
Abstract
Purpose:
To analyze the effect of different feeding types on bronchopulmonary dysplasia (BPD) in very low birth weight preterm infants.
Methods:
The Cochrane Library, PubMed, Embase, China National Knowledge Infrastructure (CNKI), Wanfang Data Knowledge Service Platform, China Biomedical Literature Database (CBM) were searched for literature related to breastfeeding and BPD, with a search period from their inception to January 2023. Two researchers independently screened the literature, extracted data, and assessed the quality of included studies before analyzing the data using Stata16 and RevMan5.4.1 software.
Results:
A total of 17 studies were included. The results showed that there was no significant difference in the frequency of BPD between human milk (HM) and donor human milk (DHM) (OR = 0.54, 95% CI: 0.29–1.03, p = 0.07). However, DHM had a significant effect in reducing the frequency of BPD compared to preterm formula (PF) (OR = 0.62, 95% CI: 0.41–0.94, p = 0.02). Exclusive HM also had a significant effect in reducing the frequency of BPD compared to exclusive PF (OR = 0.51, 95% CI: 0.34–0.78, p = 0.002), as well as compared to any PF (OR = 0.57, 95% CI: 0.37–0.88, p = 0.01). Furthermore, mainly (>50%) HM had a significant effect in reducing the frequency of BPD compared to mainly PF (OR = 0.72, 95% CI: 0.55–0.93, p = 0.01). However, there was no statistically significant difference between any HM and exclusive PF (OR = 0.88, 95% CI: 0.62–1.23, p = 0.46).
Conclusions:
Our study findings suggest that both HM and DHM have a significant protective effect in reducing the frequency of BPD occurrence compared to PF. Furthermore, even when the amount of HM is insufficient, feeding more than 50% of the HM volume still provides a protective effect against the frequency of BPD. Therefore, we recommend feeding infants with more than 50% of HM to harness the protective effect of HM against BPD occurrence.
Introduction
Very low birth weight infants (VLBWIs) are defined as newborns with a birth weight less than 1500 g. The incidence of VLBWI in China is ∼6.6%, while in the United States it is about 1.5%. 1 VLBWIs have immature development in various organs and tissues and often require admission to neonatal intensive care units (NICUs) for treatment after birth. Most of these infants require mechanical ventilation and continuous oxygen therapy in the early stages, not only leading to high rates of complications and mortality but also increasing the risk of severe disabilities among survivors. One of the common severe complications in preterm infants is bronchopulmonary dysplasia (BPD), 2 which significantly affects the quality of life of affected infants.
BPD, 3 also known as chronic lung disease of the newborn, is a common respiratory system disorder among premature infants, especially those with VLBWI or extremely low birth weight (ELBW). The main causes of BPD are damage to the immature lungs caused by various adverse factors such as oxygen toxicity, barotrauma or volutrauma, infection or inflammation, as well as abnormal repair of lung tissue after injury. The smaller the gestational age (GA) and the lower the birth weight the higher the incidence of BPD. BPD not only prolongs the hospital stay of premature infants and increases hospitalization costs but also increases the risk of long-term complications, rehospitalization, and neurocognitive impairment. 4 BPD is not just a lung disease, and its adverse effects on the respiratory, nervous, and other systems can persist into adulthood, affecting adult health and quality of life. 5 With the development of assisted reproductive technology, perinatal medicine, and neonatology, the success rate of rescuing VLBWI and ELBWI in China has been increasing. However, this has led to an increasing incidence of BPD. 6
Breastfeeding has been widely recognized for its role in improving the survival rate and health of preterm infants. Clinical studies both domestically and internationally have shown that breastfeeding can promote lung development in preterm infants, regulate immune function, and reduce the incidence of BPD by improving nutritional status and providing antioxidant and immune active factors. 7 Currently, the exclusive breastfeeding rate for preterm infants in NICUs in China is less than 15%, 8 with most being fed a mixture of breast milk and formula at varying ratios. In recent years, numerous studies both domestically and internationally have pointed out the protective effect of breastfeeding on BPD in preterm infants. Therefore, in light of the current low exclusive breastfeeding rate in China, this study is based on the current research status of the impact of breast milk on the risk of BPD, aiming to summarize the existing evidence on the relationship between breast milk and BPD.
