
Abstract
Abstract
Purpose:
To determine bone mineral density (BMD) at the age of peak bone mass in women who previously experienced pregnancy and breastfeeding during adolescence.
Materials and Methods:
In this retrospective study, female volunteers aged 24–30 years who were pregnant during the age of 15–19 years and have had one to two babies were recruited. All of them experienced breastfeeding without history of bone- or calcium-related problems, such as fracture or low calcium intake. BMD was determined at the femur and L1–L4 spine by dual-energy X-ray absorptiometry.
Results:
We found that both volunteers who previously experienced breastfeeding and age-matched control volunteers had similar BMD at the L1–L4 spines and femora. Further analysis for site-specific changes of lumbar and femoral BMDs showed that the values of the breastfeeding group were not different from those of the control group except at L1 and L2, where BMD values were greater in breastfeeding group compared with the control group. At both femoral and vertebral sites, T- and Z-scores were apparently similar between the two groups. In addition, the BMD at peak bone mass had no significant correlation with breastfeeding duration.
Conclusions:
Teenage pregnancy and breastfeeding did not negatively affect BMD later at the age of peak bone mass. Therefore, breastfeeding can be encouraged in teenage mothers.
Introduction
P
Exclusive breastfeeding has been shown to induce site-specific deterioration of bone microstructure and density that can be restored to the prebreastfeeding level after weaning.10,11 However, long-term consequence of breastfeeding on the bone is debatable, particularly in pregnant teenagers whose bone development had not yet completed. This study, therefore, aimed to determine BMDs of various bone sites, that is, L1–L4 vertebrae and femora, at the age of peak bone mass in women who experienced pregnancy and breastfeeding during adolescent period. As young adolescent mammals are normally well responsive to calciotropic hormones, particularly 1,25-dihydroxyvitamin D3 [1,25(OH)2D3] and have high capacity of bone repair, 12 it is hypothesized that BMD of women who previously experienced pregnancy and breastfeeding is fully restored without signs of low peak bone mass.
Materials and Methods
Subjects
In this retrospective study, female volunteers (aged 24–30 years; breastfeeding group) who previously became pregnant and breastfed their one or two babies for at least 1 month during the age of 15–19 years with 1–2 years were recruited. Normally, the age at peak bone mass was 24–30 years (i.e., when several bone sites reached the highest mass). All subjects had no history of bone- or calcium-related disorders, for example, bone fracture, low calcium intake, and chronic steroid use. Their previous breastfeeding durations were recorded. BMD was determined at the femora and L1–L4 vertebrae by using dual-energy X-ray absorptiometry. The control group was age-matched healthy nulliparous female volunteers (aged 24–30 years; control group). A diagram for data collection in both groups is given in Figure 1. This study had been approved by the ethics committee of the Faculty of Medicine Siriraj Hospital, Mahidol University, Thailand [515/2556(EC2)]. Written informed consent was obtained from each volunteer before history taking and data collection.
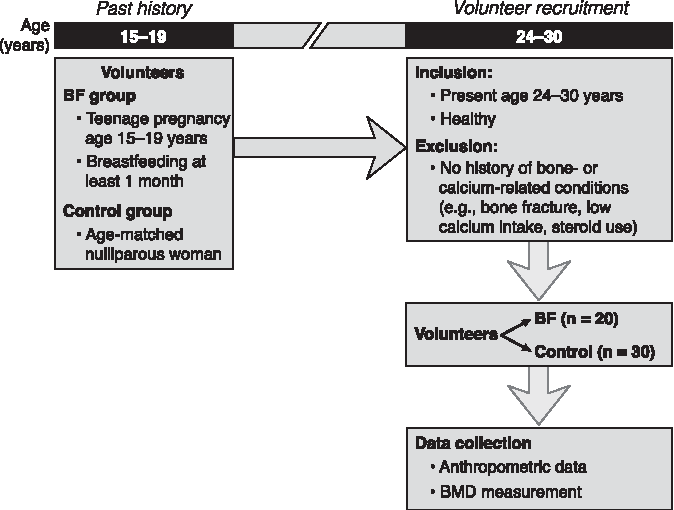
Diagram of the experimental design in this retrospective study. Volunteers who were pregnant during age 15–19 years and breastfed at least 1 month (BF group) were recruited. The control group included age-matched nulliparous female volunteers (control group).
BMD measurement
BMD values, T- and Z-scores (bone densitometer, Lunar Prodigy; DF +15974) of breastfeeding and control volunteers were obtained by experienced well-trained technicians at the Division of Endocrinology and Metabolism, Department of Medicine, Siriraj Hospital. 10
Data analysis
Results are expressed as mean ± standard error. Comparisons between the two sets of data were performed using unpaired Student's t test. The correlation between BMD at the age of peak bone mass and breastfeeding duration was assessed using Pearson's correlation coefficient. Results were considered significantly different when p < 0.05. All data were analyzed by GraphPad Prism 6.0 (GraphPad Software, Inc., San Diego, CA).
