
Abstract
Abstract
Aim:
The aim of this study was to determine levels of montelukast in human milk and to develop a simple, sensitive analytical method using mass spectrometry.
Methods:
Milk samples were collected from seven breastfeeding mothers, age 26–35 years, at 0, 1, 2, 4, 8, and 12 hours after oral ingestion of 10 mg montelukast. The samples were analyzed using a new Liquid Chromatography–Tandem Mass Spectrometry method. Area under the milk concentration time curve from zero to the time of the last sample (12 hours) was estimated by the linear trapezoidal rule.
Results:
Average montelukast levels (Cavg) in milk were 5.3 ng/mL, and the relative infant dose was 0.68% of the maternal dose. The maximum concentration (Cmax) observed at 4 hours (Tmax) was 9.7 ng/mL.
Conclusion:
The exposure to the infant seems to be very low, far below therapeutic ranges in an infant. Our data suggest that montelukast is probably safe to use in a breastfeeding mother.
Introduction
M
Asthma is the most common condition affecting the lungs. It adversely affects 8% of all pregnancies 7 and presumably breastfeeding mothers as well. If untreated, the risk of preterm delivery, vaginal hemorrhage, and pregnancy-induced hypertension is increased.8–10 Montelukast sodium has the advantage of once daily dosing and oral administration. Its clinical efficacy for asthma and allergies is found to be advantageous during pregnancy. 11 Mothers suffering from these conditions commonly use this product during pregnancy. However, its transfer into human milk in breastfeeding women has never been evaluated. This present work describes a simple, selective, and sensitive method for quantification of montelukast in milk of seven breastfeeding mothers.
Materials and Methods
Subject selection
Subjects were recruited into the study through a website following discussion and consenting with the InfantRisk Center staff. Milk samples were collected from seven breastfeeding women, age 26 to 35 years, following an oral dose of 10 mg montelukast (Singulair) and frozen at −80°C for further analysis. These women had been on an extended regimen of a daily dose (10 mg) of montelukast and thus were at a steady state and were exclusively breastfeeding. Women who supplemented their infants with formula or were pregnant were excluded from the study. The Institutional Review Board of the Texas Tech University approved this study (A12-3717), and written informed consents were obtained from all the participants. Each woman was asked to record the time and dose of montelukast taken along with the time each milk sample was collected. They collected the milk samples at their respective homes, stored the sample upright in their freezer, and shipped them frozen, with cold packs. As the samples reached our facility, they were stored in −80°C till further analysis. Other information such as women's body weight and other medications consumed was reported. Infant details such as gestational age at birth and age at time of the study were also recorded. Because the differential lipid content in human milk plays a significant role in the transfer of medication into breast milk, samples were collected from the both the breasts, combined and mixed together as one. Samples were collected at zero time before taking the drug and then at 1, 2, 3, 4, 8, and 12 hours following the dose of montelukast.
Methodology
Samples were analyzed using liquid chromatography–mass spectrometry. Determination of montelukast levels in milk required the use of AB Sciex QTRAP 5500 UHPLC/MS/MS mass spectrometer. Quantitation was achieved in the positive ion mode for both analyte and Internal standard. Detection of the ions was performed in the multiple reaction monitoring mode, monitoring the transition of the m/z 586.2 precursor ion to m/z 422.3 product ion for montelukast and similarly for internal standard m/z 395.1 to m/z 213.1. Samples were processed on a Phenomenex Luna C-18 column, 50 × 2 mm with particle size 3 μm. The mobile phase consisting of 35% water: 65% acetonitrile both containing 0.1% formic acid was set at a flow rate of 0.6 mL/min. The volume of 8 μL was injected for a 3-minute run. The column was kept at 40°C and the auto sampler at 10°C. Rotenone was used as an internal standard and was added during the protein extraction phase. A simple protein precipitation method was followed for sample preparation from human milk. To an aliquot of 100 μL of human milk, 900 μL of acetonitrile (containing a working solution of rotenone internal standard of 50 ng/mL) was added, mixed for a minute followed by centrifugation at 20817 g for 5 minutes. The supernatant obtained was collected into an autosampler vial and injected onto the column. The recoveries of analyte and internal standard from human milk were determined by comparing the peak areas of the analyte in spiked human milk samples with those of analyte spiked into the postextracted milk blank by adding equivalent concentrations of the analyte. Percent recovery was calculated to be 85%.
Calibration curve samples were prepared by spiking human blank milk with the appropriate working solution of montelukast. The calibration curves were constructed using values ranging from 39 to 10,000 pg/mL (10 ng/mL) of montelukast in human milk samples. Quality controls (QCs) were prepared at 39 pg/mL (lower limit of quantitation), 78 pg/mL (low quality control), 625 pg/mL (medium quality control), and 2.5 ng/mL (high quality control). Calibration curve standard and QC samples were prepared for analysis and accuracy and precision for the back calculations of calibration standards.
