
Abstract
Long-term neurological damage as a result of head trauma while playing sports is a major concern for football athletes today. Repetitive concussions have been linked to many neurological disorders. Recently, it has been reported that repetitive subconcussive events can be a significant source of accrued damage. Since football athletes can experience hundreds of subconcussive hits during a single season, it is of utmost importance to understand their effect on brain health in the short and long term. In this study, resting-state functional magnetic resonance imaging (rs-fMRI) was used to study changes in the default mode network (DMN) after repetitive subconcussive mild traumatic brain injury. Twenty-two high school American football athletes, clinically asymptomatic, were scanned using the rs-fMRI for a single season. Baseline scans were acquired before the start of the season, and follow-up scans were obtained during and after the season to track the potential changes in the DMN as a result of experienced trauma. Ten noncollision-sport athletes were scanned over two sessions as controls. Overall, football athletes had significantly different functional connectivity measures than controls for most of the year. The presence of this deviation of football athletes from their healthy peers even before the start of the season suggests a neurological change that has accumulated over the years of playing the sport. Football athletes also demonstrate short-term changes relative to their own baseline at the start of the season. Football athletes exhibited hyperconnectivity in the DMN compared to controls for most of the sessions, which indicates that, despite the absence of symptoms typically associated with concussion, the repetitive trauma accrued produced long-term brain changes compared to their healthy peers.
Introduction
American football, the most popular sport in the United States, has been the subject of a growing concern about the effects of concussions sustained during practices and competitions, especially in high school athletes (Bailes et al., 2013; Belson, 2013; Breslow, 2013; Landau, 2013). An estimated 1.6–3.8 million sports- and recreation-related traumatic brain injuries (TBIs) occur each year in the United States (Langlois et al., 2006) and mild TBI (mTBI), often synonymous with concussion, is the most prevalent type, constituting ∼80–90% of all TBIs (Bigler and Maxwell, 2012). A considerable percentage of sports-related concussions go undiagnosed (Gregory, 2010; Meehan et al., 2013), which is particularly dangerous as research has suggested that mild head injury can accumulate to a more severe injury (Goldsmith and Monson, 2005; Ommaya et al., 1994). Further, athletes with undiagnosed concussions and associated potential neurological damage are at a higher risk for additional concussions (McCrea et al., 2004). Although awareness is growing (McCrory et al., 2013), better understanding of the neurological changes resulting from undiagnosed concussions and how these changes accumulate over time is needed to detect and mitigate long-term damage.
As of yet, concussion remains poorly understood (Cantu, 2006; Shaw, 2002), and there exists no reliable set of biometrics for concussion diagnosis that predicts recovery or long-term damage. Conventional structural neuroimaging techniques (e.g., magnetic resonance imaging [MRI] or computed tomography) are unable to detect this sort of subtle structural brain damage following concussion (Schrader et al., 2009). In sports, athletic trainers, medical personnel, and coaches rely on manifestation of recognizable acute signs and symptoms such as altered mental state, loss of consciousness, or motor instability to diagnose a concussion (Bruns and Jagoda, 2009; McCrory and Berkovic et al., 2000; Putukian, 2011). However, these symptoms have been shown to be poor measures of the time needed to recover (Hinton-Bayre and Geffen, 2002). Further, research studies have reported changes in neurophysiology in football athletes without any conventional physical or behavioral symptoms of concussion (Breedlove et al., 2012, 2014; Marchi et al., 2013; Poole et al., 2014; Talavage et al., 2014), which should be a cause for concern as collision sport athletes can experience hundreds of subconcussive hits during a single season (Broglio et al., 2011; Crisco et al., 2010, 2011; Guskiewicz et al., 2007). This finding is consistent with prior observation of chronic traumatic encephalopathy (CTE) in ex-National Football League (NFL) athletes without a history of concussion (G.P.O., 2010; Omalu et al., 2005, 2006, 2010), and that CTE severity is correlated with the number of years of playing professional football, but not necessarily the number of concussions reported (McKee et al., 2012). Thus, football athletes could accumulate neurological damage in the form of subconcussive insults even without the injury resulting in observable symptoms of concussion that would lead them to be removed from play. Therefore, more sophisticated techniques than symptom assessment are needed to accurately assess this damage as it occurs.
Previous work has firmly established that resting-state functional MRI (rs-fMRI) is able to detect subtle changes in the brain due to TBI, and thus is an ideal tool for studying subconcussive brain injury in collision sport athletes (Cao and Slobounov, 2010; Johnson et al., 2012; Kumar et al., 2009; Marquez De La Plata et al., 2011; Mayer et al., 2011; Slobounov et al., 2011; Sponheim et al., 2011; Zhou et al., 2012). The rs-fMRI uses intrinsic fluctuations in the blood oxygen level-dependent signal to measure brain network connectivity (Biswal et al., 1995; see Fox and Raichle, 2007, for review). One of these networks, the default mode network (DMN), is perhaps the mostly widely studied resting-state network (see Broyd et al., 2009, for review), and is used in this study because it has been shown to be both consistent (Shehzad et al., 2009) and clinically useful (Castellanos et al., 2008; Greicius et al., 2004, 2007).
