
Abstract
Introduction:
The percentage of working women with children under the age of 3 has nearly doubled since the 1970s, elevating the importance of understanding and improving workplace lactation support. This study aimed to examine employee perceptions of and experiences with workplace lactation support within a single health care system. We used a socioecological approach and included the views of a broad range of employees with and without lactation experience to capture diverse perspectives at multiple levels.
Materials and Methods:
Employees were recruited from an integrated health care system in the southeastern United States. Five focus groups were conducted during June to August 2017. Transcripts were analyzed using qualitative content analysis, with key themes organized at four levels of analysis: individual, interpersonal, departmental, and organizational.
Results:
Thirty-five clinical and nonclinical employees participated. Employees shared varied perspectives on workplace lactation support, which emphasized the: (1) importance of having a lactation policy, (2) critical role of leadership in setting the tone for workplace lactation, and (3) differential experience between clinical and non-clinical lactating employees.
Conclusion:
Employee experiences with lactation support in the health care setting are influenced by individual, interpersonal, departmental, and organizational factors that must be considered in the design of effective workplace lactation support programs. Policies and programs that align with organizational values and accommodate the needs of employees in varying roles are recommended. By using a socioecological perspective, this study identifies practical strategies for implementing, improving, and sustaining workplace lactation support across multiple levels of a large health care organization.
Introduction
The percentage of working women in the United States with children under the age of 3 has nearly doubled from 34% in 1975 to 61% in 2015, 1 elevating the importance of understanding and improving workplace lactation support. The American Academy of Pediatrics recommends exclusive breastfeeding for the first 6 months postpartum, and continued breastfeeding for at least 1 year. 2 While mothers initiate breastfeeding in 83.3% of infants, only 25.4% of infants remain exclusively breastfed at 6 months. 3
Postpartum return to work is known to impact breastfeeding outcomes,4–6 particularly for mothers working full time.7,8 Returning to work reduces the frequency and duration of mother–infant contact as well as the convenience and comfort of breastfeeding and milk expression. A longitudinal study of employed U.S. women found that 69.4% initiated breastfeeding and that women who took longer periods of maternity leave had higher breastfeeding initiation rates than those who took shorter periods. 8 Women who had not yet returned to work by 9 months represented the highest proportion of mothers continuing to breastfeed beyond 6 months (46.7%), whereas women who returned to work within 7–12 weeks were the lowest proportion to breastfeed past 6 months (30.1%). The lack of a supportive work environment for lactation increases mothers' risk of not meeting personal breastfeeding goals and contributes to experiences of psychosocial distress. 9 This issue has particular salience in health care settings, where women comprise nearly 80% of employees 10 and occupy >90% of the clinical roles (e.g., nurses and medical assistants). 11
Research on workplace lactation support in health care settings has predominantly focused on the population of breastfeeding residents and physicians.12–17 Limited studies have included: (1) the perspectives and experiences of other clinical roles such as nurses 9 and health system employees in nonclinical roles; (2) male employees; and (3) female employees without lactation experience. Furthermore, few studies on lactation support in health care settings have been theoretically informed or guided by a theoretical framework. Research guided by theory is useful for examining, understanding, and specifying the relationship among variables within a particular context.
