
Abstract
Background:
Donor milk is a good alternative for premature babies whose mothers cannot breastfeed. To reduce the risk of milk contamination, donors have to follow some hygiene instructions, including disinfecting their breast pump (BP). This study aims to investigate the efficacy of BP cleaning and disinfection methods.
Methods:
Contamination of BP parts was performed by passing milk inoculated with Bacillus cereus, Staphylococcus aureus, or Escherichia coli, through BPs. Devices were then rinsed with cold water or cleaned with hot soapy water. Disinfection was achieved using either a microwave or by immersing BP parts in boiling water. After treatment, residual bacteria were recovered by passing sterile phosphate buffer saline (PBS) through BPs before being inoculated on plates and performing bacterial counts. Method efficiency was assessed by comparing BP residual bioburden to results obtained from BPs that have not undergone cleaning or disinfection treatment (controls).
Results:
Rinsing BP parts with cold water leads to a diminution of residual bacteria in PBS recovered from device. This decrease is even more effective when hot soapy water is used. There is a slight persistence of all bacteria if disinfection of BPs is performed by using a microwave. This persistence reached up to 3.58 colony-forming unit/mL of sporulating B. cereus in PBS eluted from the pump parts. The use of boiling water, with or without cleaning step, removes bacteria to a level such that no residual contamination was observed.
Conclusions:
Cleaning BP parts in hot soapy water followed by a disinfection in boiling water ensures a completed decontamination of the BP. These results give evidences for instructions to milk bank donors for whom reducing risks of infections to minimal level is essential.
Introduction
Premature infants can be exposed to health complications or growth issues and maternal milk represents for them the most appropriate source of nutrition and protection. When maternal milk is not available, donor milk from public banks offers the best alternative for appropriate feeding.
To fulfill their mission aiming to distribute qualitative and safe products, milk banks rely on their donors. Contamination of donor milk is a matter of concern for the milk banks to limit their rejection rate and the waste of this life-saving fluid. In that way, the identification of sources of contamination and consecutive enforcement of operating procedures able to mitigate this risk are of particular importance. Several studies, among which a prospective observational study, concluded that standard or strict personal hygiene regimen had limited effects on reducing the contamination of expressed breast milk.1–4 Haiden et al observed a 10% increase of breast milk contamination likelihood when collection was done at home independent of body, hand, or nipple hygiene regimen, suggesting that domestic milk storage, cold chain maintaining, and reusable collection equipment could possibly have contributed to higher contamination rates. 1
Among milk donors, many of them use a breast pump (BP) for its expression and collection. There are many types of BPs on the market, whether manual, electric single, or electric double. Although these products have been available for many years, experimental data are missing to justify the frequency and methods of cleaning and decontamination necessary to ensure their safety, despite multiple uses. BPs have been identified as a potential source of milk contamination since decades 5 and collection at home has already been correlated to higher contamination rates than collection at hospital. 6 Some investigations following infant infections have clearly incriminated some BPs at several occasions.7–10
However, BP remains a useful device appreciated by most mothers for milk expression. Depending on the regulations, BPs appear or not to be classified as medical devices. United States and Canada regulate BPs as medical devices and in such case, users benefit from regulators' guidelines.11,12 Milk banks or health professionals usually refer mothers to manufacturers' instructions if appropriate, or to the one elaborated on their own based on good practices and the available literature to ensure safe collection of donor milk.13–15 Instructions provided by BP manufacturers are not intended for the particular situation of milk collection for premature infants, which requires increased vigilance due to supply, quality, and safety concerns, sometimes resulting in wasting of contaminated collected milk.
The Héma-Québec Public Mothers' Milk Bank is the only one authorized in the Province of Québec to offer donor milk for preterm infants <32 weeks of age, and it counts on the contribution of several hundred donors per year. After a period of high rates of donor milk rejection due to milk contamination before and after pasteurization, Héma-Québec proceeded to a revision of instructions regarding the cleaning and disinfection of BPs. To base mothers' dedicated instructions on experimental results, we investigated two methods of BP cleaning and two methods of disinfection following the contamination of three different types of BPs, that is, manual, electric single, or electric double, by Bacillus cereus, Escherichia coli, and Staphylococcus aureus. Pathogens were chosen among the ones that induce automatic donor milk discard if their presence is proven.
