
Abstract
Obesity and pneumoperitoneum in the reverse-Trendelenburg position during laparoscopic sleeve gastrectomy (LSG) are reported to negatively affect cerebral oxygenation. Anesthetic agents can have variable effects on the regional cerebral tissue oxygen saturation (rSO2) measured with near-infrared spectroscopy. Our study investigated the potential impact of sevoflurane versus propofol-based anesthesia on rSO2 in LSG cases. Sixty American Society of Anesthesiologists (ASA) II-III patients, 18–65 years of age, with a body mass index of ≥35 kg/m2, undergoing LSG were randomized to two groups: sevoflurane/remifentanil (inhalation) and propofol/remifentanil (total intravenous anesthesia [TIVA]) groups for anesthesia maintenance. The rSO2 values were recorded preoperatively, 1 min after anesthesia induction, and every 5 min during surgery. Arterial blood gases (ABG) were measured in the fifth minute postinduction (t1), 30th minute postinsufflation (t2), and postextubation (t3), and correlation with rSO2 was examined. No significant difference was found between the groups in terms of rSO2 values, and cerebral desaturation was not observed in either group. ABG values were similar in both groups with moderate positive correlation between rSO2 and hemoglobin (t1, t2, t3: r = 0.365; 0.005; 0.454: p < 0.001; p = 0.494; p < 0.001, respectively). Cerebral oxygenation was preserved during both anesthetic regimens, and moderate positive correlation was found between rSO2 and hemoglobin levels.
Introduction
Obesity is a global health issue that affects different organ systems and may cause severe health issues. 1 The World Health Organization defines obesity as a body mass index [BMI = weight (kg)/height (m2)] ≥30 kg/m2. 2 Patients with a BMI >40 kg/m2 or those with a BMI >35 kg/m2 with accompanying comorbidities are candidates for weight loss surgeries, which are generally referred to as bariatric surgeries. 3 Laparoscopic sleeve gastrectomy (LSG) is a restrictive bariatric surgery procedure gaining increased popularity in the surgical treatment of morbid obesity. When applied as a primary treatment in bariatric surgery, LSG is both effective and safe, with low mortality and morbidity rates. 4 However, LSG requires a reverse-Trendelenburg position and prolonged pneumoperitoneum. Carbon dioxide pneumoperitoneum increases intracranial pressure (ICP) by increasing intra-abdominal pressure and by causing dilation of cerebral vessels through carbon dioxide reabsorption. Also, the reverse-Trendelenburg position decreases cardiac output and mean arterial pressure (MAP) by reducing cardiac venous return.5,6 According to the formulation of cerebral blood flow (CBF) = cerebral perfusion pressure/cerebral vascular resistance (CVR) = (MAP − ICP)/CVR, all these changes negatively affect cerebral perfusion and oxygenation. Additionally, increased cerebrovascular bed resistance and decreased CBF, particularly in the prefrontal cortex, due to obesity, which is a risk factor for cerebrovascular disease, make the monitoring of cerebral oxygenation more important in such cases.7,8 Near-infrared spectroscopy (NIRS) is a noninvasive technique and provides continuous monitoring of regional cerebral tissue oxygen saturation (rSO2). Even though rSO2 values are influenced by extracerebral blood flow, hemoglobin concentration, arterial carbon dioxide concentrations, inspired oxygen content, and systemic blood pressure management, they are beneficial in the assessment of cerebral oxygen supply/demand balance in surgeries with potential neurological side effects. 9
Sevoflurane and propofol are widely used for the maintenance of general anesthesia during bariatric surgery. Sevoflurane is an efficacious halogenated inhalational anesthetic for bariatric surgery because of its rapid and consistent recovery and because it does not cause hemodynamic instability because of its low blood solubility. 10 Moreover, it increases global CBF through a direct intrinsic cerebral vasodilatory action and, in addition, it might improve cerebral oxygenation by decreasing the cerebral metabolic rate of oxygen (CMRO2; luxury perfusion).11–14 Propofol can also be a suitable option for the maintenance of anesthesia in bariatric surgery. Propofol is a short-acting intravenous (IV) anesthetic agent with a very good recovery profile, and its elimination half-life and duration of action do not change in obese individuals. 15 However, it has been reported that propofol may significantly decrease CBF by both suppressing CMRO2 and through a direct vasoconstrictive action. 16 The impact of propofol on global CBF is more salient than that on CMRO2, resulting in a decrease in rSO2.16,17 The aim of the present study was to test the hypothesis that rSO2 is better preserved with sevoflurane than propofol in morbidly obese patients who have undergone LSG.
Materials and Methods
This study was conducted at the Department of Anesthesiology of the medical school hospital following approval by the medical school and the Ethics Committee of the Surgical Research Center (approval number B.30.2.ODM.0.20.08/27-230). The study was also registered with ClinicalTrials.gov (NCT03946657).
Study participants
All study participants provided a written informed consent before enrollment. Sixty patients in the American Society of Anesthesiologists (ASA) physical status class II–III, 18–65 years of age, with a BMI of ≥35 kg/m2 who were planning on undergoing an elective LSG were enrolled in the study. Patients with preexisting cerebrovascular diseases, overt neurological signs, alcohol or psychoactive drug addiction, uncontrolled diabetes or hypertension, advanced organ failure, preoperative peripheral oxygen saturation (SpO2) <96%, or a hemoglobin <9 g/dL were excluded.
