
Abstract
Background:
Autistic people are at significant risk for suicidal thoughts and behaviors (STBs) and nonsuicidal self-injury (NSSI). We examined STB and NSSI in different age-groups, considering sex- and age-based effects, in a pooled multinational sample of English-speaking autistic children and adults.
Methods:
We administered the Columbia-Suicide Severity Rating Scale to 245 autistic people without intellectual disability (139 youth and 106 adults; 46.1% female sex; Mage = 24.8, SDage = 16.3 years, range = 7–70) or their caregivers in Australia, Canada, and the United States. The study samples were enriched with autistic people experiencing depression and suicidality.
Results:
Most participants (87.8%) reported suicidal ideation and NSSI (56.3%). Nearly one-third of autistic people (31.0%) reported a lifetime suicide attempt (M = 2.9 attempts; range = 1–26); overdosing was the most common method of suicide attempt. Sex was not a significant risk factor for suicidal ideation, behavior, or NSSI. Increases in lifetime suicidal ideation were observed across older age-groups, with those aged over 18 years reporting more severe and longer-lasting ideation than in children or adolescents. The youngest age of suicide attempt was 7 years in this sample, and the average ages of first/initial, most lethal, and most recent suicide attempts in youth (n = 24) and adults (n = 42) were 16.6, 19.2, and 20.8 years old, respectively.
Conclusion:
Regardless of age-group, autistic people across the lifespan constitute a high-priority group for suicide prevention strategies, development of appropriate assessments, and evaluation of system-level programs that effectively address the problem of preventable death by suicide.
Community Brief
Why is this an important issue?
Suicide is a leading cause of death among autistic people and a top research and clinical priority among autistic communities. To our knowledge, most research on suicide in autistic people has been limited to one research site and a single time in development (e.g., childhood, adolescence), without consideration of suicide across different age-groups.
What was the purpose of this study?
Our international teams (i.e., Australia, Canada, and the United States) wanted to understand suicidal thoughts and behaviors (STBs) and nonsuicidal self-injury (NSSI) in verbally fluent autistic people without intellectual disability across several age-groups. We studied the most common methods of suicide attempts in this sample and how old a person was at their first, most lethal (i.e., most severe), and most recent suicide attempts. We also tested potential differences in STBs and NSSI in autistic people by sex assigned at birth and age-groups (i.e., childhood, adolescence, early adulthood, and late adulthood). By studying STBs and NSSI in a larger sample at different ages, we hope to improve assessments and interventions for suicide and self-harm risk in autistic people.
What did the researchers do?
Across our three sites, we reviewed responses from 245 autistic people and some of their caregivers about lifetime experiences of STBs and NSSI in a semi-structured clinical interview, the Columbia-Suicide Severity Rating Scale (C-SSRS; Posner et al. 29 ). Autistic people who participated in the study were from the community and those with depression and/or STB who were seeking support for their mental health. Using information from the C-SSRS, we studied the number of autistic people who reported lifetime STBs and NSSI and then checked if there were any differences based on a person’s sex assigned at birth and age-group.
What were the results of the study?
Most participants (87.8%) reported lifetime suicidal ideation/thoughts and NSSI (56.3%). Nearly one-third of autistic people (31.0%) reported a suicide attempt in their lifetime, with an average of three lifetime attempts reported by participants. Overdosing was the most common method of suicide attempt in this sample. Sex only seemed to impact the number of suicide attempts, with females reporting a slightly higher number of attempts than males. We observed some increases in lifetime suicidal thoughts across older age-groups; those aged over 18 years reported more severe and longer-lasting thoughts than children or adolescents. We found that the youngest age of suicide attempt was 7 years old, and the average ages of the first/initial, most lethal, and most recent suicide attempts in youth (n = 24) and adults (n = 42) were 16.6, 19.2, and 20.8 years old, respectively.
What do these findings add to what was already known?
Our findings show that STBs and NSSI are common among autistic people across all age-groups, beginning as early as 7 years of age. Autistic people of both male and female sexes are likely to experience STBs. We found that females may be slightly more likely to attempt suicide than males. Across age-groups, the frequency and severity of STBs and NSSI seem to increase among autistic people, with autistic people reporting overdosing as the most common method of suicide attempt.
What are potential weaknesses in the study?
Although our study examines suicide in different age-groups, our study relies on data that were collected at one timepoint versus following someone over time. By using this type of data, it may not capture the dynamic and changing nature of STBs and NSSI. Across the three sites, autistic people were recruited from different areas, such as the community or from people seeking mental health support (i.e., clinical samples), which leads to sampling differences. As a result, it is important to consider our findings with a level of caution. Furthermore, our sample of verbally fluent autistic people without intellectual disability is not representative of the suicidal experiences of all autistic people.
How will these findings help autistic adults now or in the future?
Our findings add to the existing knowledge of how common and severe STBs as well as nonsuicidal self-injurious behavior are for autistic people of both sexes and across age-groups, particularly among autistic adults. Findings also point to key areas for tailoring suicide assessment and prevention approaches to the needs of autistic people.
Introduction
Autistic people are at increased risk for suicidal ideation, attempts, and death by suicide compared with the general population.1–3 The pooled relative risk for suicide in autistic people was found to be 2.85 (95% uncertainty interval [UI] = 2.05–4.03) compared with Global Burden of Disease Study 2021 population data, contributing to an estimated 1.8% (95% UI = 1.0%–2.9%) of suicide deaths globally. 4 Over the past decade, there has been a rapidly growing literature base investigating (1) country-specific prevalence of suicidal thoughts and behaviors (STBs) among autistic people,1,2,5–7 (2) mechanisms underpinning nonsuicidal self-injury (NSSI),3,8–10 and (3) predictors and mechanisms of STB and NSSI in autistic people.11–17 However, few studies have simultaneously and comprehensively characterized STB in autistic people, particularly across age-groups. Crucially, comprehensive characterization of key correlates of STB is largely missing from current literature. Thus, to enhance assessment practices and prevention efforts for suicide in autistic people, more knowledge is needed concerning the age at which autistic people first contemplate and attempt suicide, the methods used by autistic people who attempt suicide, and whether the prevalence rates of STB and NSSI change across sexes and age-groups.
Suicide risk across age-groups
Research in the general population underscores the importance of investigating STB across age-groups (e.g., children, adolescents, young adults) not only to inform crisis assessments but also to tailor suicide prevention efforts to the unique needs of each age-group. For example, prepubescent children (5–11 years) have extremely low (completed) suicide rates in the general population: 0.6 per 100,000 for ages 5–14 years and 0.03 per 100,000 for ages 5–9 years and slightly higher rates for ages 10–11 years. 18 In adolescents and young adults, suicide is the second leading cause of death 19 ; however, rates are stratified across age-groups. A dynamic pattern across age-groups is also observed in the frequency of NSSI, with a meta-analysis by De Luca et al. identifying a peak in frequency among younger adolescents (Mage = 12.93 years), followed by stabilization in middle adolescence (Mage = 14.23 years) and decrease in older adolescents (Mage = 15.53 years). 20
Despite the promise of emerging research on suicide risk across age-groups in non-autistic populations, this research has not been extended to autistic people. An extension of this work to autistic people is important as some developmental experiences (e.g., puberty and cognitive and motor development) occur differently, or may be delayed, in this population.21,22 Research is therefore required to determine whether age-based differences associated with STB and NSSI observed in non-autistic populations are also observed within the autistic population.
