
Abstract
Abstract
Background and Objectives:
Lack of physician knowledge about breastfeeding is associated with decreased initiation and continuation of breastfeeding by patients. We evaluated the effects of a breastfeeding education program on physicians' breastfeeding knowledge, attitudes, and beliefs, measured changes in clinical practice, and examined breastfeeding rates of patients of participating physicians.
Study Design and Methods:
Six breastfeeding sessions addressed breastfeeding problem-solving and counseling and specific clinical issues including mastitis, perceived insufficient milk, poor infant weight gain, and return to work. We measured physicians' breastfeeding knowledge, attitudes, and beliefs before and after curriculum implementation and also measured changes in practice. We analyzed breastfeeding rates of patients in the practice before, during, and after the intervention.
Results:
We studied 24 residents and 15 faculty members at the intervention site; there were 12 residents and nine faculty in a similar control program. Attendance at education sessions improved breastfeeding knowledge (p<0.01) and attitudes/beliefs (p=0.03). Participants identified 15 unique practice changes with a strong commitment to make these changes (4.7 on a 5-point scale) and fulfillment of practice change of 3.6. Participation in education sessions improved patients' rates of any breastfeeding at 4 and 6 months and of full breastfeeding at 4 months.
Conclusions:
A breastfeeding education program at a semirural residency program improved physicians' breastfeeding knowledge. Implementation of practice changes was fair. Two years into the intervention, breastfeeding rates improved for patients of the physicians with high levels of participation in the program.
Introduction
Improvement of breastfeeding rates in the United States is an important public health issue; it has been included as a Healthy People 2020 goal 14 and was the subject of the Surgeon General's Call to Action to Support Breastfeeding in 2011. 15 Breastfeeding is a health disparities issue because infants of mothers with poor educational achievement or low socioeconomic status are less likely to engage in any breastfeeding or exclusive breastfeeding or to continue breastfeeding if they have begun.15–17 Improving physician knowledge and skills regarding breastfeeding management may be critical to improving breastfeeding rates. Family physicians are uniquely situated to manage breastfeeding problems as they care for both mother and infant in the context of the family. Rural populations of patients, who are less likely to breastfeed, are also more likely to be cared for by family physicians. Thus, improving counseling and medical management of breastfeeding could have a large impact at a population level.18,19 Almost all prior breastfeeding education interventions have examined provider knowledge or performance with standardized patients, but not breastfeeding rates of actual patients.20–25
We developed an educational program in medical breastfeeding management for the residents and faculty at a semirural family medicine residency program. The content was based on core medical knowledge and patient care principles developed by the Academy of Breastfeeding Medicine (ABM), from “What Every Physician Should Know About Breastfeeding,” a basic breastfeeding medicine precourse offered at the annual meeting. We evaluated the effectiveness of the curriculum in three ways: a written pretest and posttest of breastfeeding knowledge, attitudes, and beliefs; an analysis of breastfeeding practice changes made by those who participated in the curriculum; and an evaluation of breastfeeding rates on patient panels of both residents and faculty in the continuity clinic setting. These analyses were designed to determine if participation in the curriculum improved both physician knowledge and clinical breastfeeding outcomes.
Subjects and Methods
Participants and setting
The New Hampshire-Dartmouth Family Medicine Residency program is an eight residents per year program at Concord Hospital (Concord, NH), a 240-bed community hospital in central New Hampshire with a primarily rural catchment area. It is the clinical site for the Geisel School of Medicine at Dartmouth family medicine residency and a primary site for family medicine medical student clerkships. It is the only family medicine resident training program in the state. The family medicine continuity clinic serves a mainly medically indigent patient population of 25,000 patients. At the time the project began in July 2007, there were 19 full-time faculty members from the various primary care specialties of family medicine, pediatrics, internal medicine/geriatrics, obstetrics/gynecology, and behavioral health. The educational intervention was open to faculty and residents during the 2007–2008 academic year. The Institutional Review Board of Concord Hospital approved this study.