Randomization
For the investigation, the patients were randomly assigned using opaque sealed envelopes to two groups; the Inhalation group, including those who received sevoflurane/remifentanil for the maintenance of anesthesia (n = 30), and the TIVA (total intravenous anesthesia) group, including those who had propofol/remifentanil infusion for the maintenance of anesthesia (n = 30). Randomization was performed according to a computer-generated randomization code, and a statement showing the patients' group was placed in a sealed, numbered envelope according to the results. Each patient drew an envelope and was enrolled in the study depending on the group written in the envelope. Randomization was performed by a physician who was not involved in the monitoring of the patients. The anesthesiologist caring for the patient was aware of the group assignments. The patients were blinded to the group assignments.
Anesthesia protocol
All patients were administered 300 mg of oral ranitidine the night before the surgery and 10 mg IV metoclopramide in combination with 150 mg ranitidine 1 h before arrival to the operating room. Upon the arrival to the operating room, an electrocardiogram, noninvasive blood pressure, SpO2, rSO2 (INVOS™ 5100C oximeter; Covidien), and neuromuscular monitoring (TOF-Watch™ SX; Organon, Dublin, Ireland) were performed on the patients. Afterward, preoxygenation was performed with 4 L/min oxygen (80%) for 3 min by using facemasks, and anesthesia was induced with an IV propofol injection (1.5–2.5 mg/kg of ideal body weight) and an IV bolus administration of remifentanil (1 μg/kg of lean body weight [LBW]) for 30–60 s, and then switched to infusion at 0.25 μg/kg of LBW/min. After the eyelid reflex disappeared, a neuromuscular blockade was performed using rocuronium (1.2 mg/kg of LBW), ensuring that the train-of-four count and the posttetanic count (PTC) were both zero, and performed tracheal intubation. Mechanical ventilation was performed with a Draeger Fabius™ Plus Anesthesia Workstation (Draeger Medical, Lübeck, Germany), and volume-controlled mechanical ventilation was applied. Breathing gases (oxygen, carbon dioxide, sevoflurane) were measured using Draeger Scio™ gas measurement module (Draeger Medical). The tidal volume was set as 7–8 mL/kg of LBW, inspiratory:expiratory ratio as 1:2, positive end-expiratory pressure as 5–8 cmH2O, and the respiratory rate was determined to obtain an end-tidal carbon dioxide partial pressure (PETCO2) of 32–37 mmHg. These ventilator settings were not changed throughout the operation. Furthermore, after the induction of anesthesia, a radial arterial line was placed in all patients for the continuous measurement of MAP and intermittent arterial blood gas (ABG) analysis.
Oxygen/air (fraction of inspired oxygen [FiO2] of 0.40), inspiratory fresh gas flow of 2 L/min), sevoflurane (1 minimum alveolar concentration [MAC]), and remifentanil IV infusion (0.1–0.25 μg/kg of LBW/min) were used in the Inhalation group for the maintenance of anesthesia. Propofol infusion (4–8 mg/kg of total body weight/h), oxygen/air (FiO2 of 0.40; inspiratory fresh gas flow of 2 L/min), and remifentanil IV infusion (0.1–0.25 μg/kg of LBW/min) were used in the TIVA group. Neuromuscular blockade was performed during the operation by rocuronium infusion (0.3–0.7 mg/kg of LBW/h), ensuring that PTC was zero. IV normal saline or lactated Ringer's solution at 5–7 mL/kg of LBW was also used for perioperative fluid maintenance. Nasopharyngeal temperature was monitored throughout the surgery, and the patient temperature (36–37°C) was ensured by using a forced-air warming system for the maintenance of intraoperative normothermia during the procedure.
After anesthesia induction, a neutral head position of the patients was preserved to prevent alteration of cerebral venous drainage. Carbon dioxide insufflation was performed with an electronic laparoflator using a closed Veress needle technique, and intra-abdominal pressure was automatically kept at the desired level (14–16 mmHg) during the surgery. After the insufflation of carbon dioxide, the patients were positioned in a 30° reverse-Trendelenburg and at a 10° right lateral position.
At the end of the surgery, the blockade was reversed by administering 4 mg/kg of adjusted body weight sugammadex with a PTC of 1–2. All patients were extubated in the beach chair position when fully awake. The patients were referred to the recovery unit and monitored for 50 min for complications. In cases where no complications were apparent, the recovery was evaluated using the modified Aldrete scoring system. Once the score was ≥9, the patients were taken to the unit. For postoperative nausea and vomiting, 4–5 mg dexamethasone was used (except for diabetic patients on insulin) 90 min before anesthesia induction and 4–8 mg IV ondansetron 20–30 min before the end of the operation. For postoperative pain management, 1 g IV acetaminophen was administered 20 min after induction and 30 mg IV ketorolac 20 min before onset. Then, 1 g IV acetaminophen was administered every 6 h + 50 mg IV dexketoprofen every 8 h for the first 48 h. In addition, morphine was administered using a patient-controlled analgesia delivery system (demand dose, 20 μg/kg of ideal body weight; lockout time, 6–10 min; 4 h limit, 80% of the total calculated dosage) for 48 h postoperatively.
