
Abstract
Background:
This study investigated alterations in the intrinsic thalamic network of patients with juvenile myoclonic epilepsy (JME) based on an electroencephalography (EEG) source-level analysis.
Materials and Methods:
We enrolled patients newly diagnosed with JME as well as healthy controls. The assessments were conducted in the resting state. We computed sources based on the scalp electrical potentials using a minimum-norm imaging method and a standardized, low-resolution, brain electromagnetic tomography approach. To create a functional connectivity matrix, we used the Talairach atlas to define thalamic nodes and applied the coherence method to measure brain synchronization as edges. We then calculated the intrinsic thalamic network using graph theory. We compared the intrinsic thalamic network of patients with JME with those of healthy controls.
Results:
This study included 67 patients with JME and 66 healthy controls. EEG source-level analysis revealed significant differences in the intrinsic thalamic networks between patients with JME and healthy controls. The measures of functional connectivity (radius, diameter, and characteristic path length) were significantly lower in patients with JME than in healthy controls (radius: 2.769 vs. 3.544, p = 0.015; diameter: 4.464 vs. 5.443, p = 0.024; and characteristic path length: 2.248 vs. 2.616, p = 0.046).
Conclusions:
We demonstrated alterations in the intrinsic thalamic network in patients with JME compared with those in healthy controls based on the EEG source-level analysis. These findings indicated increased thalamic connectivity in the JME group. These intrinsic thalamic network changes may be related to the pathophysiology of JME.
Impact statement
This study investigated alterations in the intrinsic thalamic network of patients with juvenile myoclonic epilepsy (JME) based on an electroencephalography source-level analysis. Our findings showed alterations in the intrinsic thalamic network of patients with JME compared with healthy controls. These alterations indicated increased thalamic connectivity in the JME group, suggesting the potential role of intrinsic thalamic network changes in JME pathophysiology.
Introduction
Childhood absence epilepsy, juvenile absence epilepsy, juvenile myoclonic epilepsy (JME), and epilepsy with generalized tonic–clonic seizures are classified as idiopathic generalized epilepsy. Among them, JME is the most common syndrome in adolescents and adults, with an age of onset between 10 and 24 years (Baykan and Wolf, 2017; Grunewald and Panayiotopoulos, 1993; Hirsch et al., 2022). It is characterized by myoclonic seizures, predominantly on awakening, and is typically triggered by sleep deprivation and photic stimulation (Baykan and Wolf, 2017; Grunewald and Panayiotopoulos, 1993; Hirsch et al., 2022).
Interictal epileptiform discharges on electroencephalography (EEG) commonly show irregular generalized 3- to 5.5-Hz spike- and polyspike-wave discharges, whereas ictal EEG presents generalized polyspike waves with myoclonic jerks (Baykan and Wolf, 2017; Grunewald and Panayiotopoulos, 1993; Hirsch et al., 2022). Furthermore, patients with JME exhibit impaired cognitive function (memory and execution) despite having normal intelligence and mood (Kim et al., 2007b).
Evidence from existing literature suggests the pivotal role of the thalamus in JME pathophysiology. For instance, neuroimaging studies using magnetic resonance imaging (MRI) have shown structural and functional alterations in the thalamus in patients with JME (Kim, 2017). A voxel-based morphometry study demonstrated similar findings, indicating reduced gray matter volume in the bilateral thalamus in JME patients despite normal visual assessment of structural MRI (Kim et al., 2007a).
Specifically, significant alterations in the laterodorsal, suprageniculate, ventral posterolateral, ventromedial, and inferior pulvinar nuclei were observed in patients with JME compared with healthy controls (Lee et al., 2020). Diffusion tensor imaging (DTI) further demonstrates these changes, revealing reduced fractional anisotropy in white matter regions associated with the anterior thalamus and prefrontal cortex (Deppe et al., 2008).
Resting-state functional MRI (rs-fMRI) analyses of the thalamus similarly revealed reduced thalamocortical functional connectivity in the medial prefrontal cortex and precuneus/posterior cingulate cortex (Kim et al., 2014). Furthermore, a meta-analysis of magnetic resonance spectroscopy findings reported decreased N-acetyl aspartate levels in the thalamus (Zhang et al., 2016). Collectively, these findings have consistently underscored the importance of the thalamus in JME.