Educational interventions
The breastfeeding curriculum content for the residency was adapted from the ABM's course “What Every Physician Should Know About Breastfeeding.” The educational sessions involved the following six components:
1. A case-based seminar for the postgraduate year (PGY)-1 residents is a part of their first-year nursery/inpatient pediatrics rotation. Often, the supervisory PGY-2 and −3 residents participate. In this session, basic issues are covered, such as recommended breastfeeding duration and exclusivity, breastfeeding benefits, barriers to successful breastfeeding in the newborn hospitalization, normal breastfeeding patterns and weight gain, and related issues for primary care such as return to work, introduction of solid foods, resources for maternal medication use, etc. An International Breastfeeding Certified Lactation Consultant (IBCLC) joins to talk about correct latch, some troubleshooting techniques for excessive weight loss, supplementation, and the services that the lactation program provides. 2. Most faculty physicians at our institution give Grand Rounds once every few years. As there is mostly a primary care audience, the Grand Rounds given as part of this curriculum was based upon “ABM protocol #14: Breastfeeding-Friendly Physician's Office, Part 1: Optimizing Care for Infants and Children.”
26
3. When the PGY-2 residents are on their outpatient pediatrics month, they spend one morning on inpatient nursery rounds with an IBCLC and an afternoon seeing outpatient visits in lactation clinic. 4. Part of the noon conference curriculum within the family medicine residency involves quality improvement, where different teams, working on different problems, present clinical data about improvement efforts in the outpatient setting. This was the venue used for examining baseline breastfeeding rates, duration, and exclusivity in the health center population, prior to any projects to actually make improvements in this setting. 5. All PGY-2 and PGY-3 residents (together with a faculty member) present a journal club each year, usually on a meta-analysis or large randomized trial about an important primary care issue. During the period of this curricular intervention, a resident presented her journal club on a meta-analysis of 38 randomized controlled trials of breastfeeding promotion strategies in primary care settings in developed countries. The presentation demonstrated that educational programs in primary care settings had a significant effect on both initiation (relative risk 0.23; 95% confidence interval 0.12–0.34) and short-term duration (relative risk 0.39; 95% confidence interval 0.27–0.50).
9
6. A 2-hour workshop with structured clinical encounters and role-playing with standardized patients. These were done in small groups of four residents so that each resident had to role-play one of the provider roles in one of the scenarios. The standardized patients were either faculty members or were breastfeeding mothers recruited from the community. There were 15 minutes to role-play and 15 minutes to review each of the scenarios. The topics included mastitis, slow weight gain/failure to thrive, returning to work, and avoiding medically unnecessary supplementation.
All curriculum materials are available from the corresponding author at Alison.v.holmes@hitchcock.org
Two of the authors (A.V.H. and A.Y.M.) were new faculty members at the start of the curriculum. As they were expected to develop teaching materials and make them fit in with resident education, the six breastfeeding modules were fit into an already present curricular structure. It was fairly straightforward to teach in a case-based manner on the nursery/inpatient pediatrics rotation, where breastfeeding had always been considered a core curriculum topic, and there are 45 minutes of teaching time 4 days per week. In prior years, this session had been taught by an IBCLC only, was not a full 45-minute seminar, and was not case-based—it had been more of just an introduction to the services provided by the lactation department and had not focused on clinical reasoning. Grand Rounds topics are left up to the discretion of the presenting faculty member, and a primary care focus engages the audience, as most attendees are primary care clinicians. It is, again, an expectation that faculty members will present in this venue. The coordinator of the outpatient pediatrics curriculum had been having difficulty finding sufficient learning experiences, so adding a day of lactation for the PGY-2 residents was a welcome addition. The noontime quality improvement sessions occurred once per month, so for any improvement project, time was allotted for presentation. As all PGY-2 and PGY-3 residents are required to present journal club twice during residency, it was not out of the ordinary that one would want to present on a breastfeeding topic. Every 2 weeks a 2-hour workshop session is held on Wednesdays, so that methods such as structured clinical role-playing or procedural skills are given sufficient attention. The breastfeeding workshop fit well into this time slot.
