
Abstract
Community Brief
Why is this an important issue?
Autistic adults have high rates of physical inactivity, and many do not meet physical activity guidelines promoted by the World Health Organization. The benefits of physical activity include improved sleep, increased social interactions, and reduced psychological distress. Participation in physical activity is important for autistic adults who have a propensity to sleep poorly, be socially isolated, and have a high likelihood of mental health issues.
What was the purpose of the review?
In this scoping review, we sought to identify and describe what is known about physical activity interventions for autistic adults and understand how the interventions worked in practice, who took part, and the safety of these interventions.
What did the authors do to review the literature?
Following published guidelines for conducting scoping reviews, we identified and screened peer-reviewed articles for studies that investigated a physical activity intervention involving autistic adults. We extracted information from each study to better understand how the intervention was carried out, who took part and the reasons for this, and the safety of the interventions, including any measures to ensure safe participation.
What studies did the authors find?
We identified nine studies describing physical activity interventions for autistic adults. Most participants were male, and all studies were done in high-income countries. The types of physical activity carried out were weight and aerobic training, walking and jogging programs, motor skill development, soccer, swimming and “exer-gaming” (i.e., active video games). These activities were completed either in small groups or one-to-one and were supervised by a trained person. Strategies to support participation included logistical support, orientation and specialist support, and motivation and peer support. Support strategies were used to adapt and give structure to the activity to meet the needs of individuals. Only one study gave reasons for people not taking part, which included a lack of interest, scheduling, and personal issues. Preexisting health conditions and complexity of needs excluded some autistic adults from taking part. Safety strategies included pre-exercise screening, having cardiopulmonary resuscitation-trained supervisors and physical and psychological training for support people. No studies reported adverse events because of participation in physical activity.
In summary, what did those studies show?
Having support in place, making adaptations, and having a structure that meets an individual’s needs and preferences may facilitate uptake of physical activity among autistic adults.
What are the remaining gaps in the literature?
Understanding the reasons for low or nonparticipation needs further exploration. There remains a need to better understand physical activity from the perspective of autistic women and among autistic individuals with complex needs and those living in low-income countries.
Based on this review, what do the authors recommend?
Understanding the needs of all autistic adults is important to facilitate their uptake and inclusion in a variety of physical activities regardless of the setting. Autistic individuals need to be included in the design of physical activity programs to ensure their needs and preferences are met. Further, there is a need for physical activity programs that can translate to low socioeconomic environments.
Introduction
Physical activity is an integral part of a healthy lifestyle. Defined “as any bodily movement produced by skeletal muscles that requires energy expenditure,” it encompasses exercise (a subset of physical activity), physical recreation, active transport, and active work. 1 The World Health Organization and Australian Government guidelines recommend adults participate in 150 minutes of moderate-intensity physical activity per week.2,3 Autistic adults fall short of this guidance and are less active than the general population, with one study reporting that 67% of autistic participants “sometimes” or “often” engaged in physical activity compared with 87% of non-autistic adults. 4 While available evidence assessing physical activity levels in autistic adults is limited in quantity and faces methodological challenges (e.g., underutilization of objective measures of activity), 5 findings suggest autistic adults lead more sedentary lives than neurotypical adults.6-8
Regular physical activity is an effective primary and secondary preventative strategy for common health and psychosocial conditions, 3 including those to which autistic adults are predisposed. For example, autistic adults experience higher prevalence of co-occurring mental health problems (e.g., anxiety and depression),9,10 poorer physical health (e.g., obesity, sleep disturbance, and low physical fitness),5,11 and reduced social participation (e.g., smaller social networks and fewer reciprocal friendships).12,13 These health and well-being disparities are associated with lower life expectancy for autistic adults, who are more likely to die from preventable causes such as diabetes, cancer, and suicide.14-16 A large population-based longitudinal study has shown that 15 minutes of moderate intensity physical activity a day reduces morbidity and increases life expectancy, 17 illustrating that any movement is good for health.
Like non-autistic adults, physical activity offers health and well-being benefits to autistic adults. These benefits include improved sleep, better fitness, and increased social interaction.8,18,19 For example, a peer-mentored gym-based physical activity program for young people with disability, including autistic individuals, found an important and meaningful benefit of the program was a “strong sense of social connectedness.” 20 Conversely, psychological distress (e.g., stress and anxiety)21,22 and obesity 23 are negatively associated with autistic adults’ level of physical activity. Together, this suggests facilitating participation in physical activity has the potential to significantly improve well-being for autistic adults.