Sex effects on suicide risk
In the general population, sex assigned at birth confers differential risks for STB such that some studies suggest that female sex is associated with elevated risk for both suicide ideation and attempts.4,23 In terms of autistic people, findings on sex-based differences in STB and NSSI are mixed. One study reported a higher risk of STB among autistic females in pooled estimates from both population-based and clinical samples (odds ratio = 1.96; 95% confidence interval [CI] = 1.5–2.5). 23 However, in the same study, people of male sex are 2.5 times more likely to die by suicide than people of female sex (hazard ratio [HR] = 2.50; 95% CI = 1.8–3.6). 23 A recent systematic review and meta-analysis utilizing data from the Global Burden of Disease Study 2021 found that autistic females had a greater risk (relative risk [RR] = 3.85, 95% UI = 2.71–5.40) of suicide compared with autistic males (RR = 2.13, 95% UI = 1.54–3.01; b = 0.60, p < 0.001). 4 At the same time, others have highlighted the importance of continued research on potential sex differences in risk of STB among autistic people. 24
Consideration of sex effects in the context of autistic people is particularly pertinent given the substantial sex imbalances in this population and associated psychopathology. 25 Compared with same-sex non-autistic people, a Swedish population-based cohort study found that young (16–24 years) autistic females had a significantly higher relative risk for psychiatric hospitalizations and diagnoses than autistic males, including self-harm (HR = 2.21, 95% CI = 2.00–2.46, p < 0.001). 26 Consistent with this finding, a higher percentage of autistic girls than boys (12–18 years) present at psychiatric emergency services for suicide and self-harm; however, for both sexes, risk of suicide or self-harm was the most common reason for referral to services. 27 A smaller study from the United States 28 used the Columbia-Suicide Severity Rating Scale (C-SSRS 29 ) to characterize STB and NSSI in a community sample of autistic (n = 138) and non-autistic (n = 101) early adolescents aged 10–13 years. Higher instances of suicidal ideation and NSSI, but not suicidal behavior, were reported by autistic youth compared with non-autistic youth; however, no sex-based differences in prevalence rates of STB or NSSI were observed, 28 which raises the question as to whether sex effects in suicide risk emerge later in development for autistic people. Even among youth in crisis, elevated autistic traits may confer additional risk for suicidal thoughts 30 ; however, continued research in this area is needed. Thus, increasing understanding of sex and gender differences in suicide among autistic people is a crucial area. 24
Current study
In the present study, we examined multiple aspects of STB (e.g., prevalence, age at first attempt, methods/means) and the prevalence of NSSI in a large autistic sample without intellectual disability from three Anglophone countries (Australia, Canada, and the United States) with considerations of sex- and age-based differences. Specifically, we aimed to (1) examine frequencies of lifetime STB in the total sample, (2) test sex-based differences in lifetime STB, and (3) determine age-based differences in lifetime STB in autistic people of male and female sex spanning from children to adults. To report all findings from the C-SSRS, we explored the prevalence of NSSI in the total sample and between the sexes and age-groups; however, NSSI was assessed with a singular item on the C-SSRS, and thus, findings are limited to prevalence and to be interpreted with caution. Based on previous research showing increased prevalence of STB in autistic populations compared with general populations, gender,1–4 and, in non-autistic populations, developmental influences,18,20 we hypothesized that (H1) STB would be common across our samples; (H2) in our sample, the prevalence and severity of STB would not differ by sex; and (H3) prevalence and severity of STB would increase over age-groups with the highest acuity among autistic adults. Furthermore, we hypothesized that the presence of NSSI would be elevated in the total sample.
Methods
Our study was a secondary data analysis of pooled data from three research studies from Australia, Canada, and the United States that used different recruitment strategies for different purposes; it is important to interpret our findings with this perspective. Of note, this is a suicide-enriched sample that is not representative of a neutral population sample, and thus, findings should be interpreted with this perspective. All studies were approved by the relevant university ethics committees at La Trobe University (Australia), University of Calgary (Canada), and Vanderbilt University (USA), and all participants provided informed consent.
Participants
We characterized lifetime STB and NSSI in 245 autistic people without intellectual disability (139 youth and 106 adults; 46.1% female sex; Mage = 24.78, SDage = 16.25 years, range = 7–70) using self- and caregiver-reported versions of the C-SSRS. We provided demographic data for the total sample in Table 1. For the Australian sample, autistic adults self-reported a formal diagnosis of autism from a qualified health professional. For the Canadian sample, the research team confirmed autism diagnostic status through caregiver-reported formal diagnosis of autism from a qualified health professional. For the U.S. sample, clinicians confirmed autism diagnostic status by review of medical records and administration of autism diagnostic assessments (e.g., Autism Diagnostic Observation Schedule, Second Edition, 31 Social Communication Questionnaire, 32 Social Responsiveness Scale, Second Edition, 33 and clinical judgment based on diagnostic criteria in the Diagnostic and Statistical Manual of Mental Disorders, 5th edition). 34
Sample Demographics of Total Sample (N = 245) and by Site (Australia, Canada, and the United States)
Birth country from autistic adults in Australia in lieu of race.
SD, standard deviation.
There was a marked discrepancy between income for the Australian sample compared with the samples from Canada and the United States, with 58% of the Australian sample reporting an income less than AUD35,000. This discrepancy is likely explained by the autistic adults in the Australian sample reporting their own income, whereas income for the Canadian and U.S. studies corresponded to that of family or caregivers.
Procedure
Each site examined STB and NSSI in autistic people without intellectual disability using the lifetime version of the C-SSRS. 29 The Australian research team recruited participants between October 2020 and June 2021 from one of two national longitudinal studies on autism, which recruited broadly from the general Australian autistic population.35,36 Participants responded to an advertisement in an emailed newsletter sent to all participants in the two national longitudinal studies, with the study advertised as pertaining to “mental health, wellbeing, and suicide prevention in autism.” Interested individuals first registered their interest in the study via REDCap 37 and were contacted by a member of the research team to determine interest and eligibility. Inclusion criteria included adults (a) 18 years or older, (b) identifying as autistic or having a diagnosis of autism, (c) comfortable reading or speaking English, (d) without a diagnosis of an intellectual disability, and (e) participating in one of the longitudinal studies (to enable linkage with previous data). During the study visit, the research team administered the C-SSRS via face-to-face Zoom interview to autistic adults as part of a larger mixed-method follow-up study on mental health and STB in autism. Author M.U., a trained medical doctor, reviewed the C-SSRS coding. Australian participants received up to AUD100 in vouchers.