In this study, we investigated the neurophysiological changes associated with the exposure to subconcussive head impacts using rs-fMRI of the DMN. Neurophysiological changes in a cohort of high school football athletes were tracked for a season, along with a cohort of noncollision-sport control athletes. If subconcussive head impacts induce neurophysiological changes due to accumulated mechanical loading, it would be expected that the functional connectivity measures of the DMN in football athletes would differ from those obtained in noncollision-sport control athletes because of accrued damage over years of playing. These measures would also change during the season as the athletes experience head impacts.
Materials and Methods
The Purdue University Institutional Review Board approved all research procedures used in this study. Parental consent and participant assent were obtained from all subjects under the age of 18. Consent was obtained from all subjects aged 18 and over. The data reported in this study correspond to those collected in year 2011 of the larger Purdue Neurotrauma Group study.
Participants
Two groups of high school male athletes participated in this study, on a voluntary basis. The first group comprised 22 collision-sport (football) athletes between the ages of 14 and 18 (mean 16.7 years), recruited from two local high schools to participate in this study during the 2011 football season (July–November). The second group comprised of 10 noncollision-sport athletes, aged 14–18 years (mean 16.7 years), recruited as controls for this study. These control athletes were recruited from three local high schools and participated in tennis (5 participants), cross-country running (1 participant), golf (1 participant), baseball (2 participants), and swimming (1 participant).
No participants were excluded on the basis of prior history of concussion. Noncollision-sport athletes did not have a history of concussion, whereas 9 out of 22 collision-sport athletes reported exactly one previously diagnosed concussion at the time of enrollment in this study. All athletes with a history of concussion had been cleared for contact participation by the team physician or athletic trainer before participation in this study. None of the participants was diagnosed by their athletic trainer or team physician as having experienced a concussion during the period of the study.
All athletes participated in at least two imaging sessions. The noncollision-sport athletes participated in two imaging sessions (20 total) spaced 4–6 weeks apart (Baseline and Follow-up). Collision-sport (football) athletes participated in 3–6 imaging sessions (87 in total); one before the start of contact practices (Pre-Season), at least one during the competition schedule (In-Season; all completed within 48 h of a game or practice), and one after the end of the season (Post-Season). All Pre-Season sessions were performed within the 4-week interval before the start of practice. In-Season sessions were performed during the season, at which time athletes were experiencing head collision events due to hits sustained at practices and games. Analysis of In-Season sessions, which included multiple sessions for some athletes, was grouped into 4-month-long windows (Month-1 to Month-4), such that no participant was represented more than once in any of these groups. In the case of multiple In-Season sessions conducted on a given participant, no two such sessions were conducted closer than 3 weeks apart. Post-Season sessions were conducted ∼5 months after the end of the football season. In the time period between the last In-Season and the Post-Season, all but one football athlete played another sport (e.g., basketball, baseball, track, golf, etc.), of which only one participated in a collision-sport (i.e., wrestling). The number of participants in each imaging session category is shown at the bottom of Figure 3.
Data acquisition
MRI imaging
All imaging was performed using a 3T General Electric (Waukesha, WI) Signa HDx, located at the Purdue MRI Facility (West Lafayette, IN). All data were acquired with a 16-channel brain array (Nova Medical, Wilmington, MA). rs-fMRI scans (gradient-echo echo-planar sequence with scan length 5 min 30 sec; repetition time (TR) 1500 ms; echo time (TE) 26 ms; flip angle 35°; 34 slices at 3.8 mm; field of view 20 cm; 64×64 acquisition, resulting in 3.125 mm×3.125 mm in-plane resolution) were acquired on all participants. These data were acquired immediately following two functional working memory scans, and before a high resolution T1-weighted anatomical, acquired for registration purposes using a three-dimensional spoiled gradient-recalled echo sequence (TR 5.768 ms; TE 2.032 ms; flip angle 73°; 0.9375 mm×0.9375 mm×1 mm).
Football telemetry
The Head Impact Telemetry System (HITS™; Simbex, Lebnon, NH) was installed in the helmets of all participating football athletes before the beginning of contact activities. This system was used to monitor head impacts (linear acceleration and hit counts) during every contact practice and game. A researcher was present at each practice, home game, and away game to ensure proper function at all times, as described in Talavage et al. (2014).
fMRI data preprocessing
Imaging data were preprocessed and analyzed using the Analysis of Functional NeuroImages (Cox, 1996) and FMRIB Software Library (Jenkinson et al., 2012; Smith, 2002). A preprocessing pipeline for the rs-fMRI data (see Fig. 1) was implemented based on that suggested by Jo et al. (2013), where localized white matter regressors were extracted and used to implement a reduced version of the ANATICOR (Jo et al., 2010), which results in minimal sensitivity to motion and dependence of correlation results on censoring. Volumes associated with movement of 0.4 mm or greater were censored from the regression.
