
Abstract
Background:
Disparities in breastfeeding patterns by race and ethnicity in the United States have been documented, and Latinx ethnicity is often associated with higher rates of breastfeeding initiation and longer breastfeeding duration compared to other U.S. racial and ethnic groups. Despite marked differences in infant feeding practices in Latinx countries of origin, U.S. breastfeeding data are routinely presented with Latinx as a single category.
Objective:
To analyze breastfeeding duration of New York City Latinx mothers by birth region.
Methods:
Using data from the 2016 New York City Work and Family Leave Survey (WAFLS) surveying residents who gave birth in 2014, we conducted a survival analysis of breastfeeding duration in a sample of Latinx-identifying mothers (n = 271), who reported having ever breastfed their child. Kaplan-Meier survival curves for time to breastfeeding cessation were created for four birth regions (United States, Caribbean, Mexico/Central America, and South America) and compared using the log-rank test. Adjusted hazard ratios (AHRs) were calculated using Cox regression.
Results:
Survival curves and median breastfeeding duration were significantly different between the four regions. AHR models found that non-Caribbean birthplace was significantly associated with a lower risk of early breastfeeding cessation. Being partnered at the time of childbirth and neonate hospitalization of 6 days or longer was associated with a greater risk of earlier breastfeeding cessation.
Conclusion:
The significant differences reinforce the need to separate breastfeeding findings by birth region in the Latinx population. Within-group differences are lost in combined analyses and reinforce conclusions that Latinx mothers have optimal breastfeeding behaviors.
Introduction
Breastfeeding is the recommended method of feeding by the World Health Organization 1 and American Academy of Pediatrics 2 for its association with improved health outcomes for both mothers and their breastfed infants. 3 Improving breastfeeding behaviors is a national policy goal for the United States, as evidenced by two Healthy People 2030 objectives seeking to improve breastfeeding rates at 1 year and exclusive breastfeeding rates at 6 months. 4
Multiple demographic factors and other social determinants of health have been shown to influence breastfeeding behaviors. Mothers who are young, non-Hispanic Black/African American, low income, unmarried, less educated, overweight or obese before pregnancy, or participating in nutrition benefits programs such as the Supplemental Nutrition Assistance Program (SNAP), or women, infants, and children (WIC) tend to have lower rates of breastfeeding.5–8
Disparities in breastfeeding patterns by race and ethnicity in the United States have been documented with mixed results for the Latinx population. In many studies, Latinx ethnicity is considered a protective factor related to higher rates of breastfeeding initiation9–12 and longer breastfeeding duration. 12 Studies have found that after controlling for socioeconomic factors, which are often associated with poor health outcomes, Latinx ethnicity persists as a factor related to better breastfeeding outcomes compared to non-Hispanic Black women,5,13,14 a phenomenon referred to as the “Hispanic Paradox.” 15 Comparisons between foreign-born and U.S.-born Latinx mothers have found that less acculturated mothers have higher rates of breastfeeding initiation and longer duration compared to more acculturated mothers. 16
Despite the apparent good findings and marked differences in breastfeeding behaviors by country of origin, research on breastfeeding behaviors in Latinx-identifying women in the United States are rarely separated by birth country. 17 A World Breastfeeding Trends Initiative (WBTI) publication documenting breastfeeding trends in 33 countries found extreme differences in median exclusive and overall breastfeeding durations and bottle-feeding habits across the Latinx countries of origin. 18 For example, median breastfeeding durations differed significantly by over 12 months between Peru and the Dominican Republic, with the Dominican Republic having one of the shortest median durations of breastfeeding globally. 18
There is limited literature on breastfeeding behaviors, which takes into account Latinx subgroups. 17 A single study published in 1999 on a survey conducted in 1985 and 1986 addressed these differences in New York City. 19 A 2019 cross-sectional analysis of breastfeeding behaviors in Chicago found that Puerto Rican mothers have the lowest prevalence of breastfeeding in a sample of Puerto Rican, Mexican, non-Hispanic Black, and non-Hispanic white mothers, 20 while a study in Connecticut found that Puerto Rican mothers breastfed for significantly shorter time compared to Latinx-identifying mothers with different nativity. 21 None of the recent literature takes into account recent immigration trends that show growth in migration from Central America, the Dominican Republic, and South America, especially in metropolitan areas on the East Coast. 22
Objective
The purpose of this study is to address a critical gap in the literature around breastfeeding practices in the Latinx population by analyzing breastfeeding duration stratified by birth region.
