
Abstract
Importance:
Lamotrigine use during breastfeeding has significantly increased in the recent years, whereas breast milk lamotrigine pharmacokinetics data are still sparse.
Objectives:
To assess lamotrigine exposure in breastfed infants by monitoring maternal serum and breast milk concentrations.
Methods:
Breastfeeding women treated with lamotrigine were recruited to this study. Maternal trough breast milk and serum samples were collected, and additional breast milk samples were collected 1, 3, 6, 9, 12 hours after lamotrigine consumption. Trough breast milk/serum ratios (M/S ratio) and breast milk area under the curve (AUC) values were calculated.
Results:
Twenty-one breastfeeding women were recruited to this study, and the final dataset was based on the samples collected from 17 women. Lamotrigine trough serum and mother's milk concentrations were 5.1 ± 3.3 mg/L and 3.1 ± 1.9 mg/L, respectively (mean ± standard deviation). The trough M/S ratio of lamotrigine was 0.66 ± 0.22. The lamotrigine breast milk average AUC was 41.7 ± 24.6 mg·h/L. The estimated infant dose of lamotrigine was 0.52 ± 0.31 mg/kg/day and 0.26 ± 0.15 mg/kg/day for fully and partially breastfed infants, respectively. Significant correlation was found between the maternal lamotrigine serum trough concentrations and the breast milk parameters: trough breast milk concentrations (Spearman's rho = 0.986, p < 0.0001) and breast milk AUC values (Spearman's rho = 0.941, p < 0.0001). No significant correlation was found between the maternal lamotrigine daily dose and serum trough concentrations, breast milk trough concentrations, and breast milk AUC values (Spearman's rho = 0.294, 0.285, and 0.438, p = 0.252, 0.396, and 0.078, respectively).
Conclusion and Relevance:
High correlation between the maternal lamotrigine trough serum concentrations and the breast milk AUC values was found, implying that monitoring the maternal lamotrigine serum concentrations can be useful for prediction of exposure of infants to lamotrigine through the breast milk.
The trial was registered in the Israeli trials registry MOH_2021-09-05_010243 at September 5, 2021 Retrospectively registered https://my.health.gov.il/CliniTrials
KEY POINTS
Introduction
B
Epilepsy is the most common neurological disorder in pregnancy, with a prevalence of 0.5–1% in this population. 3 An epileptic seizure is associated with many risks for pregnant and breastfeeding women, ranging from mild to severe complications. 4 Thus, an effective management of epilepsy is required to prevent maternal, fetal, and newborn morbidities and mortalities, most commonly through consumption of oral antiepileptic drugs (AEDs).
As a class, AEDs have complex pharmacokinetics and a narrow therapeutic window, which lead to substantial risks in the patients, especially in the population of the pregnant and breastfeeding women. Some partial information and recommendations on the use and safety of the specific AED during pregnancy is usually available, while these data regarding the breastfeeding period are even more scarce. Analysis of the accumulation of the drug in the breast milk, its relationship to the dose and the maternal systemic drug concentrations, is the basis for the safety assessment of the AED and the risk of the infant exposure to the drug through the breast milk.
Lamotrigine is a phenyl-triazine AED that is used in the treatment of both epilepsy and bipolar disorder, as a mood stabilizer and women of childbearing age are frequently prescribed with the drug. 5 Lamotrigine is rapidly and completely absorbed after oral administration, with a negligible first-pass effect, and its absolute bioavailability reaches 98%. Approximately 55% of lamotrigine is bound to the plasma proteins, and it has a relatively small volume of distribution (1.3 L/kg). 6 The major elimination pathway of lamotrigine is glucuronidation 7 followed by renal elimination.
Direct evaluation of the infant exposure to the drug consumed with the breast milk is based on the measurement of the drug concentrations in the serum/blood sample collected from the infant, which is seldom possible due to practical reasons.8,9,12–14 Therefore, exposure of the infant to the drug is usually estimated based on an indirect approach based on the measurement of the drug concentrations in the breast milk, which is easier to collect. Several previous studies, usually based on single samples collected from the individual women, reported lamotrigine concentrations in the breast milk, which differed substantially between the studies, leading to different conclusions regarding the infant exposure to the drug through the breast milk and of the associated risks to the infant.8–11
This study aimed to analyze in a more detailed fashion the accumulation of lamotrigine in the breast milk of breastfeeding women, as an indirect measure of the infant's exposure to lamotrigine through the breast milk and of the drug safety in the breastfed infants. Additionally, we aimed to analyze the correlation between lamotrigine maternal dose, maternal serum concentrations, and the breast milk concentrations, and to identify the most feasible approach (sample type, collection time/s, etc.) for monitoring the potential infant exposure to lamotrigine through the breast milk.