Grounded in Ecological Systems Theory, 18 the social ecological model (SEM; also referred to as socioecological model) is a framework for examining the intersection between the experiences of individuals and multiple layers of their social system and environment. 19 The SEM is widely used in research to understand the complexity of factors that influence health-related experiences, including breastfeeding.20–25 Bronfenbrenner's original ecological framework comprised five nested layers (individual, microsystem, mesosystem, exosystem, and macrosystem). 26 The framework has subsequently been adapted to varying ecological contexts. For example, in breastfeeding research, Munn et al., 20 examined the impact of the Baby Friendly Hospital Initiative on early infant health and breastfeeding outcomes through four SEM factors (intrapersonal/individual, interpersonal, organizational, and policy). In a qualitative breastfeeding study, Dunn et al. 21 assessed barriers and positive contributors to breastfeeding among field-based professionals across five SEM levels (individual, interpersonal, community, organizational, and public policy). Three studies have examined workplace lactation support through a socioecological lens involving three SEM levels (microsystem, mesosystem, and exosystem).22–24 Two were based in Pakistan,23,24 and the third study was a systematic review of barriers and facilitators to breastfeeding among U.S. working women. 25
In this article, we apply the socioecological framework to the context of a health care setting in the United States. The aim of our research was to examine employee perceptions of and experiences with workplace lactation support across multiple levels (individual, interpersonal, departmental, and organizational) of a health care system. Examining workplace lactation experiences through an ecological lens offers a multilevel understanding of associated challenges and opportunities. While breastfeeding is a personal decision, the act of milk expression in the workplace can be conceptualized as a social affair because of perceived and actual influences of workplace settings and relationships on lactation behavior and outcomes.21,24,25,27 Thus, we included the views of a broad range of employees with and without direct lactation experience to capture diverse perspectives on the issue.
Materials and Methods
Design
This qualitative study involved five focus groups, which were conducted between June and August 2017. Each focus group lasted ∼75 minutes. Focus groups were moderated by one member of the research team (V.C.S.) using a semistructured interview guide (Table 1). Focus group questions were informed by existing breastfeeding research and generated by the study co-Principal Investigators (V.C.S. and Y.J.T.), both of whom had recent experience as women working in health care settings while breastfeeding. The questions anchored around perceptions of and experiences with workplace lactation support, and included suggestions for improving workplace lactation support. Prompts and clarifying questions were posed per participant responses. Each participant received an information leaflet that outlined the study purpose, risks, and benefits, and was offered lunch and a $25 gift card. This study was reviewed by the Chesapeake Institutional Review Board and classified as exempt.
Guiding Focus Group Questions
Setting
This study was conducted within a large health care system in the southeastern United States that includes several hospital facilities, doctor's offices, and corporate offices across three states. The health care system had ∼60,000 employees during the time of data collection. Focus groups took place in the metropolitan region, where the health care system is headquartered. At the time of this study, the health care system did not have a corporate policy regarding support for breastfeeding employees.
Sample
As part of a larger study, employees were recruited by e-mail, intranet postings, and in-person at two hospital locations to complete an online questionnaire assessing employee perspectives and experiences with workplace lactation support. 27 Employees were eligible to participate in the larger study if they were ≥18 years of age, employed within the health care system for ≥6 months, and able to read and comprehend English. Employees who completed the online questionnaire and provided their contact information (n = 325) were invited to participate in a focus group. Invitations were sent out in the order in which employees signed up until a target of 6–10 participants was achieved.
Data collection and analysis
Participants were verbally consented at the beginning of each focus group. Focus groups were audiorecorded and transcribed by a doctoral student with formal training in qualitative research. Participant names were removed from transcriptions to maintain confidentiality. In addition, the anonymity of employee responses was protected by excluding personal identifiers (age, race, ethnicity) from data collection. Transcripts were imported into NVivo 11, and data were analyzed using a contextualist method of qualitative content analysis. A content analysis involves the systematic classification of text data into categories that represent similar meanings. 28 The contextualist method focuses on the characteristics of the language and the contextual meaning of the text to formulate codes and identify themes. 29 First, two research team members independently reviewed the transcripts to identify themes. Then, data codes were reviewed in pairs with discrepant codes initially reconciled at the dyad level. Data codes that could not be reconciled at a dyad level were presented to the larger research team for consensus coding. Informed by the socioecological approach, themes were mapped to four ecological levels (individual, interpersonal, departmental, and organizational), using definitions based on prior research on workplace lactation support.24,25,27 The individual level included personal attitudes, beliefs, and experiences. The interpersonal level focused on relationships among coworkers. The department level focused on the immediate workplace environment (structure and function of the unit) and department-specific policies, whereas the organizational level focused on system-wide culture and policies. Intercoder agreement had a Cohen alpha coefficient of 0.84.