Materials and Methods
Study design
Three different kinds of BPs were selected from best sellers in the Province of Québec and among those advised by lactation support associations: a manual pump, Medela Harmony™, an electric pump, Medela Swing™, and a double electric pump, Purely Yours™ from Ameda. Before first use, cleaning of pumps was performed following manufacturer's recommendations. Medela Harmony 16 and Swing 17 : pump set was disassembled into its individual parts, rinsed with cold clear water, and cleaned with plenty of warm soapy water using a brush. All parts were rinsed again with cold clear water, and left to dry on a clean cloth. All parts were covered with water, boiled for 10 minutes, and leaf to dry on a clean cloth. Ameda Purely Yours 18 : all parts excepted tubing, adapter cap, and tubing adapter were covered with water, boiled for 20 minutes, and leaf to dry on a clean cloth.
All bottles of milk were kindly provided by the Public Mothers' Milk Bank of Héma-Québec. Informed consent from the mothers was obtained in accordance with our approved institutional review board protocol. Pooling of milk from 16 different mothers after thawing overnight at 2–6°C resulted in an 18 L preparation of milk. The pool of milk was distributed in 330 mL bottles and pasteurized by high-pressure processing (HPP).
Bottles were initially heated up at 60°C for 4 minutes to reach a milk inner temperature of 30–37°C. HPP was done at 425 MPas for 4 cycles of 6 minutes each in a hydrostatic pressure unit of 135 L (Hiperbaric 135; Hiperbaric, Burgos, Spain). Bioburden of the pool of milk was checked before and after HPP by plating 500 μL of milk from three bottles on two blood agar plates each time (MP0351; Oxoid). A 0 colony-forming unit (CFU)/mL count was obtained after pasteurization.
B. cereus, S. aureus, and E. coli vials were each inoculated in a bottle containing a volume of 110 mL of high-pressure processed milk to reach an estimated final concentration of 105 CFU/mL. The concentration of 105 CFU/mL was chosen because it is the limit of milk contamination accepted before pasteurization by several milk banks. 15 This level of contamination allows to better observe a bioburden reduction depending on the cleaning and sterilization methods tested. Plating of 100 μL of contaminated milk on blood agar plates was done in duplicate to check the viability of bacteria and to ensure that the desired concentration of bacteria in milk was reached. Then, 100 mL of the contaminated milk was spread with a pipette on the breast shield of a BP tested and aspirated by it.
The volume of milk aspirated by the first BP was used to contaminate the other BPs in the same way. The milk was retrieved under sterile conditions and a sample of 100 μL was collected and plated on blood agar in duplicate to confirm the bacterial contamination of milk after processing in the BP, by CFU observation and counting. Concentration of bacteria that contaminated the BPs was then calculated as CFU/mL.
After contamination of BPs, two cleaning methods were compared to results obtained from BPs that have not undergone a washing and decontamination step (control). The first method of cleaning tested was to rinse all parts of a BP with clear cold water. The second method was to clean pump components with warm soapy water (Selection original detergent, Metro™; Montreal). Previously, all parts were rinsed with clear cold water, then cleaned up as mentioned with a brush, and eventually rinsed another time with cold water.
In addition to the cleaning methods, disinfection was also tested using either a boiling method or a microwave method. Disinfection was then performed following no BP cleaning, or rinsing with cold water, or after cleaning with soapy warm water. The boiling method was realized by covering all parts of a BP with water and boiling for 10 minutes. The microwave method used a Philips Avent™ microwave steam sterilizer (No. 100730428). We complied with the manufacturer's recommendations for use. All BP components were inserted in the device containing 200 mL of water and put in a microwave (900W; Panasonic) for 4 minutes. Then, each component of the pump was dried on single-use paper towel in a biological safety cabinet.
The efficiency of cleaning and disinfection methods was assessed by bacterial count with the membrane filtration technique. Following each cleaning and sterilization step, the BP parts were assembled and 50 mL of sterile phosphate buffer saline (PBS) was used to rinse the breast shields, while the pump aspirating to collect any bacteria still deposited on the surface of the device. This step was done twice for a final rinsing volume of 100 mL.
