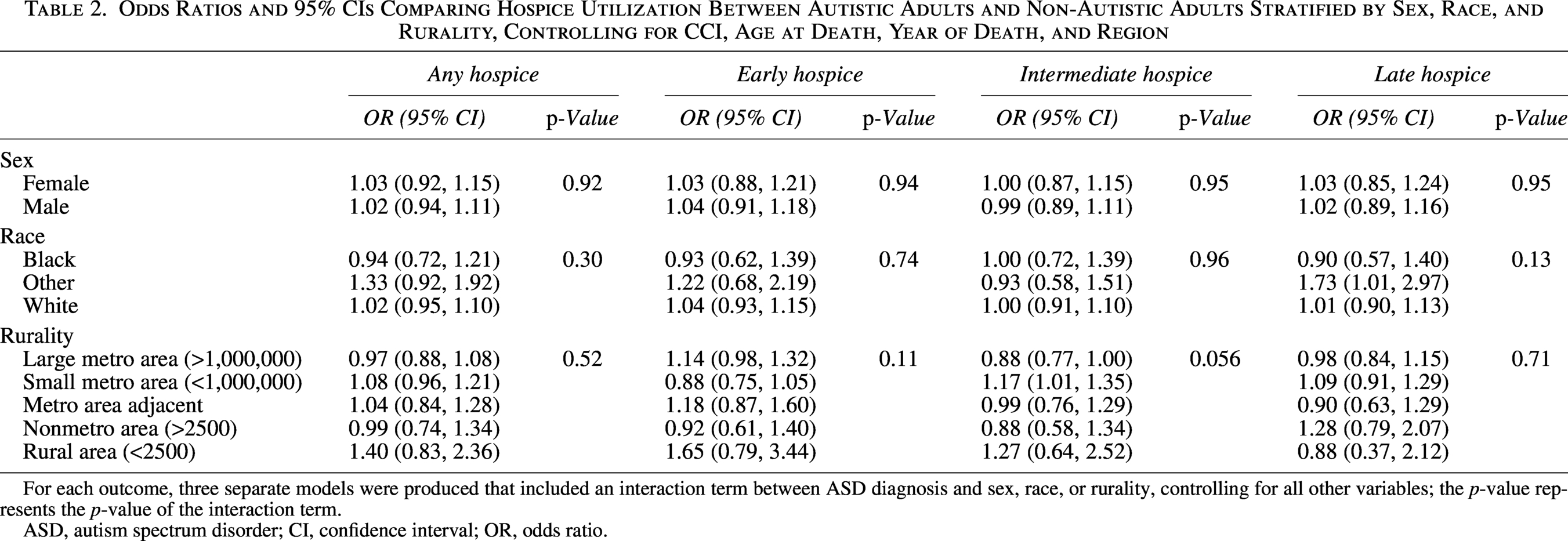
For each outcome, three separate models were produced that included an interaction term between ASD diagnosis and sex, race, or rurality, controlling for all other variables; the p-value represents the p-value of the interaction term.
ASD, autism spectrum disorder; CI, confidence interval; OR, odds ratio.
Sensitivity analysis
The sensitivity analysis included 5474 autistic older adults (six autistic older adults were unable to be matched and were thus excluded from our main analyses) and 1,298,277 population comparison beneficiaries (Table 3). The unmatched results were consistent with the matched results in terms of statistical significance. The autistic older adult and population comparison groups had similar odds of any hospice utilization (OR: 0.97; 95% CI: 0.92–1.03). Also, our autistic older adult and population comparison groups had similar odds of utilizing early hospice (OR: 0.99; 95% CI: 0.92–1.08), intermediate hospice (OR: 0.96; 95% CI: 0.90–1.04), and late hospice (OR: 0.97; 95% CI: 0.89–1.06). In our multivariable models evaluating the impact of other known inequities in the unmatched samples (Table 4), we did not find significant interactions between autism diagnostic status and sex, race, or rurality.