Intraoperative measurements
Physiological variables
Measurement values of the physiological variables including heart rate (HR), MAP, SpO2, and PETCO2 were recorded preoperatively, 1 min after the induction, and every 5 min until the patient was referred to the recovery unit. The MAP and HR values were allowed to fluctuate up to 20% of the preoperative values of the patients. For this purpose, the infusion rate of remifentanil was accordingly increased and decreased. When hypotension (MAP <60 mmHg) or bradycardia (HR <45 beats/min) continued for longer than 3 min, they were treated with 5 mg ephedrine and 0.5 mg atropine, respectively. Patients who received ephedrine or atropine more than twice were excluded from the study.
Cerebral oxygen saturation
The rSO2 values of the patients were recorded preoperatively, 1 min after the induction, and every 5 min until the patient was referred to the recovery unit. Measurements in the last 30 s of preoxygenation, performed for 3 min with 4 L/min oxygen (80%) preinduction, were accepted as preoperative values. To assess rSO2, cerebral oximetry sensors were placed at least 2 cm above the left and right eyebrows and 3 cm from the midline (to prevent the sagittal sinus from influencing the results) before the induction in accordance with the manufacturer's instructions. Before applying the sensor pads, the forehead of the patient was cleaned with acetone alcohol and bandaged to protect the sensors from ambient light and to keep them stable. Cerebral oxygen desaturation was defined as a >25% decrease in the rSO2 value compared with the preoperative value (decrease should be more than 20% if the preoperative value is <50) and maintenance of this situation for ≥15 s. In this case, the following algorithm was used. First of all, normotension of the patient was ensured (administration of vasopressors such as ephedrine, and/or infusion of isotonic fluids) and the patient's neck was checked. External factors causing arterial or venous obstruction were restored, if any. If no recovery was seen despite these steps, FiO2 was set at 100%. Moreover, in case of cerebral oxygen desaturation, these data were recorded and ABG was checked simultaneously. Mean values from the right and left sensors at the time of each measurement were used to evaluate rSO2.
ABG analysis
For ABG analysis, pH, partial pressure of carbon dioxide, and hemoglobin values were measured in the fifth minute postinduction with the patient in the neutral position (t1), in the 30th minute postinsufflation in the reverse-Trendelenburg position of patient (t2), and postextubation right before the patient was referred to the recovery unit (t3).
Operating times
Anesthesia, surgery, reverse-Trendelenburg, pneumoperitoneum, and recovery times were recorded. Recovery time was defined as the time from discontinuation of sevoflurane or propofol and remifentanil at the end of the surgery to the restoration of spontaneous breathing, opening of the eyes upon a verbal command, squeezing of the hand of the observer and extubation. Additionally, the complications (including nausea and vomiting) developed by the patients were also recorded.
Statistical analysis
Based on the article by Kim et al., 18 a sample size of 25 is necessary for both groups to identify a difference of 5.7 units in rSO2 values between the two groups, with a deviation of 6.9 units, at a 95% confidence limit with 80% power. Five back-up subjects were assigned to each group and enrolled in the study for both groups to make up n = 30. Data were analyzed using the Statistical Package for the Social Sciences Version 21.0 software (IBM SPSS Statistics, IBM, Armonk, NY). Data were presented as mean ± standard deviation, median (minimum to maximum), and as frequency (%). To compare the qualitative and quantitative variables, the Chi-square analysis and a Student's t-test, with a normal distribution, and the Mann–Whitney U test, without normal distribution, were used, respectively. Pearson's Correlation analysis and Spearman's Rho correlation analysis were used for data with a normal distribution and without a normal distribution, respectively, to calculate the correlation between rSO2 and ABG. A p-value <0.05 was considered statistically significant.
Results
Patients' characteristics and hemodynamic parameters
Sixty patients were enrolled in the study and all of them completed the study (Fig. 1). The demographical data of the patients in the groups were similar, whereas anesthesia time, surgical time, pneumoperitoneum time, reverse-Trendelenburg time, and recovery time were longer in the TIVA group than the Inhalation group (Table 1). In the comparison of the physiological variables (MAP, HR, SpO2, and PETCO2), no difference was found in terms of MAP and PETCO2, whereas significant differences were found in the HR and SpO2 (Figs. 2 and 3).