For the Canadian sample, the research team recruited caregivers of autistic children and young people (7–24 years) with a history of STB from outpatient clinics in which they were receiving mental health services or an existing database of autistic youth who consented to be contacted for research purposes. Interested caregivers first contacted the research team via email, and if they were eligible, they were asked to complete an online consent form and questionnaire regarding their child’s/youth’s STB history. Specifically, caregivers completed a modified caregiver-reported questionnaire version of the C-SSRS (described in more detail below), and coded responses were all reviewed by a licensed clinical psychologist (author C.A.M.). Although the C-SSRS has not been previously modified in this way, caregiver-reported measures of suicide have been shown to be valid and reliable. 38
Autistic adolescents in the United States presented for psychiatric services (e.g., autism diagnostic evaluations, psychotherapy, and medication management) at the Psychiatry Autism Research Team clinic at Vanderbilt University Medical Center. In the intake appointment, families provided verbal and written consent/assent for these services, which included the use of interviews and questionnaires. The C-SSRS was administered to all adolescents by a trained clinician and separately from their caregivers. We recorded adolescent responses to the C-SSRS on REDCap. All families provided clinical data that could be deidentified and used for research purposes with approval from the Vanderbilt Institutional Review Board (IRB). For the present study, we analyzed deidentified data from intake appointments between January 2021 and December 2022 in accordance with approval from the IRB at Vanderbilt University (Protocol #211870). The IRB approved a waiver of consent to extract deidentified data from the clinical intake battery for research purposes. Although the Psychiatry Autism Research Team clinic provides psychiatric services to autistic and other neurodivergent youth with different communication and intellectual abilities, we extracted deidentified clinical data only from youth who met the following inclusion/exclusion criteria for the present study: (a) 11:00–17:11 years old, (b) with a diagnosis of autism, (c) without intellectual disability, and (d) comfortable reading and writing in English.
Across sites, the interviewers completed the online C-SSRS training offered by the Columbia Lighthouse Project 29 and received ongoing supervision and consultation in administration, scoring, and safety planning from experienced administrators or researchers of the instrument. All sites developed and implemented detailed risk assessment and intervention procedures for managing suicide risk39,40 including, but not limited to, ways to identify warning signs of crisis, use coping strategies, reach out to social supports (if helpful), contact professional supports (e.g., counselors, psychiatrists, etc.), and use 24/7 crisis hotlines (e.g., 988 in the United States). All participants were alive at the time of the C-SSRS interview (i.e., no caregivers were reporting on individuals postmortem), and no deaths were reported across sites.
Measures
Demographics
Participants reported demographic information on standard surveys. The research teams collected education level, employment status, annual household income, race, and birth country from caregivers of autistic youth (Canada and the United States; see Table 1) and autistic adults (Australia).
Columbia-Suicide Severity Rating Scale
The C-SSRS 29 is a brief, semi-structured interview designed to screen for the presence of STB and NSSI; we administered the lifetime version to all participants across the three sites. The C-SSRS is comprised of dichotomous yes/no items to assess the presence of suicidal ideation, NSSI, and suicidal behavior. For positive screens (i.e., endorsed yes on any of the initial items), follow-up questions are administered to categorize the severity/intensity, actual lethality, and/or potential lethality of STB. For the lifetime version of the C-SSRS, participants are asked if they have ever experienced STB at any point in their lifetime, with specific questions related to a time they felt the most suicidal (e.g., thinking about how they might end their life). We recorded the number of attempts (count variable) if a participant endorsed a lifetime suicide attempt/s. The C-SSRS shows initial reliability in assessing for suicide risk in autistic people. 28 Of note, the C-SSRS contains one dichotomous item about the presence/absence of current or lifetime NSSI; detailed information on NSSI (e.g., type, triggers) is not collected in the C-SSRS and, thus, not included in the present study.
We obtained the Canadian sample using an adapted version of the C-SSRS to allow for caregivers to report on their child’s suicidality experiences (see Supplementary Data for the modified version). Specifically, we changed the first-person statements to third-person statements (e.g., “Have you wished you were dead or wished you could go to sleep and not wake up?” to “Has your child ever wish he/she were dead or wished he/she could go to sleep and not wake up?”). We first asked caregivers a screening question, “Has your child ever experienced any form of suicidal thoughts or behaviors?” If caregivers answered “no,” the form was completed. An answer of “yes” would redirect caregivers to items from the modified C-SSRS. We collected all data in REDCap, a secure, online survey platform.
For participants in Australia and the United States who attempted suicide, we recorded the methods/means of attempt (e.g., overdosing, suffocating) and participant ages at the initial, most recent, and most lethal attempts.
Data analysis
We carried out all analyses in the R statistical computing environment (R version 4.4.1 41 ). We fit statistical models 42 in a Bayesian framework using the brms R package,43,44 which implements Hamiltonian Monte Carlo sampling 45 via the Stan probabilistic programming language. 46 We used additional custom functions programmed by author Z.J.W. (publicly available in the ZPack.Bayes library 42 ) extensively in the present analyses.
Descriptive models
To summarize the sample, we reported raw descriptive statistics (i.e., mean and SD or percentage endorsement) for most parameters of interest. However, as data in the present study were sourced from three separate datasets representing substantially different populations, we sought to eliminate the effects of collection site imbalances on sample-average descriptive statistics to the extent possible. To this end, we fit a series of intercept-only Bayesian hierarchical models with a random intercept term for the site. These models utilized (1) a Bernoulli likelihood (probit link) for dichotomous data; (2) a cumulative likelihood (probit link) for ordinal data; (3) a zero-inflated negative binomial likelihood (log link for p and r, logit link for zero-inflation parameter) for count data; and (4) a skew-normal likelihood (log link for sigma) for continuous data. Continuous variables were normalized (Z-scored) before model fitting.
For the descriptive models examining the lethality of attempts, we fit slightly more complex models that included all three types of suicide attempts (first attempt, most recent attempt, and most lethal attempt) as a categorical fixed effect, with the random-effects structure expanded to include not only a random intercept by site but also (1) a random intercept by person (nested within site), (2) a random slope for attempt type by site, and (3) a random slope for attempt type by person (nested within site). Default brms priors were used in all cases, with the exception of a Student-t3(0, 2.5) prior on all intercepts, a Normal(0, 1) prior on all regression slopes, and a Lewandowski–Kurowicka–Joe(η = 2) prior on correlation matrices.
We estimated models in brms using 20,000 postwarmup Monte Carlo draws from 10 separate Markov chains. From each descriptive model, we used the posterior_predict function from the brms function to simulate a full conditional posterior predictive distribution of the variable of interest with the “site” variable converted to a hypothetical unobserved variable and the new level’s posterior draws taken at random from all posterior draws of all other levels (“uncertainty” sampling used for new levels). 47 From these posterior distributions, we summarized parameters of interest (e.g., proportion endorsement of a given response category, mean age, and median number of suicide attempts) using the posterior median and 95% highest-density credible interval (CrI). 48 We presented raw descriptive statistics for each parameter along with the simulated descriptives from the (conditional) posterior predictive distribution.
Predictive models
To examine age and sex effects on C-SSRS outcomes while controlling for site effects, we fit a series of six Bayesian hierarchical models for each outcome, performing a model-selection procedure to determine the most appropriate age and sex terms to include in the model. For each STB outcome, the following models were fit: (1) a baseline model, including no age or sex term (only a random intercept by site); (2) a model including a fixed effect of sex but no effect of age (including a random slope for sex and random intercept by site); (3) a model including a fixed effect of age but no effect of sex (including a random slope for age and random intercept by site); (4) a model with fixed effects of both age and sex (including random slopes for both age and sex by site, as well as a random intercept by site); (5) a generalized additive model with a smooth term (thin plate regression spline) for age but no effect of sex (including a random slope for age and random intercept by site); and (6) a generalized additive model with a smooth term for age and a fixed effect of sex (including random slopes for both age and sex by site, as well as a random intercept by site). As with descriptive models, we normalized all continuous variables before model fitting. We used the same likelihood functions for different variable types as in the descriptive models, and model priors included a Student-t3 (0, 2.5) prior on all intercepts, a Normal(0, 1) prior on all regression slopes, a half-Student-t3 (0, 2.5) prior on all random-effect SDs, a Lewandowski–Kurowicka–Joe (η = 1) prior on correlation matrices, and Student-t3 (0, 2.5) priors on the sds parameter of the smooth term.
