
Abstract
Background:
Laparoscopic Roux-en-Y gastric bypass (LRYGBP) and laparoscopic sleeve gastrectomy (LSG) are the most common bariatric procedures globally and they have been reported to impart similar weight loss outcomes. However, their effects on gastrointestinal quality of life (GIQoL), which is a major determinant of patient satisfaction, are less well defined. This meta-analysis aims to compare GIQoL in patients who have undergone LRYGBP or LSG.
Methods:
A systematic review and meta-analysis of the studies comparing changes in the gastrointestinal quality of life index (GIQLI) scores after LSG or LRYGBP was performed. This meta-analysis is exempt from ethical approval because the data is collected from the clinical studies in which informed consent has already been obtained by the study investigators.
Results:
Six studies including 1726 patients were included. Although there was a significant improvement in GIQoL after bariatric surgery (LSG mean difference [MD] −14.98, 95% confidence interval [CI], −22.28 to −7.69, p < 0.0001; LRYGBP [MD] −16.99, 95% CI, −26.28 to −7.71, p = 0.0003), there was no significant difference in GIQLI scores between LSG and LRYGBP in short- or long-term follow-up in random effect meta-analysis.
Conclusion:
Bariatric surgery is associated with significant improvements in GIQoL, and similar changes in this outcome measure are reported after LSG and LRYGBP. It is infrequently reported in the bariatric literature and inclusion of this relevant patient-reported outcome measure in future bariatric studies is recommended.
Introduction
Obesity is conventionally defined as a body mass index (BMI) of ≥30 kg/m2. It is increasingly prevalent and it is associated with increased risk of developing metabolic comorbidities, including type 2 diabetes, cardiovascular disease (CVD), and nonalcoholic fatty liver disease (NAFLD). Obesity and these associated comorbidities are known to have a significant detrimental impact on an individual's quality of life (QOL) and represent a considerable economic burden for global health care systems1,2
Bariatric surgery is regarded as the most effective method of achieving durable weight loss. The two most commonly performed bariatric procedures are laparoscopic Roux-en-Y gastric bypass (LRYGBP) and laparoscopic sleeve gastrectomy (LSG), 3 and it has been reported that these operations are similarly effective at reducing body weight. 4 Bariatric surgery with medical therapy has been shown to be superior for the treatment of type 2 diabetes mellitus in comparison with medical therapy alone. 5 There are emerging reports of its beneficial effects in the treatment of CVD 6 and NAFLD. 7 However, the anatomical and physiological gastrointestinal (GI) tract changes induced by bariatric surgery have also been associated complications that may be lead to a deterioration in QOL for some patients. 8
The gastrointestinal quality of life index (GIQLI) is a patient-reported outcome (PRO) tool that has been validated for use in GI disease and to assess the effects of GI tract operations on QOL. 9 It assesses disease-specific health-related QOL as well as psychosocial well-being and GI-specific symptoms. Symptoms resulting from gastroesophageal reflux disease (GERD), biliary disease, irritable bowel syndrome (including bloatedness and abdominal pain) are more prevalent in individuals with obesity than nonobese controls, leading to poorer GIQLI.1,2,10–12
Since GI symptoms have also been reported after bariatric surgery, it is not clear whether postoperative weight reduction might “normalize” gastrointestinal quality of life (GIQoL), and an evaluation of the effects of common bariatric operations on GIQoL would be of value. We hypothesize that there is no difference in GIQLI score between LSG and LRYGBP because Biter et al. 13 found no difference in QOL scores between these two procedures along with significant improvement in QOL scores after bariatric surgery without any difference in complication rates between the two procedures. The aims of this review are to clarify the impact of bariatric surgery on GIQLI and whether LRYGBP is associated with a differential effect on GIQLI when compared with LSG.