Recent brain network research emphasizes the concept of epilepsy as a brain network disorder, including the mechanisms underlying JME (Lee and Park, 2019; Lee et al., 2021; Lee et al., 2020). In brain network analysis, structural connectivity can be evaluated using DTI, whereas functional connectivity is assessed using rs-fMRI or EEG (Babaeeghazvini et al., 2021; Rossini et al., 2019).
Compared with rs-fMRI analysis, EEG provides lower spatial resolution, but has superior temporal resolution (Babaeeghazvini et al., 2021; Rossini et al., 2019). This makes EEG particularly useful in management of patients with epilepsy. Notably, the quantitative EEG analysis can be divided into sensor-level and source-level analyses (Brunner et al., 2016; Lai et al., 2018; Yu et al., 2022).
Of the two, source-level analysis is known for its ability to analyze subcortical structures (e.g., thalamus) and its improvement of temporal resolution by increasing the number of nodes (Brunner et al., 2016; Lai et al., 2018; Lee et al., 2023; Yu et al., 2022). However, spatial resolution in EEG is limited due to the small number of channels and the inherent inverse problem (Van Diessen et al., 2015).
Despite the proposal of several solutions to this issue (e.g., shifting from sensor- to source-level analysis), no definitive solution has been established. As such, the combination of connectivity analysis with source-level analysis is thought to be a promising approach to this problem (Van Diessen et al., 2015).
While previous neuroimaging studies have indicated the significant role of the thalamus in JME pathophysiology, evidence from EEG-based functional studies is lacking. Therefore, the aim of this study is to understand the pathophysiology of JME through source-level analysis using scalp EEG, particularly by examining the intrinsic thalamus network. Additionally, the study aims to demonstrate the utility of graph theory in future EEG source-level analyses.
Materials and Methods
Participants
This study was approved by the institutional review board of our hospital (IRB No.: HPIRB 2022-04-022-002). This retrospective study was conducted at a single epilepsy center, where patients were retrospectively enrolled based on the following criteria: (1) JME diagnosis by three epileptologists (S.E.K., K.M.P., and D.A.L.) based on diagnostic criteria, clinical assessments, and EEG findings (Baykan and Wolf, 2017; Grunewald and Panayiotopoulos, 1993; Hirsch et al., 2022); (2) high-quality EEG sufficient for quantitative analysis performed at our hospital at the time of diagnosis; and (3) drug-naïve status, including antiseizure medication (ASM), between March 2010 and August 2022.
Age- and sex-matched healthy controls in our previous study were also enrolled for the current study (Jang et al., 2017). These participants had normal brain MRI and EEG findings and did not have any other medical, neurological, or psychiatric diseases. Collected data included demographic and clinical characteristics of patients with JME, including age, sex, age at seizure onset, and seizure type.
EEG acquisition
Both patients with JME and healthy controls underwent resting-state EEG while awake, but with their eyes closed. All recordings were performed using the same type of EEG machine (TWin® EEG software system) and methodology. Trained personnel performed the recordings using gold electrodes attached with electrode paste according to the international 10–20 system, which made use of 23 electrodes (Fp1, Fp2, F7, F8, T1, T2, T3, T4, T5, T6, O1, O2, F3, F4, C3, C4, P3, P4, Cz, Pz, Oz, A1, and A2).
Electrode impedance was maintained at <5 kΩ. Recordings were sampled at a frequency of 250 Hz for at least 30 min.
EEG preprocessing and source modeling
EEG preprocessing and source modeling were performed using the Curry program, version 8. Data were re-referenced to an average montage and filtered between 1.0 Hz (low) and 30.0 Hz (high). After manual review, 3-sec epochs were selected, which showed the presence of alpha activity with maximum voltage in posterior regions without any artifacts or epileptiform discharges (Fraschini et al., 2016). All EEG data were reviewed by D.A.L.
Source estimation was then conducted using a combination of minimum-norm imaging, which estimated the amplitude and distribution of brain sources using scalp electric potentials, and standardized low-resolution brain electromagnetic tomography (sLORETA). Moreover, a functional connectivity matrix was constructed by defining nodes using the Talairach atlas and measuring brain synchronization (edges) using coherence.