Results
A total of 35 employees participated in the focus groups. Participants occupied various clinical (e.g., nurses, therapists) and nonclinical roles (administrative, operations, management, accounting, and facilities management/maintenance). Approximately 50% (n = 17) had breastfeeding experience while working within the health care system. Approximately 25% (n = 8) of participants were in leadership (executive, manager, supervisorial) roles, and 17% (n = 6) were males. A summary of themes within each ecological level are presented in Figure 1, with sample quotes available in Table 2.
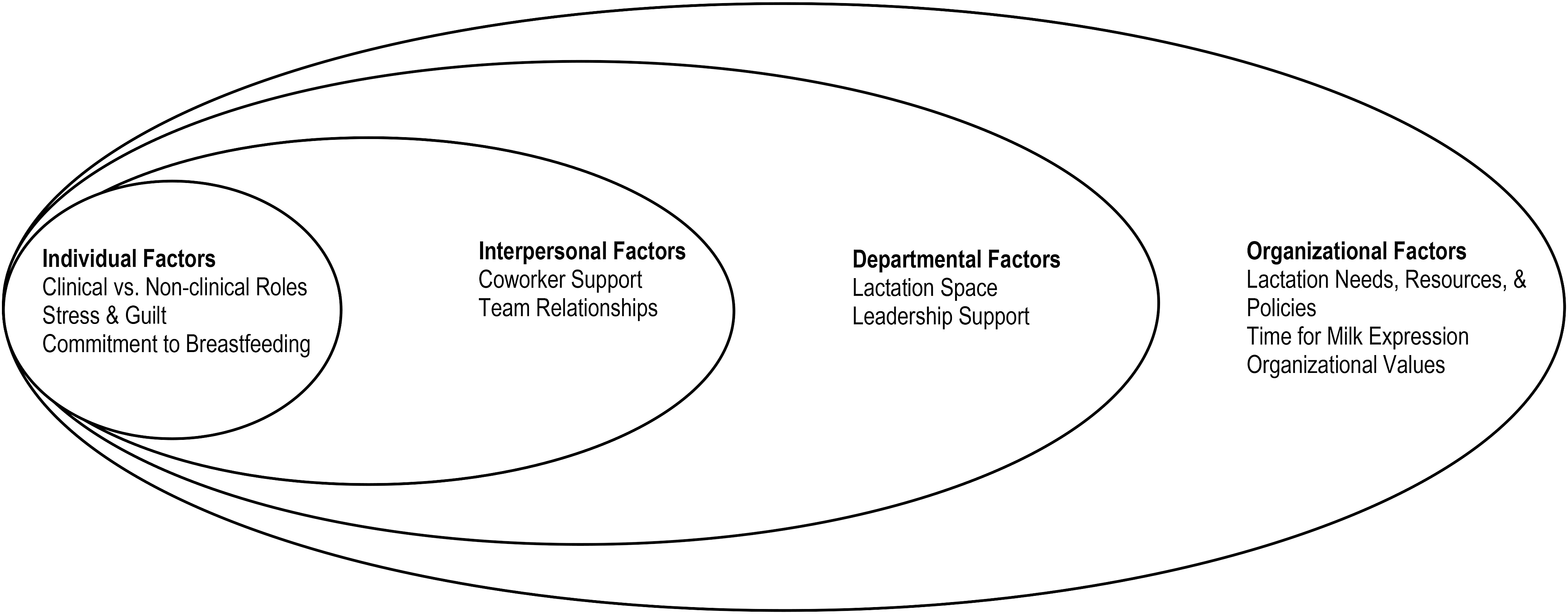
Factors relevant to workplace lactation support in the health care setting from a socioecological perspective. The four ecological levels depicted are an adaptation of the socioecological model developed by Urie Bronfenbrenner.