Methods
Search strategy
We conducted a comprehensive literature search of MEDLINE, Embase, CINAHL, Cochrane Library, and Clinical Trials Registry database with adherence to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 14 The search strategy was devised in collaboration with a professional health care librarian. Search terms used included “Gastrointestinal quality of life” OR “GIQLI” AND “Laparoscopic sleeve gastrectomy” OR “Laparoscopic Roux-en-Y gastric bypass” OR “LSG” OR “LRYGBP.” All citations were imported into Covidence, which is a dedicated software platform for systematic reviews and meta-analysis. All citations and abstracts identified were reviewed by independent investigators (A.T./E.C.). The last date for this search was January 31, 2020. The review was registered with international prospective register for systematic reviews—PROSPERO with registration number CRD42018097435. 15
Study selection
The literature search was independently performed by two authors (A.T. and E.C.). The abstract of each study was then reviewed by both authors to exclude those that did not satisfy the inclusion criteria and full copies of the remaining studies were obtained. Only studies that met the inclusion criteria were used for data extraction. If there was any doubt regarding these criteria, the full article was retrieved for clarification. The references of the selected studies were manually searched to identify additional relevant studies. Differences of opinion between the two authors (A.T. and E.C.) were resolved by discussion with the senior author (B.S.) with his decision considered final in the event that consensus was not reached.
Inclusion criteria
Human studies, including randomized controlled trials (RCTs), cohort studies, and retrospective observational studies that compared the GIQLI scores after LSG and LRYGBP, were included in the review. For studies that published duplicate or overlapping data sets, only the most recent report providing the highest level of evidence was included.
Exclusion criteria
Nonhuman studies, studies reporting nonsurgical interventions, case reports, small case series (<10 cases) and non-English reports were excluded 16 along with conference abstracts and editorials. Studies evaluating the effect of bariatric surgery on patients with renal failure, liver cirrhosis, and pulmonary hypertension were also excluded.
Outcome measures
Primary outcome
Comparison of GIQLI scores between LSG and LRYGBP in the first postoperative year and at >12 months. These time points were selected as GIQLI scores were consistently reported in the first postoperative year, but relative weight stability is achieved later, so the analysis of studies with longer-term follow-up is also required.
Secondary outcomes
Comparison of GIQLI scores before and after LSG or LRYGBP surgery.
Complications after LSG and LRYGBP. Complications were defined as events after surgery, which required medical or surgical intervention.
Data extraction
Primary and secondary outcomes data were collected by the primary author (A.T.) and independently confirmed by the second review author (E.C.) using the Covidence program. Study characteristics, including first author, year of publication, type of study (prospective or retrospective case controlled studies or randomized clinical trials), number of patients, patient demographics, inclusion and exclusion criteria, were recorded. Corresponding authors of all included studies were contacted to request the provision of any missing data.
Statistical analysis
Statistical analysis was undertaken using REVMAN 5.0. Data were pooled and mean differences (MDs) with their corresponding 95% confidence intervals were calculated for continuous data and risk ratios (RRs) were calculated for dichotomous data. The I2 statistic was used to estimate the heterogeneity of included studies. I2 > 50% was considered reflective of significant heterogeneity. A random effects model was used as the effects were expected to be heterogeneous due to the variety of study populations and study design included in the analysis. 17 A p-value of <0.05 was considered statistically significant.
Quality assessment
Two review authors (A.T. and E.C.) assessed the risk of bias and quality of studies independently. For nonrandomized studies, the MINORS criteria 18 was used to assess the quality of studies. The Jadad scoring system 19 was used to assess the quality of randomized studies. The maximum achievable global score for nonrandomized studies as per MINORS criteria is 24. 18 The highest score was 1920 and lowest score was 16. 21 The included randomized studies assessed to be of relatively low quality when assessed according to the Jadad scoring system (Table 1).
Quality of Randomized Control Trials
Results
Description of studies
The search conducted through the specified databases identified 888 articles, 758 of which remained after exclusion of duplicates and animal studies. After title and abstract reviews, 548 studies were excluded, as it was determined that they did not meet our inclusion criteria. Of the remaining 210 articles, an additional 204 studies were then excluded as their study design, patient population, study setting, or reporting format (e.g., conference abstract) did not meet our criteria for inclusion (Fig. 1). After full text review, six studies20,22–24 were included in this review. Three randomized control trials,13,22,23 two prospective cohort studies,20,21 and one retrospective cohort study 24 were identified.