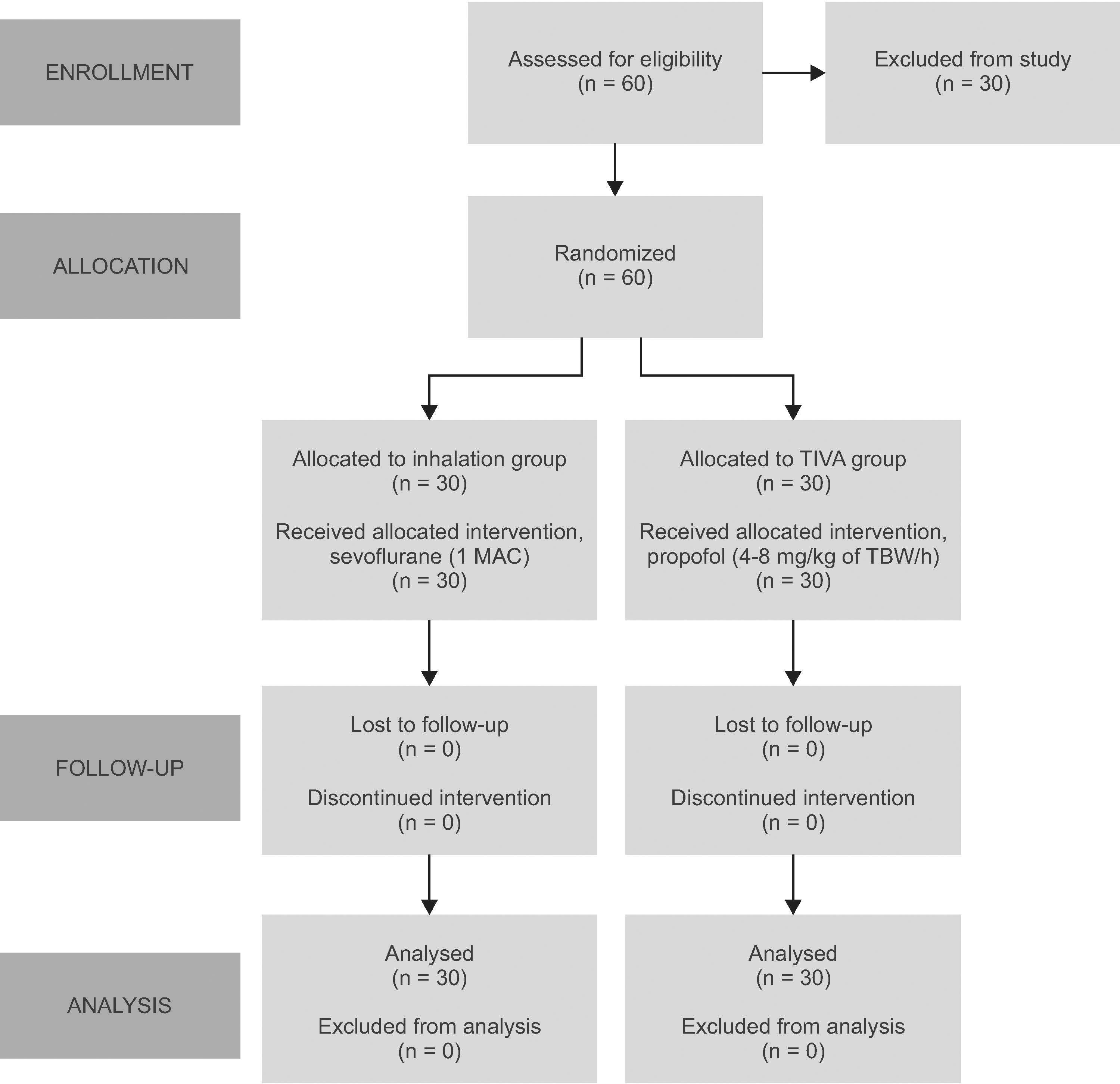
Flow diagram of patients' data distribution. MAC, minimum alveolar concentration; TBW, total body weight; TIVA, total intravenous anesthesia.
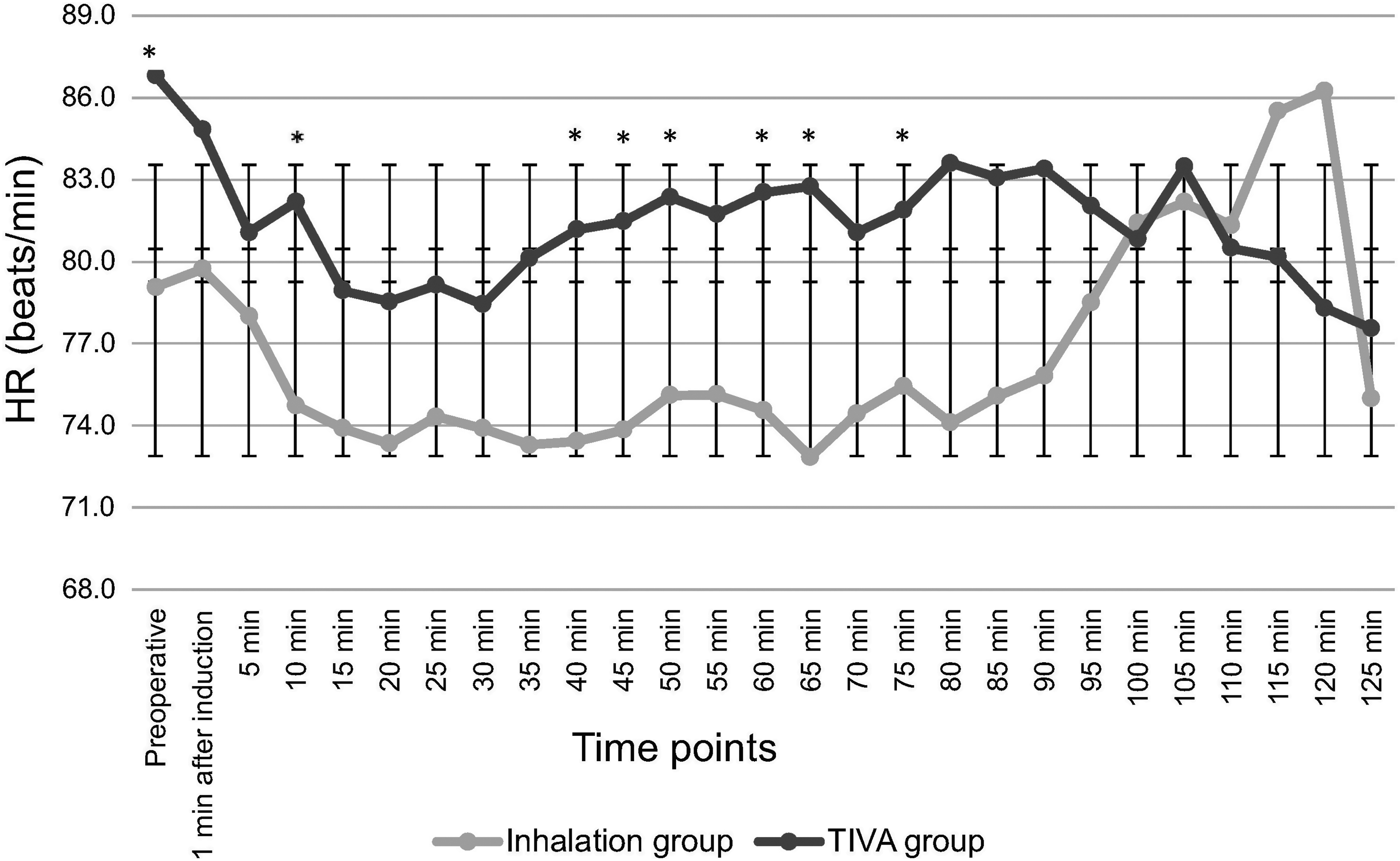
HR (beats/min) values of the groups. The error bars indicate standard deviation. *p < 0.05 statistically significant versus inhalation group. HR, heart rate.