Materials and Methods
Database and retrieval strategy
We conducted a systematic search of English databases, including Cochrane Library, PubMed, and Embase, as well as Chinese databases, including China National Knowledge Infrastructure (CNKI), Wan Fang Data, and China Biology Medicine (CBM), from their inception to January 2023. Both subject headings and free-text terms were used for the search. The search terms included “Milk, Human or Breast Feeding or Breast Milk Expression or Milk Banks AND Premature Birth or Infant, Premature or Intensive Care Units, Neonatal or Infant, Very Low Birth Weight or Infant, Extremely Low Birth Weight AND Bronchopulmonary Dysplasia or Outcome Assessment, Health Care”. In addition, we performed a secondary search of the reference lists of included studies to identify relevant research that met our criteria.
Qualification criteria and research selection
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram (Fig. 1) and PRISMA checklist (Supplementary Table S1) were used.
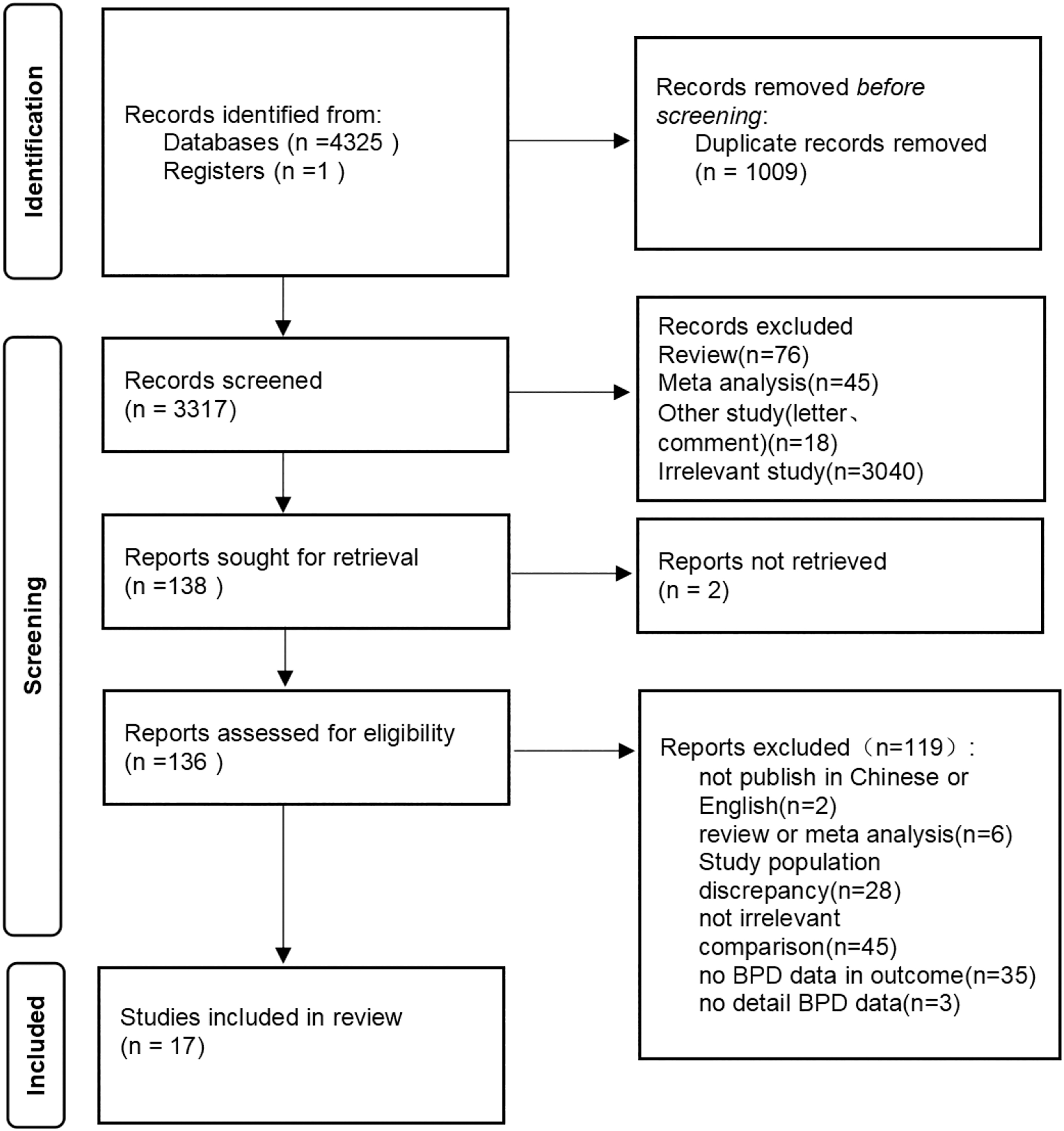
Flow-chart of search strategy.
Inclusion criteria: (1) randomized controlled trials (RCTs) or cohort studies; (2) study participants were extremely preterm infants (<32 weeks) and/or VLBWIs (weight <1500 g); (3) outcome measures included BPD.
Exclusion criteria: (1) absence of a control group; (2) mixed feeding without specific feeding proportions; (3) erroneous data or study quality lower than 6 points; (4) case reports, meta-analyses, reviews, and other studies.
The definition of BPD was oxygen dependency at 28 days postnatal or at a corrected GA of 36 weeks.
Literature screening and data extraction
Two researchers (L.X. and G.Y.) independently searched the database using the same inclusion criteria to identify potentially eligible studies. Subsequently, the two members compared the initially included studies and resolved any discrepancies through discussion and consultation with a third member when necessary, ultimately selecting the literature that met the study's requirements and could be extracted. Using a predesigned data extraction table, data on study name, publication year, country, grouping status, birth weight, GA, gender, BPD definition, duration of mechanical ventilation, and duration of oxygen therapy were extracted independently by the two researchers, with any disputes resolved through joint discussion and judgment. The registration number for this article is CRD42023380749.