Characteristics of Unmatched Cohort
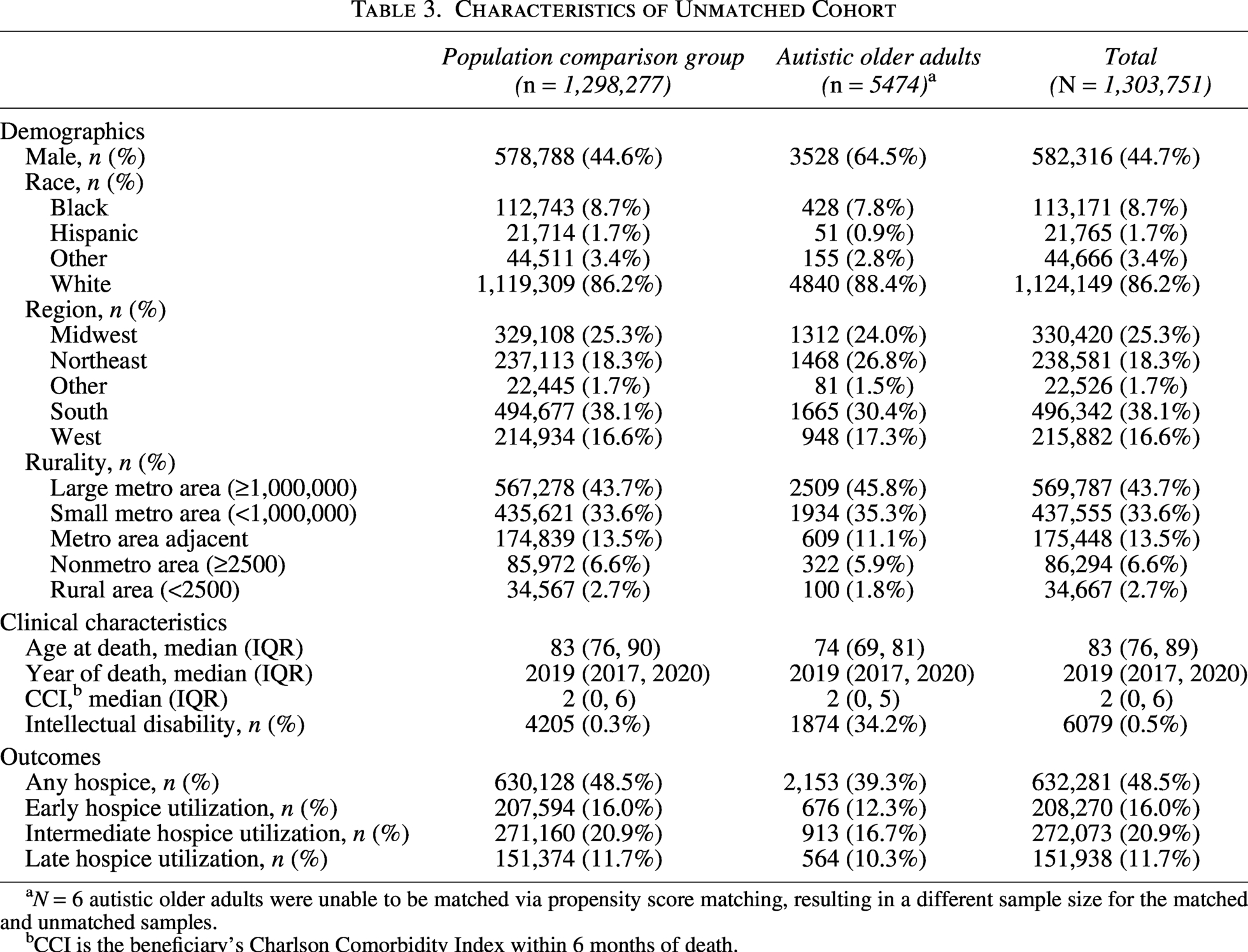
N = 6 autistic older adults were unable to be matched via propensity score matching, resulting in a different sample size for the matched and unmatched samples.
CCI is the beneficiary’s Charlson Comorbidity Index within 6 months of death.