Results
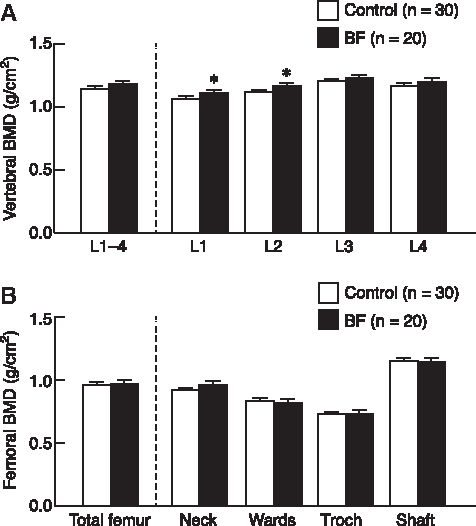
We found that age (26.89 ± 0.41 years versus 26.48 ± 0.43 years), height (156.10 ± 1.08 cm versus 155.10 ± 1.51 cm), and calcium intake (344.60 ± 29.7 mg Ca/day versus 328.90 ± 52.4 mg Ca/day) of control (n = 30) and breastfeeding (n = 20) groups were not statistically different. Both breastfeeding and control groups had similar BMDs at the L1–L4 spines (1.178 ± 0.028 g/cm2 versus 1.135 ± 0.028 g/cm2; p = 0.071). The total femoral BMD values of the breastfeeding and control groups were also comparable (0.966 ± 0.031 g/cm2 versus 0.946 ± 0.023 g/cm2; p = 0.270). Further analyses for site-specific BMD of L3 and L4 lumbar vertebrae and femora showed that the BMD values of breastfeeding group were not different from those of the control group. However, L1 and L2 vertebral BMDs in breastfeeding group were slightly but significantly greater than those of the control group (Fig. 2). In addition, the BMD values at the ages of peak bone mass had no significant correlation with the previous breastfeeding duration (Fig. 3).
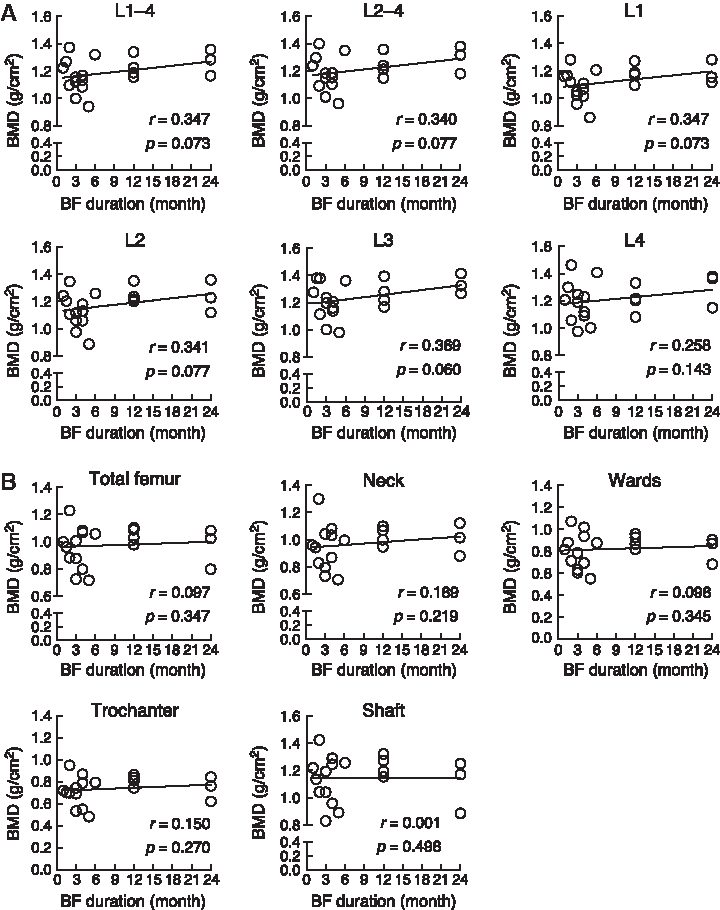
Correlations between BMD values at the ages of peak bone mass and the duration of breastfeeding (months) in the spines
According to the World Health Organization, T- and Z-scores (proxy indicators of osteopenia and osteoporosis) are the standard deviations of volunteers' BMDs compared with the standard BMD of reference means in young normal and age-matched normal groups, respectively. As given in Table 1, the T- and Z-scores were within the normal range despite a higher value in breastfeeding group compared with the control group.
T- and Z-scores (proxy indicators of osteopenia and osteoporosis) are the standard deviations of a volunteers' BMD as compared with the standard BMD of reference means in young normal and age-matched normal groups, respectively. Breastfeeding (n = 20), volunteers previously experienced exclusive breastfeeding during teenage; control (n = 30), age-matched nonpregnant nonlactating volunteers.
BMD, bone mineral density.