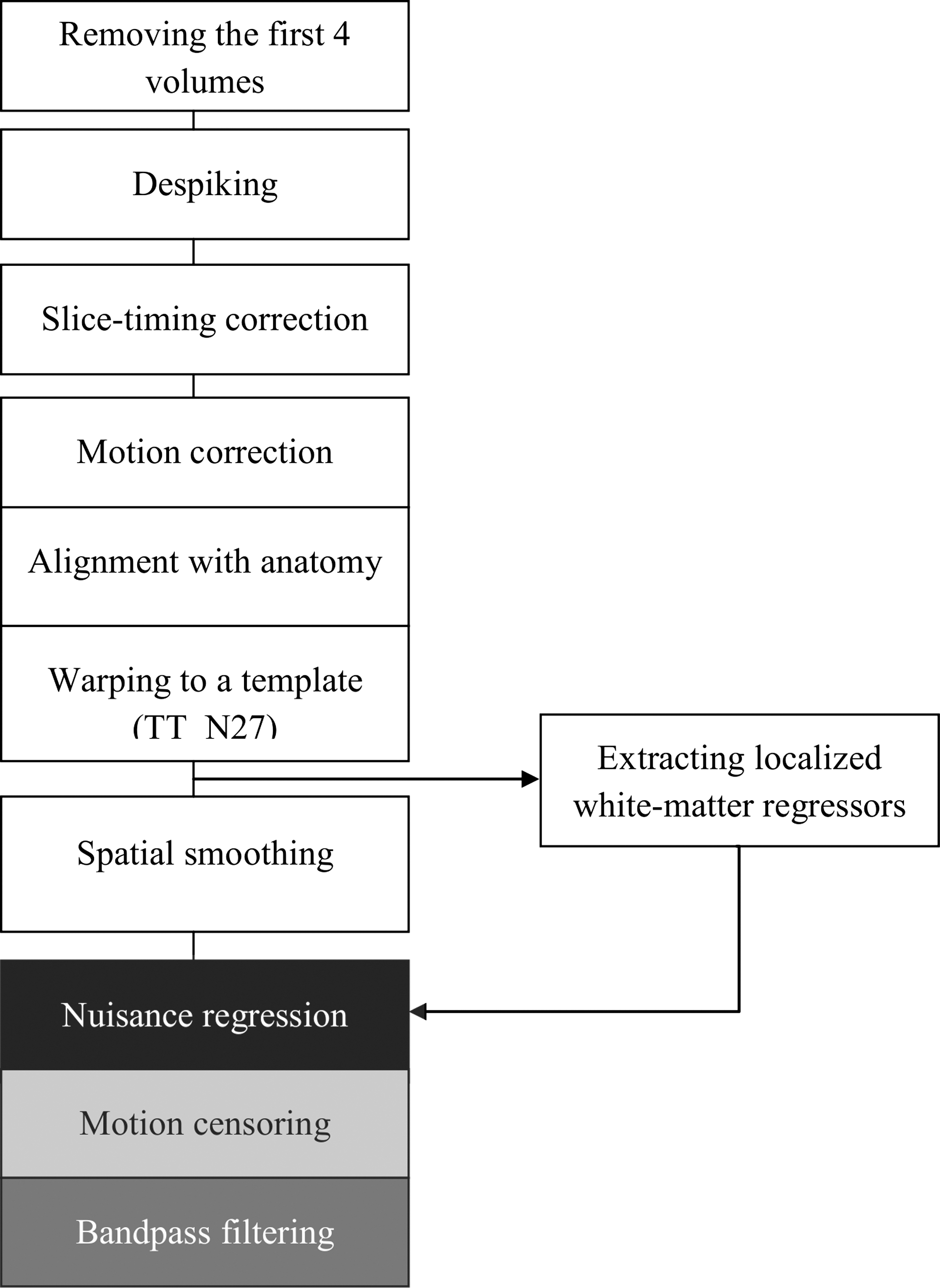
Annotated processing flowchart for the resting-state fMRI data. Warping to the Talairach template (TT_N27) was done using an Analysis of Functional NeuroImages tool, 3dQwarp, which uses nonlinear transformation and gives extremely accurate alignment.
Data analysis
To perform region-of-interest (ROI)-based correlational analyses, the Automated Anatomical Labeling atlas using the labels of Tzourio-Mazoyer, accessed using MarsBaR (Brett et al., 2002) was used to divide the brain into the 116 ROIs. The ROIs were made using the ROI definitions from the vbeta1 version of the Automatic Anatomical Labeling package (Tzourio-Mazoyer et al., 2002). A seed region was defined by a 12 mm radius spherical ROI placed at the posterior cingulate/precuneus (Talairach −5,49,40) (Jones et al., 2010). Bivariate correlations were used as a reflection of connection between ROI pairs. Each of the 116 ROIs were considered as possible connections to the seed ROI.
For each session of collision-sport and noncollision-sport athletes, ROI analyses were performed with a general linear model test to determine significant rs-fMRI DMN connections at the individual level. Based upon these results, correlation coefficients were converted into standard scores using a Fisher Transform. These standard scores were used for all subsequent group comparisons.
Any comparison between two groups was considered significant if it resulted in more than 12 regions with a change significant at p<0.05. This multiple comparison correction threshold is the upper bound of the 95% confidence interval around the expected 5.8 significant ROIs.
To establish a baseline measure of the reproducibility of the DMN, a paired t-test with Monte Carlo simulation [20,000 combinations; N-CHOOSE-(N–1)] was used to compare Baseline and Follow-up sessions of the noncollision-sport athletes and a threshold set at pFDR <0.05 to determine DMN connections that were significantly different.
To visualize possible spatial structural differences in the DMN of collision-sport and noncollision-sport athletes, all participants were analyzed at each session using a one-sample sign-rank test with a threshold set a pFDR <0.05 to determine significant connections in the DMN.