Outcomes measures
Test of knowledge, attitudes, and beliefs
We excluded from the project three faculty members who did not routinely see breastfeeding dyads and one faculty member who facilitated the project (A.V.H.). All but one of the remaining 15 faculty members and 22 of 24 residents completed a validated test of breastfeeding knowledge, attitudes, and beliefs. 7 We chose for our control group the Maine-Dartmouth family medicine residency program in Augusta, ME, which has 21 faculty, 29 residents, and a similar rural and medically indigent patient population. There is no formal breastfeeding curriculum at the control site. From the control program, nine faculty and 12 residents completed the pretest, which included items on demographic data and factors known to affect breastfeeding outcomes. Content of the test was divided into knowledge and attitudes/belief items, and we calculated composite knowledge and attitudes/beliefs scores. Posttests were conducted in both the intervention and control programs after the completion of the curriculum for the academic year in June 2008.
Commitment to change
After each educational session at the intervention site, we gave participating residents and faculty members at the intervention site a simple “Commitment to Change” form. 27 “Commitment to Change” is an evaluation tool that has been mostly used in the realm of Continuing Medical Education. It has been shown that when physicians in practice identify and write down practice changes they would like to make during a Continuing Medical Education event, they are significantly more likely to use their new knowledge to change and improve patient care. The resident and faculty participants identified one new piece of knowledge that they had learned in each of the six activities and one new way that they would change their practice based on this new knowledge. They rated their intention to change practice on a 1 to 5 Likert scale. Between 3 to 6 months after their commitment to change was submitted, participants were contacted by e-mail and asked how successful they had been in implementing their self-selected change. They again rated their success in making that practice change using a 1 to 5 scale. Participants received and submitted a “Commitment to Change” form after each session that they attended.
Breastfeeding rates
We determined overall and exclusive breastfeeding rates for all of the newborns born in the Family Health Center in academic year 2008–2009 (post-intervention). The family medicine residents and faculty provided prenatal and newborn care. We calculated breastfeeding rates from individual chart review at hospital discharge, 2 weeks, 1 month, 2 months, 4 months, and 6 months, using data from the outpatient electronic health record. Of the 179 infants born into the health center patient panels during that year and seen there for their first newborn follow-up visit at 1–2 weeks, all but three were followed up in the health center after delivery for at least one further well-child visit. All infants with at least one well-child visit were included in the data analysis.
Data analysis
All data was entered into Excel (Microsoft, Redmond, WA). For the pretest and posttest evaluations, p values were calculated with analysis of variance. During the analysis of the pre- and posttests, the analyst was blinded to the identity of the participants and whether the test was a pre- or posttest. We analyzed the commitment to change data with descriptive statistics. Survival curves of breastfeeding duration were constructed by the Kaplan–Meier method, and p values were calculated for differences between groups with the χ2 test. Comparisons regarding the three main study outcomes (breastfeeding knowledge and attitudes/beliefs, practice changes, and patient panel breastfeeding rates) were made between participants who attended none to two educational sessions and three to six educational sessions.
Results
At the intervention site, breastfeeding knowledge and attitude/beliefs scores increased significantly after the curriculum was completed, even though there were varying levels of participation (Table 1). The residents and faculty at the intervention site attended a mean of 2.2 and median of two sessions (range, none to six). There was no difference in pre- and posttest knowledge or attitude/beliefs scores at the control site (Table 1).
There were 37 participants in the intervention group and 25 in the control group.
Breastfeeding knowledge, but not attitudes and beliefs, improved more in those who attended more educational sessions, in a within-site comparison at the intervention site (Table 2). These findings did not differ in a stratified analysis of faculty versus resident (data not shown).