Methods
This study was approved by the Institutional Review Board of the Shamir Medical Center and the patients that were recruited to the study provided their written informed consent to participate. The inclusion criteria were women with epilepsy diagnosis, treated with lamotrigine, fully or partially (at least half of the infant's daily meals) breastfeeding their infants.
Twenty-one nursing women were recruited to this study and completed a questionnaire with demographic details, medical history, dosing of lamotrigine and other medications, and information on the pregnancy, delivery, and infant's health (Table 1). The participants attended an appointment at the Clinical Pharmacology Unit of the Shamir Medical Center, at least 5 days after the last adjustment of lamotrigine daily dose (i.e., at the steady state), during which the trough serum and breast milk samples were collected, and were stored frozen at −20°C pending analysis.
Demographic and Medical Characteristics of the Participants (n = 17)
The values are presented as mean ± SD (range), median (IQR) or n (%).
SD, standard deviation.
The participants were instructed to collect six consecutive breast milk samples: one sample before the administration of the morning lamotrigine dose, and 1, 3, 6, 9, and 12 hours after the consumption of the drug. All these breast milk samples were frozen immediately after collection and were stored frozen pending analysis.
Concentrations of lamotrigine in the collected serum and breast milk samples were determined using a commercial kit (Chromsystems Instruments & Chemicals GmbH, Germany) and Varian ProStar HPLC-UV apparatus (Varian, Inc.), using appropriate calibration curves based on drug-free serum samples spiked with known concentrations of lamotrigine. The 3–14 mg/L serum concentrations of lamotrigine were considered to represent the therapeutic range of this drug, in accordance with the kit manual.
The trough breast milk/serum (M/S) ratio of lamotrigine was calculated based on the drug concentrations in the simultaneously collected trough breast milk and serum samples. The individual patients' area under the curve (AUC) of lamotrigine in the breast milk was calculated using a trapezoidal rule, and served as a basis for the calculation of the average lamotrigine breast milk concentration:
Equation 1:
The infant daily dose of lamotrigine was estimated based on the average lamotrigine breast milk concentration and the estimated daily breast milk consumption of fully and partially breastfed infants 15 :
Equation 2:
The relative infant dose (RID) of lamotrigine was calculated by dividing the infant daily dose by the maternal daily dose:
Equation 3:
Statistical analyses
Linear regression and Spearman correlation coefficients were used to assess the relationship between the continuous variables. Linear regression was evaluated to meet the assumptions of linear relationship, normal distribution of the residual and heteroscedasticity. All statistical tests were two-sided and p < 0.05 was considered to indicate statistically significant differences. SPSS software (IBMS SPSS Statistics for Windows, Version 25; IBM Corp, Armonk, NY) was used for all the statistical analyses.
Results
Twenty-one breastfeeding women were recruited to this study. Four participants did not provide milk samples according to the protocol and were excluded from the study. Table 1 summarizes the characteristics of the mothers and their infants. Thirteen infants (76%) were exclusively breastfed, while four infants (24%) were primarily breastfed (at least half of infant's nutrition based on the breast milk) and were supplemented with infant formulas; Table 2.
Individual and Average Patient Pharmacokinetic Data
AUC, area under the curve; NA, not applicable.
The maternal total daily dose of lamotrigine was 299 ± 130 (100–500) mg/day, which corresponds to 4.66 ± 2.02 (1.59–7.63) mg/kg/day [mean ± standard deviation (range)]. Maternal lamotrigine trough serum concentration was 5.09 ± 3.35 (0.95–14.1) mg/L and the trough breast milk concentrations were 3.12 ± 1.90 (0.89–8.14) mg/L. The M/S ratio of lamotrigine was 0.66 ± 0.22 (0.48–1.36).