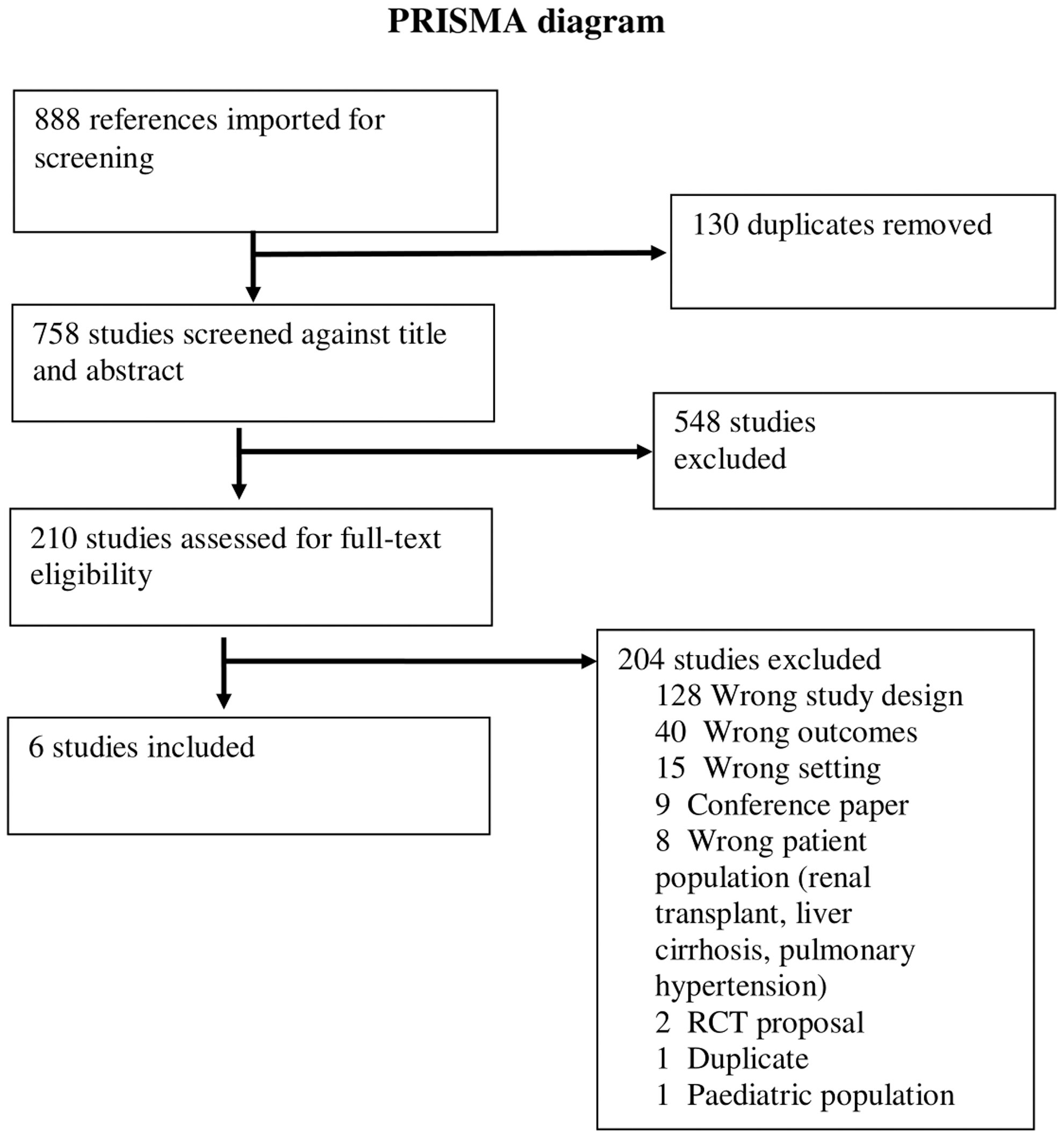
PRISMA diagram showing study selection for the review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study and patient characteristics
A total of 1726 patients were included in 6 studies,13,20–24 of which 864 patients underwent LSG and 862 patients underwent LRYGBP. The mean age reported in LSG group ranged from 35.2 to 45.5 years and in LRYGBP group was 35.1–43.8 years. There was no difference in patient characteristics in the included studies. The included studies adopted similar inclusion criteria for BMI except for the study by Lee et al., 24 in which the mean BMI was similar (37.5 kg/m2 for both the LRYGB and LSG groups) but the BMI range was wider (25.8–75.3 kg/m2). The inclusion of patients with BMI <30 kg/m2 in this study of patients undergoing primary bariatric surgery may be due to the different BMI thresholds for classifying overweight and obesity in China compared with western countries 25 (Table 2).