Twenty-one participants attended none to two sessions, 12 attended three or more sessions, and four did not complete the posttest.
In the commitment to change analysis, 24 individuals identified 37 practice changes they planned to make after an educational session. The top five planned practice changes, which included over 95% of the planned changes, were increasing prenatal counseling to breastfeed, increasing other types of counseling and patient education, increasing referrals to community support services for breastfeeding, increasing referrals to hospital lactation services, and using the National Library of Medicine's online LactMed database for medication questions. 28 Level of commitment to make individual changes was high, with all respondents saying they would either “definitely make the change” or “have a high likelihood” of making the change. When followed up 3–6 months later, 21 of the 37 changes had either been implemented with complete or partial success. Of the seven changes that were not made, all participants cited that they had not seen an appropriate patient in the interim to make the change, usually because they had been on a series of rotations where they were not caring for pregnant women or breastfeeding dyads.
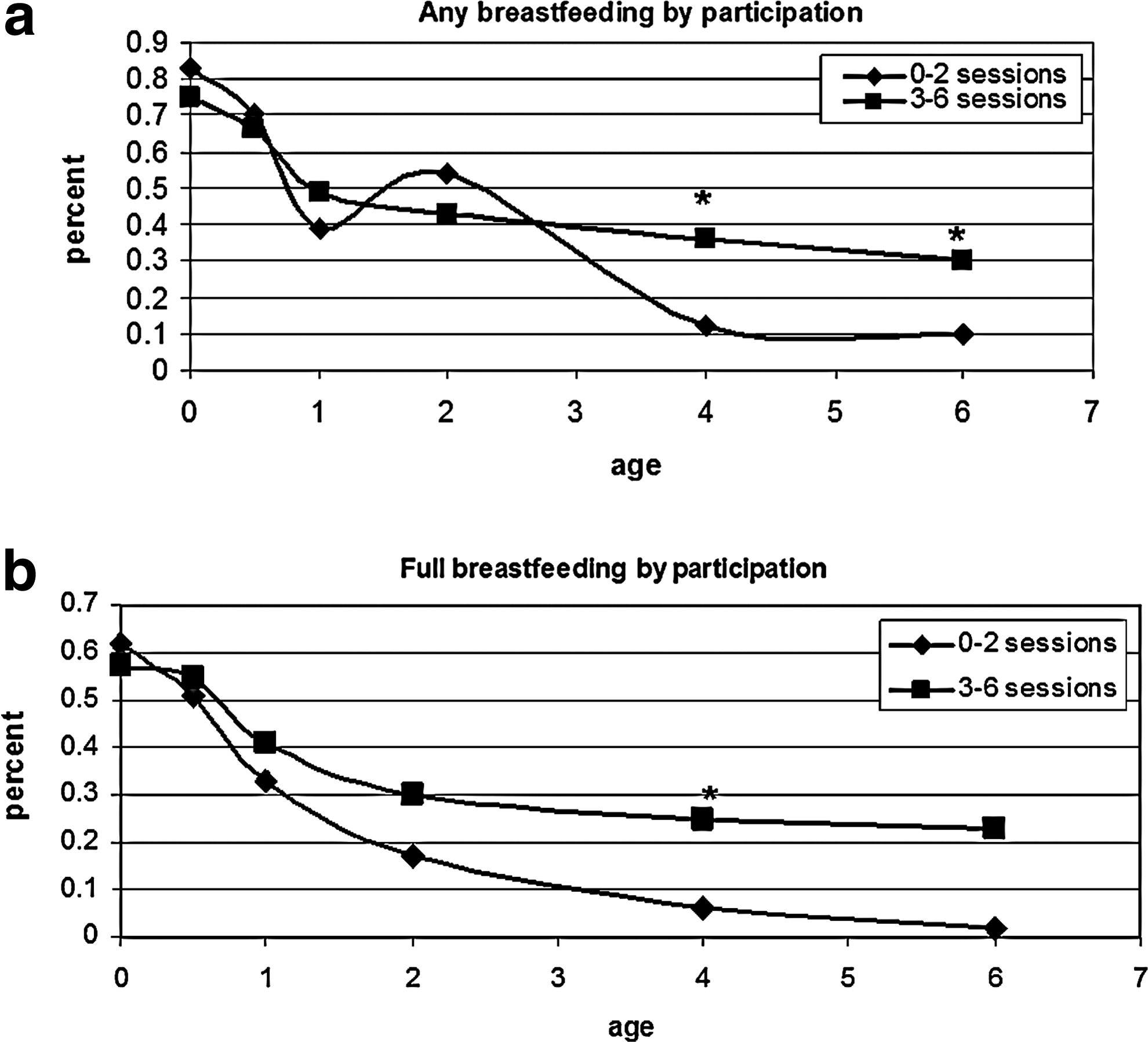
As our final measure of educational outcomes, we examined whether participation in the breastfeeding sessions improved clinical outcomes. Comparing physicians who attended none to two versus three to six sessions, we looked at breastfeeding rates of patients on provider patient panels 1 year after the end of the intervention. There was no difference between the two groups for rates of any breastfeeding at birth, 2 weeks, 1 month, or 2 months. However, at the later well-child visits (4 and 6 months), patients of physicians who had high levels of participation had rates of any breastfeeding of 36% at 4 months and 30% at 6 months, whereas patients of participants with low participation had rates of only 11% and 9% (p<0.001) (Fig. 1a). Likewise, rates of full breastfeeding revealed no differences at birth, 2 weeks, 1 month, or 2 months, but at 4 months, rates showed a difference of 26% versus 6% between the high and low participation groups (p<0.0001) (Fig. 1b). The difference at 6 months for full breastfeeding was 22% versus 5%, but this was not statistically significant (p=0.07).