Despite the potential benefit of physical activity for autistic adults, several barriers may limit their participation in regular activity. Intrapersonal barriers to participation can include difficulties associated with poor motor skills, sensory differences, reduced fitness, and motivation levels, as well as psychological factors (e.g., fear and anxiety), which may stem from prior negative experiences with physical activity (e.g., experiences of exclusion and bullying).24-26 Interpersonal barriers involve factors such as undervaluation of physical activity by family members, lack of social support, communication difficulties, and experiences of bullying.25,26 Environmental and community barriers may include transportation and financial constraints, limited access to programs, discrimination, and a lack of programs that promote and support participation among minority groups, such as autistic individuals.4,26
Given the potential benefits of physical activity coupled with the barriers to inclusion faced by autistic adults, understanding the implementation of physical activity interventions for autistic adults is critical to living a happy and healthy life. This aligns with recommendations from the recent Lancet Commission on future care and clinical research in autism, which highlighted the need for interventions that enhance the physical and mental well-being of autistic individuals across the lifespan. 15 These priorities also reflect the autistic community’s emphasis on physical health, well-being, and mental health in research. 27
However, our understanding of the implementation of physical activity interventions for autistic adults remains limited. Most research has focused on children, with three systematic reviews addressing exercise and autism in those aged 18 years or younger.28-30 While these reviews suggest physical activity improves social, behavioral, and cognitive functioning, in addition to gross motor skills and other physical health benefits for autistic children,28-30 their findings may not generalize to autistic adults. For example, community-based recreational activities for children include structured classes with additional formal supports (e.g., one-to-one swimming lessons or martial arts classes) that are not set up for adult participation or structured to support autistic adults with complex behavioral needs. Therefore, further research is needed to understand the types of physical activity interventions that have involved autistic adults.
Current study
Autistic adults face high rates of physical and mental health challenges that could potentially be mitigated by increased physical activity. Health and exercise professionals working with autistic adults are interested in understanding what adaptations can be made to physical activity programs that are neuro-affirming and facilitate participation. However, there is limited understanding of the implementation—what works, reach—how to engage, and safety—both physical and importantly psychological safety—of physical activity interventions for autistic adults. We conducted a scoping review to synthesize current research findings, specifically focusing on the following research questions:
What physical activity intervention(s) have been studied and how they were implemented for autistic adults? What is the reach (i.e. the number, proportion, and representativeness) of the autistic population who participated in physical activity intervention studies? Are physical activity interventions safe for autistic adults?
Methods
We were guided by the framework for scoping reviews proposed by Arksey and O’Malley 31 and the recommendations of the Joanna Briggs Institute. 32 We registered the study protocol with the Open Science Framework on December 4, 2023, 33 and reported our findings according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for scoping reviews guidelines (PRISMA-ScR). 34
Eligibility criteria
We included studies if (1) participants were aged 18 years and over, the mean age of participants was greater than 18 years of age, or if more than 50% of participants were 18 years or older and (2) participants had either a formal autism diagnosis or self-identified as autistic. Where studies included participants with other diagnoses, the proportion of autistic participants and data pertaining to autistic adults needed to be reported separately and (3) a physical activity intervention of any type and duration was implemented, for example, structured or unstructured physical activity including aerobic or strengthening exercise program, a gym or sports program (e.g., soccer), or a walking program. The intervention could be delivered in any setting, including universities, clinics, and community settings. All study designs were included but needed to have been published in a peer-reviewed journal. Conference abstracts, theses, narratives reviews, and case studies (other than n = 1 trials) were excluded. There were no limits on language.
Search strategy
We searched five databases from inception to June 17, 2024: Medline, EMBASE, CINAHL, SPORTDiscus, and PEDro. In addition, we searched PubMed for the years 2023–2024, to ensure we would identify citations that preceded an article’s final publication in a Medline indexed journal. Our search strategy included keywords and MeSH headings related to autism (AND) physical activity (OR) exercise (OR) sport (Supplementary Appendix A). We supplemented database searches by citation tracking of included studies using Google Scholar and manual checking of reference lists.