Themes and Sample Quotes
Individual level
The following themes emerged at the individual level: differing experiences between clinical and nonclinical roles, feelings of stress and guilt, and commitment to breastfeeding success.
Differences in experience between clinical and nonclinical roles
Focus group discussions revealed distinctions in the challenges faced by employees in clinical and nonclinical roles. While finding a private space to pump was the main challenge reported by nonclinical employees, the primary challenge for clinical employees was finding time to pump. The demands of patient care made it difficult for clinical employees to maintain a consistent schedule for milk expression. These employees shared feeling significant distress associated with negotiating between the need to pump and the needs of patient care. Clinical employees suggested instituting a “buddy” system to improve teammate support. This could reduce the individual burden of identifying coverage often placed on lactating employees.
Stress and guilt associated with workplace milk expression
Employees with lactation experience commonly used words like “stressful” and “hectic” to describe their experience expressing milk at work. Maintaining breastfeeding upon returning to work was anxiety provoking for women, particularly with regard to balancing work demands with pumping. Lactating women were often apprehensive about discussing personal lactation needs in the workplace. They worried that such conversation would result in the perception that they were less productive employees. Lactating employees also expressed distress associated with the dual role of being a “good employee” and a “good mother.” When women fell short of their personal breastfeeding goals, they perceived it as a “failure,” felt guilty, and often internalized the experience.
Commitment to breastfeeding success
Despite the myriad challenges employees experienced with workplace milk expression, employees were creative with generating solutions to sustain breastfeeding. Employees with lactation experience described developing a lactation schedule for their department in response to private space limitations, taking a laptop into the lactation room to maximize productivity, and posting self-affirmations to remain positive during the challenge of workplace milk expression. Personal commitment to breastfeeding success facilitated individual breastfeeding goals. Employees suggested proactive, early planning (i.e., talking with their supervisors about lactation needs before maternity leave and immediately upon returning to work) as a strategy for improving workplace lactation experiences. Individuals in leadership roles noted that, while successful workplace lactation is a team-based responsibility, it was helpful to have employees initiate the conversation—explaining that oftentimes they were unsure about when and how best to hold conversations about lactation accommodations.
Interpersonal level
Two themes emerged at the interpersonal level: variability in coworker support and quality of work team relationships.
Variability in coworker support
Coworker support for workplace lactation was a barrier for some lactating employees and a facilitator for others. Some lactating employees expressed anxiety about asking and receiving coworker support; a common concern of lactating employees was that other employees would not understand the importance of milk expression and why they needed to take multiple breaks during the workday to do so. This concern was illustrated during a focus group session when an employee with no lactation experience curiously inquired about the process and time required to express milk. After listening to the experiences of lactating employees, the participant expressed: “… I never thought that it would take that long. So if I noticed someone was away that long, I might think they're taking their time and not really hurrying back and not realizing it takes that long.” The same employee also expressed concern about the impact of lactation accommodations on his work: “… it's tough because … I'm very supportive of it, but at the same time, I wouldn't want my work being impacted by it.” This concern was also expressed by other participants without lactation experience.
While some lactating employees experienced challenges with coworker support, other participants reported positive experiences. Employees with previous direct lactation experience were identified as particularly supportive coworkers. Lactating employees shared instances when coworkers “showed [them] the ropes” to sustaining workplace lactation, shared their office space as a private place to pump, and offered advice on juggling the demands of work with milk expression. Both participants with and without lactation experience expressed value in simply being able to talk openly with other coworkers about workplace lactation, noting the topic was not commonly discussed among employees. Video-based educational content on how to support a lactating employee was suggested as a strategy for improving coworker support.
Quality of team-based relationships
Team-based relationships, particularly trust among coworkers, impacted how comfortable lactating employees felt taking breaks to express milk. The quality of team-based relationships was described as more salient when teams were predominantly male. A positive team-based culture and strong foundation of trust among male-dominant teams helped lactating employees feel greater ease with workplace lactation. In this way, positive team relationships were a facilitator for lactating employees.