Patients' breastfeeding rates after the intervention, comparing physician participants who attended none to two sessions versus those who attended three or more sessions:
Discussion
A breastfeeding curriculum covering basic medical breastfeeding content was able to improve resident and faculty physician knowledge, attitudes, and beliefs at a semirural family medicine residency program. In addition, physicians who participated in the curriculum were able to translate new breastfeeding knowledge into relevant practice changes to help their patients, as indicated by reported fulfillment of their self-identified goals. Most importantly, the patients of those physicians with the highest levels of participation in the curriculum had significantly higher rates of any breastfeeding at 4 and 6 months and of full breastfeeding at 4 months.
Prior studies have identified major gaps in physician knowledge of basic breastfeeding facts and skills,5–7 and others have demonstrated that physicians can improve breastfeeding knowledge by participating in formal breastfeeding curricula. Specifically, in family medicine, Haughwout et al. 20 demonstrated that after a half-day interactive workshop, family medicine residents were able to improve scores on Objective Structured Clinical examinations specific to common breastfeeding issues. Ogburn et al. 21 have published a description of an adaptation of the Wellstart Lactation Management Guide that included family medicine residents, but improvement in knowledge or practice patterns was not assessed. Two different projects in pediatrics have shown that structured curricula regarding breastfeeding improved pediatric resident knowledge and increase in good practices with patients; however, neither of these looked at important clinical outcomes such as breastfeeding duration or exclusivity.22,23
In this study, the demonstrated improvement in clinical outcomes was likely a result of the interactive workshop formats, case-based interactive sessions, and the feedback of continuity panel breastfeeding rates to participants, all of which created active and relevant learning opportunities. The use of the “Commitment to Change” in evaluation has also been shown to have a positive effect on stimulating changes in practice. 27 It is likely that those who were most successful at being able to incorporate the changes into their clinical practices saw better clinical outcomes in their patients.