Results
Demographic data of the participants are represented in the Table 1. The women had mean age of 31.5 (range 26–35) years and average body weight as 85.7 (range 70–114) kg. All the women had been on montelukast for months to years and five out of seven even took the drug during their pregnancies. The remaining two started after delivery. Thus, all subjects were at a steady state during sample collection in this study. The mean age of the infants at the time of the study was 4.3 (range 1.4–8.2) months. Mean gestational age was 39.2 (range 36.7–41.6) weeks. There were no drug–drug interactions with any of the other medications taken by the women. None of the mothers reported any adverse effects or any concerns in their fully breastfed infants.
Due to the low levels of montelukast in breast milk, extreme sensitivity and specificity were required in this assay to accurately measure the levels of montelukast in human milk samples. The representative graph for the milk calibration curve is shown in Figure 1, and the correlation coefficient observed was 0.997. Area under the milk (AUC) concentration time curve from zero to the time of the last sample was estimated by the linear trapezoidal rule. Figure 2 depicts the mean ± SEM concentrations of montelukast versus time. The average concentration of montelukast in milk (Cavg) was 5.3 ng/mL. The maximum concentration in milk (Cmax) observed was 9.7 ng/mL at 4 hours following the oral dose. The daily absolute infant dose was estimated as Cavg multiplied by an average milk intake of 150 mL/kg/day. Based on these data, the relative infant dose (RID) was calculated to be 0.68% and the absolute infant dose was calculated at 0.798 μg/kg/day. The area under curve, Cavg, Cmax, Tmax, and the RID for montelukast are summarized in Table 2.
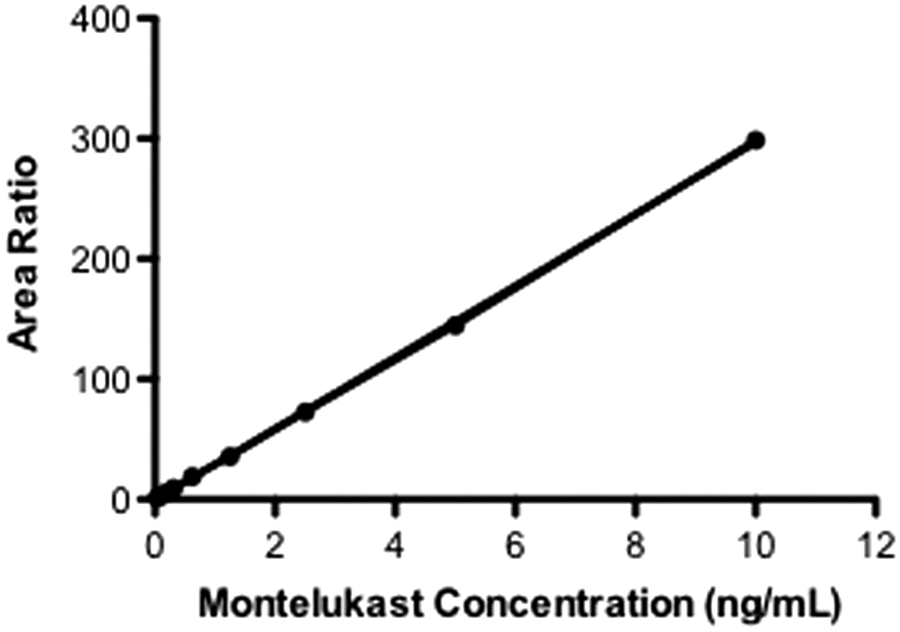
Montelukast calibration curves derived from human milk calibration standards (linear range 0.039–10 ng/mL).