Studies and Patient Characteristics
LRYGBP, laparoscopic Roux-en-Y gastric bypass; LSG, laparoscopic sleeve gastrectomy; RCT, randomized controlled trial.
Primary outcome
GIQLI scores in the first postoperative year after LSG or LRYGBP
Four studies13,21–23 compared the GIQLI scores between LSG and LRYGBP 12 months after the procedure with no reported significant difference in mean scores (MD of 2.12, 95% confidence interval [CI], −3.36 to 7.61, p = 0.45). Heterogeneity was 70% (Fig. 2).
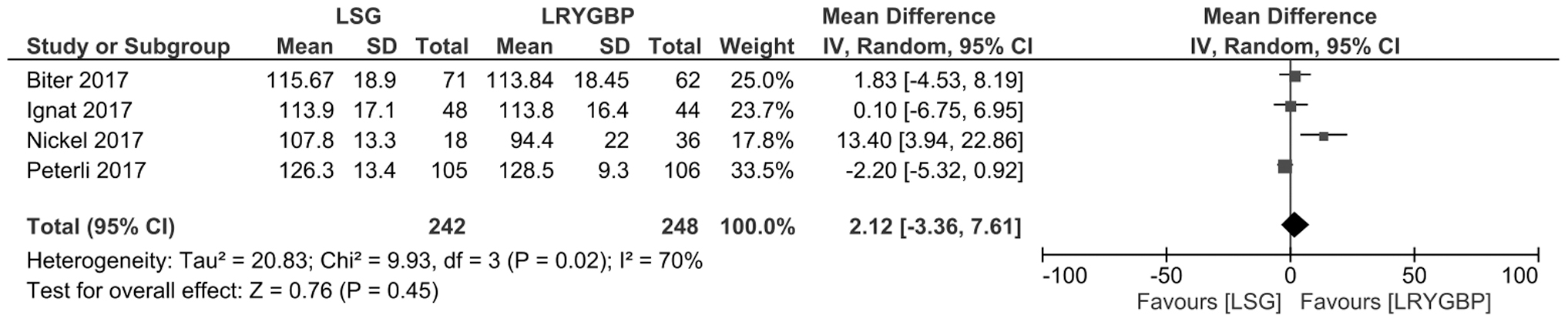
Comparison between GIQLI score at up to 12 months follow-up after LSG and LRYGBP. GIQLI, gastrointestinal quality of life index; LRYGBP, laparoscopic Roux-en-Y gastric bypass; LSG, laparoscopic sleeve gastrectomy.
GIQLI scores between 12 months and 5 years after LSG and LRYGBP
All six studies13,20–24 additionally reported and compared longer-term GIQLI scores after both operations. There was no significant difference in the mean GIQLI scores reported up to 5 years after LSG or LRYGBP (MD of −1.84, 95% CI, −4.73 to 1.05, p = 0.21). There was no heterogeneity in the studies (Fig. 3).
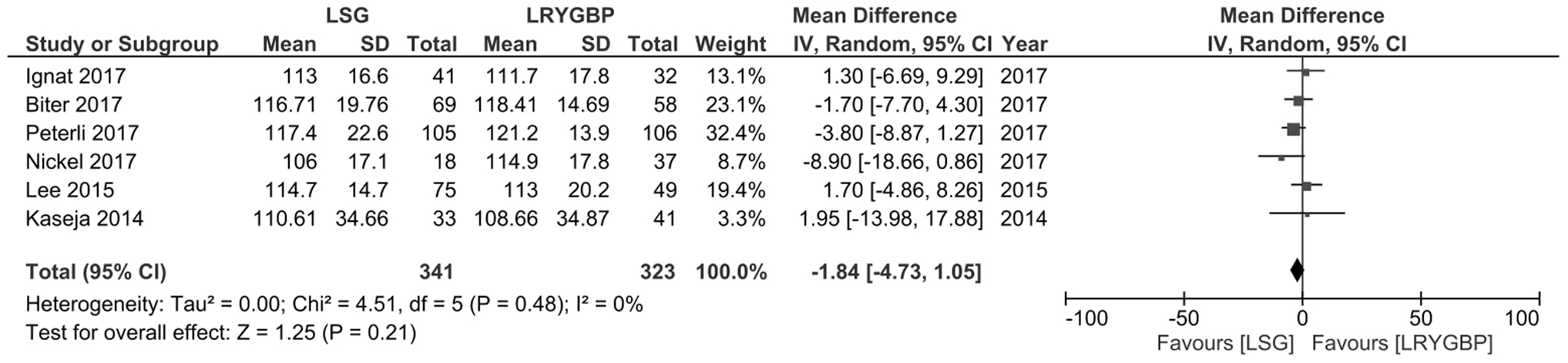
Long-term gastrointestinal quality of life after LSG and LRYGBP.