Literature quality evaluation
Two researchers (L.X. and G.Y.) used RevMan 5.4.1 to assess the risk of bias in the included RCT studies and evaluated the quality of the included observational studies using the Newcastle–Ottawa Scale (NOS). The NOS items include selection of studies (0–4 points), comparability (0–2 points), and outcome/exposure (0–3 points), with a total score of 9 points. For RCT studies, the Cochrane risk of bias assessment tool was used, which includes selection bias (random sequence generation, allocation concealment), performance bias (blinding of participants and personnel), detection bias (blinding of outcome assessors), attrition bias (incomplete outcome data), reporting bias (selective reporting of study results), and other potential biases. After independent evaluation by the two researchers, the first and second authors cross-checked and discussed the literature with different opinions. If unresolved, the third researcher arbitrated.
Statistical methods
All data were imported into Stata 16 software and RevMan 5.4.1 software for Meta-analysis. The effect size was measured using the odds ratio (OR), 95% confidence interval (CI), and p-value. Results with a p-value <0.05 were considered statistically significant. Considering the heterogeneity among studies, we used a random-effects model for analysis, which accounts for between-study variability. Subgroup analysis and sensitivity analysis were also performed to further explore the sources of heterogeneity and assess the stability of the results. For publication bias, we evaluated RCT studies using the Cochrane risk of bias assessment tool and assessed all included studies using Egger's Test and Begg's and Mazumdar's Tests. Subsequently, meta-regression analyses were conducted on publication year, sex, birth weight, and GA using a random regression model.