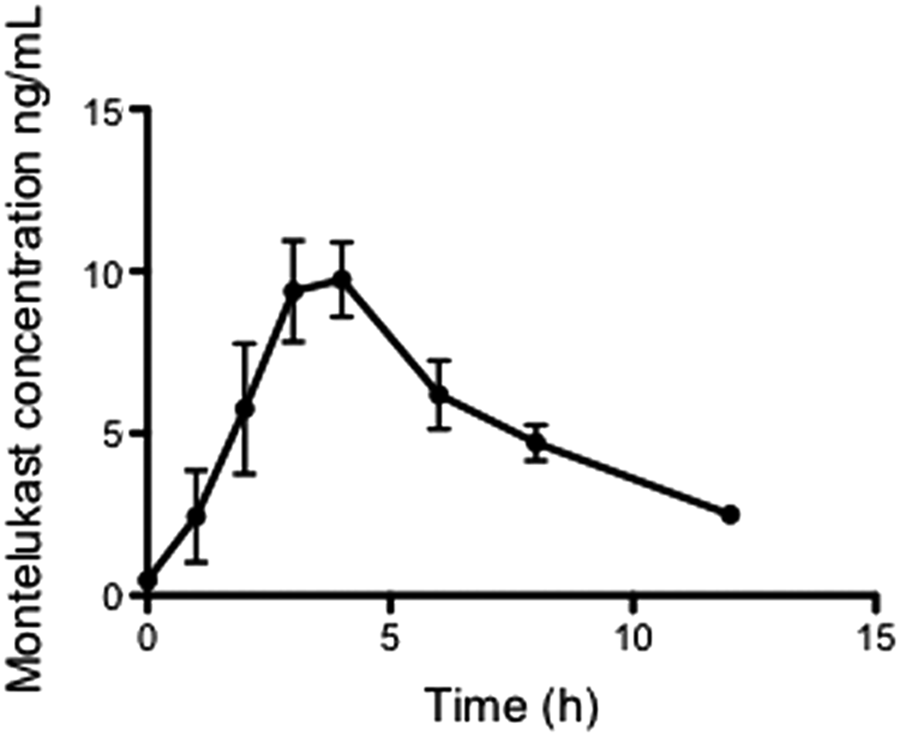
Mean milk concentration time profile of montelukast in human milk following the oral administration of montelukast 10 mg tablets to breastfeeding mothers (n = 7).
Area under the drug concentration time curve.
Average drug concentration across the dose interval.
Maximum drug concentration across the dose interval.
Time at which maximum concentration is observed.
Relative infant dose for montelukast in milk%.
Discussion
Human milk is the best form of nourishment for infants. It is a complex biological matrix, whose constituents vary daily as well as between individuals, so the detection of a drug is difficult. Montelukast has been analyzed by liquid chromatography-tandem mass spectrometry in a variety of other matrices such as urine 5 and plasma.12,13 To our knowledge, this is the first quantitative description of montelukast transfer into human milk. Our study, which included milk samples from seven mothers, reports the average drug concentration across a 12-hour dose interval (Cavg) to be 5.3 ng/mL and the estimated infant dose as 0.798 μg/kg/day. The RID value calculated was found to be well below 10%, thus suggesting the drug is probably safe during breastfeeding. The peak concentration (Cmax) occurred at 4 hours, which is similar to what has been found for the peak serum concentration in adults given a single dose of montelukast 10 mg. 14 The literature suggests the maximum concentrations of montelukast in plasma are found to be in the range of 300 to 500 ng/mL.13,15 In our study, it was found to be 9.7 ng/mL in the milk samples.
Several previous studies have only focused on testing for montelukast concentration in the blood plasma,13,16 but none have yet reported levels in human milk. Studies have been done to examine the therapeutic effects of montelukast in infants. When administered to premature infants (n = 11), suffering from bronchopulmonary dysplasia, at 1–2 mg/kg/day per body weight, montelukast proved clinically effective at this dose. The prior study suggests montelukast is completely safe even when used in preterm infants. 17
One weakness of this study is that we only collected samples over 12 hours of the 24-hour therapeutic interval. That said, the mean concentration detected in milk samples at 12 hours was exceedingly low (2.4 ng/mL) and the 24-hour samples would likely have been undetectable. Thus, our RID estimates would therefore be slightly lower if we had collected all 24 hours of samples.
The procedure used in this method was highly specific and exceedingly sensitive. Our method determined the lower limit of quantification to be 39 pg/mL, lower than any other reported methods for its detection in blood plasma.18,19 Finally the levels of montelukast detected in human milk samples were very low. These results suggest that it should be quite safe for the mothers to breastfeed their children while consuming montelukast at the 10 mg dose.
Conclusions
Levels of montelukast in human milk are exceedingly low. Mothers can be advised that it is safe to consume this product while breastfeeding. In addition, the described method uses a fast and easy sample preparation in an UHPLC-MS/MS system. The sensitivity of the assay will be useful for quantification of montelukast in breast milk from mothers maintained on montelukast after pregnancy.
Footnotes
Acknowledgments
The authors thank the core facility of the Texas Tech University for the usage of the AB Sciex QTRAP 5500 UHPLC/MS/MS equipment. They are also grateful to Dr. Raja Reddy Kallem for his scientific input. The authors would also like to thank the InfantRisk Center and Clinical Research Unit for their support in the collection of the milk samples.
Disclosure Statement
No competing financial interests exist.