Methods
Study design and data
We conducted a secondary data analysis of the New York City Work and Family Leave Survey (NYC WAFLS). 23 The WAFLS was conducted by telephone in March and April 2016 surveying NYC residents who gave birth in 2014, and the dataset was made publicly available in 2017. Participants were identified using birth certificate data and were randomly sampled to participate in the survey. The study sought to describe paid family leave patterns and study the impact of family leave policies. To meet these aims, women who self-identified as working for pay during pregnancy were oversampled. Women were eligible if they were older than 18 years at the time of the survey, spoke English or Spanish, and lived in NYC when they gave birth in 2014. Women who had already participated in an NYC survey or those whose children had died or were adopted following childbirth were excluded. Women who gave birth to multiple children in 2014 answered the survey questions about one child, randomly selected by the interviewer.
Based on the above criteria, the survey is representative of about 108,000 (90%) of the total 120,000 births in NYC in 2014. 24 The survey had a 37% response rate and an 87.6% cooperation rate, and on average took 19 minutes to complete. All questions in the survey included “I don't know” and refusal options, coded as missing data for the purposes of this study. Based on inclusion and exclusion criteria and the survey timeline, women in the sample ranged from 14 months to 2 years postchildbirth. The WAFLS dataset is available on the NYC Open Data webpage for analyses and confirmation of statistical findings. 23 Institutional Review Board approval was not required as we conducted a secondary data analysis of an existing dataset.
Research framework
The study was guided by the National Institute of Minority Health and Health Disparities (NIMHD) research framework. This framework enables a multidimensional approach to understand the complex determinants of health and health disparities. 25 The framework is a combination of the National Institute of Aging (NIA) health disparities research framework and Bronfenbrenner's socioecological model. 26 The framework is a matrix with five domains of influence on the y-axis and four levels of influence on the x-axis, creating 20 cells that represent unique factors related to health disparities. 25 The five domains of influence cover biological and behavioral factors, physical and sociocultural environments, and the health care system. The four levels of influence categorize the various levels of impact from the socioecological model: individual, interpersonal, community, and societal. The matrix of intersecting factors guided the design of the study and the selection of variables.
Measures
Table 1 is a depiction of the NIMHD framework with all included variables represented in the appropriate cell within the framework. While not all cells are included in the analysis, each domain and level of influence have at least one accompanying variable.
Variable Mapping to the National Institute of Minority Health and Health Disparities Research Framework
Dependent variable: breastfeeding
Breastfeeding survival was the dependent variable of interest measured as time to breastfeeding cessation. Participants were asked if their child ever received breast milk, and if so, for how long. Participants could respond in weeks or months or respond with “my child did not receive breast milk” or “less than one week.” Responses given in weeks were transformed into months by dividing the number of weeks by four, with each week equivalent to 0.25 months. If participants responded that children did not receive breast milk for at least 1 week, responses were recorded as 0 months. Breastfeeding initiation rate was dichotomized considering responses of 1 week or longer as positive responses.
Latinx identity, region of birth
Latinx identity was assessed with the question, “Are you Hispanic or Latino?” and recorded as a binary variable in the study. Region of birth was assessed in the survey as a closed-ended question with a numerical list of countries available for data coding. Responses were initially recorded by individual country for each participant and then subsequently grouped by region into four categories to enable statistical analyses with large enough sample sizes (Caribbean, Mexico/Central America, South America, and United States).
Covariates
We included variables identified in the U.S.-focused literature as associated with breastfeeding behaviors and available in the dataset as covariates. Participants were asked if they took any time off work after their child was born in 2014 and could answer in weeks or months or state that they took no time off. Responses given in weeks were transformed into months by dividing the number of weeks by four, with 1 week equivalent to 0.25 months. If participants responded that they did not take any time off, responses were coded as 0 months for analyses. Length of maternity leave data was subsequently categorized into four groups, (no leave, less than 2 months, 2–6 months, and greater than 6 months).
We categorized variables for age (18–24, 25–34, and 35+), highest education achieved (less than high school diploma, high school graduate or some college, college graduate, or higher), and length of neonate hospitalization (2 or fewer days, 3–5 days, and 6 or more days) into three groups. We dichotomized variables for prepregnancy health (poor/fair/good or very good/excellent), parity (primiparous or multiparous), being partnered at the time of childbirth (yes or no), type of delivery (vaginal or c-section), postpartum depressive symptom frequency in the first year (rarely/never or sometimes/often/always), language (English interview or Spanish interview), and nutrition benefit utilization (used in prenatal/postpartum time period or not used). Annual household income was not included in the analysis as it included the most missing data; however, nutrition benefit program participation can serve as a proxy for income as eligibility is income based.