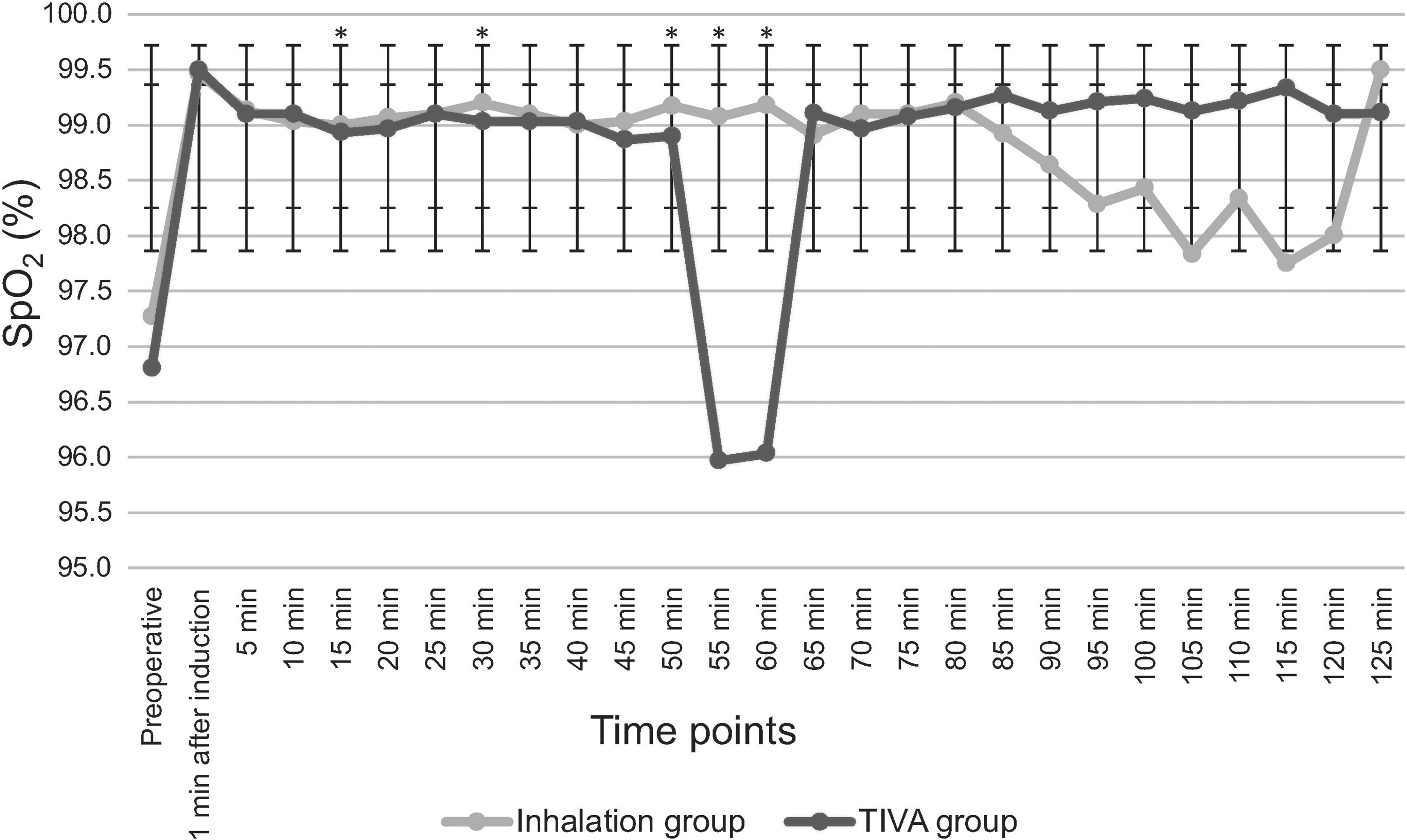
SpO2 values (%) of the groups. The error bars indicate standard deviation. *p < 0.05 statistically significant versus TIVA group. SpO2, peripheral oxygen saturation.
Demographic and Clinical Characteristics of Study Patients
Data are presented as mean ± SD, median (minimum to maximum) or number (%).
p < 0.05 statistically significant versus inhalation group. The anesthesia time, surgical time, pneumoperitoneum time, reverse-Trendelenburg time, and recovery time were longer, and also BMI was higher in the TIVA group than the Inhalation group.