This recovery method simulates what would be recovered from BPs, and ends up in the milk, during milk expression and collection. The two aliquots of 50 mL of PBS were filtered on a 0.45 μm pore size Millipore filtration unit (No. MVHAWGS24) by using a peristaltic pump (No. DOA-p704-AA; Gast). The filtration membrane was deposited on a blood agar plate and incubated at 37°C for 18–24 hours. Plates containing 25–250 colonies were counted for concentration of bacteria calculation (CFU/mL).
Whenever bacterial growth was observed, culture on selective media was performed for bacteria identification: B. cereus, Oxoid No. MP0201; S. aureus, Biomérieux No. 43671; and E. coli, Biomérieux No. M1260.
The study design described is summarized in Figure 1. At the end of each day, each BP and the brushes used for cleaning were disassembled and dipped into a bleaching solution (25% v/v) with cold water for 15 minutes for reprocessing. Then all components were brushed, rinsed with distilled water, and dried on single-use paper towel in a biological safety cabinet. The following day, residual contamination was investigated by rinsing the breast shields with sterile PBS, filtering on membrane, and counting bacteria on culture plates (in duplicate). The absence of CFU was a necessary condition.
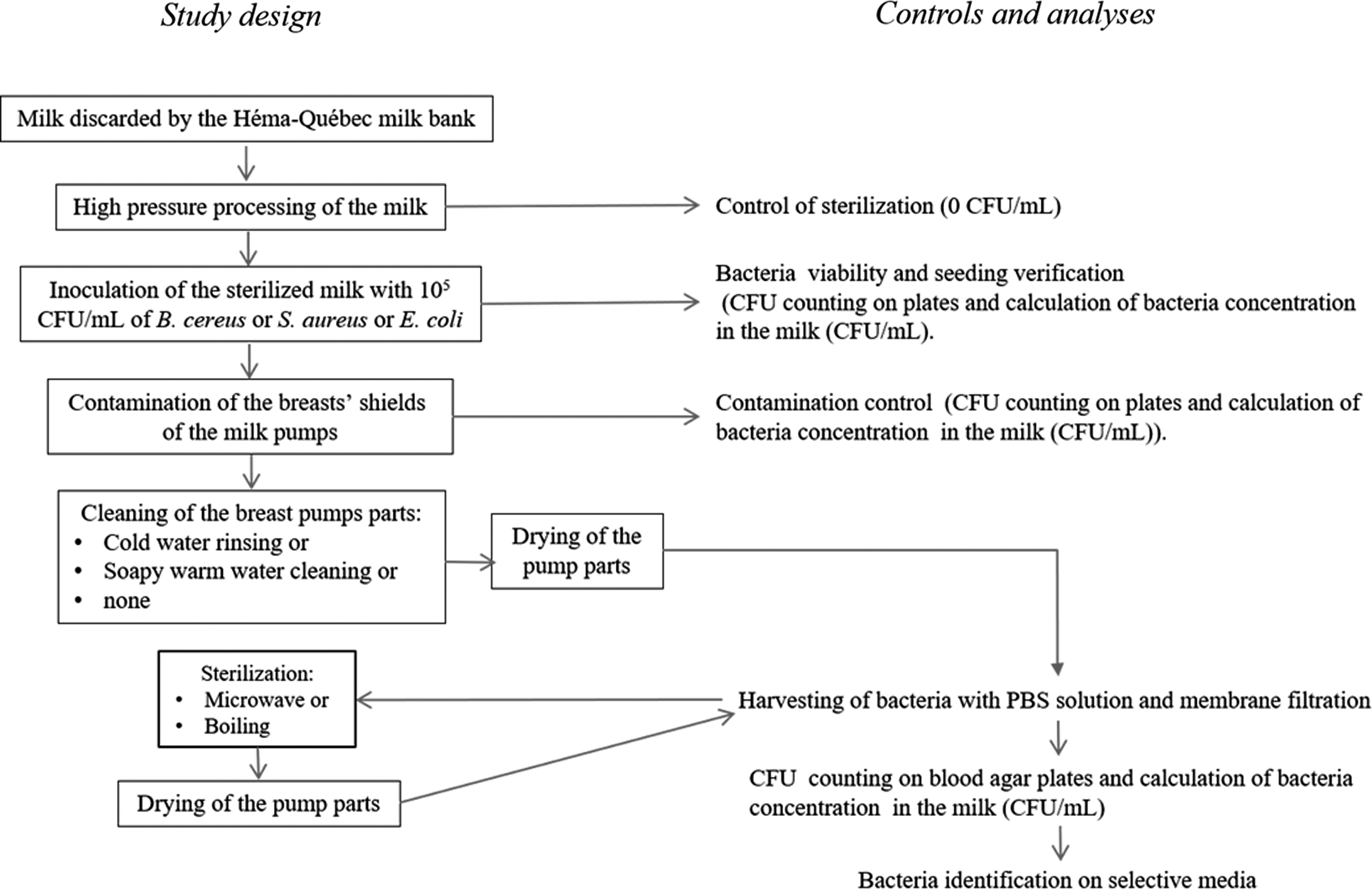
Study design, controls, and analyses. CFU, colony-forming unit; PBS, phosphate buffer saline.