Secondary outcomes
Comparison of GIQLI scores pre- and postbariatric procedures
GIQLI scores before and after LSG and LRYGBP are reported in five studies.13,21–24 Significant improvement in GIQLI has been reported after both bariatric procedures. For LSG an MD of −14.98, 95% CI, −22.28 to −7.69, p < 0.0001, heterogeneity of 87% was observed and compared with MD of −16.99, 95% CI, −26.28 to −7.71, p = 0.0003, heterogeneity of 92% after LRYGBP (Figs. 4 and 5).
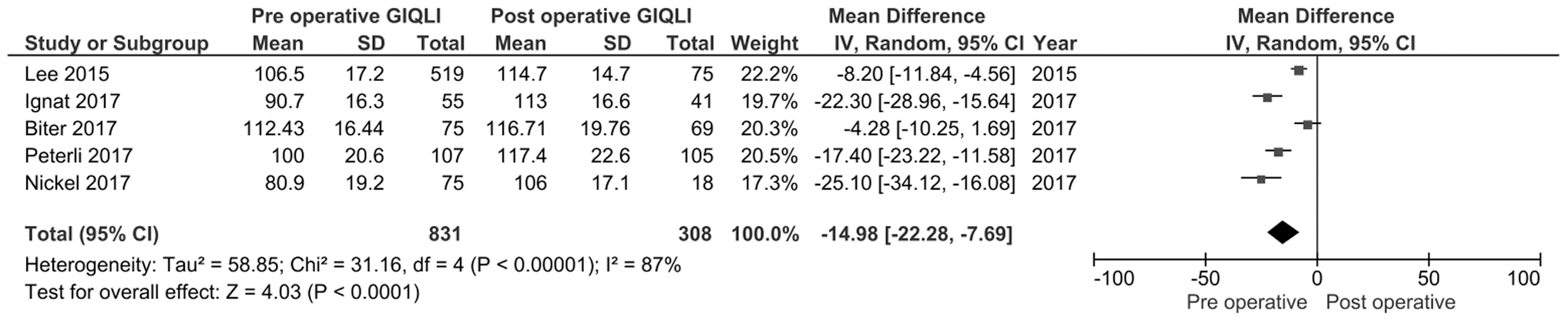
Comparison of pre- and postoperative GIQLI after sleeve gastrectomy.
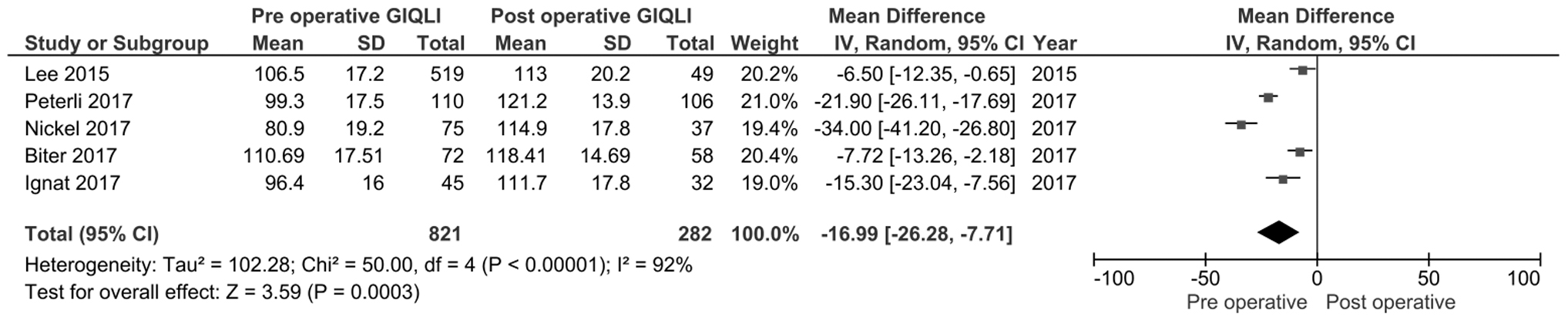
Comparison of pre- and postoperative GIQLI after Roux-en-Y gastric bypass.