Departmental level
Two themes emerged at the departmental level: lactation space and the critical role of leadership support.
Availability, access, and quality of lactation space
While the hospital system has several lactation rooms across its facilities, some participants indicated that there were not enough lactation rooms to accommodate the number of lactating employees within their department. Employees shared experiences of not being able to find a time slot on lactation room schedules and not being able to readily identify an alternative pumping time when they missed a scheduled time for work-related reasons. Limited availability and poor access to lactation space was identified by employees as a barrier to workplace lactation. When lactation rooms were not available, women pumped in cars, bathrooms, closets, exam rooms, and vacant offices.
Participants also reported variability in how lactation rooms were equipped. For example, some rooms included an electronic pump, sink, and refrigerator while others included only a chair and an outlet. This created uncertainty for lactating employees who had to travel between different work locations. Women noted the following attributes for an ideal lactation space: occupancy signage; lockable door; nonreclining, wipeable chair; outlet; sink; and a refrigerator for milk storage. Several women also suggested equipping rooms with a computer for employees who desire to work while pumping.
Critical role of proximal leadership support
The importance of supervisors and managers in setting the tone for the departmental support for workplace milk expression was a recurring, strongly emphasized theme among all participants. Participants explained that department leadership shapes the culture and norms of the unit. Some participants took it upon themselves as department leaders to support employees with lactation needs. For example, a former department chair described setting up a private lactation space by first scanning the floor plan of her department to identify unused space and then asking teammates to donate furniture for the lactation space.
Lactating employees reported that whether or not they felt supported by their manager directly influenced how comfortable they felt when taking the time to express milk. Participants suggested that it would be helpful to provide all managers and supervisor education regarding how to effectively discuss workplace lactation support with lactating and nonlactating employees and facts about breastfeeding and workplace lactation.
Organizational level
Organizational level themes included: awareness of lactation needs, resources, and policy; time for milk expression; and aligning employee experiences with organizational values.
Awareness of lactation needs, resources, and policy
Employees without lactation experience expressed having limited knowledge about workplace lactation, including requirements and associated benefits of milk expression. Employees with lactation experience indicated a lack of clarity on how to access lactation resources (e.g., lactation room key, breast pump, health care system lactation room map), which made it difficult for employees to express milk when they travel between facilities. Participants recommended more frequent mass communication (e.g., newsletters, emails) from the health care system to improve communication and increase knowledge about lactation needs and supports.
Although there was not an organizational policy regarding workplace lactation support, a few participants reported that their department had a policy in place to support milk expression in the workplace. Developing a system-wide policy was the most frequent suggestion participants gave for improving workplace lactation support. An organizational-level policy was described as critical for clarifying lactation norms and expectations. Participants noted that the development of a lactation policy should include guidelines for implementation, explaining that having a policy was “necessary, but not sufficient.”
Time for milk expression
Employees described struggles with finding time to successfully express milk at work (i.e., travel to the provided lactation space, set up their equipment, pump and clean up). Employees reported using meal breaks and 15-minute respite breaks to express milk. The stress of the finding time to pump was noted to adversely interfere with milk supply. Participants recommended having an organizational policy that addresses break time needs for breastfeeding employees while acknowledging that the amount of time needed to pump varies from one person to another.
Aligning employee experience with organizational values
Employees felt that providing more comprehensive lactation support for employees would align with organizational values and with the care provided for patients. While lactation rooms were available in many facilities, employees expressed a desire for additional supports such as access to commercial-grade lactation equipment and access to lactation consultants as well as a culture that supports employees in attaining their breastfeeding goals. Participants explained that the health system provided patients with a robust program of breastfeeding supports, however, these same resources were not widely available to employees. This left some lactating employees feeling unvalued. Despite challenges with lactation support, participants noted that the organization has made visible advances, specifically citing observed increases in both the number and quality of lactation rooms.