Each experimental condition of milk contamination, cleaning, disinfection, and reprocessing of BPs was replicated thrice (n = 3).
Bacterial strains
Strains selected came from the American Type Culture Collection (Staphylococcus aureus ATCC 27217) or were isolated from milk of the milk bank (Escherichia coli CLI-LSPQ-56 and Bacillus cereus CLI-LSPQ-52).
Bacteria were cultured at 37 ± 2°C in Nutrient Broth culture media. Bacterial culture concentration was estimated by spectrophotometry at 600 nm. Stocks were constituted and stored at −80°C in vials containing 20% of glycerol. Aliquots were plated on blood agar to determine by serial dilution the concentration of bacterial stocks. The mean concentrations of E. coli, S. aureus, and B. cereus were, respectively, estimated at 4.15 × 108 CFU/mL (% coefficient of variation [%CV] of 10%), 7.3 × 108 CFU/mL (7% [%CV]), and 1.43 × 107 CFU/mL (3% [%CV]).
Bacillus sp. sporulation
For B. cereus sporulation, we used the strain CLI-LSPQ-52 isolated at the milk bank. A bottle of 25 mL of Nutrient Broth medium was inoculated with a selected sporulating colony of the strain of B. cereus and then incubated for 24 hours at 37°C. A volume of 200 μL of cultured B. cereus was used to seed each of 50 agar plates. Following 8 days of incubation at 37°C, 2 mL of sterile water was added to the plates to harvest the spores. Spores in suspension were mixed in a bottle and warmed at 65°C for 15 minutes under agitation to inactivate the vegetative cells.
The suspension was centrifuged at 2,700 g for 15 minutes at 4°C. Supernatant concentration was estimated by serial dilution on agar plates. Vials of 1 mL of spore suspension were stored at −80°C. The mean concentration estimated in three vials was 7.43 × 107 CFU/mL (14% [%CV]). Sporulation was not only assessed by microscopy but also verified by comparing bacterial growth on agar plates of nonheated (allow the growth of vegetative and sporulating bacteria) and heated vials at 65°C for 15 minutes (allow only the growth of sporulating bacteria).
Statistics
Averages and standard deviations were determined using the Microsoft Excel software. Mean ± standard deviation and median were obtained on all plates by specific cleaning and disinfection conditions.
Results
The viability and concentration of bacteria at the time of milk inoculation and after contamination of breast shields of the pumps were determined and the results are shown in Table 1. Bacteria were all seeded at the estimated concentration of 105 CFU/mL and we observed in the milk a mean concentration (± standard deviation [minimum–maximum]) of 104,685 ± 31,131 (26,000–151,000) CFU/mL for E. coli and 126,296 ± 76,999 (69,000–364,000) CFU/mL for the spores of B. cereus.
Concentration of Total Bacteria Following Inoculation of 100,000 CFU/mL in Milk and Concentration of Bacteria Following Breast Pump Contamination
Results are shown as mean ± standard deviation (minimum–maximum) (n = 3).