Complications
Overall complication rate between two groups was reported in five studies13,20,22–24 with range of 3–8.4% in LSG group and 2.4–14% in LRYGBP. The difference between the two groups was statistically significant (6.9% [55/790] vs. 10% [79/789]) with a combined RR of 0.7 (95% CI 0.5–0.97, p = 0.03). There was no heterogeneity in the studies (Fig. 6).
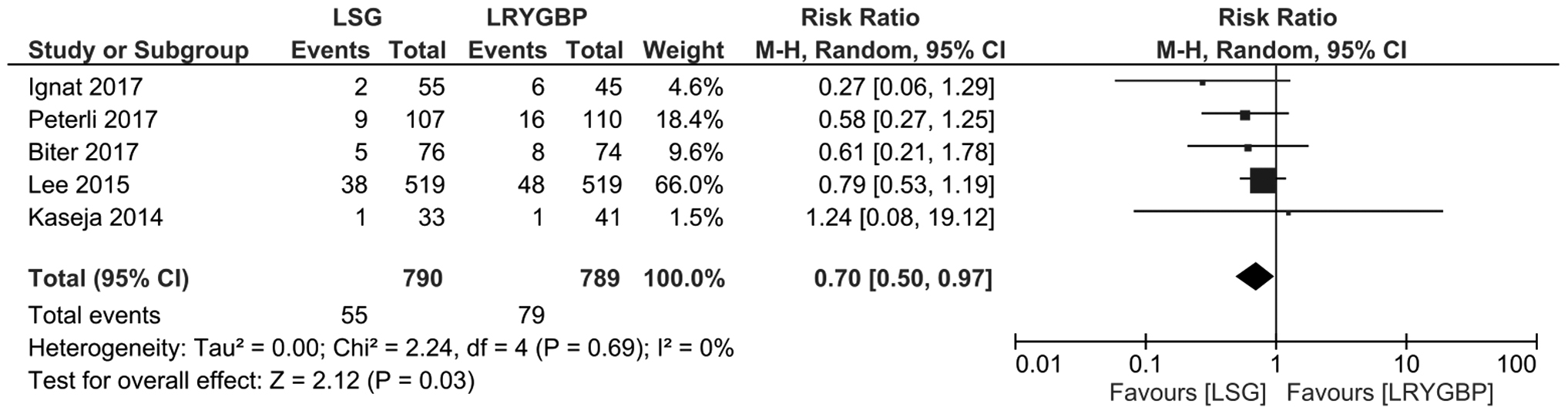
Comparison of complications events after LSG and LRYGBP.
Discussion
Primary findings
This meta-analysis supports the hypothesis that GIQLI scores in patients who underwent LSG and LRYGBP surgery are not significantly different. Baseline characteristics were similar between the two groups. This finding is consistent with a recently published meta-analysis by Hu et al., 26 which compared postoperative GIQLI scores but did not include preoperative data. Our meta-analysis, therefore, improves on this existing evidence by providing an additional comparison of the GIQoL pre- and postsurgery for the two procedures. All the included studies except Kaseja et al. 20 reported longitudinal analysis after bariatric surgical intervention. There was no difference observed in all six studies between GIQLI scores after intervention in both groups.13,20–24 Sustainable improvement of GIQLI scores and Bariatric Analysis and Reporting Outcome System (BAROS QOL) scores was observed by Peterli et al. 22 in both groups up to 3 years even though GERD is more efficiently improved in LRYGBP than LSG in long term. Early improvements in GIQLI scores after LSG were higher than after LRYGBP, but no significant difference was observed in longer term comparisons.13,21 Kaseja et al. compared postoperative GIQLI scores and found no difference between two groups. 20
In addition to well-described cardiometabolic consequences, obesity is also associated with a detrimental impact on GIQoL. Our study has shown that GIQoL significantly improves in patients with obesity after bariatric surgery. One explanation for this finding may be that preoperative disease such as GERD, which is associated with increased intra-abdominal pressure and known to be more prevalent in individuals with obesity, may improve after surgically induced reductions in visceral adipose tissue and hepatic steatosis. 5 Impaired GIQoL is not currently recognized in national guidelines as an indication for bariatric surgery, and our analysis found few previous studies addressing this topic. Robust prospective longitudinal studies would be beneficial to determine whether bariatric surgery may represent a promising intervention for the combined treatment of obesity and adverse GIQoL scores.