We performed model selection using approximate leave-one-out cross-validation based on Pareto-smoothed importance sampling (PSIS-LOO), 49 as implemented in the loo R package. The PSIS-LOO-based pseudo-Bayesian-model-averaging process (with Bayesian bootstrap for variance stabilization) described by Yao et al. 50 (denoted PseudoBMA+ and implemented in the loo_model_weights function) was used to generate model weights for the six candidate models. Furthermore, in the tradition of classical Bayesian model averaging, 51 we calculated pseudo-Bayes factors for each candidate model (pBFmodel; based on uniform prior model probabilities of 0.1667 each), as well as inclusion pseudo-Bayes factors (pBFinc; representing the evidence for each term [any age term, linear age term, nonlinear age term, sex term] being included in the final model, averaged over the entire sampled model space). We also reported raw posterior probabilities of each model or variable inclusion (Pmodel and Pinc, respectively) to help interpretation. The sum total of these indices was used to decide on a single model of the six, the parameters of which were interpreted and used to determine the presence/absence and functional form of age and sex effects.
Results
Lifetime STB and NSSI in total sample
We present lifetime STB and NSSI data for the total sample from the C-SSRS in Table 2. Most participants reported experiencing a wish to be dead at some point in their life (n = 215; 87.8%; model estimate: 96.7%, CrI95% [93.1, 99.2]). Approximately one-third of the sample (n = 88; 35.9%; model estimate 55.5%, CrI95% [44.1, 66.5]) endorsed the highest level of suicidal ideation in their lifetimes, consisting of both a specific plan and an intent to act on it. Nearly half of autistic people (n = 116; 47.3%; model estimate 48.6%, CrI95% [18.9, 95.3]) who experienced lifetime suicidal ideation reported that the reasons for the ideation were mostly or completely to end or stop the pain. Over half of autistic people (n = 138; 56.3%; model estimate 56.3%, CrI95% [43.3, 71.4]) endorsed lifetime NSSI. Nearly one-third of autistic people (n = 76; 31.0%; model estimate 28.6%, CrI95% [14.3, 48.2]) reported a lifetime suicide attempt with an average of 2.92 lifetime attempts (range = 1–26 attempts; model-estimated average attempts 3.53, CrI95% [2.40, 5.08]) among those who attempted suicide. The earliest age of reported suicide attempt was 7 years old in this sample. Among autistic youth and adults in Australia and the United States with lifetime suicide attempts (n = 66), the average ages of an individual’s first/initial, most lethal, and most recent attempts were 16.56 years old (SD = 8.23; range: 7–45; model-estimated mean age 18.29 years, CrI95% [15.85, 21.03]), 19.18 years old (SD = 9.16; range: 9–45; model estimate [13.94, 26.63]), and 20.77 years old (SD = 10.19; range: 9–45), respectively. Some autistic people reported an interrupted attempt (n = 31; 13.9%; model estimate 13.5%, CrI95% [2.7, 22.0]), aborted attempt (n = 31; 13.9%; model estimate 11.3%, CrI95% [0.0, 25.2]), and/or preparatory acts (e.g., collecting pills, writing a suicide note; n = 41; 16.3%; model estimate 17.2%, CrI95% [3.3, 32.6]).
Frequencies and Model-Based Category Predictions of Lifetime Suicidal Thoughts and Behaviors and Nonsuicidal Self-Injury from the C-SSRS in the Total Sample
Category predictions are based on a posterior predictive (intercept-only) model with an outcome-specific likelihood (i.e., Bernoulli for binary, cumulative for ordinal, zero-inflated negative-binomial for count, and skew-normal for continuous) and a random intercept for site (different model used for methods/means outcomes; see main text for more details). The new data for the posterior predictive draws include the same predictor values as the existing data used to fit the model except site, which was recorded as an unobserved value (same for all datapoints), and the sample_new_levels = “uncertainty” option within brms was used to combine posterior draws across all levels of existing sites for this new level. Because of this additional uncertainty, predicted category proportions could sometimes deviate quite substantially from the observed category proportions.
“Levels” of lethality are as follows: 0. No physical damage or very minor physical damage (e.g., surface scratches); 1. Minor physical damage (e.g., lethargic speech; first-degree burns; mild bleeding; and sprains); 2. Moderate physical damage; medical attention needed (e.g., conscious but sleepy, somewhat responsive; second-degree burns; and bleeding of major vessel); 3. Moderately severe physical damage; medical hospitalization and likely intensive care required (e.g., comatose with reflexes intact; third-degree burns less than 20% of body; extensive blood loss but can recover; and major fractures); 4. Severe physical damage; medical hospitalization with intensive care required (e.g., comatose without reflexes; third-degree burns over 20% of body; extensive blood loss with unstable vital signs; and major damage to a vital area); and 5. Death. No deaths occurred, and therefore the “Death” level is omitted from the table.
Data only available from participants in Australia and the United States.
Only completed if actual lethality was no physical damage or very minor physical damage (e.g., surface scratches).
CrI, credible interval; C-SSRS, Columbia-Suicide Severity Rating Scale; NSSI, nonsuicidal self-injury; SD, standard deviation.
In terms of the lethality/medical damage of actual attempts, moderate-severity damage (i.e., damage severe enough to warrant medical attention, such as being sedated after an overdose, damaging a major blood vessel, or causing second-degree burns) or more was reported in 26 of the 93 autistic people with a recent suicide attempt (28.0%; model estimate 41.9% [32.3, 55.9]), with slightly lower rates of moderate-or-higher lethality for the first attempt (n = 18/65; 27.7%; model estimate 35.4% [26.2, 50.8]) and necessarily higher rates for the most lethal attempt (n = 26/61; 42.6%; model estimate 55.7% [45.9, 68.9]). Overdosing was the most common method/means of suicide attempt.
Age and sex effects on lifetime STB and NSSI
Model selection coefficients can be found in Table 3. When examining the ordinal level of suicidal ideation over the lifespan, pseudoBMA+ based on PSIS-LOO demonstrated that the model with the best predictive power was one with no sex effect included and a nonlinear effect for age (PModel = 0.714, pBFModel = 12.5). This model was broadly supported by the pseudo-inclusion Bayes factors, which demonstrated strong evidence in favor of any age term (PInc = 0.980, pBFInc = 25.0), strong evidence against a linear age effect (PInc = 0.007, pBFInc = 0.014), strong evidence for a nonlinear age effect (PInc = 0.973, pBFInc = 72.9), and slight-to-ambiguous evidence against a sex effect (PInc = 0.267 pBFInc = 0.365). Graphical examination of the nonlinear age trend (Fig. 1A) demonstrated that the “level” of lifetime suicidality increased with age-group through childhood and early adulthood, reaching an asymptote in the late 20s and staying at a constant level for most of adult life before beginning to decline between ages 55 and 70. A similar predictive model (no sex term and nonlinear age term) was selected to describe the presence of NSSI (binary Yes/No ever present) in the sample (PModel = 0.570, pBFModel = 6.62), again supported by pBFInc values (any age effect: PInc = 0.951, pBFInc = 9.73; linear age effect: PInc = 0.025, pBFInc = 0.052; nonlinear age effect: PInc = 0.926, pBFInc = 24.9; sex effect: PInc = 0.398, pBFInc = 0.660). Graphical inspection of the nonlinear trend (Fig. 1B) demonstrated that the likelihood of lifetime NSSI increased over the course of childhood/adolescence to a peak in the early 30s, afterward declining to the lowest probability in individuals in their 50s, increasing slightly in frequency between ages 50 and 70.