BP, breast pump; CFU, colony-forming unit.
After BP contamination, the concentration of both E. coli or the spores of B. cereus collected on the shields was in the same range as measured for the respective contaminated milk, whatever the type of BP.
We observed that the concentrations in the milk immediately after inoculation of both S. aureus and the vegetative form of B. cereus were <105 CFU/mL. We determined a concentration of 22,390 ± 15,572 CFU/mL of S. aureus and 530 ± 308 CFU/mL of the vegetative form of B. cereus. Both concentrations determined after BP contamination were even lower, showing a bacterial content decrease along time as it took about 30 minutes from the inoculation of the milk to the last BP contamination. Particularly, the concentration of vegetative form of B. cereus drastically reduced as low as 23 ± 17 CFU/mL, as measured on double electric BP.
The different cleaning and disinfection conditions have been tested following contamination of the three types of BPs by E. coli, S. aureus, or B. cereus in vegetative and sporulated forms. The results showing residual bacterial median concentration on the devices are shown in Tables 2 to 5 , respectively. Total residual bacteria on cleaned and/or disinfected BPs following induced contamination is shown in Supplementary Figures S1 to S4 in the Supplementary Data.
Concentration of Escherichia coli Recovered in Phosphate Buffer Following the Cleaning and Disinfection of Breast Pumps
Results are shown as median ± standard deviation (minimum–maximum) (n = 3).
BP, breast pump; CFU, colony-forming unit.
When rinsing with cold water only, without any disinfection method, and depending the use of manual, single or double electronic pumps, residual concentration of E. coli detected was between 0.0 and 3.76 CFU/mL (Table 2), while the residual concentration of S. aureus was between 0.0 and 0.6 CFU/mL (Table 3). B. cereus, in its sporulated form, residual concentration following cold water rinsing was between 0.02 and 8.88 CFU/mL (Table 4).
Concentration of Staphylococcus aureus Recovered in Phosphate Buffer Following the Cleaning and Disinfection of Breast Pumps
Results are shown as median ± standard deviation (minimum–maximum) (n = 3).
BP, breast pump; CFU, colony-forming unit.
Concentration of Sporulating Bacillus cereus Recovered in Phosphate Buffer Following the Cleaning and Disinfection of Breast Pumps
Results are shown as median ± standard deviation (minimum–maximum) (n = 3).
BP, breast pump; CFU, colony-forming unit.
Cleaning of pumps parts with soapy warm water revealed to remove bacteria to a level such that no residual contamination was observed (median of 0.0 CFU/mL), whatever the type of bacterial contamination. Two disinfection methods were evaluated, boiling or using a microwave. When tested without previous cleaning, the disinfection with a microwave following contamination with spores of B. cereus revealed a persistence of 0.02–3.58 CFU/mL on the pump parts (Table 4). The use of microwave to disinfect uncleaned BPs contaminated with E. coli or S. aureus was efficient as no residual persistence of both bacteria was detected (median of 0.0 CFU/mL) (Tables 2 and 3). Boiling alone, without prior cleaning of pump parts, reduced the bacterial contamination so much that no bacteria could be detected on each type of the BPs, whatever the pathogens used for contamination of devices (median of 0.0 CFU/mL in all conditions) (Tables 2–5).
Concentration of Bacillus cereus in Its Vegetative Form Recovered in Phosphate Buffer Following the Cleaning and Disinfection of Breast Pumps
Results are shown as median ± standard deviation (minimum–maximum) (n = 3).
BP, breast pump; CFU, colony-forming unit.
When combining a cleaning step and a disinfection step, a median of 0.0 CFU/mL was detected in all conditions tested. The initial level of contamination by the vegetative form of B. cereus revealed to not be sufficient to observe a diminution of bacterial load following the cleaning or the disinfection of the pump's parts. Residual contamination on the three BPs and on the brush has also been tested following sterilization after daily experiments were completed. We observed a median of 0.00 CFU/mL on each type of pumps, while a mean residual bacterial load of 0.13 CFU/mL was detected on the brush (data not shown).