Odds Ratios and 95% CIs Comparing Hospice Utilization Between Autistic Adults and Non-Autistic Adults Stratified by Sex, Race, and Rurality, Controlling for CCI, Age at Death, Year of Death, and Region for the Unmatched Cohort
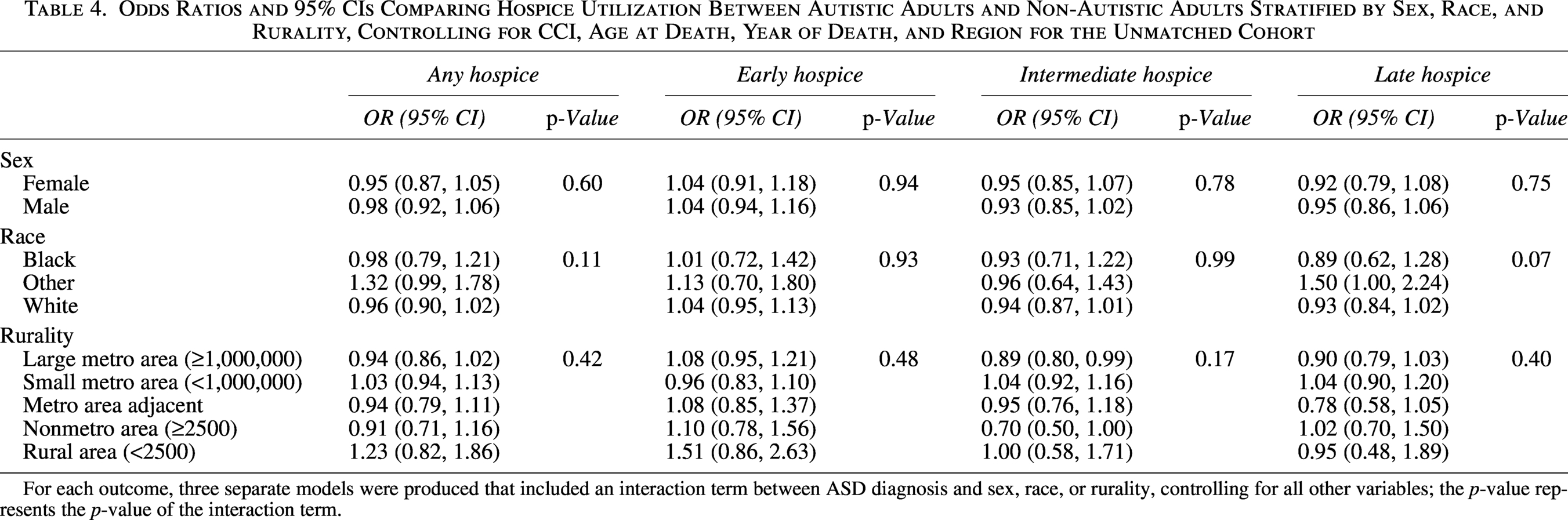
For each outcome, three separate models were produced that included an interaction term between ASD diagnosis and sex, race, or rurality, controlling for all other variables; the p-value represents the p-value of the interaction term.
Discussion
Contrary to our hypotheses, we found that Medicare-enrolled autistic older adults and older adults in our population comparison group had similar odds of hospice utilization and experienced similar timing of hospice utilization. Furthermore, we found that hospice utilization differences between autistic and population comparison beneficiaries were not moderated by sex, race, or rurality, although known disparities related to sex, race, and rurality were present in both groups. These findings suggest that Medicare-enrolled autistic older adults and their loved ones are making similar choices about accessing hospice services compared with people in the general population.
Health disparities for autistic adults may be multidimensional in that they may be driven by health care access, health care quality, biological processes, and/or social determinants of health. Although a growing body of research suggests significant and pervasive disparities in the prevalence of co-occurring physical and mental health conditions in adulthood among autistic people,2,4–6,29,30 a more limited body of research assesses disparities in health care access and utilization among autistic adults.29,31–36 Research suggests that autistic adults experience greater continuity of care within health care systems5,30 and similar levels of health insurance coverage internationally 29 compared with non-autistic adults. Some studies find less overall health care utilization, while other studies find similar or higher levels of care utilization between autistic and non-autistic adults.37,38 Findings on health care utilization disparities are thus inconclusive but may be attenuated by age such that disparities in care utilization are reduced as autistic people age. However, the quality of health care received by autistic adults is likely to be substantively worse compared with the quality of health care received by non-autistic adults.29,32,34–36,39
Our finding of a lack of disparities in utilization of hospice care among Medicare-enrolled autistic older adults may be explained by several factors. First, access to no-cost hospice care coverage through Medicare Part A (a universal benefit) may directly and mechanistically reduce health care utilization disparities for autistic older adults. This explanation would suggest that policy mechanisms that provide no-cost, universal health care coverage to all Americans may be a promising strategy for reducing health care utilization disparities among autistic older adults. More research is needed assessing whether other no-cost, universal benefits provided through Medicare, such as skilled nursing facility care, yield similar findings. Second, as seen in the bimodal distributions of age of death captured in the literature on life expectancy disparities,5,40,41 our findings may represent a bimodal distribution of both underutilization and overutilization of hospice care services that were washed out by analyses that averaged odds of receiving care. Testing this would be an excellent next step. Finally, it is also possible that there are disparities in the quality of hospice care received by older autistic adults, beyond the timing of hospice care, that cannot be evaluated using administrative data. Our findings also cannot tell us whether autistic older adults receive hospice care that meets their unique and autism-specific needs. Additional studies, including studies using qualitative data, are needed to assess autistic people’s experiences with hospice care.