Selection of sources of evidence
We combined database search yields in an EndNote library and removed duplicates. We uploaded the search yield into Covidence software (https://app.covidence.org), and two reviewers with expert content knowledge of physical activity, disability, or autism (authors R.A.K., L.H., A.S., R.S., and N.S,) independently screened each article. Initial screening was based on title and abstract. Where we could not determine eligibility, we retrieved the full text, and two reviewers independently reapplied the criteria. Any disagreements were resolved by consensus, or if consensus could not be reached, a third reviewer was consulted.
Data extraction
We modified a Template for Intervention Description and Replication (TIDieR) checklist 35 to the requirements of the study aims and used the eligibility criteria to develop a standardized data extraction template in Microsoft Excel (Supplementary Appendix B). In addition to referencing details (i.e., author(s) and year of publication), we extracted data about study design, participants (e.g., sample size, age, and gender), setting (including country of origin), intervention (e.g., duration, frequency, and intensity), and implementation (e.g., who provided the intervention, mode of delivery, and any strategies to support implementation).
We considered reach by using the reach-related items contained in the RE-AIM framework data extraction coding tool. 36 We extracted eight items from the coding tool: methods to identify target population, recruitment strategies, participant inclusion/exclusion criteria, participation rate, sample size, characteristics of participants, representativeness of participants, and reasons for declining participation. We calculated the participation rate from the number of participants assessed for eligibility compared with those who entered the study.
We recorded any documented safety concerns about interventions, including the outcome(s) of these events. We categorized adverse events by seriousness, expectedness, and relatedness to physical activity. 37 Author R.S. completed data extraction. Authors R.A.K. and L.H. checked the data extraction. We did not formally appraise risk of bias and quality assessment as the aim of our scoping review was to explore the implementation, reach, and safety of physical activity interventions.
Data analysis
We characterized the studies, interventions, and participants descriptively. We mapped extracted data deductively using a descriptive analytical approach to categories associated with the key aims of the review, that is, implementation, reach, and safety. 38
Results
Following systematic database searches and citation checking, we identified 3897 articles; 9 studies met our inclusion criteria (see Fig. 1).8,39B40 -46 Table 1 describes the characteristics of the included studies. Of 148 identified autistic participants, 108 (73%) were male and the range of mean ages was 19–34 years. Diagnosis of autism included the use of diagnostic criteria Diagnostic and Statistical Manual of Mental Disorders (DSM) appropriate to the time of the study publication (DSM-III, DSM-IV, International Classification of Diseases, Ninth Revision (ICD-9), n = 5),8,39B40 -42 diagnosis by a psychiatrist (n = 3),39,41,42 or psychologist (n = 3)39,40,42 or medical physician. 