Only 14 nodes within the thalamus were selected from the available nodes to calculate the intrinsic thalamic network (Table 1).
Thalamic Nodes Selected from Among Several Nodes
Graph theoretical analysis
The graph theoretical analysis was performed using Brain Analysis Using Graph Theory (Mijalkov et al., 2017). Fpr functional connectivity measures were extracted from the undirected weighted connectivity matrix, which included the average degree, average strength, radius, diameter, characteristic path length, global efficiency, local efficiency, mean clustering coefficient, transitivity, modularity, and small-worldness index (Farahani et al., 2019).
These measures were computed for both groups and subsequently compared. Figure 1 illustrates the complete EEG analysis process of the study.
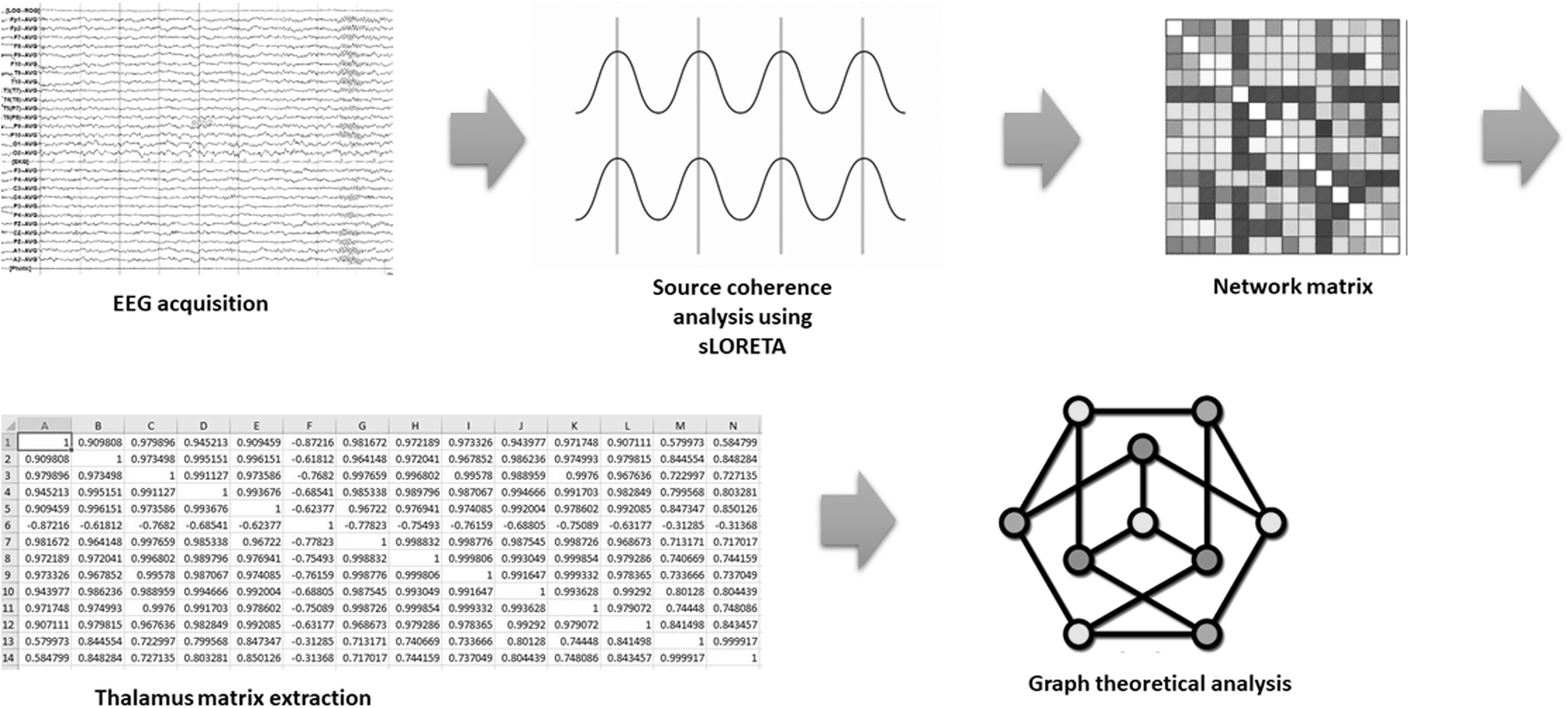
Process of the EEG source-level analysis. EEG, electroencephalography.