Discussion
In this study, we show that rinsing BP parts with cold water only results in residual detection of E. coli, S. aureus, or B. cereus. The disinfection of BP parts not previously cleaned was incomplete when using a microwave, following contamination with spores of B. cereus. Boiling alone, without prior cleaning of the pump parts, or combining a cleaning step and a disinfection step, was an efficient method to remove bacterial contamination.
Human milk is naturally colonized by commensal micro-organisms, 19 but contamination by pathogenic bacteria can occur throughout the process of expressing and storing milk due to insufficient cleaning of hands and pumping equipment, or improper handling. This is really of interest when talking about collecting breast milk for very fragile premature babies through a milk bank. To our knowledge, this study is the first experimental demonstration in a controlled environment, which shows the efficiency of cleaning and disinfection methods employed routinely by milk donors at home with BPs available on the market.
Experiments of contamination of BPs with about 105 CFU/mL of E. coli and B. cereus spores, and about 104 CFU/mL of S. aureus, showed that rinsing with cold water reduced the number of pathogens, but did not remove all bacteria from the pump parts. Cleaning with soapy warm water and brushing the BPs revealed to be efficient enough to reduce bacterial load to undetectable level on each type of the devices tested. This is the recommended method by several health agencies for common use of BPs, and adopted by several manufacturers.20–23 However, boiling of BP parts should also be performed since very dangerous pathogens, Pseudomonas aeruginosa, for example, can be found in domestic water, and therefore, on the brushes used to clean BPs and left wet between uses. This is less of a problem for milk destined for milk banks and which will be pasteurized.
However, this could cause a real health risk for babies in intensive care units, for whom mothers express their milk. A disinfection of pump parts with a microwave alone, without prior cleaning, was partially efficient, given the residual contamination observed with spores of B. cereus. This should draw attention to the fact that using a microwave bag should not replace cleaning the pump parts with soapy warm water. Boiling pump parts for 10 minutes in water was a good disinfection method since any pathogen was detectable in our experiments. This method is thus preferred to microwaving alone.
The difference between these two decontamination methods lies in the fact that the BP that is immersed in boiling water benefits from a direct dilution of heat-resistant contaminants, relative to the volume of boiling water used) compared to the microwave-disinfected BP, which is located on the top of the apparatus, and treated with steam using the boiling water found in the bottom. Then, there is no contact with the water, and consequently, the dilution of contaminants is therefore reduced.
An efficient cleaning of BP parts at home depends on the care taken to do it, on the compliance with instructions, and on the level of contamination of the brush or the sink used, if not cleaned properly or replaced after each use. Combination of cleaning using warm soapy water with an additional disinfection method could be justified, depending on risk assessment and the collection context.
To face the issues of donated milk wasting at the human milk bank of Madrid, Spain, Flores-Antón et al report the implementation of BP steam decontamination, in addition to washing with water and detergent after each use, 24 while Swedish milk donors are required to wash and disinfect by boiling the pump parts after milk expression. 25 Recently, Rigourd et al suggested a guideline for the use of chlorine solution for BP cold decontamination following liquid soap pre-cleaning, based on extended safety analysis of chemical residuals and bacterial content. 26
Recommendations of best practices are still based mostly on consensus views, emphasizing a need for evidences relying on experimental data to support them and to go beyond the ones adopted by manufacturers for common use. 14
Manufacturers' instructions must be followed when provided, but it has to be kept in mind that BPs are not regulated the same way throughout the world and that safety instruction requirements could be impacted and lacking. For example, in Europe, BPs intended for use without medical purpose by the manufacturer are not considered medical devices and do not need a Conformité Européenne (European compliance) marking under 93/42/European Economic Community Directive, which means that no detailed instruction is needed. 27 In the United States and in Canada, BPs are all considered medical devices.11,12 This status protects consumers and patients, but it does not mean that instructions for use provided by the manufacturer related to the cleaning or disinfection of the pump have been extensively validated or will be evaluated in the regulation process to ensure their effectiveness.
Instructions recommended by a manufacturer may not be questioned if there is no apparent health hazard due to common use of the device. The resulting situation where there is a lack of publicly available data on the evaluation of BP cleaning and disinfection methods is prejudicial when additional measures are needed to mitigate the risks of milk contamination, for example, in the context of premature or weakened condition infant feeding.