The relatively higher complication rate observed after LRYGBP compared with LSG in this review is consistent with rates reported in the existing literature,4,26–29 and GI complications are known to vary between these interventions. Internal herniation, anastomotic strictures, and marginal ulceration have been reported after LRYGB, whereas GERD and gastric strictures are more characteristic of LSG. 8 However, previous studies that performed GIQLI subscore analysis detected no significant difference in core GI symptoms such as abdominal pain, bloating, bowel frequency, restricted eating, fatigue, and flatulence.21,23,24 The higher reported complication rates reported after LRYGB compared with sleeve gastrectomy should be weighed against potentially greater improvements in specific comorbidities (such as GERD) in a shared decision-making process. 26
Strengths and limitations
The strengths of our meta-analysis include use of recommended methodology, including prospective registration and adherence to PRISMA guidelines. The search strategy was comprehensive and conducted by a professional health care librarian, with independent reviews of the identified studies by two authors. This meta-analysis is also the first to have described longitudinal changes in GIQoL in patients with obesity undergoing bariatric surgery. GIQoL was chosen as the primary outcome measure because GI symptoms are reported to be more common in people with obesity and adversely affect well-being. The retention rates of the patients reported in majority of the studies are >80% (Table 2). The importance of QOL after bariatric surgery has been increasingly recognized30,31 and patient-reported outcome measures assessing this have been incorporated into the design of several recently published and ongoing RCTs. 30 No meta-analysis has previously described longitudinal changes in GIQoL after bariatric surgery. We performed an additional analysis of LSG and LRYGBP interventions in which we compared longitudinal changes in GIQLI score. This repeated-measures analysis is considered more statistically powerful and robust than comparing cross-sectional postintervention scores alone. 32 Bariatric surgery may, therefore, represent a potential intervention for the combined treatment of obesity and impaired GIQoL. We hope that our findings will both inform patient-centered care and stimulate additional patient-centered research in this area.
However, the number of studies meeting our prespecified criteria was small. Only three of the included studies were RCTs—all of low quality and the other three studies were nonrandomized with low score when assessed using the MINORS criteria. The small number of low-quality studies limits the strength of the conclusions that can be drawn from this meta-analysis. In addition, the inclusion criteria were not clearly defined in the retrospective study from Lee et al., 24 which accounts for more than half of the subjects in this review. Although surgical science has advanced in recent years, surgical RCTs remain relatively infrequent, often in part due to a lack of surgeon and patient equipoise and specific methodological challenges such as blinding. In contrast, nonrandomized studies may be more representative of actual clinical practice. 33 The inclusion of nonrandomized observational studies in meta-analysis is, therefore, becoming more prevalent,34,35 although their inclusion in systematic review and meta-analysis remains controversial because causal inference is limited and the comparison of interventions may be confounded by selection bias.
Conclusion
This meta-analysis has shown that there is no difference in GIQLI scores at 1 and 5 years between LSG and LRYGBP. There was significant improvement in GIQLI scores after LSG and LRYGBP. GIQoL is an infrequently reported outcome measure in the bariatric literature and its inclusion in future randomized studies would be beneficial in improving the quality of available evidence and to enhance clinical care.
Footnotes
Author Disclosure Statement
A.T., K.A., E.C., R.G., and B.S. have no competing financial interests exist. N.D. is a University of Oxford Novo Nordisk Clinical Research Fellow.
Funding Information
No funding was received for this study.