Limitations and opportunities for future research
As with other studies of autistic older adult Medicare beneficiaries,4,39,40 there are some unique characteristics of administrative claims data and of our sample that should be acknowledged. First, these beneficiaries were part of the “lost generation” and were born and raised during a historical period in which access to modern diagnoses and supports for autistic people were not available. 42 As a result, our findings may not be predictive of hospice utilization among future generations of autistic older adults. Second, variables not captured within administrative claims may be associated with hospice utilization, including the quality of care provided and the extent to which the care met autistic adults’ unique needs. This data source focuses on service use, and future studies could use different data sources or prospectively collected data to examine these other variables. Third, examining longitudinal change in hospice utilization among autistic older adults was beyond the scope of the present study but is an important consideration for future work. Fourth, it is possible that some autistic older adults may have been incorrectly classified as being in the population comparison group if they did not have a formal autism diagnosis (i.e., are self-diagnosed) or did not have a health care encounter with an “institutional provider” in which an autism diagnosis code was included during the observation period. For Medicare, “institutional providers” include hospitals, hospital outpatient departments, rural health clinics, renal dialysis facilities, and outpatient rehabilitation facilities that provide service to Medicare beneficiaries. Professional service claims from noninstitutional professional providers, including physicians, physician assistants, clinical social workers, and nurse practitioners, were not included in this study. Therefore, it is possible that some autistic older adults who saw noninstitutional providers, including autistic individuals with higher support needs who receive long-term care services, may have been misclassified as belonging to the population comparison group. Finally, determining whether autistic adults who met the criteria for hospice care received hospice care was beyond the scope of this study. It is possible that some individuals who should have been offered hospice care were not, and/or that providers used different—and potentially discriminatory—criteria for deciding whether autistic older adults had a terminal health condition. Future work examining physician notes in electronic medical records has the potential to elucidate when and how providers make decisions about hospice referral for autistic older adults.
Conclusions
Given the proliferation of studies that find that autistic people experience health, health care utilization, and health care quality disparities, our findings are heartening and suggest that Medicare-enrolled autistic older adults experience similar receipt and timing of hospice care as non-autistic peers. Our findings highlight that health policies that provide zero-cost, universal benefits to all Americans may reduce health care utilization disparities among autistic older adults. It is important to note that hospice care is a personal decision that should be made by an autistic person and their loved ones. All autistic adults should be able to self-determine whether or not they want to receive hospice care and the level of medical treatments that they will receive while in hospice.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Research reported in this publication was supported by the
Authorship Confirmation Statement
L.B.: Conceptualization, methodology, resources, writing—original draft, writing—review and editing, supervision, project administration, and funding acquisition. M.N.: Data curation, formal analysis, and writing—original draft. B.J.W.: Conceptualization, funding acquisition, and writing—review and editing. B.W.P.: Conceptualization, funding acquisition, and writing—review and editing. A.L.: Writing—original draft and writing—review and editing. D.R.: Writing—original draft. E.K.: Writing—original draft. J.M.H.: Conceptualization, funding acquisition, supervision, and writing—review and editing. B.N.H.: Conceptualization, methodology, resources, writing—original draft, writing—review and editing, supervision, project administration, and funding acquisition. All the coauthors have reviewed and approved this article before submission. This article has been submitted solely to Autism in Adulthood and is not published, in press, or submitted elsewhere.
Ethical Approval
The Ohio State University’s Institutional Review Board (IRB) reviewed this study and determined that it was IRB exempt because of the use of limited datasets in analyses.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.