There is often debate about if and how educational interventions can lead to practice changes and improved patient outcomes. The literature is replete with examples of curricula that improve knowledge and attitudes, without any effects seen on patient outcomes. These critiques tend to focus on didactic curricula only, with good evidence that certain formats, such as interactive workshops, and practice-based improvement activities, such as those used in the present study, can improve patient care and health outcomes. Recent studies have demonstrated that appropriately designed breastfeeding curricula can not only improve knowledge, attitudes, and practices, but also actually improve breastfeeding rates. Grossman et al. 24 implemented a multidisciplinary curriculum in the inpatient nursery setting of four hospitals with low breastfeeding rates and demonstrated an increase in breastfeeding initiation after a 12-hour program. Feldman-Winter et al. 25 recently published a large study of 417 pediatrics, obstetric-gynecology, and family medicine residents at six training sites who demonstrated gains in knowledge and confidence and improved practice patterns compared with controls at seven nonintervention sites. In addition, rates of exclusive breastfeeding at 6 months were significantly higher after the educational intervention for infants born at the intervention hospitals compared with the control hospitals. 25
It is noteworthy that the changes in clinical outcomes related to curriculum participation were seen at 4 and 6 months, but not at times closer to birth. We suggest that this finding reflects the more powerful influence of the hospital environment and policies on mothers' early rather than later breastfeeding. The hospital at the intervention site had a Baby-Friendly Hospital Initiative Certificate of Intent at the time of the study and has since been designated as Baby-Friendly, so good breastfeeding practices were emphasized in the perinatal period and likely improved breastfeeding practices for all neonates born at the study hospital. In prior studies about the effects of Baby-Friendly hospital policies, investigators have found improvements in rates of breastfeeding initiation and exclusivity in the hospital setting and out up to 6–8 weeks into the newborn period.29,30 Effects of the hospital setting may not be as significant when looking at outcomes at 4 and 6 months of life. There were no other significant public health efforts or other projects underway to improve breastfeeding at the hospitals and the health centers or in the wider communities at the time of the educational intervention.
Later on in infancy, however, a more powerful source of influence on breastfeeding is good clinical practices by primary care physicians and physician knowledge about dealing with breastfeeding problems. Hence our curriculum, which focused on the primary care clinicians, likely led to the better clinical outcomes at 4 and 6 months postpartum for participants who received the full curriculum.
There are several limitations in this study. First, this is a small study in one semirural residency program. The patient population was not racially or ethnically diverse and was uniformly economically disadvantaged. This is a population, however, that may be more challenging to move toward improved rates of breastfeeding than those in more affluent communities. Nonetheless, these factors may limit the generalizability of the study to dissimilar sites or patient populations. There could also be barriers to adapting this rather intensive breastfeeding curriculum to other residency training programs. Finally, collecting data on outcomes may be more challenging in other settings, particular those without electronic medical records.
Conclusions
This study demonstrates that a formal breastfeeding curriculum can improve physician knowledge and attitudes, change practices around breastfeeding care, and also improve clinical outcomes. The highly interactive educational intervention stimulated participants to identify practice changes that they were frequently able to implement in the months after the intervention. High levels of curriculum participation led to significant improvements in patients' breastfeeding duration and exclusivity for this disadvantaged population. This curricular approach could be adapted in other family medicine or primary care residency programs.
Footnotes
Acknowledgments
The authors are indebted to the Pediatric Academic Societies' Educational Scholars Program, which provided the stimulus for and oversight of the project as well as training in the educational methods and analysis tools used herein. In particular, we would like to thank Dr. Constance Baldwin and Dr. Judy Shaw for their guidance. We would also like to thank Dr. Gail Fayre, Family Medicine Residency Program Director, and Dr. Skip DeVito, Chairman of the Department of Pediatrics, for project support. Laura Greer, M.D., John Orzano, M.D., M.P.H., Tina Kenyon, ACSW, and Constance Baldwin, Ph.D., provided critical commentary on the manuscript.
Disclosure Statement
No competing financial interests exist.