43 One study relied on self-report or carer report of autism and a score of 28 or higher on the Childhood Autism Rating Scale 2nd Edition (CARS-2), administered by a trained assessor to assess autistic traits in the participants (n = 1). 45 A further two studies stated a diagnosis of autism without identifying how the diagnosis was determined.44,46 Reported co-occurring conditions included intellectual disability ranging from mild to profound in all participants in five studies,39B40 -42,45 attention deficit hyperactivity disorder, obsessive compulsive disorder, or schizoaffective disorder in one study 44 and scoliosis in a further study. 46 One study did not report or characterize intellectual disability or other indicators of autism diagnostic level due to ethics committee stipulation. 8 The studies originated from high-income countries, five from the United States8,39,40,44,45 and one each from Canada, 41 Greece, 46 Spain, 42 and Israel. 43 Publication dates ranged from 1994 to 2023; six of the nine studies were published since 2017.8,42B43 -46
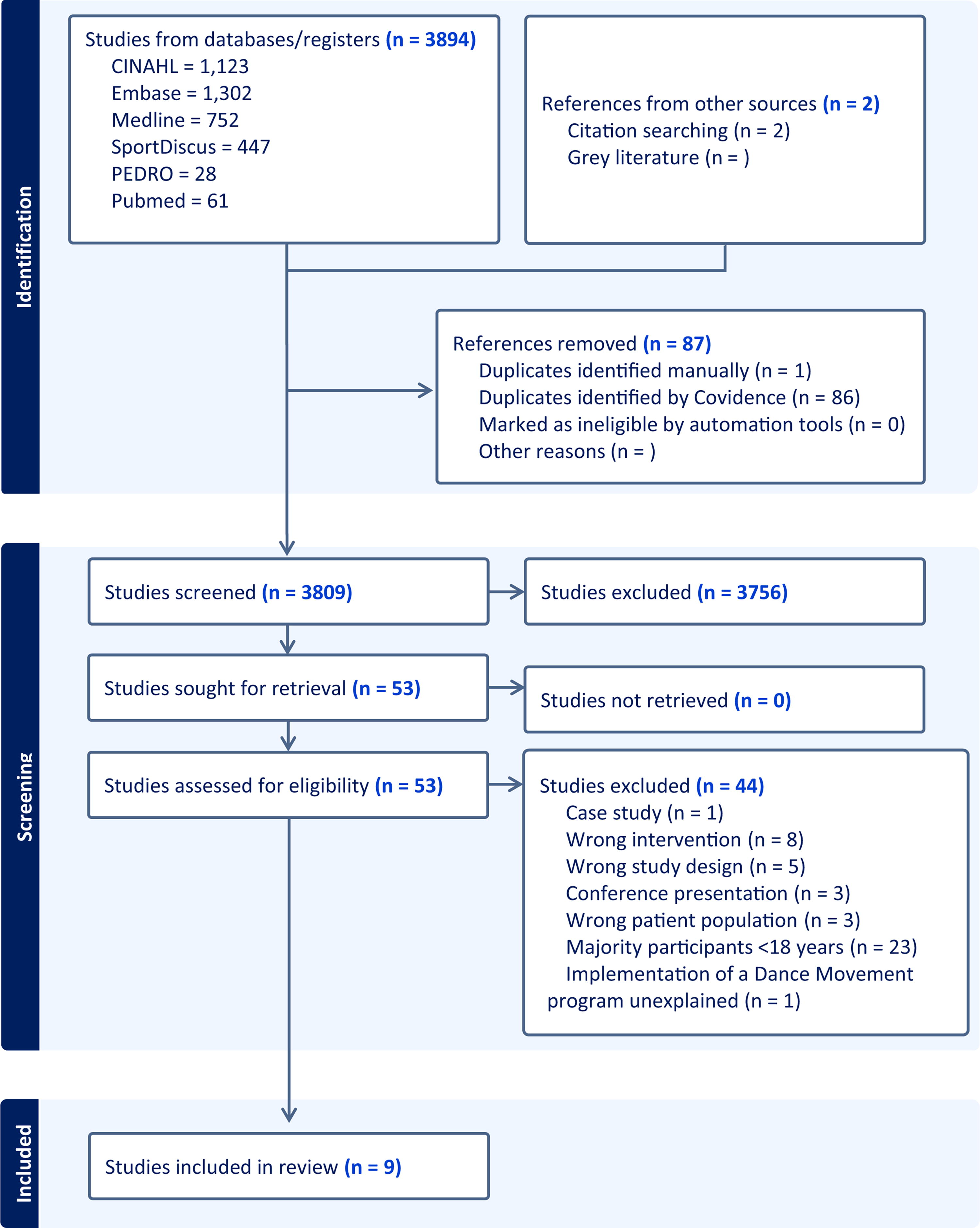
PRISMA flow diagram for selection of eligible studies.
Characteristics of Included Studies
Only participants in the aerobic exercise program were reported. The aerobic exercisers were aged 16, 20, and 21 years. Two participants in the strength training program were aged <18 years and were not reported.
Only participants with a diagnosis of Autism and/or aged 18 years and older reported.
AE, adverse event; CPR, cardiopulmonary resuscitation; N/A, not applicable; NR, not reported.
Interventions and implementation
The physical activity interventions are detailed in Table 2. Interventions included aerobic exercise (n = 3),39,40,44 walking or jogging (n = 2),41,42 strength training, 44 motor skills training, 39 snowshoeing, 41 soccer, 43 exer-gaming (Kinect for Xbox360 Kinect Sports TennisTM and Kinect Sports BoxingTM), 8 self-selected physical activities (e.g., running), 45 and a combination of aquatic therapy and swimming program 46 (all n = 1). The programs ranged in duration from 6 weeks to 10 months (one did not report duration 39 ) with the median length of programs being 12 weeks (interquartile range 17). Participants exercised as often as five times per week for 60 minutes during a walking program, 42 and as little as once a week for 30 minutes in an “exer-gaming” active video gaming intervention. 8 Reported exercise intensity ranged from self-selected in two studies including a self-managed home-based physical activity program and a snow-shoeing-walking/jogging program41,45 to moderate to vigorous aerobic exercise.8,39,44,45 Three programs described the exercise intensity as self-selected or low volume.42,43,46 Five programs recorded exercise intensity as moderate or moderate to vigorous.8,40,41,44,45
Intervention Details
BPM, beats per minute; HR, heart rate; NR, not reported.