Discussion
Previously, studies in humans and rodents have suggested that breastfeeding and lactation are associated with osteopenia predominantly in trabecular sites, such as vertebrae and femurs, from the very first days of lactation until cessation of breastfeeding.10,13 Although the lactation-associated osteopenia is almost asymptomatic and reversible, a few individuals may experience bone pain, height loss, fragility fracture, and even nerve root compression, all of which are signs of a pathological condition known as pregnancy/lactation-induced osteoporosis (PLO). 14 Chronic low calcium intake, particularly during pregnancy, is one of the risk factors of PLO, 15 but the exact pathogenesis has never been elucidated. Furthermore, whether lactation contributes to the increase in the incidence of senile osteoporosis later in life remains controversial. Some investigations seem to support an increase in osteoporosis risk after menopause from previous long-term breastfeeding (e.g., breastfeeding period >1 year). 16 As the bone gradually accretes calcium and other essential minerals (e.g., phosphorus, magnesium, and zinc) during the adolescent period until bone mass reaches a peak at the age of ∼30 years, the dramatic disturbance of bone metabolism during this period—that is, teenage pregnancy and breastfeeding—might interfere with the attainment of peak bone mass, which is a known determinant of future osteoporosis. 17 Nevertheless, this hypothesis was very unlikely because we found in this study that pregnancy and breastfeeding at 15–19 years of age did not significantly affect BMD at ∼24–30 years of age, when the peak bone mass had been attained. Moreover, the absence of correlations between BMD and the breastfeeding duration also suggested that duration of breastfeeding beyond 6 months and up to 24 months did not negatively affect BMD at the ages of peak bone mass.
How lactation leads to bone loss is not completely understood. Most explanations point to hormones released for lactogenesis or during lactation, such as parathyroid hormone-related peptide (PTHrP) from the mammary gland and pituitary prolactin.18,19 Among these two endocrine factors, prolactin levels in the circulation exhibit a surge up to 300–400 ng/mL, which were >30 times greater than that in nulliparous women.20,21 A high amount of prolactin in this range was capable of stimulating osteoclast-mediated bone resorption and osteocytic osteolysis, presumably to liberate free-ionized calcium from the bone for milk production.13,22 In humans and rodents, exogenous prolactin administration or conditions with hyperprolactinemia (e.g., long-term treatment with D2-receptor-modulating antipsychotic drug) were associated with widespread osteopenia or osteoporosis that was evident throughout the body.23,24 Therefore, repetitive prolactin surge owing to suckling (or breast pumping) could contribute to the lactation-associated bone loss, and was perhaps one of the aggravating factors of PLO. 25
In this study, more or less normal bone mass in breastfeeding group suggested that transient bone loss during lactation did not produce a conspicuous long-term impact, at least on the peak bone mass. In other words, breastfeeding in teenage mothers did not pose an adverse consequence pertaining to BMD at the age of ∼30 years. Ardeshirpou et al. have reported that osteoclast underwent apoptosis after weaning, when osteoblast activity commenced to dominate over osteoclast activity. 26 Moreover, osteoblasts of young individuals have been known to be more responsive to anabolic hormones, including growth hormone, sex hormones (i.e., estrogen and testosterone), and 1,25(OH)2D3; therefore, bones continued to efficiently accrete minerals after weaning, and long-term defect was not detected. 27 Indeed, there was a slight but significant increase in L1–L2 vertebral BMD in breastfeeding group compared with the control group. The exact cause for this finding is unknown, but it might partly be the result of the anabolic effects of the aforementioned hormones. A study in rats with persistent endochondral bone growth—that is, bone development has not yet completed—suggested that pregnancy could induce bone gain, presumably because of pregnancy-associated anabolic hormones, for example, IGF-1. 28
Although our study provided evidence that encourages breastfeeding in teenage mothers, the study had some limitations, such as relatively small sample size and the absence of bone mechanical study or microstructural analysis. A retrospective design had also prevented analyses of baseline BMD and bone turnover markers during breastfeeding. In addition, further investigation is required to demonstrate the major determinants of peak bone mass in volunteers who have previously experienced breastfeeding, and to elucidate whether teenage breastfeeding is able to increase the risk of postmenopausal osteoporosis.
Conclusions
Our data support the conclusion that teenage pregnancy and breastfeeding does not compromise BMD at the age of peak bone mass. Therefore, breastfeeding should be encouraged in teenage mothers without hesitation.
Footnotes
Acknowledgments
The authors thank Prof. Nateetip Krishnamra for valuable comments and proofreading of the article. This study was supported by grants from the Cluster and Program Management Office (CPMO), National Science and Technology Development Agency (P–13–00100, to N. Charoenphandhu), Faculty of Science, Mahidol University (CIF Grant; to N. Charoenphandhu), the Thailand Research Fund (TRF) through the TRF Senior Research Scholar Grant (RTA6080007 to N. Charoenphandhu), and TRF International Research Network Program (IRN60W0001 to N. Charoenphandhu).
Disclosure Statement
No competing financial interests exist.