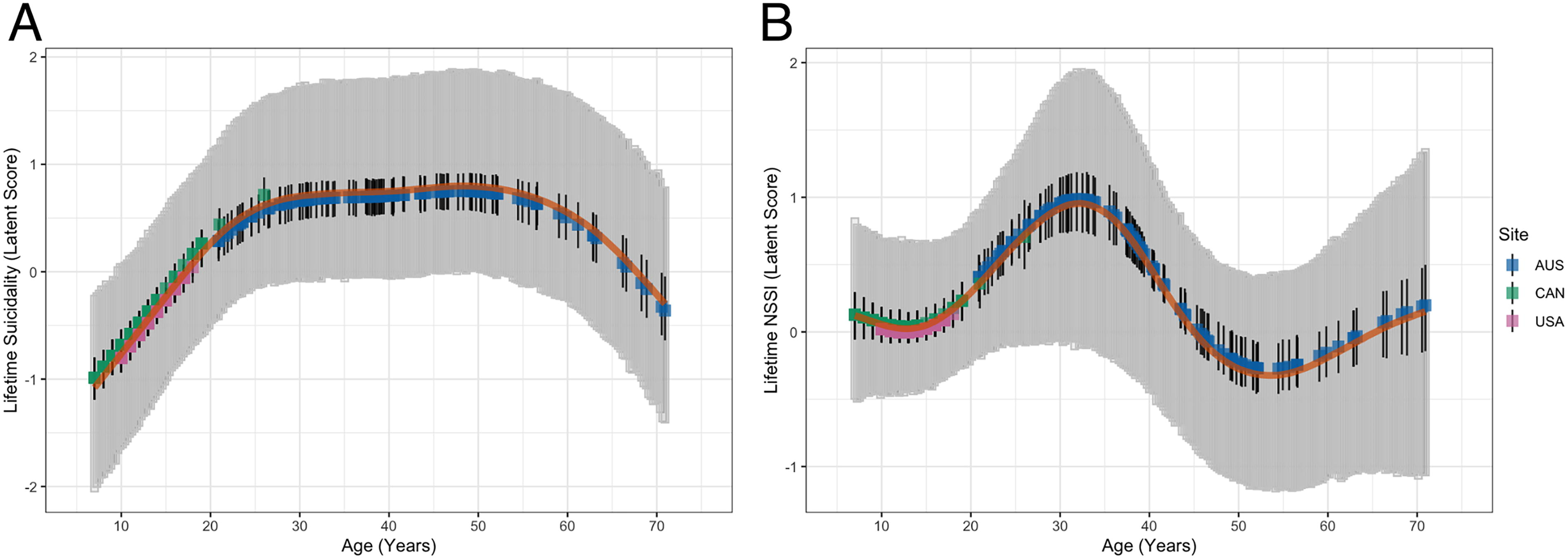
Nonlinear age trends for
Estimated Log Posterior Density, Posterior Model Probability, and Pseudo-Bayes Factor Averaging for Each Candidate Model Assessed in Pseudo-Bayesian Model Averaging
elpdloo, expected log pointwise predictive density; PModel, posterior model probability; pBFModel, pseudo-Bayes factor for model (based on pseudo-Bayesian model averaging with weights based on approximate leave-one-out cross validation and Bayesian bootstrapping); NSSI, nonsuicidal self-injury; SI, suicidal ideation. Note: Bold indicates the model with the best predictive power.
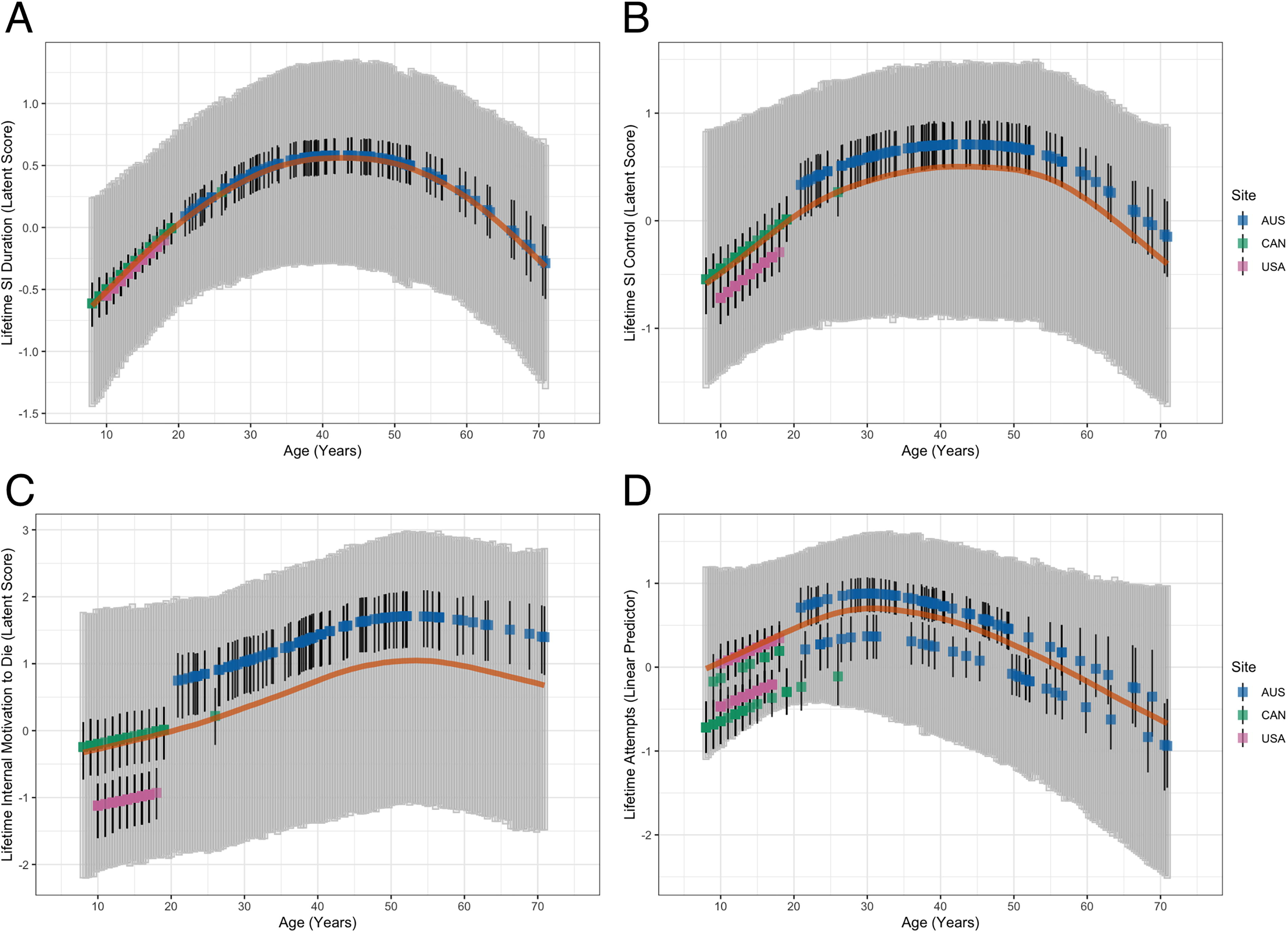
Notably, other outcome models demonstrated somewhat different combinations of effects. When examining the effects of age and sex on suicidality severity indicators, the suicidal ideation frequency item demonstrated the baseline model (i.e., random intercept-only) as the most suitable model based on PseudoBMA+ (PModel = 0.352, pBFModel = 2.72). Although somewhat more ambiguous, inclusion pseudo-BF values still demonstrated a pattern of results in line with these findings (any age effect: PInc = 0.408, pBFInc = 0.345; linear age effect: PInc = 0.155, pBFInc = 0.367; nonlinear age effect: PInc = 0.253, pBFInc = 0.677; sex effect: PInc = 0.393, pBFInc = 0.649). Alternatively, the suicidal ideation duration item was best explained by a no-sex/nonlinear-age model (PModel = 0.510, pBFModel = 5.20), with clear support from inclusion pseudo-Bayes factors (any age effect: PInc = 0.764, pBFInc = 1.62; linear age effect: PInc = 0.060, pBFInc = 0.128; nonlinear age effect: PInc = 0.704, pBFInc = 4.76; sex effect: PInc = 0.294, pBFInc = 0.415). Graphical inspection of the nonlinear age trend for duration demonstrated an inverse U-shaped relationship, with a peak at approximately age 40 (Fig. 2A).