Statistical analyses
We conducted statistical analyses using Stata 16.1 with statistical significance set at 0.05. The final analytic sample was determined using listwise deletion to enable a complete case analysis for all included variables. Descriptive statistics were calculated as frequencies and compared by birth region using chi-square tests. Unadjusted Kaplan-Meier survival curves were created to investigate differences in breastfeeding duration stratified by birth region, and log-rank tests were conducted to compare survival distributions. Finally, adjusted hazards ratios were calculated through a Cox proportional hazards regression analysis to compare breastfeeding hazard ratios between the countries/regions of origin controlling for covariates.
Results
Sample characteristics
A total of 1,063 mothers participated in the WAFLS, and of these, 354 identified as Latinx. Of these participants, 342 had available breastfeeding and nativity data, and in total, 282 initiated breastfeeding. There was no significant difference in breastfeeding initiation rates between the four regions (chi-square 1.6, df = 3, p = 0.666). Following listwise deletion to enable a complete case analysis, 271 (96%) of the 282 participants are included in the final analytic sample. In this final sample, 92 (34.0%) were born in the United States, 70 (26.8%) were born in the Caribbean, 64 (23.6%) were born in Central America or Mexico, and 45 (16.6%) were born in South America.
Table 2 describes the final analytic sample stratified by birth region. The groups were significantly different in terms of age (chi-square 14.9, df = 6, p = 0.021) highest level of education (chi-square 73.6, df = 6, p < 0.0001), self-assessed prepregnancy health (chi-square 52.8, df = 3, p < 0.0001), parity (chi-square 12.2, df = 3, p = 0.007), length of maternity leave (chi-square 39.0, df = 9, p < 0.0001), participation in nutrition benefits programs during the pregnancy or postpartum periods (chi-square 10.5, df = 3, p = 0.015), and survey language (chi-square 123.3, df = 3, p < 0.0001). The groups were similar in terms of type of delivery, length of neonate hospitalization, and depressive symptom frequency in the first year postpartum.
Descriptive Statistics by Birth Region
p < 0.05, **p < 0.01.
HS, high school.
Breastfeeding duration by region of birth
Kaplan-Meier survival curves (Fig. 1) were created for each birth region group, and a subsequent log-rank test indicated a significant difference of breastfeeding duration between the four groups (chi-square 19.7, df = 3, p = 0.0002). Median survival differed between the four groups (United States: 5 months, Caribbean: 3 months, Mexico/Central America: 7 months, and South America: 8 months).
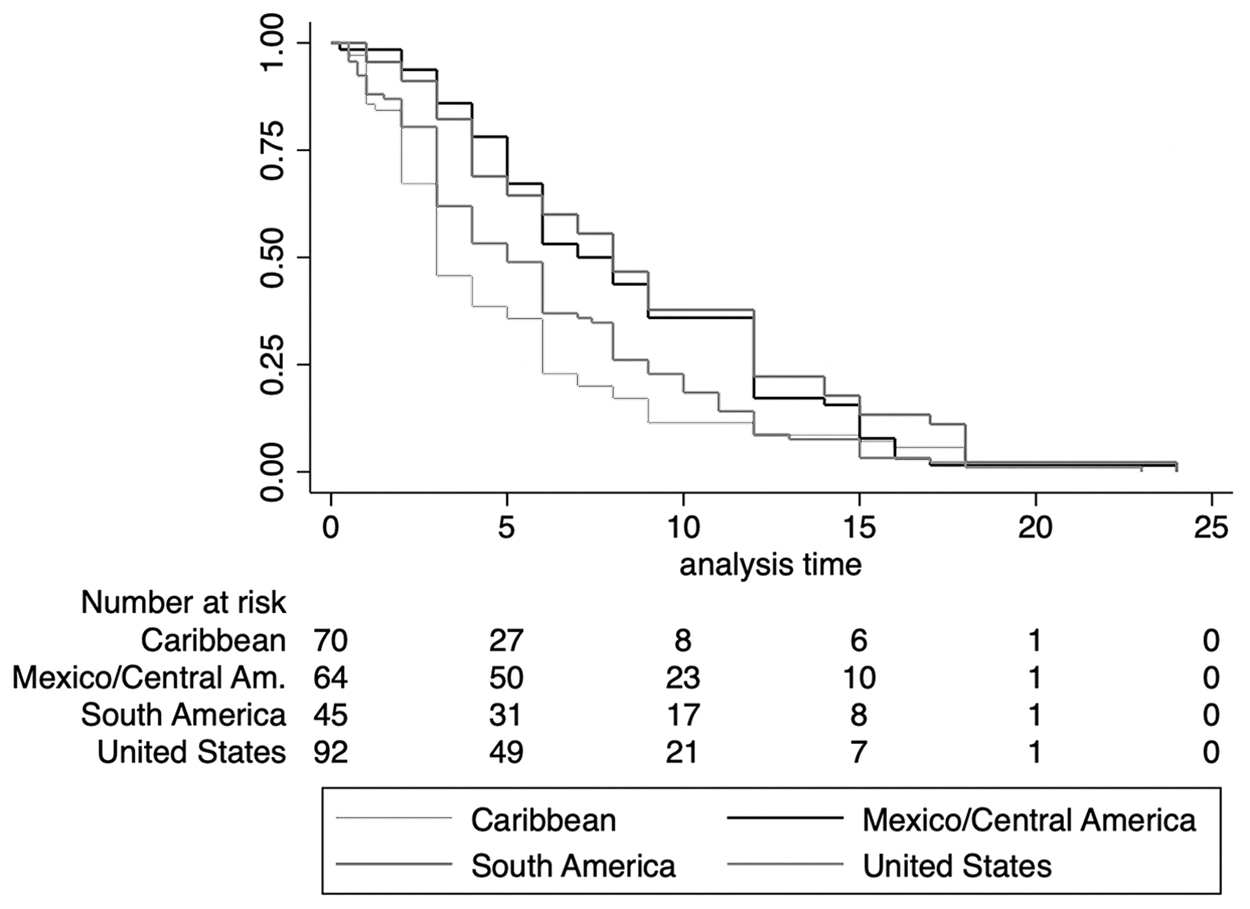
Unadjusted Kaplan-Meier survival estimates by birth region and number at risk over time.