This precaution is of importance if we consider the results obtained by Flores-Antón et al who observed, in a prospective comparative study, that a standard method of washing, rinsing, and drying resulted in higher rates of milk discarding pre-pasteurization due to contamination of donor milk than a combination of standard method with steam decontamination of BP parts. 24 In the situation where the milk banks must ensure to collect the safest raw milk, limit wastage, and ensure optimal supply, appropriate decontamination procedures following milk expression by mothers must be found to reach these objectives, while considering that they may be demanding for the donors and be a source of difficulties. 25
At Héma-Québec, an extensive work has been done to improve donor milk quality before its processing, notably illustrated through strict hygiene practice supporting information for the benefit of mothers. A collaboration between the Héma-Québec customer services and the Public Mothers' Milk Bank has resulted in the edition of a pamphlet distributed to first donors, detailing how to collect their own milk the best way and describing BP cleaning after each use, as follows: after each collection, the BP components and collection bottles should be thoroughly cleaned with hot soapy water.
Following a rinsing step with clear water, the BP components and collection bottles should be boiled for 5 to 10 minutes, placed on a clean unused cloth, air dried, and stored in a clean place. Mother's milk qualification criteria are also in place for milk pre-selection. Batch contamination must be below 100,000 CFU/mL total bacteria, below 10,000 CFU/mL Enterobacteriaceae, and without any bacillus or S. aureus CFU.
Among the limitations of this work, we were unable to contaminate BPs with 105 CFU/mL of S. aureus or with the vegetative form of B. cereus. Thus, it cannot be excluded that a residual contamination could have been found after cleaning or disinfection if higher initial bacterial load was used. We observed that these two Gram-positive bacteria had a low survival rate in HPP breast milk (Table 1). Antibacterial property of the milk is well known28,29 and has already been shown that the presence of lysozyme in breast milk causes the lysis of walls of Gram-positive bacteria such as B. cereus.30,31 Because our team and others have observed that HPP preserves lysozyme activity in breast milk,32–34 antibacterial property of lysozyme could therefore explain the nonviability of the vegetative form of B. cereus observed.
At the opposite, in our experimental setting, spores of B. cereus and E. coli seemed to be very resistant to any natural antimicrobial substance in the milk since their concentration was stable and equivalent to their concentration at inoculation time (Table 1).35,36 It is of interest to note that PBS has minimal detergency capacity. We are aware that the simple rinsing of the BP with this solution will not recover 100% of the contaminant and that bacteria still deposited on the surface of the device. A detergent without antimicrobial activity, such as Fluid D, would have been a better solution. Another limitation is that this type of experiments would benefit to be done with other kinds of pathogens to further test the methods of cleaning and disinfection.
Conclusions
Because donor milk is intended for very vulnerable babies, breast milk contamination represents a significant challenge for milk banks, which must ensure to communicate appropriate instructions to milk donors to reduce contamination during handling and collection of milk. Our results show that cleaning of BP parts with soapy warm water and using boiling water for 10 minutes as a disinfection method showed excellent results of BP decontamination and gives evidence for instructions to milk donors when reducing risks of infections to minimal level is needed. This study is important because it provides scientific evidences that were lacking, as mentioned by several infection control experts and agencies14,21 and could support future or existing best practice recommendations for milk banks.
Footnotes
Acknowledgments
The authors want to thank all mothers who donate milk to Héma-Québec's Public Mothers' bank. We also wish to thank Charles Lavigne from Centre de développement bioalimentaire du Québec for human milk processing by HPP.
Authors' Contributions
A.L.L.: significant contribution to performing the research, data compilation, and analysis, participated in writing the article, and prepared the tables and figure. A.T.: contributed to performing the research and data compilation. A.G.: contributed to data analysis, writing the article, and preparing tables and figure. M.G.: contribution to conceptualization and methodology of the study, supervision of personnel, data analysis, and article review and editing.
Disclosure Statement
The authors have no conflicts of interest to report.
Funding Information
No financial support was used for this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.