Result
General situation of inclusion in the study
After screening titles, abstracts, and full texts, 138 potentially relevant studies were identified. Ultimately, 17 studies9–25 met the inclusion criteria, with 3 being RCTs17,20,23 and 14 being observational studies.9–16,18,21,22,24,25 The literature inclusion process is shown in Figure 1, and the general characteristics of the included studies are presented in Table 1. To facilitate data synthesis, multiple intervention groups in some studies were merged for analysis according to the inclusion criteria. Feeding types were categorized into six groups: human milk (HM) and donor human milk (DHM); DHM and preterm formula (PF); Exclusive HM and Exclusive PF; Exclusive HM and Any PF; Mainly HM and Mainly PF; Any HM and Exclusive PF.
Characteristics of Included Studies
HM, human milk; PF, preterm formula; DHM, donor human milk; M, mixed feeding with HM and PF; NOS, Newcastle–Ottawa Scale; RCT, Randomized Controlled Trial; BPD36, need for supplemental oxygen or any respiratory support, including moderate and severe BPD, at 36 weeks postmenstrual age; BPD28, moderate to severe BPD defined as requiring >21% supplemental oxygen for at least 28 days of oxygen therapy.
Quality assessment and bias risk assessment
Three RCTs17,20,23 scored high in terms of random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, and selective reporting. One study 23 was assessed as having an unclear risk of bias due to incomplete outcome data, and two studies17,20 were assessed as having an unclear risk of bias for other potential biases (Supplementary Fig. S10). Fourteen observational studies9–16,18,21,22,24,25 scored between 6 and 9 points on the NOS, with the highest score being 9 points. The average score for the included studies was 7.3 points (Table 2).
Newcastle–Ottawa Scale Scoring Results
Selection, Maximum score of 4 points; Comparability, Maximum score of 2 points; Outcome, Maximum score of 3 points.
Meta-analysis and meta-regression results
HM versus DHM
Four studies13,17,22,23 (n = 717) compared infants fed exclusively HM to those fed DHM. The meta-analysis results showed that, compared to DHM, exclusive HM had no significant effect on BPD (OR = 0.54, 95% CI: 0.29–1.03, p = 0.07) (Table 3 and Supplementary Fig. S1). After excluding the study by Schanler et al., 23 who did not provide a clear definition of BPD in their article, exclusive HM still had no significant effect on BPD (OR = 0.45, 95% CI: 0.19–1.09, p = 0.08). After excluding the study by Sun et al., 13 whose control group was frozen HM without pasteurization, the effect of exclusive HM on BPD remained statistically nonsignificant (OR = 0.70, 95% CI: 0.45–1.09, p = 0.11).
Meta-Analysis Results
HM; human milk; PF, preterm formula; DHM, donor human milk; OR, odds ratio; 95% CI, 95% confidence interval.
When analyzing the between-group differences in GA, the meta-analysis found no significant differences (OR = −0.05, 95% CI: −0.20 to 0.10, p = 0.59) (Supplementary Fig. S2). Two of the studies17,23 were RCTs, and a subgroup analysis showed that in RCTs, exclusive HM had no significant effect on BPD (OR = 0.69, 95% CI: 0.42–1.12, p = 0.13) (Supplementary Fig. S3). Sensitivity analysis revealed that after removing any single study, exclusive HM had no significant effect on BPD (Supplementary Fig. S4).
Three studies13,17,23 reported data on the number of days on mechanical ventilation. The meta-analysis showed that exclusive HM had a significant effect on reducing the number of days on mechanical ventilation (MD −2.66, 95% CI: −4.14 to −1.18, p = 0.0004) (Supplementary Fig. S5).
The meta-regression analysis results showed that year, sex, GA, and birth weight had no statistical significance for BPD, indicating that these factors do not affect the incidence of BPD (Table 4).
Meta-Regression Results
HM, human milk; PF, preterm formula; DHM, donor human milk; GA, gestational age; k, numbers of primary studies.