The number of significant DMN connections at each session could be affected by sample size, so this effect was investigated using an N-CHOOSE-K combinatorial analysis. Session Month-4 had the smallest sample size (N=8), so k=7 was selected for analysis of all sessions. For each session, all possible N-CHOOSE-7 combinations of participants were traversed with significant connections in the DMN identified using a one-sample sign-rank test with a significance threshold set at pFDR <0.05. From these combinatorial analyses, the median number of significant connections in DMN was computed for all the sessions of collision-sport and noncollision-sport athletes.
The effect of collision-sport versus noncollision-sport participation on DMN connections was evaluated by separately comparing the Baseline and Follow-up sessions of noncollision-sport controls with each session of collision-sport athletes. This was performed using a Monte Carlo simulation unpaired t-test (20,000 combinations) and a threshold set at pFDR <0.05 to determine whether the number of DMN connections significantly differed between the athlete groups in any particular session pairing.
Changes in the number of significant DMN connections across sessions were evaluated in the collision-sport athletes for possible relationship to exposure to collision events. Evaluations were made to detect the effect of recent collision events by comparing each session relative to its preceding session, and to detect cumulative effects of collision events by comparing each session relative to the Pre-Season session. Changes in DMN connections across consecutive sessions were evaluated using a combinatorial analysis. At least eight participants were common to each pair of consecutive sessions (e.g., Month-2 and Month-3), except for Month-3 to Month-4 (three common subjects). Therefore, for the session pairs Pre-Season/Month-1, Month-1/Month-2, Month-2/Month-3, and Month-4/Post, an N-CHOOSE-K (k=7) combinatorial analysis was performed as above for each of the two sessions separately and a Monte Carlo simulation paired t-test (20,000 combinations) was used to compare the numbers of significant DMN connections observed in these successive sessions. Changes in DMN connections relative to preparticipation evaluations were performed using this same approach. For collision-sport athletes this corresponds to the analysis of the Pre-Season/Month-X (X=1, 2, 3, and 4) and Pre-Season/Post-Season session pairs. For both recent and cumulative effect cases, the control analysis involved N-CHOOSE-7 combinatorial comparison of the noncollision-sport athletes' Baseline and Follow-up sessions.