There were substantial differences in the concentrations of lamotrigine in the breast milk samples collected from the individual participants (Fig. 1 and Table 2). The AUC of lamotrigine in the breast milk was 42.09 ± 25.59 (17.1–115.66) mg·h/L, and the average lamotrigine breast milk concentration (Cbreast milk av) 2.75 ± 1.97 (0.65–7.8) mg/L. Based on these data, the estimated infant daily dose of lamotrigine was 0.40 ± 0.16 (0.21–0.73) mg/kg/day for fully breastfed infants. The RID of lamotrigine was 11.6% ± 7.2% (4.9–31.5%) in 13 out of the 17 infants who were fully breastfed (Table 2). The estimated infant dose and RID could not be calculated for partial breastfed infants as the mothers gave only rough estimation of the daily ingested amount (e.g., “more than 50% breastfed but less than 75%”).
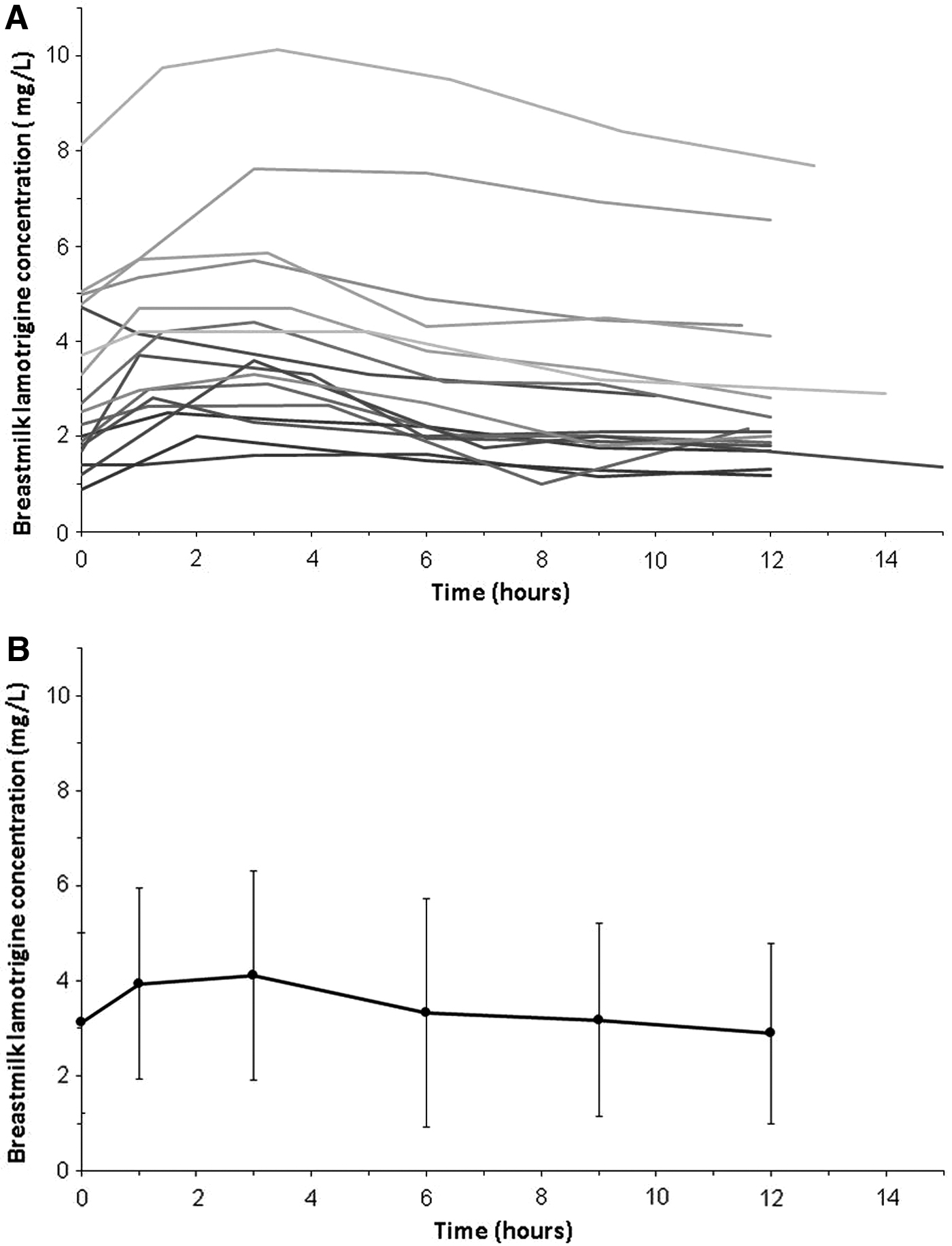
The individual and average lamotrigine breast milk concentration versus time curves (n = 17).