Discussion
We adapted the socioecological framework to analyze issues of workplace lactation support in a large integrated health care system at four levels: individual, interpersonal, departmental, and organizational. Previous studies examining workplace lactation support in the context of a health care system have primarily focused on physicians and residents, and have been atheoretical. This study uniquely contributes to breastfeeding research by framing workplace lactation issues in a theoretical model, and including the perspective of employees with and without direct lactation experience from a broad range of health system roles. The inclusion of employees with and without lactation experience and in varying organizational roles within a single setting created a unique opportunity for (1) identifying gaps in understanding of workplace lactation, (2) illuminating areas of agreement between lactating and nonlactating employees, and (3) gaining a broader view of workplace culture regarding breastfeeding, including strategies for improving workplace lactation support.
At the individual level, lactating employees experienced both stress and success with juggling milk expression and occupational responsibilities. Employees with lactation experience suggested proactive early (antenatal) lactation planning involving conversations with supervisors and coworkers. Employees in clinical roles primarily experienced challenges with finding time to pump, while nonclinical employees primarily experienced barriers with having a private space. The relationship between occupational role and workplace lactation experience has been noted in other studies.6,30 While many studies have examined workplace lactation experiences in health care settings,31–34 few have focused on the specific experiences of nurses whose responsibilities for patient care can interfere with the length and frequency of breaks needed to maintain an adequate milk supply.9,35 Addressing this need is an important consideration for health care organizations and a target of existing breastfeeding initiatives. 36
At the interpersonal level, we found that coworkers can be a valuable source of support for lactating employees, particularly those with previous lactation experience. The focus groups illuminated varying ways in which coworkers provide support. For example, a coworker may be emotionally supportive of a lactating employee but reticent to provide instrumental support (e.g., cover an extra shift)—especially when doing so adds to one's own workload. An implication for research is that coworker lactation support may better be conceptualized as a multidimensional construct. Research on workplace lactation has largely examined coworker support as a unidimensional construct.32,37,38 Suggestions for improving coworker support include the development of virtual and in-person structures for peer mentorship, as well as coordination of schedules with peers for clinical rotations.15,17 An example of peer support model is Dr. MILK (Mothers Interested in Lactation Knowledge), 15 which offers physician mothers a social support group for addressing work-based lactation issues along with other motherhood and childrearing issues. During the focus group, participants suggested a similar strategy—specifically, the development of a health system intranet social media group to facilitate lactation support among coworkers.
Consistent with existing research in health care settings,9,30 lactating employees experienced variability in availability of, access to, and quality of lactation space within their departments. Participants discussed the practical value of the system-wide lactation room map, particularly for employees whose roles require traveling between multiple facilities. To maximize the value of the lactation room map, participants indicated the map should be electronically accessible, regularly updated, indicate lactation equipment available in each room, and be linked to a space reservation function. Similar maps developed by Michigan State University * and California Polytechnic State University † are a core component of lactation support programs in organizations with multiple facilities or campuses. Employers should ensure that all lactation rooms have basic accommodations (lockable door, electrical outlet, table, comfortable chair, and sink) and may expand to accommodate additional employee preferences. 11
The study findings regarding the critical role of leaders (managers, directors, and supervisors) in setting the tone for workplace lactation support confirm prior research in health care and other settings.27,39–42 Managers are involved in frontline implementation of organizational policies and can help to ease individual concerns about stigma and guilt by sharing resources and education about lactation support with employees and supporting needs for flexible schedules. In clinical settings, managers may need additional staff or other resources to accommodate their breastfeeding employees while maintaining high-quality patient care. Managers can also support the needs of lactating employees by eliciting scheduling support from administrative staff. 17 Developing strategies to educate and equip managers about workplace lactation needs, and allowing feedback to identify and address individual challenges with meeting those needs may help.