Results
Data from one session were discarded because of excessive censoring (27% of volumes) due to motion artifacts.
The Baseline and Follow-up sessions of noncollision-sport controls had no significantly different DMN connections between the two sessions, confirming the reliability of the measurement.
DMN connectivity maps for each session are shown in Figure 2 for (A) noncollision-sport controls, and (B) collision-sport athletes. Collision-sport athletes show higher numbers of significant DMN connections than noncollision-sport athletes for Pre-Season, Month-2, Month-3, and Post-Season sessions, but lower or comparable number of DMN connections for Month-1 and Month-4 sessions.

Default mode network (DMN) connectivity maps for
The number of DMN connections, corrected for sample size, exhibited greater variability with session for the collision-sport athletes than their noncollision-sport peers (Fig. 3). At four of the measurement points (Pre-Season, Month-2, Month-3, and Post-Season) the collision-sport athletes exhibited a higher (but not necessarily significantly higher) median number of DMN connections than the noncollision-sport controls. Conversely, collision-sport athletes exhibited a lower (but not necessarily significantly lower) number of DMN connections relative to their noncollision peers at Month-1 and Month-4.
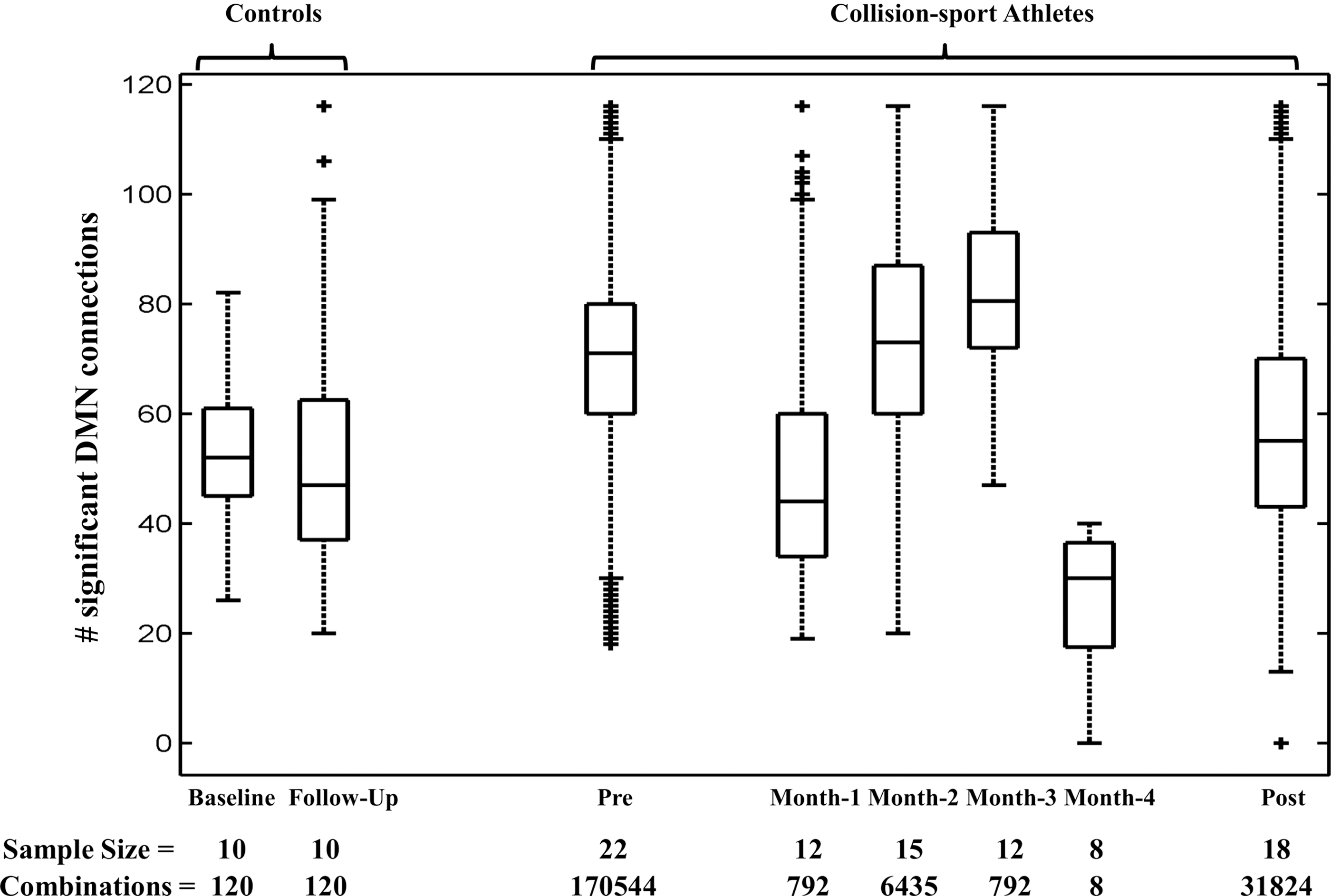
Box and whisker plots for number of significant DMN connections for all sessions of collision-, and noncollision-sport athletes, as determined using an N-CHOOSE-7 combinatorial analysis (see text for details). The line within the box indicates the median, and the box is bounded by the 25th and 75th percentiles from the combinatorial analysis. Also indicated is the raw sample size for each session, and the number of combinations used in the N-CHOOSE-7 analysis to derive the depicted distribution of DMN connections.
Table 1 presents the effect of participation in collision-sport on the DMN connectivity. It shows the number of DMN connections observed to be significantly different (i.e., correlation to the seed being either significantly higher or lower) between each session of collision-sport athletes relative to each of the Baseline and Follow-Up sessions for the noncollision-sport athletes.