Nonlinear age trends for
The same no-sex/nonlinear-age model was also found to fit best for control over suicidal ideation (PModel = 0.374, pBFModel = 2.98), with moderate support from inclusion pseudo-Bayes factors (any age effect: PInc = 0.650, pBFInc = 0.930; linear age effect: PInc = 0.138, pBFInc = 0.321; nonlinear age effect: PInc = 0.512, pBFInc = 2.10; sex effect: PInc = 0.275, pBFInc = 0.379). A similar inverted U-shaped curve was demonstrated for control over SI, with a flattened peak maximal between 30 and 50 years of age (Fig. 2B). With regard to deterrents for suicidal ideation, the baseline model was found to be slightly preferred in the model selection (PModel = 0.310, pBFModel = 2.24), with ambiguous inclusion pseudo-Bayes factors that provided limited support for or against any age term and slight evidence against a sex effect (any age effect: PInc = 0.547, pBFInc = 0.605; linear age effect: PInc = 0.306, pBFInc = 0.880; nonlinear age effect: PInc = 0.242, pBFInc = 0.638; sex effect: PInc = 0.315, pBFInc = 0.461).
As a final ideation severity item, reasons for ideation (more severe being for internal reasons such as ending suffering and less severe being for external reasons such as causing harm to others) demonstrated a no-sex/nonlinear-age model, similar to the previous duration and control models (PModel = 0.255, pBFModel = 1.71). Notably, the baseline model fit the data nearly as well in this case (PModel = 0.235, pBFModel = 1.53), and inclusion pseudo-Bayes factors provided somewhat limited support for either pattern of coefficients (any age effect: PInc = 0.636, pBFInc = 0.873; linear age effect: PInc = 0.229, pBFInc = 0.595; nonlinear age effect: PInc = 0.407, pBFInc = 1.37; sex effect: PInc = 0.366, pBFInc = 0.578). Graphical examination of the nonlinear age trend demonstrated yet another (albeit flatter) inverted U-shaped relationship, with a peak near the late 40s/early 50s and decline thereafter (Fig. 2C).
As a final outcome, we also examined the total number of suicide attempts using a zero-inflated negative-binomial model; in this case, model selection indicated that the model with a sex term and a nonlinear age effect was the best-fitting to the data (PModel = 0.311, pBFModel = 2.26). Inclusion pseudo-Bayes factors supported this conclusion, although evidence for the sex effect was somewhat limited (any age effect: PInc = 0.816, pBFInc = 2.21; linear age effect: PInc = 0.230, pBFInc = 0.598; nonlinear age effect: PInc = 0.585, pBFInc = 2.82; sex effect: PInc = 0.563, pBFInc = 1.29). Notably, the effect of sex did demonstrate a 95% CrI that intersected the point null hypothesis [Incidence Rate Ratio (IRR) = 1], but there was still a greater than 95% posterior probability that male participants demonstrated a lower overall rate of suicide attempts than female participants when controlling for age and site (IRR = 0.599, CrI95% [0.330, 1.054], Pd = 0.958). Graphical inspection of the nonlinear effect of age demonstrated another inverted U-shaped curve, increasing with age up until approximately 30 years of age and decreasing thereafter (Fig. 2D).
Discussion
Our multisite, multinational study is one of the first to characterize STBs and the prevalence of NSSI simultaneously in autistic people without intellectual disability across a wide age range, additionally examining the presence of both linear and nonlinear age effects. Of note, this is a suicide-enriched sample, and thus, findings should be interpreted with this perspective. Overall, lifetime experiences of STB were common across the sample; almost one-third of participants reported at least one suicide attempt, and among those having attempted suicide prior, the average number of attempts was nearly 3 with a maximum of 26 (in one individual). Almost 60% of autistic people experienced some physical damage resulting from the attempt, and moderate-to-severe damage was present in over 25% of all attempts, regardless of category. Sex differences in STB were exceedingly minimal, with most outcomes demonstrating no convincing evidence for sex effects; only the number of suicide attempts indicated a slight female predominance that would have been of borderline “significance” if evaluated in a frequentist hypothesis-testing framework (i.e., Pd > 0.975 approximates p < 0.05 if CrIs are treated as frequentist CIs).
We additionally found a trend of increasing severity of suicidal ideation over the age-groups, with those aged over 18 years reporting more severe and longer-lasting ideation than in children or adolescents. Curvilinear effects were common in our data and variably demonstrated peaks in the age curve from young adulthood to late middle age. However, given that the outcomes being studied were lifetime prevalence or severity estimates, decreasing effects with age are likely to reflect a statistical artifact, such as ascertainment bias for the older-aged participants (perhaps due to completed suicides, lower research participation rates, or less likelihood of diagnosed autism in elderly individuals with the most severe STB), as similar effects would be impossible in a truly longitudinal cohort. There is also a possibility of secular changes in STB with time (i.e., cohort effects), as participants who are now in middle age could simply have a more severe depressive/suicidal phenotype over their lives than those of the previous cohort; however, this remains to be empirically demonstrated. A final possibility is that of reporting bias from older individuals, which could indicate (particularly when one’s “worst ever” experience of suicidal thoughts or behavior was decades prior, as indicated by “most lethal” attempts typically being in one’s 20s even for older cohorts) a tendency to underreport the presence or severity of certain experiences that are more remote in one’s life. 52
Across the full sample, the youngest age of suicide attempt was 7 years old, the average age of first suicide attempt was 16 years old, and the average age of the attempt with the greatest potential lethality was 19 years old. Overall, overdose was the most common means of attempting suicide within the sample, with cutting and suffocation also common. In younger children (i.e., 7–12 years), stepping into traffic was a commonly reported method for suicide attempts. Given the stated differences in sampling across sites and cross-sectional nature of all data, it is critical to interpret findings with caution. Further large-scale studies that sample STB as a “current” symptom longitudinally (while still accounting for meaningful cross-site differences) will be necessary to accurately determine the demographic predictors of these impactful symptoms across the life course of autistic people.