Programs were completed at home (family home or residential care facility, n = 3),39,42,45 school (schools for students with disability, n = 2),40,41 university (university-affiliated autism center and a university gym, n = 2),8,44 privately operated facility (pool n = 1), 46 and community settings (soccer fields or other community facility, n = 2).41,43 Six studies were situated in or recruited from residential or specialist education settings.8,39B40 -43 All programs were delivered in-person with direct supervision.
The interventions included various social strategies to support the participation of autistic adults in physical activity (Table 3). Social supports included supervision, education, orientation, motivation, specialist support, peer-mentoring, postexercise socialization, and logistical support. 47 Programs were supervised by exercise or health professionals (exercise physiologist, occupational therapist, or researchers with expertise in autism and/or physical activity programming, n = 5),8,40,41,44,46 trained instructors (n = 2),42,43 university student peer mentors (n = 2),8,44 a coach (often a family member, n = 1), 45 and teaching assistants or residential staff (n = 2).39,41 Four programs involved a familiarization or orientation program.8,40,41,45 Two programs included a peer mentor in addition to supervision from a person with training and experience in autism8,44 and one was a group-based program. 43 Explicit logistical support was provided in seven programs and included adapting and tailoring programs to participants’ needs to enhance access and participation.8,39,41B42 -45 Motivation strategies were used in eight programs usually verbal encouragement, the use of activity trackers and monitoring or documenting progress, feedback, debriefs and check-ins.8,40B41 -46 Education was provided in four studies41,43-45 and postexercise socialization including nutritional snacks in one study. 44
Strategies Used in the Physical Activity Interventions to Support the Autistic Participants
Specialist and peer support provided supervision in addition to the specialist knowledge or peer support provided.
In addition to social support strategies, four studies promoted self-determination strategies that allowed participants to choose the type of physical activity, the location, and the pace or intensity at which they exercised.41,42,44,45 Adherence was reported in five studies and ranged from 78% to 100% attendance.39-41,44,45
Reach
Methods to identify and recruit the target population
Only two included studies reported methods to identify the target population and associated recruitment strategies.44,45 In one study, the researchers developed a website with information about the intervention and an option for prospective participants to enter contact details. The website was promoted with local autism groups in two states of the United States. 45 In the second study, the researchers targeted autistic college students by contacting campus, community, and disability agencies that provided services to autistic adults, distributing flyers and via word of mouth to reach students. 44 For the remaining seven studies, the researchers did not provide any information on methods to identify the target population and provided limited information on recruitment strategies, which was confined to providing information on where participants were recruited from rather than providing specific information as to how they were recruited.8,39B40 -43,46
Participant eligibility criteria
Only one study did not report eligibility criteria. 46 Inclusion criteria most often referred to a diagnosis of autism. In one study, participants required a diagnosis of autism or intellectual disability, 43 whereas participants in another study required a diagnosis of autism and intellectual disability. 40 All participants were required to be over 18 years of age. Ability to participate in physical activity was a key inclusion criterion in two studies.44,45 Other key inclusion criteria involved being at risk for falling 43 and having access to the internet and a computer or smart phone. 45 The most common exclusion criterion was any health issue that prevented a prospective participant from being physically active. In one study, prospective participants who were not accepting of wearing an activity tracker, which was the primary outcome measure of the study, were excluded. 45 Those ineligible were reported to have more severe autism traits (determined by CARS-2 average score 40.4) and lower nonverbal intelligence quotient (IQ) scores (average 54.0 assessed with the Leiter-3 test). Three studies excluded participants based on health and fitness,40,42,43 including the presence of an acute illness or injury, history of significant medical or health comorbidities, or inability to participate in moderate to vigorous physical activity.
Sample size
All included studies reported a sample size, which ranged from 1 to 69 (median = 16).