Number of Regions Significantly Different Between Collision- and Noncollision-Sport Athletes
Number of atlas regions in collision-sport athletes exhibiting significantly different correlation with the seed region relative to Baseline and Follow-Up sessions of noncollision-sport athletes (n=10). Region counts representing a statistically significant group difference are indicated by an asterisk (*).
Figure 4 shows those areas of the brain in which the DMN connections appear to have been most affected by exposure to collision events. These ROIs are subsequently listed in Table 2.
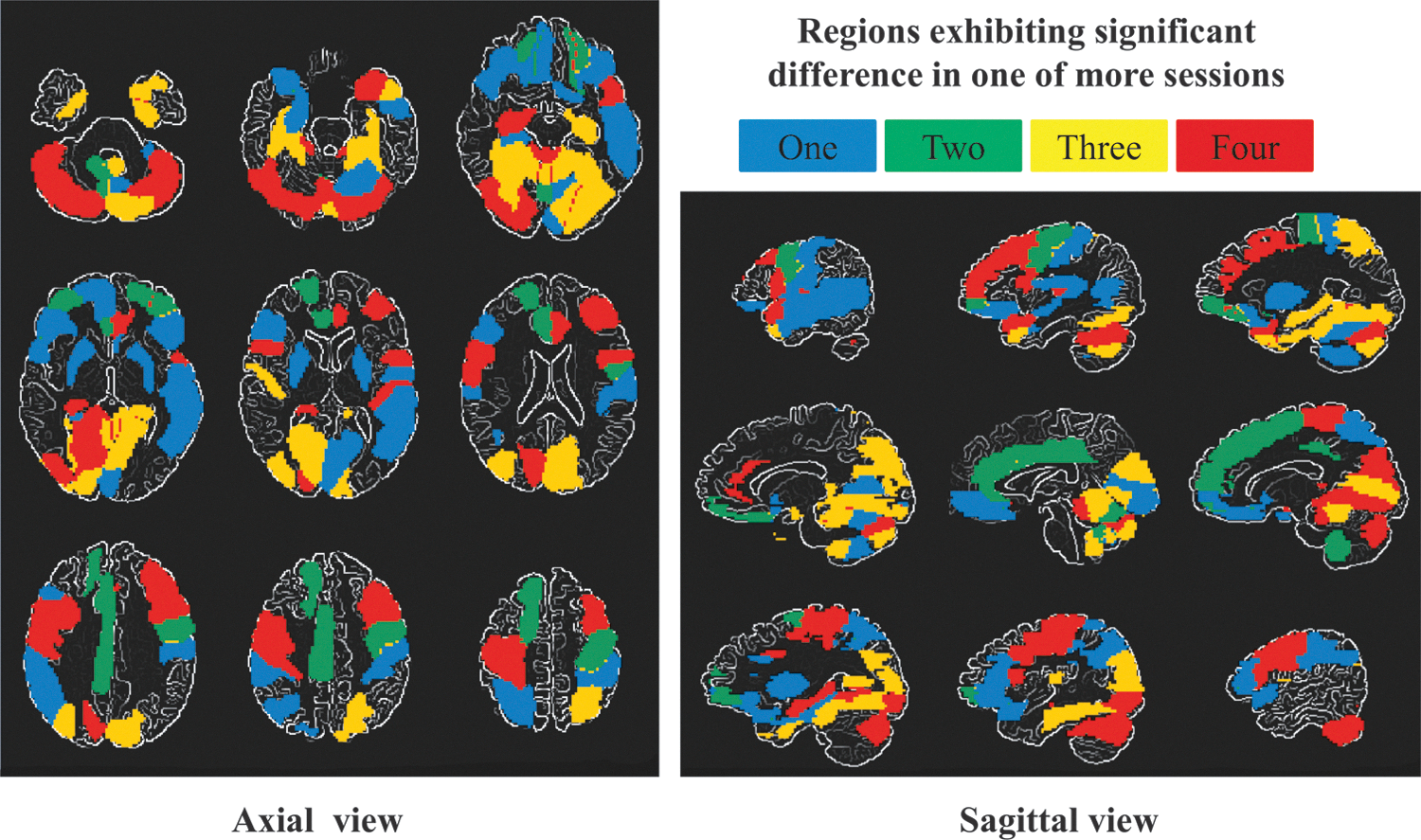
Map depicting atlas regions observed to exhibit statistically significant differences between collision-sport and noncollision-sport athletes in one or more imaging sessions. Coloration indicates the number of collision-sport athlete sessions at which differences were observed, counting as one any differences observed relative to Baseline and/or Follow-up sessions at a given Pre-/Month-X/Post-Season comparison.
List of Regions Exhibiting Statistically Significant Differences Between Collision-Sport and Noncollision-Sport Athletes
List of regions exhibiting statistically significant differences between collision-sport and noncollision-sport athletes in at least one session-wise comparison, as depicted in Figure 4, grouped by the number of collision-sport athlete sessions in which such differences were observed.
The effects of recent and cumulative collision events on the number of significant DMN connections are presented in Figure 5. Session-to-session changes in the number of DMN connections for the collision-sport athletes noted above were found to be statistically significant from Pre-Season to Month-1 and from Month-1 to Month-2 (Fig. 5A). Cumulative effects of collision events on the number of DMN connections (relative to the Pre-Season session) were found to be statistically significant at Month-1, Month-3, and Post-Season sessions (Fig. 5B). The number of DMN connections was significantly reduced at Month-1 and in the Post-Season, with a small increase in connections observed at Month-3. Note that Month-4 exhibited a marked average and median reduction, but this difference was not statistically significant.
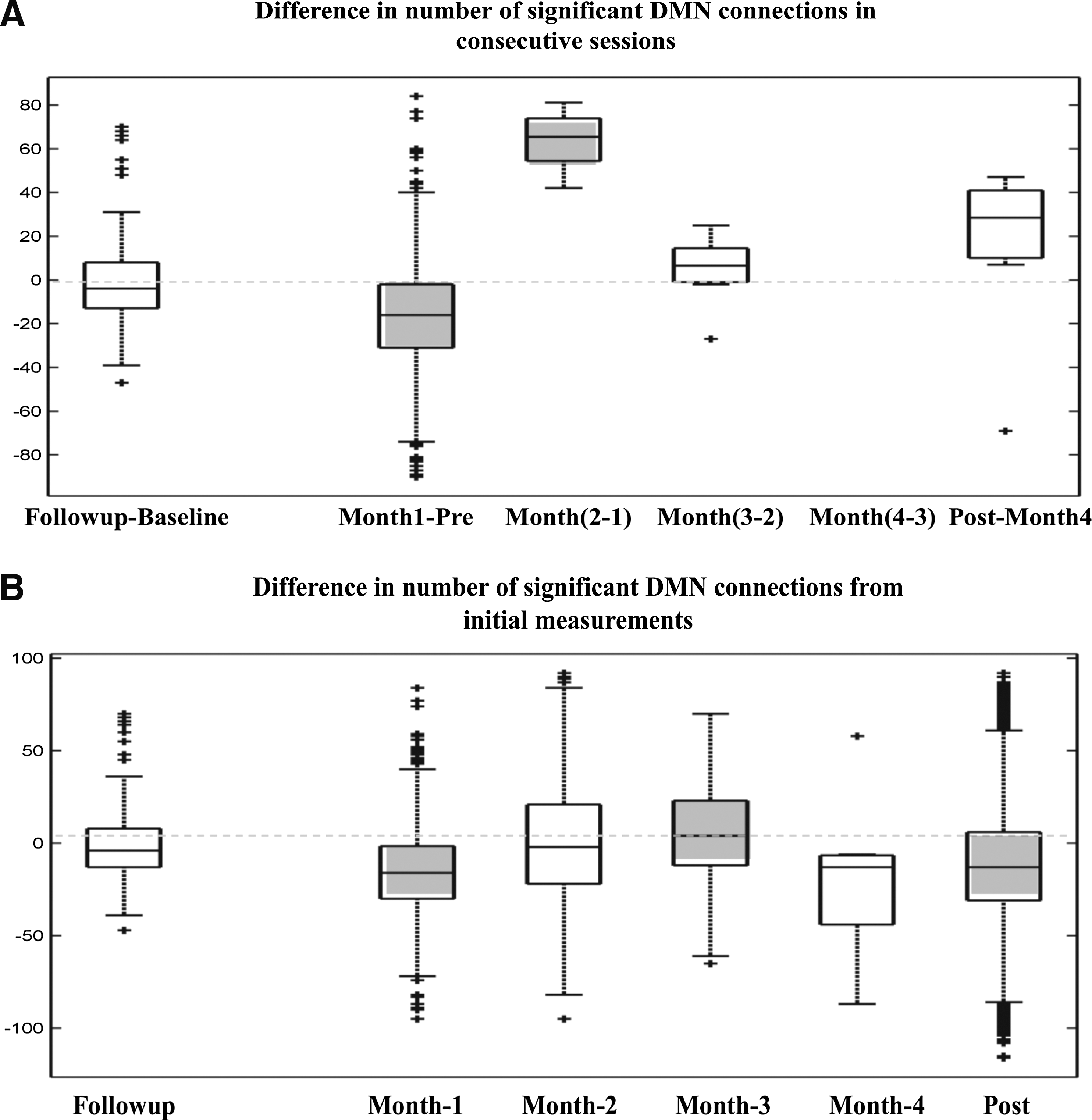
Comparison of the number of significant DMN connections across sessions for both noncollision- and collision-sport athletes.