The drug concentrations in the body fluids (serum and breast milk trough concentrations, and the breast milk AUC values) had no correlation with the maternal lamotrigine daily dose values (Spearman's rho = 0.294, 0.285, and 0.438, p = 0.252, 0.396, and 0.078, respectively). This indicates substantial pharmacokinetic variability of the drug in the subjects that participated in our study. On the other hand, significant correlation was found between the maternal lamotrigine trough serum concentrations and trough breast milk concentrations (Spearman's rho = 0.986, p < 0.0001) or breast milk AUC values (Spearman's rho = 0.941, p < 0.0001).
There were no reports of lamotrigine adverse effects in the nursing women and the breastfed infants during the study. None of the mothers reported developmental problems in their infants during the follow-up telephone calls that were done when the infants reached the age of 12–24 months.
Discussion
Lamotrigine is an AED that has specific pharmacokinetic advantages over the older antiepileptic agents, and improved safety/efficacy balance. Specifically, it has more predictable pharmacokinetics and is less prone to undergo pharmacokinetic interactions with other drugs due to lower extent of plasma protein binding and non-CYP-mediated primary metabolic elimination pathways. 16 Still, lamotrigine is characterized by substantial pharmacokinetic variability that requires monitoring of exposure to this drug and dose adjustment in the individual patients. 17 Specifically, concomitant AEDs, body weight, and genetic polymorphisms were identified as the most significant pharmacokinetic covariates of lamotrigine that affect the drug clearance and the resulting dose–exposure relationship. 18
Results of our study, on a limited sample of Israeli breastfeeding women (n = 17), corroborate the results of the previous analyses in other countries, and indicate substantial pharmacokinetic variability of the drug (Fig. 1 and Table 2). As a result, lamotrigine concentrations in the body fluids correlated to a limited extent with the maternal daily dose (see Results section). The weight-adjusted daily dose was not correlated with serum and breast milk trough levels, which were considerably variable. This suggests that estimation of exposure of breastfed infants cannot rely on maternal dose but rather be evaluated by monitoring the drug levels in body fluids.
On the other hand, we found a high correlation between the lamotrigine breast milk concentrations and the maternal serum trough concentrations (Fig. 2A). This finding is in agreement with the results of the previous studies.8–11 The most comprehensive study, in 30 mother–infant pairs, was performed by Newport et al., 8 and revealed a wide variability in the breast milk lamotrigine concentrations (2.1–5.3 mg/L range) and in the breast milk/plasma (M/P) ratios (0.26–0.63 range). Similar results were reported in other studies: Ohman et al. 9 (0.51–6.4 mg/L, 0.47–0.77 M/P ratios), Fotopoulou et al. 11 (2.8–5.9 mg/L, 0.35–0.60 M/P ratios), and Paulzen et al. 10 (1.57–6.1 mg/L, 0.32–1.43 M/P ratios). These values are similar to the concentrations and ratios that were found in our study (0.89–8.14 mg/L and 0.48–1.36 M/P ratios, respectively).