DHM versus PF
Five studies16,19,20,22,23 (n = 882) compared infants fed DHM to those fed exclusively PF. The meta-analysis found a statistically significant effect of DHM in reducing the frequency of BPD compared to PF (OR = 0.62, 95% CI: 0.41–0.94, p = 0.02) (Table 3, and Supplementary Fig. S1). When analyzing the between-group differences in GA, the meta-analysis found no significant differences (OR = 0.04, 95% CI: −0.09 to 0.17, p = 0.55) (Supplementary Fig. S2); sensitivity analysis indicated that the results remained significant after excluding any single study.
The meta-regression analysis results showed that year, sex, GA, and birth weight had no statistical significance for BPD (Table 4).
Exclusive HM versus exclusive PF
Four studies9,10,22,23 (n = 795) compared infants fed exclusively HM to those fed exclusively PF. The meta-analysis found a statistically significant effect of exclusive HM in reducing the frequency of BPD compared to exclusive PF (OR = 0.51, 95% CI: 0.34–0.78, p = 0.002) (Table 3 and Supplementary Fig. S1). One study 23 did not provide a clear definition of BPD, and after excluding it, the meta-analysis showed no statistically significant effect of exclusive HM on BPD (OR = 0.59, 95% CI: 0.32–1.07, p = 0.08). When we analyzed the between-group differences in GA, the meta-analysis found no significant differences (OR = −0.03, 95% CI: −0.17 to 0.12, p = 0.33) (Supplementary Fig. S2). However, one study had a significant between-group difference in GA of ≥0.5 weeks. After excluding the study by Assad et al., 9 the results still showed a significant effect of exclusive HM on BPD (OR = 0.46, 95% CI: 0.30–0.69, p = 0.0002).
Two studies10,23 provided data on the number of days of mechanical ventilation. The meta-analysis showed that receiving exclusive HM had no significant effect on the duration of mechanical ventilation (MD = −2.84, 95% CI: −9.57 to 3.90, p = 0.41) (Supplementary Fig. S6).
The meta-regression analysis results showed that year, sex, GA, and birth weight had no statistical significance for BPD (Table 4).
Exclusive HM versus any PF
Five studies9,10,22,23,25 (n = 2850) compared infants fed exclusively HM to those fed any amount of PF (including exclusive PF). The meta-analysis found a significant effect of feeding exclusive HM in reducing the frequency of BPD compared to any PF (OR = 0.57, 95% CI: 0.37–0.88, p = 0.01) (Table 3 and Supplementary Fig. S1). After excluding the study by Schanler et al., 23 which did not provide a clear definition of BPD, the results showed a significant effect of exclusive HM on BPD (OR = 0.61, 95% CI: 0.38–0.97, p = 0.04). Upon analyzing the between-group differences in GA, we found no significant overall differences (MD = −0.01, 95% CI: −0.10 to 0.08, p = 0.55) (Supplementary Fig. S2). However, one study 9 had a between-group GA difference of ≥0.5 weeks. After excluding this study, the meta-analysis of the remaining four studies still showed a significant effect of exclusive HM on BPD (OR = 0.61, 95% CI: 0.38–0.98, p = 0.04).
The meta-regression analyses showed that there were no significant results regarding year, birth weight, and sex, but they showed a statistically significant result with regard to GA (Table 4).
Mainly HM versus mainly PF
Twelve studies9–12,14,15,18,21–25 (n = 3617) compared infants fed mainly HM to those fed mainly PF (including exclusive HM and exclusive PF). The meta-analysis found a significant effect of mainly HM in reducing the frequency of BPD compared to mainly PF (OR = 0.72, 95% CI: 0.55–0.93, p = 0.01) (Table 3 and Supplementary Fig. S1). However, three studies18,21,22 did not provide a clear definition of BPD. After excluding these studies, the meta-analysis still showed a significant effect of mainly HM on reducing BPD (OR = 0.71, 95% CI: 0.53–0.95, p = 0.02).