Hypertension.
Diabetes mellitus (mostly noninsulin dependent), thyroid disorders.
Asthma, obstructive sleep apnea.
BMI, body mass index; Hb, hemoglobin concentration; SD, standard deviation; TIVA, total intravenous anesthesia.
The rSO2 and ABG values
No difference was found in the in-group and inter-group comparisons for rSO2, and no cerebral oxygen desaturation was observed at the follow-up (Fig. 4). When the groups were compared in terms of ABG values, a difference in pH values was found only at t1 (Table 2).
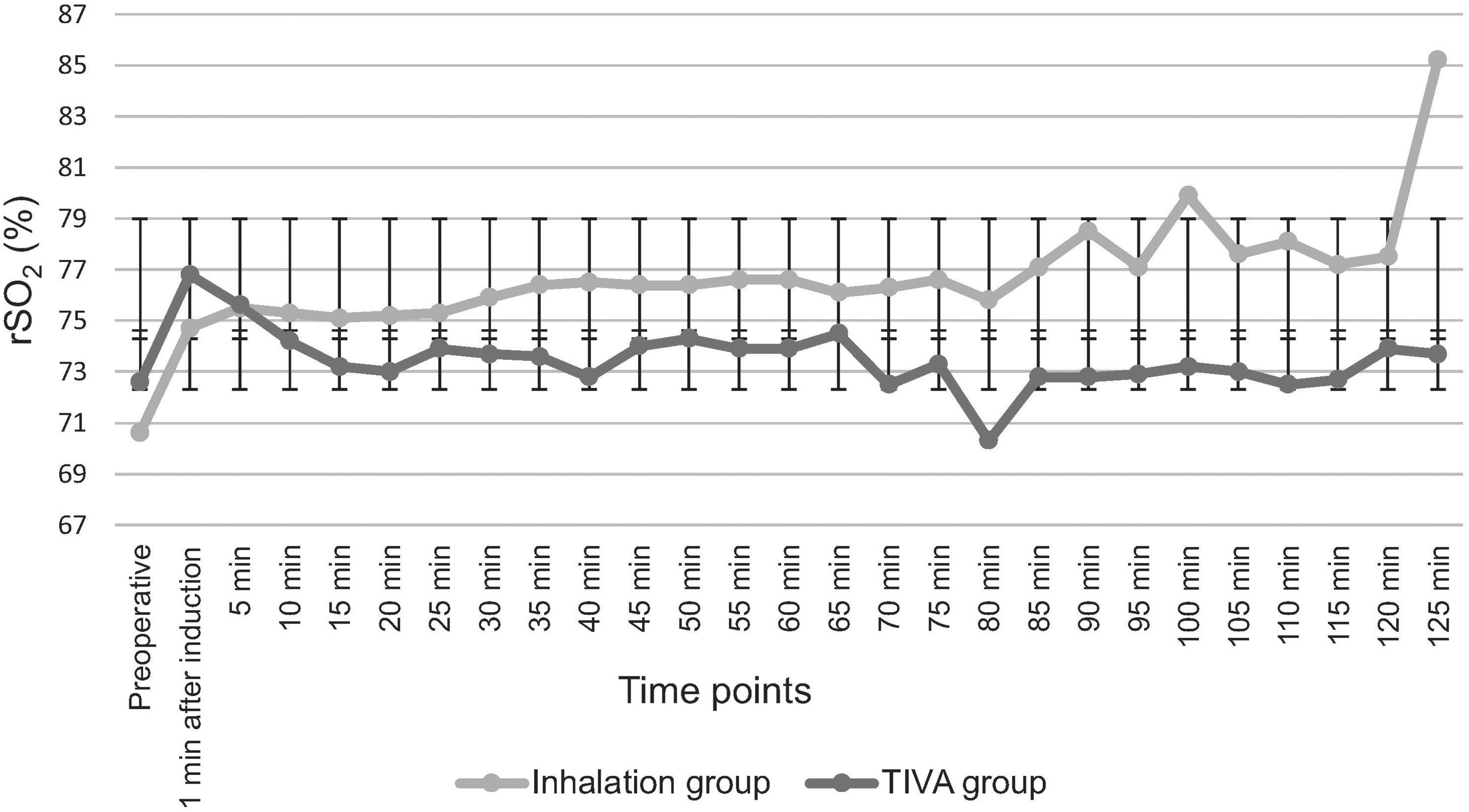
rSO2 (%) values of the groups. The error bars indicate standard deviation. rSO2, regional cerebral tissue oxygen saturation.
Arterial Blood Gas and Hemoglobin Values of the Groups
Data are presented as median (minimum to maximum). t1, 5th minute postinduction with the patient in the neutral position; t2, 30th minute postinsufflation with the patient in the reverse-Trendelenburg position; t3, right before the referral of patient to the recovery unit postextubation.
p < 0.05 statistically significant versus inhalation group.
PaCO2, partial pressure of arterial carbon dioxide; PaO2, partial pressure of arterial oxygen.
Correlations between rSO2 and ABG values
A moderate positive correlation was found between rSO2 value and Hb (hemoglobin concentration) at t1, t2, and t3. Also, at t3, a weak positive correlation and a weak negative correlation were seen between rSO2 and PaCO2 (partial pressure of arterial carbon dioxide), and between rSO2 and pH, respectively (Table 3).