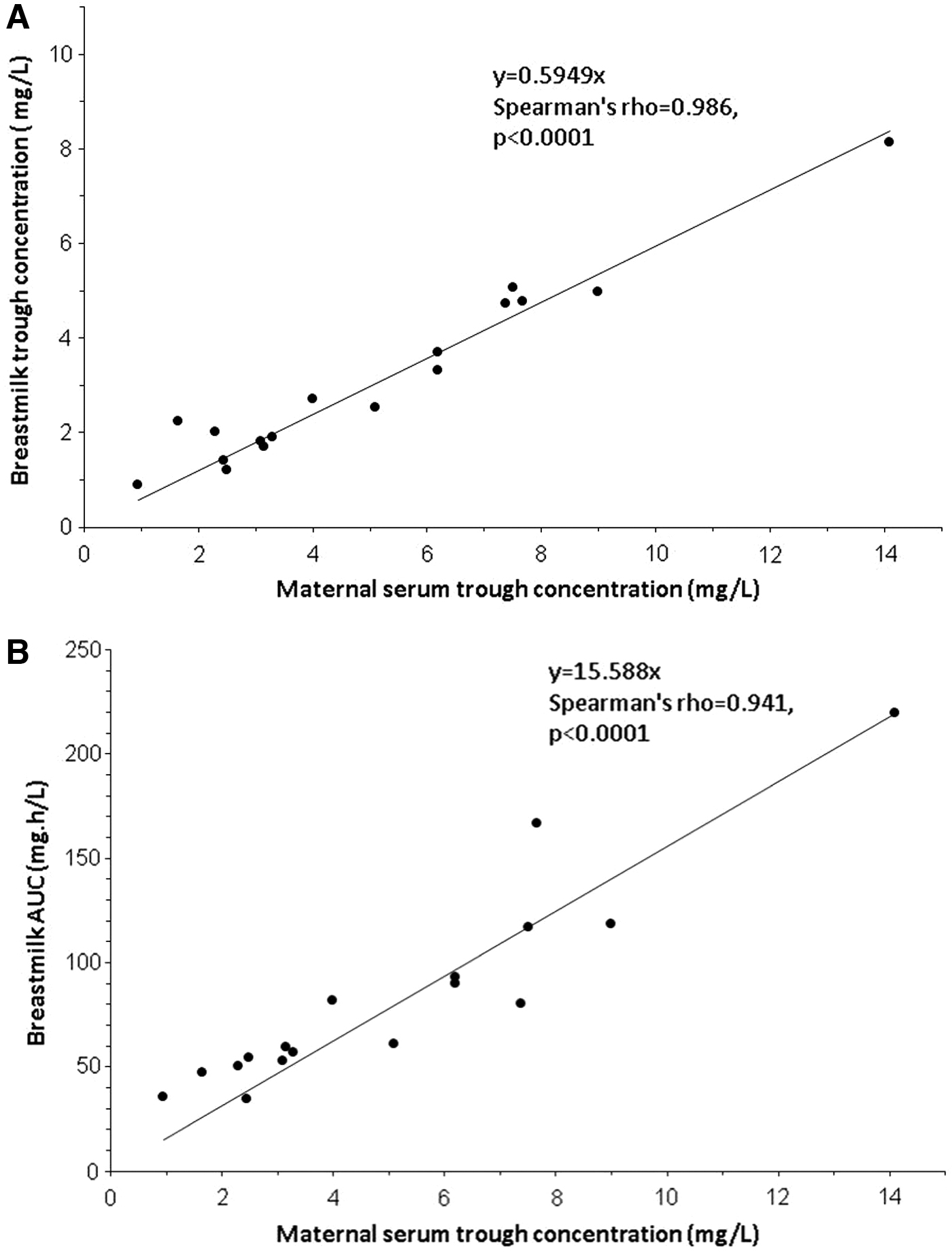
The correlation between the individual lamotrigine serum trough concentrations and the breast milk drug accumulation parameters (n = 17).
The novelty of our study originates from the serial sampling of the breast milk at different time points by the participants, which allowed the calculation of the breast milk AUC and of the average drug breast milk concentrations. Based on these data, we revealed a high correlation between the lamotrigine maternal trough serum concentrations and breast milk trough and breast milk AUC (Fig. 2A, B). We suggest, with the needed caution, which line the Equation 4 can serve to estimate breast milk AUC.