The significant difference in breastfeeding survival by region of origin was tested in a Cox-regression analysis (Table 3) where Caribbean nativity was considered the reference group. Controlling for age, education, parity, being partnered at the time of birth, type of delivery, use of nutrition benefits programs, length of infant's hospitalization, language, and frequency of depressive symptoms in the first year postpartum, non-Caribbean birth region was still significantly associated with lower risk of early breastfeeding cessation. The decrease in risk ranged from 36% for U.S.-born participants (adjusted hazard ratio [AHR] = 0.64, 95% confidence interval [CI]: 0.43–0.95) to a 49% decrease for Mexico/Central America-born participants (AHR = 0.51, 95% CI: 0.33–0.79) and a 50% decrease for South America-born participants (AHR = 0.50, 95% CI: 0.32–0.77).
Cox Proportional Hazard Regression
p < 0.05, **p < 0.01.
CI, confidence interval; HS, high school.
In addition to significant differences in the risk of breastfeeding cessation by birth region, being partnered at the time of childbirth (AHR = 1.89, 95% CI: 1.29–2.76) and neonate hospitalization of 6 days or longer (AHR 1.64, 95% CI: 1.01–2.66) were significantly associated with earlier breastfeeding cessation. No other covariate had a significant relationship to breastfeeding duration in this adjusted analysis.
Discussion
This study found significant differences in breastfeeding behaviors in a complete case analysis sample of Latinx-identifying NYC mothers by birth region. Regional or country-specific differences in birth practices, 27 feeding behaviors, 18 and acculturative stress 28 within the Latinx population are documented phenomena in the literature. However, findings on health behaviors are regularly presented treating Latinx participants as members of a monolithic group 17 or, when compared, only as U.S. born versus foreign born. 16
Our findings confirm a need to differentiate breastfeeding findings in the Latinx population to address subgroup disparities. Caribbean-born mothers in this study breastfed for less time than all other Latinx subgroups, while South America- and Central America/Mexico-born mothers breastfed for significantly longer. These within-group differences are lost in general Latinx analyses and reinforce conclusions that Latinx mothers have breastfeeding outcomes similar to or better than mothers of other racial and ethnic backgrounds. 13 Future research should include birth country and other variables related to different cultural practices by country of origin as potential influential variables. Including parent or grandparent birthplaces may also provide insight into cultural differences, which are sustained over generations. Such culture- or country-specific variables can be identified in exploratory studies and tested in future interventions, which should be country specific for the parents.