Relationship Between rSO2 and Arterial Blood Gas Values at t1, t2, and t3
t1, 5th minute postinduction with the patient in the neutral position; t2, 30th minute postinsufflation with the patient in the reverse-Trendelenburg position; t3, Right before the referral of patient to the recovery unit postextubation.
p < 0.05 is statistically significant. There was a moderate positive correlation between rSO2 and Hb, and a weak positive correlation between rSO2 and PaCO2, and also a weak negative correlation between rSO2 and pH were seen respectively.
r, correlation coefficient; rSO2, regional cerebral tissue oxygen saturation.
Discussion
While no statistically significant difference was found between the Inhalation group and the TIVA group in terms of rSO2 values, none of the patients developed cerebral desaturation in the follow-up in our study. A slight increase in rSO2 values was observed in both groups following the induction of anesthesia. While this increase continued until the end in the Inhalation group, the values started to gradually decrease as of the fifth minute of anesthesia induction and progressed to near preoperative values throughout the episode in the TIVA group. Postinduction, postinsufflation, and postextubation ABG measurements were similar, and a moderate positive correlation was found particularly between Hb and rSO2 values. Additionally, recovery time was longer in the TIVA group. This situation was associated with longer anesthesia times in the TIVA group as well as propofol accumulation and slow washout. 19
The hypothesis of the study was that rSO2 is better preserved with sevoflurane than propofol-based anesthesia in morbidly obese patients who underwent LSG. One of the findings that our hypothesis was based upon was that sevoflurane could increase global CBF through direct vasodilation and, in addition, could improve rSO2 by decreasing CMRO2 (luxury perfusion).11–14 In fact, although sevoflurane is the least vasoactive agent among volatile anesthetics, it has a dual action on the cerebral venous bed like other volatile anesthetics. Cerebral vasoconstriction secondary to the suppression of cerebral metabolism is seen at low doses (<1 MAC), and its intrinsic cerebral vasodilatory action prevails when the concentration is increased (>1 MAC). Thus, global CBF exceeds the cerebral oxygen demand.11,12,14 It has been reported that sevoflurane does not increase CBF at a concentration of 1 MAC, indicating minimal vasoactivity.11,14 Also, unlike other volatile anesthetics, it preserves global CBF and metabolism coupling at concentrations up to 1.5 MAC. 17 When its regional impacts were assessed, it was seen that increasing sevoflurane concentrations (1.4% and 2.0% end-tidal) did not have an impact on CBF and rSO2 in the cortical and subcortical regions. 20 Considering all these findings, it can be concluded that the cerebral circulation and oxygen balance can be preserved without changing to sevoflurane. Another finding, which was the basis for our hypothesis, was that propofol decreases rSO2 by reducing global CBF more remarkably than CMRO2.16,17 It has been reported that propofol decreases CBF significantly both by suppressing CMRO2 and through a direct vasoconstrictive action. 16 However, the impacts of propofol on the cerebrovascular system and on neuronal activity might be dose dependent and regionally specific. Likewise, in animal experiments, propofol was able to demonstrate its vasodilating effect on large cerebral arteries at clinically relevant doses through the inhibition of extracellular calcium influx, and only at higher doses in cerebral microvessels.21,22 Additionally, in their study evaluating regional (frontal, temporal, parietal, occipital, and cerebellar) impacts of propofol, Klein et al. did not show any effect of increasing the dose of propofol (4 and 6 mg/kg/h) on CBF and CMRO2 in the cortical and subcortical regions. They attributed this finding to propofol's varying sensitivity and dose requirement between individuals and to the fact that the doses used did not reach levels that were able to impact CBF and CMRO2. 23 When higher doses of propofol (5 and 8 mg/kg/h) were used in their subsequent study, no changes were recorded in CBF and CMRO2 in the subcortical region, whereas CMRO2 decreased and CBF regionally remained the same (frontal, temporal, and parietal) in the cortex. 24 The authors attributed these results to a more distinct microvascular vasodilation and metabolic depression in the cerebral cortex. In an imaging study on healthy volunteers, Kaisti et al. reported that the impact of propofol on CBF and CMRO2 varied dose dependently in different regions of the brain. 11 Taking all these studies into account, it can be concluded that the global and regional effects of propofol on CBF and CMRO2 may be different. As a result of this difference, statistically significant changes related to CBF and CMRO2 cannot be obtained in some regions of the brain. A study measuring global cerebral oxygen saturation found that jugular venous bulb oxygen saturation was lower in the TIVA group than in the sevoflurane/nitrous oxide group, while the rSO2 measurements of the two drugs were similar. 25
It has been inferred above that clinical doses of sevoflurane do not alter cerebral oxygenation and that propofol could have different effects on cerebral oxygenation globally and regionally. However, in their imaging study on healthy volunteers, Kaisti et al. determined that 1 MAC sevoflurane and one effective plasma concentration dose of propofol (6 μg/mL) decreased CBF globally (36–53%, 62–70%, respectively). They observed that both drugs significantly reduced CBF particularly in the frontal lobe (sevoflurane 40%; propofol 67%). 