Statistical analysis
Categorical variables are presented as frequencies and percentages, whereas numerical variables are presented as means ± standard deviations. Clinical characteristics between patients with JME and healthy controls were compared using chi-square or independent Student's t-tests. To compare functional connectivity of the network measures at the group level, nonparametric permutation tests with 5000 permutations were utilized to assess statistical significance.
All statistical tests were performed using MedCalc® Statistical Software, version 20.014 (MedCalc Software Ltd., Ostend, Belgium), and statistical significance was set at p < 0.05.
Results
Clinical characteristics
This study included 67 patients with JME and 66 healthy controls. Clinical characteristics, including age and sex (age, 23.1 vs. 22.1 years, p = 0.401; and male sex, 30/67 [44.8%] vs. 33/66 [50%], p = 0.547), showed no significant differences between these groups (Table 2).
Clinical Characteristics of Patients with Juvenile Myoclonic Epilepsy and Healthy Controls
Intrinsic thalamic network
Table 3 presents differences in intrinsic thalamic networks based on the EEG source-level analysis between patients with JME and healthy controls. Among functional connectivity measures, the radius, diameter, and characteristic path length were lower in patients with JME than those in healthy controls (radius: 2.769 vs. 3.544, p = 0.015; diameter: 4.464 vs. 5.443, p = 0.024; and characteristic path length: 2.248 vs. 2.616, p = 0.046). This suggests increased thalamic connectivity in the JME group.
Differences in the Intrinsic Thalamic Network Between Patients with Juvenile Myoclonic Epilepsy and Healthy Controls Based on Electroencephalography Source-Level Analysis
CI: 95% confidence interval of the difference between groups.
p < 0.05.
Conversely, no significant differences were observed in other functional connectivity measures, including the average degree, average strength, global efficiency, local efficiency, mean clustering coefficient, transitivity, modularity, assortativity coefficient, and small-worldness index.
Discussion
In this study, we utilized an EEG source-level analysis to investigate the intrinsic thalamic network of patients with JME and healthy controls, revealing significant differences between the two. The functional connectivity measures of radius, diameter, and characteristic path length were lower in patients with JME compared with those in healthy controls, suggesting increased thalamic connectivity in JME patients.
Graph theory serves as a robust mathematical framework for quantifying and analyzing complex networks simultaneously with active research, particularly in the field of neuroscience (Bernhardt et al., 2015). The parameters employed for network analysis predominantly involve measures of integration and segregation, or the equilibrium between these aspects, as reflected by the small-worldness index (Yun et al., 2020).
In this study, measures that are associated with network integration included the average degree, average strength, radius, diameter, characteristic path length, and global and local efficiency. Meanwhile, measures associated with network segregation included the mean clustering coefficient, transitivity, modularity, and assortativity coefficient (Yun et al., 2020).
In graph analysis, the diameter represents the greatest distance between two vertices, while the radius represents the shortest distance between a vertex and all other vertices (Farahani et al., 2019). Therefore, given the shorter distances between thalamic network nodes in patients with JME in our study, the intrinsic thalamic connectivity in the JME group was higher than that in the normal group.
Furthermore, the characteristic path length in patients with JME was lower than that in healthy controls, reflecting greater ease of information flow across the network. The average number of edges in the shortest paths between all vertex pairs is defined as the characteristic path length, which is one of the most important and frequently invoked characteristics of a network (Watts and Strogatz, 1998). These paths are formed from a sequence of distinct connected nodes in a network, wherein the characteristic path length represents the ease of integrating information.
Taking these findings collectively, our study indicates an increased integration of the global network among patients with JME, suggesting increased connectivity in their intrinsic thalamic networks.