Equation 4:
where x is the maternal serum trough concentration (mg/L) and y is the estimated breast milk AUC (mg·h/L). Then one can place the estimated AUC to solve Equations 1 and 2. This can be a useful tool for practitioners when they are asked for advice. To apply this estimation for partial breastfed infants, the estimated daily consumption of fully breastfed infant, 0.15 L/kg/day should be divided by the relative amount of breastfeeding (e.g., for 50% breastfed infant the estimated consumption would be 0.075 L/kg/day). Lamotrigine has linear pharmacokinetics that differs from pharmacokinetics of other AEDs. The correlation between lamotrigine trough serum and breast milk trough or AUC cannot be used to interpret the exposure to other drugs and they need to be investigated in separate studies. 19
Unfortunately, serial maternal serum samples, as well as serum infant samples were not collected in our study due to clinical and practical reasons. Thus, it was not possible to quantify more precisely the time course and extent of the maternal and infant's lamotrigine exposure, and to validate our conclusion, Nevertheless, we conclude that a single maternal serum sample (at the trough) reflects the overall extent of the drug accumulation in the breast milk, and we recommend to monitor the maternal serum lamotrigine concentrations as an indirect measure of infant exposure to lamotrigine through the breast milk.
Based on the results of our study, we estimated the lamotrigine infant daily dose of 0.52 ± 0.31 mg/kg/day for the fully breastfed infants (daily dosage for partial breastfed infants was not determined, see above). These values are similar to the previously published estimates: 0.2–1.0, 9 0.51, 8 and 0.45 mg/kg/day. 13 It should be noted that all these estimates are much lower than the therapeutic infant dose of lamotrigine (in the range of 2 to 4.4 mg/kg/day20–22 ), which indicates overall acceptable safety of the drug in the breastfed infants.
The RID of lamotrigine was 11.6% ± 7.2% (4.9–31.5%) in the fully breastfed infants. These values are similar to the data of Newport et al., 8 which reported the RID of 9.2% (3.1–21.1%) in 30 women treated with lamotrigine for seizure, and Page-Sharp et al. 13 who found the RID of 7.6% (5.4–9.9%) in six breastfeeding women with epilepsy and bipolar disorder.
Adverse effects related to exposure to lamotrigine through the breast milk were reported in several publications (in some cases the mothers concomitantly consumed other drugs).23–25 Nevertheless, safety of exposure to lamotrigine through the breast milk was concluded in studies that were based on the data of dozens of breastfed infants.8–12,26 Moreover, the follow-up studies, at the ages of 3 and 6 years, found that the breastfed children exposed to lamotrigine did not differ in their cognition and behavior from the unexposed children, and enjoyed from the benefits of breastfeeding.27–29
Conclusions
Lamotrigine is excreted in the breast milk to a substantial extent, and we recommend to monitor the maternal and infant's exposure to this drug, and its correlation with the antiepileptic efficacy and the risk of adverse effects. In this study, we uncovered a high correlation between the maternal lamotrigine serum trough concentrations and the breast milk trough drug concentrations and AUC values. Thus, we recommend to monitor the maternal serum lamotrigine concentrations, as a parameter that represents the accumulation of the drug in the breast milk, and as an indirect measure of infant exposure to lamotrigine through the breast milk.
Consent for Publication
All participants gave their consent to publish the data presented in this article.
Availability of Data and Materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Footnotes
Authors' Contributions
E.K. made substantial contributions to the conception and design of the work; the acquisition, analysis, and interpretation of data; and drafted the work and substantively revised it. N.D. made substantial contributions to the conception and design of the work; the acquisition, analysis, and interpretation of data; and drafted the work and substantively revised it. M.B. made substantial contributions to the conception and design of the work; the acquisition, analysis, and interpretation of data; and substantively revised it. N.B. made substantial contributions to the design of the work; the acquisition, analysis, and interpretation of data; and substantively revised it. A.B.C. made substantial contributions to the design of the work; the acquisition, analysis, and interpretation of data; and substantively revised it. I.G. made substantial contributions to the analysis and interpretation of data; and drafted the work and substantively revised it. R.K. made substantial contributions to the acquisition, analysis, and interpretation of data; and substantively revised it. A.L. made substantial contributions to the acquisition, analysis, and interpretation of data; and substantively revised it. D.S. made substantial contributions to the analysis and interpretation of data; and drafted the work and substantively revised it. M.B. made substantial contributions to the conception and design of the work; the acquisition, analysis, and interpretation of data; and drafted the work and substantively revised it. M.M. made substantial contributions to the acquisition, analysis, and interpretation of data; and drafted the work and substantively revised it.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was not funded by any commercial or noncommercial body.