Lastly, at the organizational level, this study surfaced the importance of a corporate lactation policy. Similar to other health care settings (e.g., Hojnacki et al. 37 reported <3% have a written policy), the target health care system did not have a corporate lactation policy. We found that the absence of a lactation policy adversely affected work-based lactation experiences in several ways: it contributed to confusion about workplace lactation norms and expectations; it resulted in differential employee access to lactation breaks; and it left lactating employees poorly informed about their lactation rights. Employees indicated that the development of a corporate lactation policy should be supported with specific guidance for implementation through education for leaders, coworkers, and lactating employees. An emphasis on skills for discussing lactation needs is recommended. 41
Current U.S. policies provide a favorable environment for further improvements in workplace lactation support. In addition to the 2010 Patient Protection and Affordable Care Act, which mandated that employers provide adequate break time and a private space for lactating employees, several states have established policies to provide lactation support at work. Family-friendly, mother-friendly, and similar certifications provide additional incentives for employers to develop comprehensive workplace lactation support programs. For health care organizations seeking baby-friendly designations, providing lactation support for their employees should be an organic extension of the services provided for patients. The findings of this study highlight the importance of utilizing a combination of lactation support strategies that engage multiple levels of the organization to achieve this goal. These strategies include but are not limited to a system-wide lactation policy, accessible and clear communication about workplace lactation policies and resources, active leadership support, peer mentoring structures, and adequate technical supports (e.g., lactation space, pumping equipment, and refrigerator for milk storage). A recent systematic review of workplace lactation supports reported that comprehensive lactation programs (defined as a combination of three or more support types) were associated with significantly higher rates of breastfeeding initiation, significantly lower rates of breastfeeding discontinuation upon returning to work, longer duration of breastfeeding, and higher rates of exclusive breastfeeding at 6 months. 43
The study findings also speak to the interplay of issues and experiences across ecological levels. For example, manager/leadership perspectives (department level) can impact the willingness of coworkers to cover for a lactating employee while she expresses milk (interpersonal level) as well as the beliefs a lactating employee bears about workplace milk expression (individual level). Similarly, system-wide policies and resources for workplace lactation (organizational level) shape the availability and quality of lactation rooms across department facilities (department level). While study participants largely described the impact of the context on their perceptions of and experiences with workplace lactation support, some also described individual efforts to shape the environment; for example, the aforementioned instance where a department leader took it upon herself to construct a lactation space.
We note some limitations along with the study findings: First, while appropriate for qualitative research, our study sample included only 35 employees. These employees may not be representative of all health system employees. Furthermore, participants were employed within a single health care system located in the southeastern U.S. and may not represent the experiences of health care employees in other geographic regions. However, consistencies in themes and experiences between our study findings and studies with employees from other geographic areas and industries suggest that employee experiences may be more similar than different across settings. 37 Additionally, this study is subject to the possibility of sample bias. Participants were recruited based on expressed interest in participating in a focus group on workplace lactation support. This sample may hold a more positive valence toward workplace lactation and be more invested in the issue than other nonparticipating health system employees.
Conclusion
Health care systems are complex, role-diverse settings. By using a socioecological perspective, this study identified practical strategies for implementing, improving, and sustaining workplace lactation support across multiple levels of a health care system. Findings suggest a need for a comprehensive systems-based approach to workplace lactation that (1) aligns with organizational values and is supported by organizational policies; (2) accounts for the needs of lactating and nonlactating employees in clinical and nonclinical positions, and (3) invites candid conversations about the complexity, challenges, and benefits of lactation support. Policies and programs that align with organizational values and accommodate the needs of employees in varying roles are recommended.
Footnotes
Acknowledgments
The study was made possible by the Carolinas Healthcare Employee Breastfeeding Study team and health care system leadership: Katherine Buehler, Crystal Danielle Connor, Cecily Basquin, Johnnie Jones, and Brandi Newman. We appreciate the helpful feedback of Dr. Traci Yates on an earlier draft of this manuscript. In this article, we applied the “first-last-author-emphasis” (FLAE) norm for sequence of authors.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the University of North Carolina at Charlotte Faculty Research Grant and the Center for Outcomes Research and Evaluation at Atrium Health.