Participant characteristics
Only one study did not provide details about participants’ sex. 40 Of the remaining eight studies, most participants were male, except for one study that included an equal number of males and females (sample n = 6). 39 This study was an older study (1994) based in a residential treatment program and the participants had long histories of “restrictive residential placement” due to “severe maladaptive behaviors.” 39 All studies reported the age of participants, with the mean age ranging from 19 to 34 years. Three included studies provided information on ethnicity,8,44,45 reporting most participants were “White” (63% White, 19% Asian, 13% Hispanic and 5% White/Asian, 44 70% White, 15% multiracial or biracial, 12% Black and 3% Hispanic or Latino 45 and 92% White, 6% Latino, and 2% Black 8 ).
Reasons for declining or withdrawing participation
A single study including people with both autism and intellectual disability provided reasons for declining participation prior to the study commencing: 24 individuals declined to participate due to a lack of interest. 45 One study reported five enrolled participants did not attend any study sessions and withdrew due to scheduling and personal issues. 8 In a further study, one participant was withdrawn due to safety concerns after they removed their footwear (snowshoes during a Canadian winter outdoor activity). 41 Two participants were withdrawn for unspecified medical reasons in one study. 42
Participation rate
Only one study, a randomized controlled trial, provided complete data that allowed the calculation of a participation rate; 45% of the autistic adults who expressed interest participated in the trial. 45 The reporting of two studies made it impossible to discern how many autistic participants were assessed for eligibility and commenced the study.8,43 One of these studies reported a mix of 41 autistic and neurotypical participants were enrolled or scheduled to enroll, but 5 failed to attend any sessions. From their reporting, it is unclear whether the five who failed to attend were autistic or neurotypical. Eighteen autistic individuals completed the intervention. 8 In a second study, 100 participants entered the study, who were a mix of participants with autism and participants with intellectual disability, and it is unclear how many were in each group. 43 Sixty-nine participants completed postintervention assessments, of whom 19 were autistic and 50 had an intellectual disability. 43 A third study provided information on targeting and recruitment; however, it was unclear how many were assessed for eligibility. 44 Sixteen autistic individuals completed the study. It is unknown if more individuals began the study or if any individuals dropped out or withdrew. 44 A further study reported 46 autistic participants were assessed for eligibility and 44 participants completed the study with 2 withdrawing during the study period. 42 However, these participant numbers do not align with those reported in the available research flowchart, and therefore, we do not feel confident calculating the participation rate for this study. 42 The remaining four studies comprised small samples ranging from 1 to 6 participants and did not provide enough data to calculate a participation rate.39-41,46
Representativeness
Only one study noted the representativeness of their sample was limited. 44 No other included study reported on representativeness. The section “Participant characteristics” would suggest that representativeness is limited given the samples were skewed toward the inclusion of white, male participants.
Safety
Safety considerations and adverse events were reported in four studies (Table 1).8,39,41,44 Two studies implemented pre-exercise medical screening, supervision for injury prevention, and the presence of certified cardiopulmonary resuscitation supervisors and a defibrillator on site, with no adverse events reported for either study.8,39 One study excluded a participant due to the risk of frost bite after the participant refused to wear footwear in the snow. 41 Training on physical and psychological safety for autistic participants was provided to peer mentors in one study. 44
Discussion
With support, autistic adults can safely participate in a wide range of physical activities, but little is known about the reach of these activities and reasons for nonparticipation. This review highlights the increasing interest in physical activity interventions aimed at autistic adults, as evidenced by six of the nine identified studies in this review being published since 2017. It is important to note that overall these studies contribute to a small pool of work in a population at considerable and known risk of chronic physical health, mental health, and well-being disorders associated with physical inactivity and increased sedentary behavior.48,49 The interventions described in this review span a variety of activities and settings from structured gym-based aerobic and strengthening and swimming programs to popular community-based sporting (soccer or football) and cultural activities (Canadian snowshoeing) and unstructured walking activities. All programs implemented two or more social support strategies to facilitate the participation of autistic adults in physical activity with no adverse effects. In addition, the inclusion of self-selection or choice of activities by participants was evident in more recent studies. Reach was described variably in the included studies with limited explanation of recruitment strategies or identification of the target population, little reporting of participation rates and reasons for nonparticipation and representativeness.