Discussion
In this work it has been observed that the resting-state brain connectivity in high school collision-sport athletes differs from that of noncollision-sport athletes, and exhibits temporal variations that may be associated with changes in mechanical loading over the course of a competition season. As seen in Figures 2 and 3, the collision-sport athletes were significantly hyperconnected, relative to the noncollision-sport athletes, even when they were not experiencing head collision events—before the beginning of their practice and game schedules (Pre-Season) and, again, long after the season was over (Post-Season). This observation suggests an accumulative long-term effect on brain connectivity arising from repetitive subconcussive head trauma, and accrued over multiple years of participation in collision sports. Although noncollision-sport athletes were not found to exhibit any significant change in the extent of DMN connectivity in a test/retest paradigm, their collision-sport athlete peers exhibited appreciable variability across successive sessions and relative to their own baseline (Fig. 5). This short-term variability observed in the collision-sport athlete population suggests that acute consequences of repeated head collision events do exist and do (in the short-term) affect the physiology inherently assessed using resting-state functional connectivity.
One hypothesis to explain the hyperconnectivity in collision-sport athletes observed in this study could be that, although the subconcussive blows likely produce a lesser version of the physiological response that has been observed in concussion (Giza and Hovda, 2001), when these insults are repeated in a short interval, this mechanical loading may produce neurophysiological alterations that exceed the short-term compensatory abilities of the brain. Exposure to prolonged periods of repetitive head trauma and the associated accumulating damage could lead to acute impairment of axonal tracts. However, because the brain has many parallel information processing pathways, acute trauma to any one pathway involved in a particular task does not necessarily result in the inability of the brain to perform that task. Rather, alternate pathways are used, and over time, these collateral projections will be strengthened, a phenomenon which would manifest as the hyperconnectivity observed in this study. Research has reported both hyperconnectivity and hypoconnectivity in DMN as a result of concussive blows. Whereas Mayer et al. (2011) reported decreases in DMN connectivity in the subacute phase of injury, others have observed both increases and decreases in DMN connectivity on a region-by-region basis (Johnson et al., 2012, 2014; Zhou et al., 2012). These latter reports are consistent with the hypothesis stated above. Adaptation to repeated exposure may thus result in long-term recruitment of collateral projection pathways such that the normal (i.e., asymptomatic) functioning of the brain may be maintained, even during periods of high mechanical loading, which can be detected with rs-fMRI. This hypothesis could be strengthened by concurrent cognitive studies in future work.
In-Season measurements at which collision-sport athletes exhibit the greatest difference (see Figs. 2 and 3) from their own preparticipation (Pre-Season) measures—Month-1 and Month-4—are of particular interest. It is informative to examine these two months in the context of the mechanical loading associated with hits to the head, both on the basis of high magnitude, defined in this study as hits with linear acceleration >60G, corresponding to the 95th percentile of all hits across all football athletes (Breedlove et al., 2012) and number of hits. In this particular season, the average number of high-magnitude hits per week experienced by the players during Month-1 through Month-4 (and the associated average total recorded hits per week) was 1.73 (48.1), 1.93 (35.7), 1.86 (39.6), and 2.60 (83.9). From these numbers, the greatest period of mechanical loading was Month-4. Month-1 through Month-3 had relatively stable high-magnitude loading, but with a generally higher rate of total hits in Month-1.