26 Later, again in their imaging study on healthy volunteers, they observed that propofol decreased CBF and CMRO2 by ∼60% when sevoflurane (1.5 MAC) and propofol (3.7 μg/mL) were compared, with the bispectral index (BIS) value being 40. While sevoflurane provided a lesser decrease in CBF than propofol, the decrease in CMRO2 was interestingly similar to propofol. Likewise, they found that the decrease in CBF (propofol 43%; sevoflurane 13%) and CMRO2 (propofol 39%; sevoflurane 30%) were similar to the global changes particularly in the frontal lobe. 11 When these two studies are taken into consideration, the rSO2 values can be expected to be higher with sevoflurane than with propofol in healthy individuals in the supine position. However, it is possible that the presence of factors that could affect rSO2 values and mask the effects of anesthetic drugs on cerebral oxygenation (the reverse-Trendelenburg position and pneumoperitoneum) led to similar rSO2 values in both drugs in our study. In their studies on cases of total hip arthroplasty and arthroscopic shoulder surgery, respectively, Yoshitani et al. and Jeong et al. did not find a difference between sevoflurane and propofol in terms of rSO2 values.25,27 Valencia et al. attributed the results in these two studies to the use of nitrous oxide (which increases CBF and CMRO2) and the presence of other factors (i.e., loss of hemoglobin, beach chair position) that could affect cerebral oxygenation. 28 In a subsequent study on cases of minor surgery in the supine position without using nitrous oxide, Valencia et al. found that the rSO2 values in the sevoflurane group were higher than the propofol group, confirming this interpretation. 28 On the contrary, in gynecological laparoscopic surgery cases, Kim et al. found rSO2 values in the sevoflurane group to be higher than the propofol group during pneumoperitoneum in the Trendelenburg position and after desufflation of the abdomen in the neutral position. 18 In their study conducted on laparoscopic cholecystectomy cases, Ruzman et al. also found rSO2 values of the sevoflurane group to be higher than the propofol group at all time points. 29 In both of these studies, the authors associated the results with the effect of sevoflurane causing luxury perfusion. In the present study, the results were in favor of sevoflurane although other factors were present in these two studies that could have affected the results. On the contrary, in their pilot study on laparoscopic cholecystectomy cases, Sen et al. did not find any difference in terms of rSO2 values between the groups during pneumoperitoneum in the reverse-Trendelenburg position. 30 As can be seen, there are many studies on the effects of sevoflurane and propofol on cerebral oxygenation in the literature with contradicting results. It is currently not possible to find a satisfactory explanation for such a contradiction. However, the authors of this study believe that the use of different animal species in the studies or the lack of a control group in certain studies or investigation of only global or only regional changes in some other studies could have contributed to such contradicting results.
Limitations
The present study has various limitations. First, the depth of the anesthesia might have varied during the study as the doses of anesthetic agents were not set according to a BIS value that would provide an adequate hypnotic level. It is possible that this situation affected the rSO2 values in our study by altering CBF/CMRO2 coupling, which is sensitive to the depth of general anesthesia. 31 In addition, the CMRO2 values of the cases may not have been kept stable throughout the study as cortical electrical activity could not be monitored with BIS. Additionally, there is a linear correlation between BIS values and the impact of propofol and sevoflurane on the cerebral metabolism. 32 Second, the fact that induction by propofol was used instead of vital capacity inhalation induction might be considered a limitation. The vital capacity inhalation induction technique was not the preferred one in our study due to its side effects (such as airway-related events [cough, hiccups], purposeful movements) and the patients defined this technique as unpleasant; however, this may have affected the results due to the mix-up of the effects of the two agents. 33 The third limitation might be the inclusion of only ASA II patients in our study. If ASA III–IV patients had been enrolled in this study, the changes in rSO2 might have been more remarkable due to the potential cardiovascular and cerebrovascular diseases in these patients. Another limitation is that the present study did not evaluate the postoperative neurocognitive functions of the patients although a correlation has been demonstrated in the literature between lower intraoperative rSO2 and the appearance of postoperative cognitive deficits. 34 Therefore, it is not possible to evaluate the effects of different anesthetics and changes in rSO2 on the neurocognitive outcomes.
Apart from these, there are some limitations related to the NIRS technique. For cerebral oxygenation, it is ideally recommended to assess CBF and oxygenation in different regions of the brain in a compartment-specific manner (arterial, interstitial, venous). 35 NIRS, however, is a technique that assesses arterial and capillary components, where the majority (75%) of data belongs to the venous system. Moreover, NIRS assumes that there is a constant arterial/venous ratio (25/75%) in the microvascular structure of the brain tissue. 36 However, this ratio may have been changed by sevoflurane, propofol, and changes in the body position.11,37 Consequently, NIRS may yield misleading results although there is no real change in oxygenation. Furthermore, the fact that normal values vary significantly between individuals, that there is no absolute critical cutoff value, that it shows oxygenation only in the frontal cortex, and that it does not reflect global oxygenation (considering that the metabolism and CBF vary significantly in different regions of the brain even in healthy individuals), prevent NIRS from being commonly used in the monitoring of cerebral oxygen.25,26
Conclusion
To the authors' knowledge, the present study is the first research in the literature comparing the effects of TIVA and inhalation anesthesia on the changes in rSO2 values in LSG cases. Although a decrease was expected in rSO2 values when propofol anesthesia and sevoflurane anesthesia were compared, the findings of the present study demonstrate that both anesthetic regimens preserve cerebral oxygen saturation. However, it should be emphasized that this study did not include ASA III–IV patients. The authors believe that further studies are needed that enroll patients with comorbidities potentially affecting cerebral perfusion and that also evaluate postoperative cognitive functions to support the results of the present study.