Supporting participation
The variety of activities and settings reported in the included studies is reflective of the diversity of activities available and of interest to many living in high-income countries. Self-determination or choice in activity is important to individual motivation and can impact adherence, engagement, and subsequently participation. 50 One study appeared to exclude a key group of autistic adults who did not tolerate wearing an activity tracker. 45 These participants had higher levels of autistic traits (higher CARS-2 score) and lower nonverbal IQ compared with the other study participants. The exclusion criteria in this study likely excluded individuals with more profound intellectual disability, a group who are more likely to have greater motor and movement problems. 51 However, this group does not necessarily need to be excluded from participation in physical activity. Young people with complex disability including intellectual disability and behaviors of concern can be integrated successfully into physical activity interventions with appropriate supports. 20 Effective strategies in other exercise studies have included additional screening, risk analysis and mitigation planning, specialist support, tailoring of exercise to the individual’s level of skills (e.g., taking a “just right” approach) and additional training (e.g., behavioral management), support, and familiarization for the people supervising the physical activity. 20 Health and exercise professionals, for example, recreational therapists, occupational therapists, physiotherapists, and exercise physiologists, are well positioned to facilitate physical activity participation for autistic adults across a variety of settings with appropriate adaptations and scaffolding, including social support strategies. 20
Reach and participation
Reach represents those who are willing to participate in a given activity. 52 The included studies were limited by a lack of diversity and representativeness with a strong bias among the nine included studies to “white” men. The predominance of men reflects the three to one ratio of male to female gender prevalence in autism. 53 However, autism is likely underdiagnosed in women. 53 The higher number of men may also reflect a predisposition to choose physical activity over other forms of recreation. Studies from the United States and Sweden have shown that nonparticipation in physical activity among autistic adults includes the lack of motivation and perception that exercise is boring 26 with attitudes to physical activity beginning at a young age among autistic adolescents. 54 A willingness to partake in physical activity was “conditional” on autistic adolescents’ perceived competence and confidence, motivation, adjustment to social, activity, and environmental demands, predictability of the situation, and the freedom to choose. 54 Many autistic adults cite poor motor skills and a lack of skill development in childhood as a reason for nonparticipation in physical activities as an adult. 54 While the reasons for nonparticipation were not explored in the study by Savage et al., 45 they may be similar to those expressed by the younger autistic adolescents Arnell et al. interviewed. 54 There is a need for programs that support physical activity at “just the right level,” matching the preferences and physical competencies of all autistic adults, in accessible and accommodating environments.
Strengths and limitations
The small number of included studies may be considered a limitation of our scoping review, and the largely homogenous participant group with a strong gender bias limits the generalizability of the findings of this review. However, our scoping review highlights the lack of large, well-conducted and physical activity intervention studies inclusive of females and individuals with higher and more complex needs. The strength of this review lies in the methodology including an exploration of the types of interventions, how they were implemented, and the reach and representativeness of the included participants.
Conclusion
Notwithstanding the limitations, our scoping review identified a small evidence base to support the safe implementation of physical activity for autistic adults, across a range of activities and using various social strategies to support inclusion and uptake. Importantly, this review highlights the need to address complexity of needs among autistic adults, the heterogeneity of the adult autistic population, self-determination, choice and tailoring to individual preferences, and translation of physical activity interventions to low-income settings. Further research is needed to determine participation rates, the underlying reasons for low participation in physical activity among autistic adults, and the under representation of female-identifying autistic adults. Our study highlights the need to consult with the autistic community about preferred activities and program implementation strategies. There is a need to include autistic individuals in the design of physical activity programs to ensure they meet their needs, are inclusive of abilities and gender, and enhance the physical and mental well-being of autistic adults.
Footnotes
Authorship Confirmation Statement
N.S.: Conceptualization; N.S., R.A.K., and D.A.: Methodology; R.A.K., R.S., L.H., and A.S.: Data curation; R.A.K. and D.A.: Formal analysis; R.K., N.S., D.A., and S.B.: Writing original draft; D.H., N.F.T., G.McK., A.S., L.H., and R.S.: Writing review and edit.
Author Disclosure Statement
D.H. declares he is a Deputy Editor for Autism in Adulthood. He was not involved in the editorial process for this article. All other authors report no conflicts of interest.
Funding Information
This work was funded by a La Trobe University MRFF Kickstarter grant.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.