One hypothesis to tie these observations together is that the level of connectivity in the brain can be affected by recent mechanical loading, particularly as it relates to prior mechanical loading. In other words, when the level of loading changes markedly, the brain may have to adapt, and this process may be reflected in rs-fMRI measurements. In this study, the decreases in connectivity observed at Month-1 and Month-4 are each associated with a transition in the level of collisions (total number and high-magnitude) being experienced—for example, Month-1 represents the onset of practice, and Month-4 represented an increase in general intensity of practices and games associated with the end-of-season tournament. The hypothesis would suggest that the brain was transiently unable to maintain the Pre-Season level of compensatory hyperconnectivity with the increase in the total hits and high-magnitude hits, but, during the season, was able to adapt to the stable level of mechanical stress in Month-2 and Month-3 and return to this altered state. In light of this hypothesis, it is unlikely that the Month-1 and Month-4 states, despite being more similar to the noncollision-sport athlete controls, represent a more normal state of brain activity. Rather, this would represent a second mechanism of brain alterations that is happening at a more acute scale.
Critically, these two months (Month-1 and Month-4) during which the collision-sport athletes exhibit the greatest deviation from their own baseline measures are also the times at which they are most consistent in the extent and degree of connectivity with the noncollision-sport controls (see Fig. 2). This key observation, in addition to the fact that they were not experiencing acute concussion symptoms, suggests that the hyperconnectivity may be a compensatory mechanism which permits these individuals to experience some level of acute neural trauma without exhibiting externally observable symptoms. This hypothesis is consistent with our own observations of elevated Pre-Season measures in MR spectroscopy, dropping to normal levels during the competition season (Poole et al., 2014), but in slight contrast to Hampshire et al. (2013), who observed pronounced hyperactivation, instead of hyperconnectivity, in the DLPFC region of retired NFL athletes, as a postulated compensatory mechanism.
Another significant observation is that subconcussive hits accumulated over a season caused connectivity changes that have not gone away by 5 months after the season (Fig. 3). If the Pre-Season measurement is taken as an accurate baseline, this suggests that neural reorganization occurring as a result even of subconcussive hits may preclude true return to normal. Combined with the fact that these athletes were asymptomatic, this observation suggests that neural plasticity could be acting as a compensatory mechanism for possible subconcussive damage, comparable to the postulation of Hampshire et al. (2013).
These results represent the first longitudinal analysis of the DMN in collision-sport athletes who are not concussed (i.e., have experienced only subconcussive mTBI rather than concussive mTBI), and illustrate the critical importance of having a Pre-Season baseline available to assess the health of the athletes. Were these athletes only to be evaluated one month into the season and compared with noncollision-sport controls, it would appear that there were no effects whatsoever of repetitive blows to the head. While an isolated evaluation after the season would identify the presence of changes in connectivity, this could be argued to be transient rather than (as appears to be the case) chronic. Therefore, continued longitudinal investigation is critical to understanding how mechanical loading brings about changes in connectivity, how the time course of either adaptation or repair may play a role in the observation of connectivity changes following concussive and nonconcussive injury. Of particular interest at this time would be how early in the history of exposure to repetitive head trauma does hyperconnectivity arise, and whether such connectivity may recover to normal subsequent to the end of collision-sport participation.
Several factors may have limited the conclusions that have been drawn from this study. First, the sample size for different sessions was not constant which might have influenced the changes observed, despite the combinatorial analysis introduced to compensate for this limitation. Second, it might be argued that the onset of exercise could be responsible for the drop in DMN connectivity observed at the beginning of the season (Month-1 session). However, this is unlikely as all football athletes were first evaluated during late summer when all were participating in football practice sessions. Therefore, none of the athletes had been without exercise before the beginning of monitoring.
Having observed changes in connectivity that are likely related to exposure to repetitive head trauma, a number of key questions may be highlighted for future investigation. Initial efforts will seek to determine how the changes in connectivity may be related to the collision dose, taking into account both the number and sequencing of experienced acceleration events, recognizing that this will require the use of telemetry systems that are markedly improved over the previously utilized system (Jadischke et al., 2013). While the two athlete cohorts in this study were derived from common underlying populations, and are thus well matched in socioeconomic and educational status, increases in the size of the collision-sport and noncollision-sport cohorts and matching the number of athletes for all sessions would facilitate further reduction of possible population-level confounds, including diet, academic performance, and general health. Finally, value is likely to be derived from more detailed evaluation of resting-state networks on a region-by-region basis, concurrent cognitive studies, and from the use of alternate methodologies (e.g., Independent Component Analysis [ICA], Graph Theory Analysis) that may prove more robust either for longitudinal evaluations or for identification of the contribution of exposure measures to changes in resting-state networks.
Conclusions
In summary, the results presented in this study show that high school football athletes, who were asymptomatic and not diagnosed with concussions during the season, but did receive subconcussive blows to their head, have altered functional connectivity when compared with their noncollision-sport athlete cohort and their own baseline measures, indicating both short- and long-term effects of subconcussive mechanical loading. Further, these changes persist long after the season without return of the athletes to their baseline measures. Such marked deviations in football athletes at such an early age, without readily diagnosable symptoms is a cause for concern. Observation of a cortical compensatory mechanism within DMN that counteracts these changes in functional connectivity associated with mechanical loading merits further investigation. To this end, changes in functional connectivity should be examined with more sophisticated methodologies (such as ICA or Graph Theory Analysis) in the context of changes to the history of subconcussive mechanical loading. Such efforts will be best served through longitudinal neuroimaging studies, which have the potential to achieve early detection of neurological damage that could accumulate to produce long-term cognitive impairment.
Footnotes
Acknowledgment
The authors would like to thank Dr. Gregory G. Tamer, Jr., for the assistance in data collection.
Author Disclosure Statement
No competing financial interests exist.