Thalamic stimulation has been shown to elicit a bilateral, synchronous 3-Hz spike and wave pattern on EEG in patients with JME (David et al., 1981). This implies involvement of the thalamus, particularly the nucleus reticularis thalami, in JME pathophysiology due to its crucial role in cortical synchronization and presumed function as the pacemaker for rhythmic cortical oscillations (spindle activity) (de Curtis and Avanzini, 1994).
In fact, several studies have suggested that the network mechanisms underlying spindle formation can also explain spike and wave discharges. For instance, experiments on genetic animal models of spontaneous generalized epilepsy confirmed the involvement of the thalamocortical system in spike and wave discharges (de Curtis and Avanzini, 1994).
Prior physiologic and neuroimaging studies have consistently reported structural and functional abnormalities in the frontal lobes and thalamus of patients with JME (Lin et al., 2009; Pulsipher et al., 2009). Notably, significantly smaller thalamic and frontal volumes were significantly correlated with executive functioning in these patients (Pulsipher et al., 2009). Moreover, an MRS study indicated potential nonuniform cortical hyperexcitability in JME, revealed by diverse patterns of neurochemical dysfunction within the thalamocortical circuitry (Lin et al., 2009).
In contrast, another MRI-based study confirmed findings of reduced overall thalamic volumes and increased thalamic network modularity in patients with JME (Lee et al., 2020). Since modularity is a parameter associated with network segregation, it would often show a tendency of increased network integration, as reported in our study. This discrepancy could be attributed to the inclusion of chronic JME cases in the previous study. Thus, the increased thalamic connectivity in our study is likely related to JME epileptogenesis.
This assumption is supported by the findings from two previous studies. The first study, which investigated the dynamic functional connectivity of subcortical circuit changes in patients with JME, showed increased variability in striatal–thalamic networks (Yang et al., 2022b). The second study, performed by the same authors of the first, revealed the diverse range of structural and functional connections in the anterior nucleus of the thalamus and proved the efficacy of deep brain stimulation in epilepsy (Yang et al., 2022a).
Compared with other modalities that measure brain function, EEG boasts a key advantage in its direct reflection of neuronal activity (Rossini et al., 2019). However, it is limited by its poor spatial resolution and inherent inverse problem, which remain despite several solutions, including transitioning from sensor-level to source-level analysis (Van Diessen et al., 2015).
In this study, we employed a combined approach using sLORETA for the inverse solution and coherence for the source-level analysis. Coherence, which measures the linear correlation between the amplitudes of two signals in the frequency domain (Schoffelen and Gross, 2009), is one of the most common and relatively straightforward approaches for obtaining insights into functional networks (Rossini et al., 2019).
Despite the valuable findings presented in this study, certain limitations should be acknowledged. First, due to its cross-sectional design, we could not evaluate the clinical implications of the intrinsic thalamic network. Further research is needed to elucidate these implications since ASM response and epilepsy duration are other significant associations in patients with JME (Kim et al., 2020; Park et al., 2020).
Second, due to our reliance on routine EEG to evaluate functional connectivity, the number of electrodes used in this study was limited. However, to compensate for this limitation, we used an EEG source-level analysis. Third, although we utilized the sLORETA and Talairach atlas to define nodes within the thalamus, we only identified 14 nodes for calculating the intrinsic thalamic network.
Despite this relatively small number of nodes, we used the standard brain template by Curry for source localization, which may reflect the reported thalamic volume asymmetry between the left and right sides (Keller et al., 2012).
Conclusions
This study utilized the EEG source-level analysis to demonstrate alterations in the intrinsic thalamic network of patients with JME compared with healthy controls. These findings indicate increased thalamic connectivity in the JME group, suggesting that intrinsic thalamic network changes may be related to JME pathophysiology.
Data Sharing Statement
Data that support the findings of this study are available upon reasonable request.
Footnotes
Authors' Contributions
D.A.L. was involved in methodology, formal analysis, investigation, data curation, writing—original draft, writing—review and editing, and visualization.
S.E.L. was involved in conceptualization and writing—review and editing.
K.M.P. was involved in conceptualization, methodology, software, validation, formal analysis, investigation, data curation, writing—original draft, writing—review and editing, visualization, and project administration.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Ministry of Science and ICT of the Republic of Korea (NRF-2021R1F1A1049605).