In addition, when analyzing the between-group differences in GA, we found significant overall differences in GA (OR = −0.14, 95% CI: −0.21 to −0.07, p < 0.00001) (Supplementary Fig. S2). However, it is worth noting that four studies had substantial differences in GA between groups. To address this, we conducted a subgroup analysis by excluding these four studies9,14,18,21 with between-group GA differences of ≥0.5 weeks, leaving eight studies,10–12,15,22–25 which showed a significant effect of mainly HM on BPD (OR = 0.63, 95% CI: 0.46–0.86, p = 0.004) (Supplementary Fig. S7).
Four studies10,12,21,23 provided data on the number of days on mechanical ventilation. The meta-analysis showed that receiving mainly HM had no significant effect on the duration of mechanical ventilation (MD = 0.23, 95% CI : −1.77 to 2.23, p = 0.82) (Supplementary Fig. S8). Three studies10,12,21 provided data on the number of days on oxygen supplementation. The meta-analysis showed that receiving mainly HM had no statistically significant effect on this outcome (MD = 3.21, 95% CI: −13.40 to 19.83, p = 0.70) (Supplementary Fig. S9).
The meta-regression analysis results showed that year, sex, GA, and birth weight had no statistical significance for BPD (Table 4).
Any HM versus exclusive PF
Seven studies9–11,14,22,23,25 (n = 4060) compared infants fed any HM to those fed exclusively PF (including exclusive HM). The meta-analysis found no significant effect of any HM on BPD (OR = 0.88, 95% CI: 0.62–1.23, p = 0.46) (Table 3 and Supplementary Fig. S1). After excluding the study by Xu et al., 11 which used a different BPD definition, there was still no significant effect of any HM on BPD (OR = 0.96, 95% CI: 0.62–1.48, p = 0.84). Heterogeneity was considerable (p = 0.008, I2 = 65.7%). After analyzing the between-group differences in GA, we found significant overall differences (OR = −0.15, 95% CI: −0.23 to −0.06, p = 0.004) (Supplementary Fig. S2). GA might be a confounding factor. In the subgroup analysis, we excluded three studies9,11,14 with between-group GA differences ≥0.5 weeks, leaving four studies.10,22,23,25 The meta-analysis of these studies showed no significant effect of any HM on BPD (OR = 0.78, 95% CI: 0.57–1.06, p = 0.11), with moderate heterogeneity (p = 0.18, I2 = 39%).
The meta-regression analysis results showed that year, sex, GA, and birth weight had no statistical significance for BPD (Table 4).
Discussion
Apart from when HM and DHM are used as the exclusive sources of nutrition, a predominantly HM-based feeding approach similarly demonstrates significant protective effects against BPD.
This study systematically analyzed the evidence of the effect of HM on BPD compared to DHM or PF. The results of this meta-analysis showed that although feeding exclusive HM had no significant effect on BPD compared to DHM (p = 0.07), it significantly reduced the number of days on mechanical ventilation (p = 0.0004); infants fed with DHM had a lower incidence of BPD compared to PF (p = 0.02). Furthermore, in the analysis of HM and PF, both exclusive HM and mainly HM significantly reduced the risk of BPD compared to PF (p = 0.002, p = 0.01), while any HM showed no significant protective effect on BPD compared to exclusive PF (p = 0.46).
This meta-analysis showed that HM had no protective effect on BPD compared to DHM, which is similar to the results obtained by Eduardo Villamor-Martínez et al. 26 This may be due to the limited number of included studies, where two RCT studies received partial or mainly HM feeding. However, the study by Eduardo Villamor-Martínez et al. demonstrated that raw mother's own milk significantly reduced the risk of BPD compared to pasteurized mother's own milk. When comparing exclusive HM, mainly HM, and PF, there were significant effects on the risk of BPD, which is consistent with other studies. For example, Fonseca et al. 27 found that HM intake of 7 mL/(kg·d) within 6 weeks after birth could prevent the occurrence of BPD, and HM had a significant protective effect on moderate and severe BPD. Similarly, in a 5-year single-center prospective observational study in the United States in 2017, 28 univariate and multivariate analyses showed that for every 10% increase in HM feeding by 36 weeks of corrected GA, the incidence of BPD decreased by 9.5%, confirming a dose-effect relationship between HM and BPD.