Our findings are consistent with research indicating a significantly increased risk of STB1,4 and NSSI9,10 in the autistic population, as well as similar rates and characteristics of STB and NSSI in autistic males and females.4,7 However, we did find evidence of marginal increases in the number of lifetime suicide attempts in autistic people assigned female sex at birth (combined with the very small number of individuals who reported an intersex identity) as compared with males after controlling for age and site-related differences. Although imprecise in effect size and potentially consistent with both small/trivial and moderate effects at the population level, there are multiple likely explanations for this sex difference. First, there is a known sex difference in the prevalence of lifetime depressive disorders in autistic individuals,4,7 which potentially increases the possibility of suicide risk over the course of a lifetime in females over males when such conditions are not controlled for. Second, there are other quite significant female-predominant sex imbalances in co-occurring medical and/or psychiatric conditions that may greatly increase one’s risk of attempting suicide, such as chronic pain disorders (e.g., fibromyalgia and hypermobile Ehlers–Danlos syndrome)54,55 and borderline personality disorder (BPD).56,57 Although frequently misdiagnosed in the autistic population,58,59 reports of genuinely co-occurring autism and BPD are present in the literature,60,61 and it is likely that the presence of both conditions could occur in our sample (which would, in the case of BPD, potentially be a female-biased condition in autistic people given the majority of epidemiological evidence to date56,62 on this topic). Given the excessive risk for additional suicide attempts that a diagnosis of BPD confers (i.e., as the strongest diagnostic predictor of such attempts in well-controlled prospective models 63 ), even a doubling of the risk of BPD by sex in autistic people may have pronounced effects on the number of lifetime suicide attempts seen across sex-based groups. More thorough work to establish this phenotype as a relevant contributor (or not) to sex differences in suicidality in the autistic population is needed, particularly given the high degree of stigma and misdiagnosis surrounding the BPD diagnosis in autistic people and the substantial likelihood that individuals with genuine autism-BPD co-occurrence are being underdiagnosed and undertreated in community settings.
Other sampling differences, and particularly differences between the three sites, were quite relevant to our analyses. Although models sought to account for these with site-specific effects, it remains important to be transparent about the ways in which participants systematically differed between these samples. A major difference between sites was age, in which autistic participants in Australia were all adults, whereas the U.S. sample was exclusively pediatric and the Canadian sample was predominantly (but not exclusively) pediatric. Furthermore, as autistic youth sampled in the United States comprised a clinical cohort (as opposed to those recruited into research studies in the other two cohorts), sampling bias may contribute to the higher prevalence of STB and NSSI among autistic youth in the current sample than the prevalence rates among same-age autistic youth in a separate community sample reported by Schwartzman et al. 28 Alternatively, most autistic youth in the United States were seeking treatment for their depression, anxiety, or SI, and mean-level severity did not appear lower than the comparable-aged Canadian cohort, who may not have been as actively involved in treatment despite being recruited for research on a similar topic. Lastly, the mean income (USD equivalent) and income inequality (Gini coefficients; higher numbers associated with less inequality) indicate differences in income inequality and income between the three samples, with Canadian and U.S. data having the highest frequency of cases associated with the highest income. As noted previously, this discrepancy may be explained by autistic adults in the Australian sample reporting their own income (instead of family/caregiver), which is consistent with the high levels of under- and unemployment within the autistic adult population, 64 thereby indicating differences in socioeconomic status between samples. Although site differences provide a limitation, as they cannot be fully overcome with statistical control and may lead to confounds of site and other variables in doing so, we strongly recommend that all other multisite studies seek to utilize similar random-effects models in the future that consider the origin of the data when analyzing large-scale data such as these.
With limited information on gender in our sample, we were unable to examine gender-based (rather than sex-based) differences in risk for STB and NSSI; however, it is a critical area for investigation as risks for STB and NSSI are common in transgender/gender diverse people, 65 many of whom identify as autistic; 66 autistic transgender/gender diverse people are at increased risk of STB compared with their cisgender autistic peers.3,67 With recent calls to increase research efforts for autistic people assigned female at birth,68–70 our findings add to the importance of this work and highlight the need to better understand pathways to suicide risk in this cohort.
Another finding was that over half of the sample reported lifetime NSSI on the C-SSRS. As the C-SSRS contains only one item about NSSI, insights are limited to the presence/absence of NSSI in this sample; more research is needed to better understand the mechanisms underpinning NSSI in autistic people. Furthermore, the NSSI question on the C-SSRS does not distinguish between self-harm in the context of autism (i.e., self-injurious stereotypy) or distress (i.e., “classical” NSSI), which is an ongoing area of continued research. Given the limited information of NSSI from the C-SSRS and the cross-sectional nature of this study, we cannot investigate potential associations (or not) between NSSI and suicide risk in this population; however, this remains a critical area of future research. In fact, multimethod assessments of self-harm (e.g., interviews, questionnaires, observation) administered over time to autistic people may better capture important aspects of self-harm (e.g., function, type, causes) in this population that could be leveraged to improve risk assessments and intervention supports.
Despite sampling differences, our findings have important implications for clinical care. First, lifetime experiences of STB were common across participants and highlight the importance of routine, frequent screening for suicide risk in both autistic youth and adults across settings (e.g., hospitals, schools, research studies). The need for universal and repeated assessment for STB in autistic people may be further supported by our finding that autistic people in this sample who had previously attempted suicide reported approximately three lifetime attempts, suggesting that suicide risk is elevated in this group and repeat attempts may be common. Second, the youngest age of suicide attempt was 7 years old, and the average age of first suicide attempt was 16 years old, with the greatest potential lethality averaging 19 years old. These findings can inform when to begin screening for STB risk in autistic people (i.e., early childhood) and the developmental periods (i.e., late adolescence and transition to adulthood) of highest risk for STB in this population, during which prevention efforts may be more targeted to increase safety. Third, multimethod tools to assess for suicide risk (e.g., interviews, questionnaires, parent report) may be optimal not only to capture the dynamic, episodic nature of STB but also to provide autistic people with multiple forms of communication to convey their experiences to others and seek supports. Interviews (e.g., C-SSRS) enable reciprocal exchanges to better understand an autistic person’s crisis/needs and a chance for autistic people to elaborate upon or clarify their responses, which is limited in survey/questionnaire methods. We also recognize that interviews may also be perceived as stressful or confusing to some autistic people given the social reciprocal nature of this method; therefore, it would be important for clinics, hospitals, research labs, and other organizations working with autistic people to have multimethod assessment tools (e.g., surveys, interviews) available to screen for STB in this population. Lastly, findings can guide safety planning interventions for autistic people by considering specific ways to make the environment safe such as limiting access to pills and sharp objects, as many people reported using these methods in previous suicide attempts or self-harm. Relatedly, increased supervision of autistic youth near roadways may be an important suicide prevention strategy in this population, as some autistic people reported stepping into traffic in an attempt to die by suicide. As autistic people are more likely to use psychiatric medications than non-autistic people, it may be important to have a collaborative discussion of safe ways to store, access, and use medications between autistic people and those who support them (e.g., providers, parents, spouse) to increase their safety during crisis.