In addition to significant differences by birth country, neonate hospital stays of 6 days or longer and being partnered at the time of childbirth were significantly associated with earlier breastfeeding cessation in adjusted analyses. Longer neonate lengths of stay following childbirth is often associated with prematurity, neonatal intensive care, or birth complications, which impact breastfeeding both in the hospital setting and following discharge. 29 Support systems must be in place in both the hospital and home settings to support Latinx mothers to continue breastfeeding after their newborn is discharged from a hospital stay longer than 1 week.
Our findings associated having a partner at the time of childbirth with earlier breastfeeding cessation. While much of the literature defines social support as a well-documented positive influence on breastfeeding initiation and duration, 30 Latinx-specific findings are mixed. Having a U.S.-born partner or a partner with longer U.S. residence decreased the odds of both breastfeeding initiation and continued breastfeeding at 6 months, 9 and targeted interventions for Latinx fathers may not improve breastfeeding behaviors. 31 In a primarily Mexican-origin population, partner relationship quality, rather than living with a partner, was significantly associated with positive breastfeeding behaviors. 32 Our findings support continued exploratory research into the impact of partners on breastfeeding practices for Latinx mothers. Qualitative research with Latinx mothers, partners, and support persons could inform future partner-focused interventions and improve understanding of breastfeeding attitudes across families.
Finally, research finds longer maternity leaves associated with longer breastfeeding duration in unadjusted models; however, these associations do not persist in models adjusted for maternal or family characteristics such as race, ethnicity, education, income, or being partnered.33–35 Similarly, our adjusted analysis found that length of maternity leave had no significant effect on breastfeeding duration. While it is important to support continued efforts to achieve longer paid leave for new parents and support breastfeeding in the workplace, our findings confirm the need to tailor interventions focused on other factors to improve breastfeeding duration in the Latinx population.
Strengths and limitations
The first limitation in this study is due to the survey representing mothers from a single city. However, New York City's Latinx population is uniquely diverse with the population consisting of growing and significant numbers of people from each of the four regions in this study. 36 This study could be repeated in other geographic areas to continue investigating within-culture differences in the Latinx breastfeeding population. The cross-sectional nature of the WAFLS, self-reported measures, and timing of the survey up to 2 years after childbirth also present limitations. Due to missing data on years of participant US residence, we were unable to consider immigrants' time in the US, a potentially significant factor. The NYC WAFLS did not directly assess breastfeeding behaviors and a number of breastfeeding-specific measures are missing, such as lactation education, attitudes, and self-efficacy. For instance, the question of nutrition benefit program participation does not clarify if WIC, a program that offers breastfeeding support and education to income-eligible families regardless of immigration status, was considered a positive response, in addition to the SNAP. Finally, due to the sample, we were unable to complete analyses using individual countries, and regional data may be insufficient.
These limitations notwithstanding, this study is the first study published in over 20 years to investigate breastfeeding patterns in the New York City Latinx population stratified by birth region. Our inclusion of maternal, infant, socioeconomic status, and workforce-specific covariates strengthens the conclusion that subgroup analyses are necessary to inform future research and tailored interventions.
Conclusion
Breastfeeding is an important public health objective in the United States. Initiatives to improve or sustain breastfeeding behaviors in the Latinx population must take into account birth country as a potentially significant factor in a mother's breastfeeding duration. Future research can identify the unique barriers to and attitudes toward breastfeeding in Caribbean Latinx women and identify the protective factors that encourage breastfeeding for Central American/Mexican and South American mothers. Additional research on U.S.-born Latinx mothers' parents and grandparents' birthplaces and feeding cultures will provide insight into the impact of acculturation at the region level. Without such distinctions, targeted interventions and public health initiatives may fail to address within-group disparities. NYC-based maternal child researchers, public health departments, and social service agencies should encourage and support investigation into within-group differences in perinatal behaviors and breastfeeding practices in the Latinx population.
Footnotes
Authors' Contributions
L.G.: conceptualization, software formal analysis, data curation, and writing—original draft; A.S.: conceptualization, writing—review and editing, and supervision; and S.J.: methodology, writing—review and editing, and supervision.
Disclosure Statement
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or nonfinancial interest in the subject matter or materials discussed in this article.
Funding Information
No funding was received for this article.