HM has significant protective effects against BPD. However, current breastfeeding rates are low. It is necessary to implement more measures to increase breastfeeding rates.
HM feeding is the main preventive and therapeutic measure for BPD and has become the “gold standard” for enteral nutrition support in premature infants due to its nutritional richness, low osmolarity, fast gastric emptying, and abundant immune-active substances. 29 Clinical studies both domestically and internationally have shown that HM feeding can promote lung development, regulate immune function, reduce the incidence of BPD by improving nutritional status, and providing antioxidant and immunomodulatory factors.30,31 A 2018 Chinese study 32 found that exclusive HM feeding was superior to liquid preterm formula feeding in reducing BPD incidence by 10.4% in VLBWIs. Our recent study 33 in 2020 showed that oral colostrum administration for mechanically ventilated ELBW infants within 24 hours after birth, along with a 5-day continuous intervention, could reduce the incidence of BPD by 11.25%.
Current research indicates that HM also plays a protective role in preventing retinopathy of prematurity and necrotizing enterocolitis in preterm infants. However, the low rates of breastfeeding in NICUs, as evidenced by China's NICU-exclusive breastfeeding rate of only 9.3%, 34 highlight the need for concerted efforts to improve breastfeeding practices. Comprehensive strategies encompassing education, support, and policy interventions are necessary to increase breastfeeding rates and optimize the benefits of HM feeding for preterm infants.
The results of the meta-regression analysis indicate that GA may be a potential factor influencing the risk of BPD.
Our meta-regression analysis results only found a potential impact of GA on the risk of BPD and could not explain the relationships between publication year, sex, birth weight, and BPD. However, in the study by Meizhu et al., 35 it was shown that birth weight, male sex, mechanical ventilation, mechanical ventilation >7 days, respiratory distress syndrome in preterm infants, patent ductus arteriosus in preterm infants, sepsis, and NEC in preterm infants were all risk factors for BPD. Therefore, caution should be exercised in interpreting our results, which may be attributed to the limited number of studies included in our analysis. Further research, incorporating more and higher quality studies, is required to gain a better understanding of the relationship between these factors and BPD.
Limitation
We acknowledge the limitations of our study, which include the relatively small number of studies included and the significant differences in sample sizes analyzed among them. In addition, the majority of studies included in our analysis were observational in nature, resulting in significant heterogeneity in the demographic characteristics of the populations studied. It is important to note that our study did not specifically focus on exploring the protective effect of breast milk on the severity of BPD. To address these limitations, future research should aim to include larger and more diverse samples, as well as utilize more rigorous study designs such as RCTs. Furthermore, future studies should aim to explore the impact of breast milk on both the frequency and severity of BPD to provide a more comprehensive understanding of its protective effects.
Conclusion
In conclusion, our study findings suggest that both HM and DHM have a significant protective effect in reducing the frequency of BPD occurrence compared to PF. If the amount of HM is insufficient, feeding a proportion of more than 50% HM still provides a protective effect on BPD. GA may potentially play a role in the risk of BPD. The dose-effect relationship between HM and BPD still requires further research to explore the changes in BPD incidence when feeding more specific amounts of HM.
Footnotes
Acknowledgment
We have not received funds in support of research work or for covering the costs to public in open access.
Authors' Contributions
X.C.: Guarantor of the article, study concept and design, literature search, data analysis, and article writing. X.L.: literature search, data abstraction, participant article writing. Y.G.: contributed to interpretation of results and reviewed and revised the article. C.L.: contributed to the statistical analyses and interpretation of the results, and reviewed and revised the article. M.P.: literature search. All authors approved the final article as submitted.
Disclosure Statement
The authors declare no conflict of interest.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.