We also recognize the limitations of our predominantly White, Western sample of autistic people without intellectual disability, which are areas of privilege, in informing crisis assessments and suicide prevention efforts in autistic people. There is a clear need to better assess risk for STB and NSSI among autistic people of different communication and/or intellectual abilities not only to characterize risk in these cohorts but also to increase the inclusiveness and representativeness of autism suicide research. Furthermore, few studies have considered cultural contexts, experiences, or preferences that may influence the pathway to STB and NSSI in autism or the role of intersecting identities (e.g., sexual orientation, gender, socioeconomic status) and potential associations with suicide risk and self-harm, particularly among autistic people living in non-Western countries. Given the limits of our cross-sectional data, we cannot investigate potential differences between momentary STB (e.g., during distress, shutdowns, meltdowns) and long-term STB (e.g., isolation, exclusion) that are critical to understanding trajectories of suicide risk in autistic people. We challenge our research teams, and both the suicide and autism research communities more broadly, to expand the inclusiveness of our research tools, sampling methods, and community initiatives to include autistic people of minoritized and underserved identities.
Strengths and limitations
Our study was strengthened by the use of the gold-standard C-SSRS to assess STB and NSSI, administered as a clinical interview in both the U.S. and Australian samples, as this tool integrates both self-report and clinical judgment. A first limitation of our study is the pooling of samples that recruited participants using different strategies for different purposes, which may limit the study findings. Although we accounted for site effects in our analyses, we recognize that different sampling methods (coupled with cross-sectional data) introduce bias into our study, and findings should be interpreted from this perspective. Second, we note the limitation of using caregiver report C-SSRS in the child sample from Canada given the known discrepancies between parent and child ratings in autism.71–73 Examining the effects of rater on C-SSRS scores in the current sample was outside the scope of the present study, and the lack of interview measures designed to assess self-reported suicidality in children as young as 7 years of age precludes this option at the present time. Notably, in a study involving a community sample of autistic adolescents assessed with the C-SSRS, Schwartzman et al. found that adolescents did not always disclose STB on the C-SSRS interview, although they did on a self-report questionnaire. Similarly, some autistic youth do not disclose their STB or crisis to caregivers, 74 which can affect parent-reported outcomes. Thus, our reliance on the C-SSRS alone may potentially underrepresent the true prevalence of STB and NSSI within our combined samples. Our findings highlight the need for the development of valid and reliable clinical and research instruments for assessing STB and NSSI in autistic children aged under 10 years of age, as well as ongoing screening throughout adulthood.
Third, as a cross-sectional study, we may have missed STB among some of the study participants, which is relevant given that STB are episodic and fleeting with a quick onset. 75 Future research incorporating real-time monitoring (e.g., ecological momentary assessment) offers opportunities to better understand the onset, associated environmental triggers, and course of STB. 75 Fourth, consisting of autistic people without co-occurring intellectual disability, our sample was not representative of the broader autism spectrum. Nonetheless, while autistic people with co-occurring intellectual disability may present with significantly elevated rates of NSSI, such as self-injurious stereotypy,76,77 autistic people without an intellectual disability are at the greatest risk of suicide 4 highlighting the importance of studying this population. Fifth, the C-SSRS contains one item about the presence/absence of NSSI, and thus, insights on NSSI in autistic people (e.g., type, trigger) and potential associations with STB were not explored. Sixth, co-occurring mental health diagnoses are a significant risk factor for suicidality,18,78 yet these data are not available across sites and constitute an important future direction of this work. Seventh, as our study was limited with respect to investigating possible relationships between STB/NSSI and nonbinary gender identity/gender diversity, it will be important for future studies to collect sufficient information on gender identity and conduct studies that purposively target gender diverse people to better understand STB and NSSI in this cohort. Lastly, our sample was predominantly White from economically developed Western countries and therefore not representative of autistic people who identify with different cultural, social, environmental, and economic factors. More research is needed involving autistic people from culturally and economically diverse countries. This is relevant where supports may be less accessible or where significant reduction of suicide deaths may require changes to government policies and regulations (e.g., banning of hazardous pesticides 79 ). Relatedly, this is a suicide-enriched sample, and thus, it is not representative of all autistic people.
Conclusion
Our study adds to the emerging literature concerning the frequent rate of STB and NSSI in the autistic population and highlights the importance of identifying STB early during development. We suggest that screening for STB and provision of mental health and other supports should first occur in autistic children younger than 10 years of age. Moreover, by early adolescence, supports need to be consistent, routine, and maintained in this developmental period with a clear focus on prioritizing safety in adolescents experiencing STB and associated distress. Our findings are also important for suicide prevention strategies: information concerning methods is particularly relevant for harm reduction and preventing access to means. We hope that our findings contribute to a broader acknowledgment that, such as other populations, autistic people across age-groups constitute a high-priority group for suicide prevention strategies, development of appropriate assessment instruments, and evaluation of system-level programs that effectively address the problem of preventable death by suicide within autistic people.
Footnotes
Acknowledgments
We thank the autistic people and their families who participated in this study across the United States, Canada, and Australia. We sincerely appreciate their willingness to share their experiences with us. J.M.S., C.A.M., and D.H. wish to thank the members of their autistic advisory groups who have made significant contributions to guiding their respective research programs.
Authorship Confirmation Statement
J.M.S., C.A.M., and D.H. conceived of the study. J.M.S., C.A.M., D.H., M.U., and M.A.S. collected the data and prepared the datasets for analysis. J.M.S., D.H., M.U., Z.J.W., and M.A.S. contributed to data analytic plans. J.M.S. and Z.J.W. analyzed the data. J.M.S., C.M.B., Z.J.W., and D.H. wrote the first draft. All authors reviewed the article and contributed to the final draft. The article has been submitted solely to Autism in Adulthood.
Data Access
Requests for access to the data sample should be directed to the corresponding author.
Ethics Statement
The Australian study was approved by the La Trobe University Human Research Ethics Committee (HEC20235). The Canadian study was approved by the Conjoint Health Research Ethics Board (REB19-1108). Data collected from the United States were approved by the Vanderbilt Institutional Review Board (Protocol #211870). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent and assent were obtained from participants.
Author Disclosure Statement
J.M.S. received partial salary support as a clinical provider in the Psychiatry Autism Research Team Clinic at Vanderbilt University Medical Center, from which deidentified clinical data were generated for analyses in the present study. J.M.S. was supported by the National Institute for Mental Health grant
Funding Information
The study received core support from the National Center for Advancing Translational Sciences (CTSA UL1TR000445) to utilize the REDCap system. The research was also supported by Untapped Holdings and Suicide Prevention Australia National Suicide Prevention Research Fellowships awarded to D.H. and C.M.B. The funders had no role in the study design, data collection, analysis, data interpretation, or writing of the report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.