
Abstract

Dear Editor:
C
A 27-year-old woman at 17 days postpartum visited the emergency department of Tsuyama Central Hospital (Okayama, Japan) and presented with several days' history of fever and tenderness, redness, and swelling of her left breast. She transvaginally delivered her first child at gestational week 40. She had uterine leiomyoma, and an episiotomy was performed at the time of delivery, but the delivery itself was free of any major trouble such as vaginal lacerations. Under the diagnosis of PPM, breast massage was performed by a maternity nurse several times, but high fever occurred, and the patient was admitted to the hospital. Laboratory examination upon admission revealed a highly inflammatory state (white blood cell count, 16,100/μL; C-reactive protein level, 16.6 mg/dL). Administration of ceftriaxone was initiated; however, methicillin-resistant S. aureus was identified from pus, and the antibiotic was switched to daptomycin (DAP). Although laboratory data improved, the inflammatory symptoms persisted, and ultrasonography revealed a low echoic area located in the upper part of the breast with a size of more than 5 cm. Under the diagnosis of breast abscess, a surgical incision was performed, and approximately 15 mL of purulent discharge was drained. Subsequently, her clinical symptoms resolved, and the patient was discharged on Day 10 with administration of oral clindamycin.
Later, bacterial analysis of the pathogen was performed. It showed that the isolate was CA-MRSA with the staphylococcal cassette chromosome mec (SCC mec) IVc element and that it carried toxic genes for Panton-valentine leukocidin and α-hemolysin but was negative for toxic shock syndrome toxin-1 and β- and γ-hemolysin (Fig. 1).
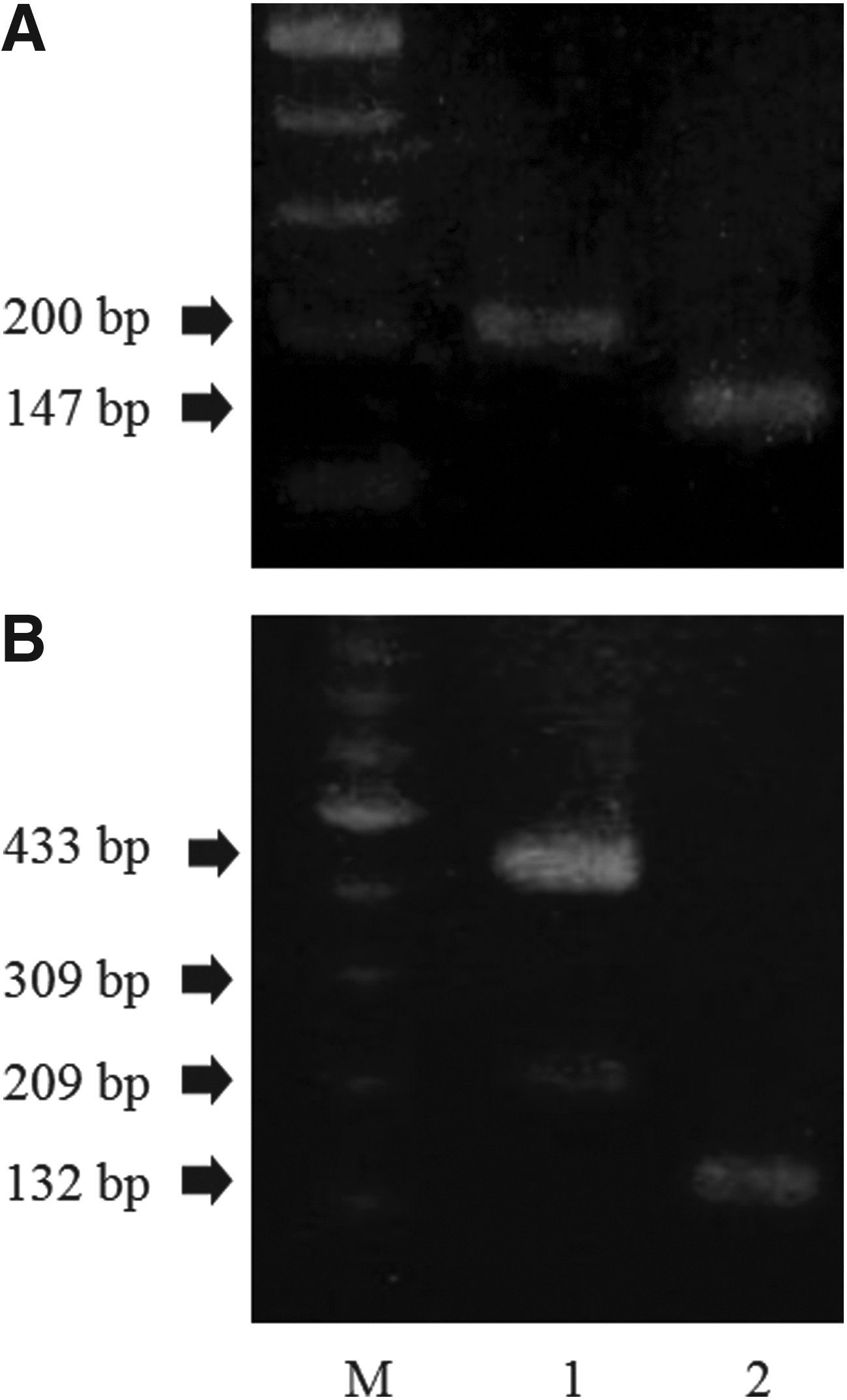
Detection of
Groups at risk for CA-MRSA infection include military personnel, prisoners, athletes, intravenous drug users, the homeless, urban populations, people in daycare facilities, and men who have sex with men. However, the incidence of CA-MRSA PPM in postpartum women without these traditional risk factors has been increasing. 3 Multiparous mothers with young children have been reported to be at increased risk for CA-MRSA PPM because the prevalence of CA-MRSA colonization is increasing among young children. 3 On the other hand, it is paradoxically reported that primiparous mothers are more commonly infected with CA-MRSA. Our patient was primiparous and had no notable history of frequent contact with children. As reported, the population at large has widely become the victim of CA-MRSA infection. We should be aware of the possible occurrence of CA-MRSA PPM in people without any particular risk factors.
For severe cases, intravenous vancomycin is a preferred option because it is secreted well into breastmilk, while little is absorbed when taken orally by the infant. Excretion of DAP into breastmilk is, in contrast, extremely low (estimated milk-to-plasma ratio of 0.0012), and efficacy against PPM therefore cannot be expected. 4 This pharmacokinetic property of DAP might have contributed to the ineffectiveness of treatment in the present case. Indeed, DAP is not recommended in current PPM treatment guidelines. 5 Considering its excellent pharmacokinetics for breastmilk, vancomycin might be a better choice, and its use might have prevented the need for surgical incision in the present case.
In summary, CA-MRSA is expected to become an increasingly common pathogen of PPM in Japan. Appropriate therapy for PPM caused by CA-MRSA should be initiated according to treatment guidelines, 5 especially in severe or refractory cases.